
Abstract
Background:
Quality improvement initiatives in the acute care setting often target reduction of mortality and length of stay (LOS). Unplanned care escalations are associated with increased mortality risk and prolonged LOS, but may be precipitated by different factors, including appropriate triage, bed availability, and post-admission deterioration.
Objectives:
This work evaluates different transfer timeframes to quantify the impact of deterioration-associated unplanned transfers to intensive care (ICU) on mortality and LOS, informing evidence-based interventions to improve patient care.
Design:
This retrospective analysis examined 519 181 adult inpatients discharged from 15 hospitals in the United States. A propensity matched cohort analysis compared mortality and overall hospital LOS for patients admitted to routine and intermediate care units who did and did not have an unplanned ICU transfer within 12, 12-48, or ⩾48 hours from admission.
Methods:
Population cohorts were matched on age, sex, admitting unit type, admission type, and admission acuity. Multivariable regression analysis was used to estimate the impact of unplanned transfer on mortality and LOS. Sensitivity sub-analyses compared direct ICU admissions to unplanned ICU transfers using the same transfer timeframes and endpoints.
Results:
Patients with unplanned transfers in each of three timeframes had statistically higher mortality rates and longer LOS than matched cohorts without unplanned transfer. Differences between cohorts was greatest in patients transferring ⩾48 hours post-admission for both mortality (25.1% vs 1.9%, P < .0001) and LOS (x¯ = 14.7 vs 5.3, P < .0001). Multivariate analysis showed unplanned ICU transfer significantly increased odds of mortality and prolonged LOS, with later transfers having the most profound influence (19-fold increase in mortality and 2-fold increase in LOS). Sensitivity analyses found a statistically significant increase in mortality and LOS associated with unplanned ICU transfer across all three timeframes.
Conclusion:
The association of later transfers with elevated mortality and LOS underscores the importance of timely intervention on patient deterioration.
Keywords
Introduction
Hospital measurement programs have for long placed an emphasis on cost and quality metrics. In particular, the Triple Aim established goals that encompassed quality and cost measures along with overall population health which encouraged healthcare organizations to take more deliberate actions to provide both high quality and cost-effective care.1,2 More recently, CMS demonstrated its commitment to these goals by incorporating quality-associated measures into public reporting and value based programs.3,4 Two of the most important measures targeted by hospital programs are inpatient mortality and inpatient length of stay (LOS) which reflects the time elapsed between a patient’s hospital admission and discharge.
In many instances, organizational efforts to improve mortality and LOS metrics focus on improving the management of inpatient complications and associated failure to rescue events.5,6 “Failure to rescue” (FTR) is the inadequate response to medical complications and deterioration resulting in a potentially preventable death, and is a function of clinical care capabilities rather than intrinsic population or patient characteristics such as diagnosis, acuity or complexity. 7 It is generally accepted that FTR, and more broadly deterioration in routine care settings, often precedes cardiac arrest, unplanned care escalations, and unexpected death, thereby contributing to excess LOS and avoidable mortality.8-11
In consequence, efforts to detect and intervene on patients who are in the early stages of deterioration is core to many quality improvement efforts. 10 In practice this can take a range of forms with an increasingly common model being to implement small groups of clinicians as Rapid Response Teams (RRTs) in routine and intermediate care settings, often operating in conjunction with early warning score technologies.9,12-14
The unplanned transfer of a patient from a lower level of care, such as routine or intermediate care to the ICU (reflecting an escalation in care intensity that is not an expected part of the patient’s care plan at the time of hospital admission) can serve as a proxy for identifying patients who have followed a trajectory of serious deterioration, in some cases due to preventable adverse events including human failures in monitoring patients.15-18 The concept of progressive clinical deterioration as an antecedent to unplanned ICU transfer 10 is reinforced by work that has demonstrated how delays in transfer to ICU from lower levels of care are associated with increased mortality rates.8,19,20 Crucially, unplanned ICU transfer events can be programmatically defined and measured using patient transfer data, allowing robust analysis of associated outcomes. For this reason unplanned transfer to ICU is a common endpoint for predictive models attempting to provide early warning of patient deterioration.18,21-26
Prior studies have found that patients with unplanned transfer to ICU have both higher mortality and longer LOS compared to similar populations of patients without time in the ICU or who were admitted directly to the ICU from the Emergency Department (ED).27,28 However, some portion of unplanned transfers may stem from issues in initial triage or bed placement rather than being the sequelae of a deterioration event,28-31 which may help explain why unplanned transfers occurring shortly after admission have a less definite impact on patient outcomes. Analysis of transfers occurring within 24 hours of presenting in the ED have been associated with higher mortality rates and longer ICU LOS but not with longer overall LOS, 32 while other work studying delays in ICU transfers directly from the ED has not found a consistent relationship with inpatient mortality risk.33,34
In this work we seek to evaluate the role of patient deterioration on mortality and LOS using unplanned transfer to ICU as a defining indicator of such deterioration. Prior work in this area either does not consider the timing of unplanned ICU escalation or else it focuses on transfers that occur within 12 or 24 hours of admission. This work presents a comparative analysis of unplanned transfers occurring within 12 hours, between 12 and 48 hours, and more than 48 hours following hospital admission. The population with an unplanned ICU transfer after more than 48 hours is of particular interest as there is a lower likelihood that the transfer is an artifact of either triage or initial placement challenges; in these later transfers there is a heightened probability that the escalation to ICU is indeed a causal result of progressive deterioration. This work aims to quantify differences in mortality and LOS between patients with later, largely deterioration-related, ICU transfers and comparable patients having earlier or no escalation to ICU.
Methods
Patient population and study design
This study comprised a quantitative retrospective analysis of patient data de-identified in accordance with 45 CFR 164.502(d) and 45 CFR 164.514(a)-(b) for patients discharged between January 1, 2022 and December 31, 2023 from 15 hospitals across five health systems in the United States. Hospitals represented different geographic regions of the United States (northeast, southeast, mid-west, and south) with diverse characteristics, ranging from a 50-bed community hospital to a 1500-bed academic medical center; all hospitals had designated ICUs.
Patient data were obtained from the electronic medical record (EMR) at each hospital, de-identified and aggregated for descriptive and statistical analyses. Hospital unit types and discharge dispositions were mapped to standardized values for analysis. Patients included in the study were 18 years of age or older at the time of hospital admission and were admitted to a routine or intermediate care unit. Patients who were missing a discharge disposition and patients without a Rothman Index (RI) score during their stay were excluded from the analysis. Additionally, patients with an overall LOS greater than 105 days (the top 1% of LOS among patients with an ICU escalation) were excluded from the analysis to reduce outlier bias. Missing data for sex, race, ethnicity and admit type were mapped to an Unknown category for reporting.
An attrition diagram describing the study population is shown in Figure 1. All patients meeting the study criteria were included in the analysis. Analysis cohorts were identified based on whether the patient had an escalation in care to the ICU during their stay. To avoid incorporation of planned post-surgical ICU transfers, any patient with a transfer to ICU from a surgery-associated location (eg, operating room or post-anesthesia care unit) was excluded. Cohorts were further segmented into escalations occurring less than 12 hours from admission, between 12 and 48 hours from admission, and more than 48 hours from admission. Analyses were conducted separately for each of these transfer groups supporting generalizability of study findings. Operationally, unplanned transfers to ICU were defined as admission to a routine or intermediate care unit that were subsequently admitted to an ICU. Unit admission and discharge was identified using Admission, Discharge and Transfer (ADT) data from the EMR.
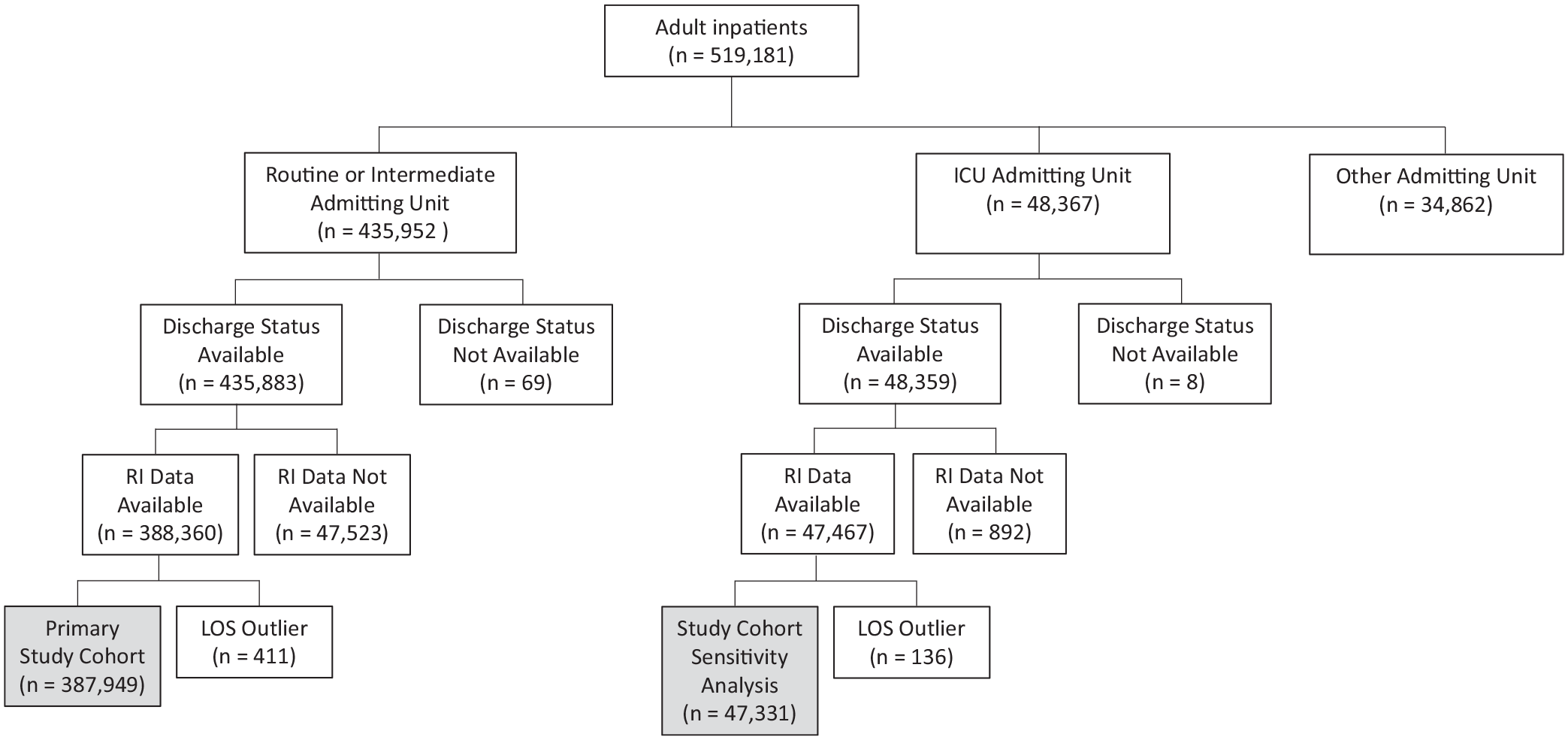
Attrition diagram.
The study protocol including ethical principles related to informed consent, permission, confidentiality and anonymity, data management and protection, and adherence to institutional guidelines related to data access and protection was reviewed and approved by Pearl IRB (Indianapolis, IN) which determined the study to be Exempt according to 45 CFR 46.104(d)(4) Secondary Research Uses of Data or Specimens (IRB ID 2024-0253).
Study outcomes
Primary outcomes of interest included inpatient mortality rate and LOS. Secondary outcomes included the rate of hospice discharge and ICU LOS. All outcomes were calculated using ADT system data from the EMR. LOS was operationally defined as the difference in days (rounded to one decimal) between patient admission and discharge from the hospital. The operational definition for ICU LOS was the difference in days between patient admission and discharge from any ICU. If a patient had multiple admissions to the ICU during their stay the ICU LOS was summed across all ICU admissions. Patients without any time in the ICU during their stay, ICU LOS was calculated as 0 days.
Statistical analysis
Propensity matching was used to balance the size and characteristics between comparison cohorts with and without ICU transfers, and to account for factors that could influence either the primary study outcomes or likelihood of ICU escalation.35-37 Logistic regression techniques were used to identify the cumulative probability of transfer to ICU using patient age and sex, admission type, admitting unit type (routine or intermediate care), and first RI during the visit (admit RI) as covariates and were conducted separately for each health system and for each population subset (ie, for transfers occurring <12, 12-48, and ⩾48 hours after admission). The RI is a machine-learning based score of patient condition that has been shown to be well-calibrated across the spectrum of patient acuity and effective at stratifying patient risk.38-42 As such, the RI has been used in multiple peer-reviewed studies to control for patient acuity across populations.41,43,44
Cases with unplanned ICU transfers were matched to controls for each health system based on these probabilities using a 1:1 Greedy matching algorithm. 45 This algorithm attempts to match cases with the highest precision match first and continues to perform matches until no additional matches are found thereby minimizing the number of incomplete and inexact matches. For this analysis, Greedy matching was restricted to propensity scores that matched to six decimal places or more to ensure a high-quality match. Since patients with an unplanned transfer occurring within 12 to 48 hours of admission have an overall LOS of at least 12 hours, patients in this control group were also required to have a minimum LOS of 12 hours. Similarly, control group patients for the cohort transferring to the ICU more than 48 hours into their stay were required to have a minimum LOS of 48 hours.
Post-match data were combined across all health systems for analysis. Study population demographics including patient characteristics (eg, sex, age, race, ethnicity), visit characteristics (eg, admit type, discharge status), and clinical features representing clinical status (eg, admit RI score), were compared across cohorts before and after the matching process to ensure that the matched sample accurately represents a balanced comparison between cohorts.
Counts and percentages were used to report and compare categorical outcomes across cohorts while mean and median values were used to compare continuous variables such as overall and ICU-specific LOS. Chi-square tests were used to analyze differences between cohorts for categorical variables. For continuous variables, ANOVA was used to analyze differences between cohorts with Kruskal–Wallis tests used for non-normal distributions.
We also sought to estimate the impact of ICU escalation on LOS and mortality using multivariable regression models. Specifically, a general linear regression model with negative binomial distribution was used for LOS and a logistic regression model for mortality. Model confounders included patient and visit characteristics as well as clinical features indicating severity of illness and physiological status.
All statistical tests were conducted using SAS version 9.4 (TS1M5 MBCS3170; SAS Institute, Cary, NC). Alpha was set at .05 for tests of significance.
Subgroup analyses
Descriptive analysis showed variation in outcomes across the different admitting unit types (Table1). Given the much higher volume of patients admitted to routine units, primary univariate analyses were stratified by admit unit type as a subgroup analysis to ensure results were consistent across both routine and intermediate care units.
Admitting unit type and transfer timing for study population.

Abbreviations: Avg, average; ICU, intensive care unit; LOS, length of stay.
Sensitivity analysis
Prior studies have evaluated quality, safety, and LOS measures associated with direct admission to the ICU from the ED.32,46-48 To mitigate potential bias, in this work we additionally conducted a sensitivity analysis to compare outcomes for patients with unplanned transfer to ICU with outcomes for patients admitted directly to ICU.
Similar to the primary analysis, propensity score matching with a 1:1 Greedy matching algorithm (requiring a match of six decimal places or more) was used to control for differences between cohorts. For this analysis matching variables included patient age and sex, type of admission, and the admit RI score. Comparative analyses included descriptive and bivariate statistics (ANOVA/Kruskal–Wallis for continuous variables and chi-square tests for categorical variables).
Results
The study population was comprised of 387 949 adult inpatients with an overall unplanned ICU transfer rate of 4.1% of which 48.8% occurred 48 hours or more after admission (Table 1). Average total hospital LOS, ICU LOS, and mortality rates were greater for patients with transfers after 48 hours compared to patients with transfers less than 48 hours following admission (Table 1).
Table 2 reports the patient demographic, visit, and clinical characteristics of the study sub-populations prior to the matching process. Patients with an ICU transfer tended to be older than those without an ICU transfer during their stay and patients with transfers later in their stay were older than patients transferred closer to the time of admission (P < .0001). Males were more likely to have an unplanned transfer to the ICU compared to females (P < .0001) across all transfer groups. ICU escalations had lower RI scores upon admission (reflecting higher physiologic acuity) compared to those who did not transfer to the ICU (P < .0001). Admitting RI scores were higher in the patients with escalations of more than 48 hours (mean RI = 62) and between 12 and 48 hours (mean RI = 59) compared to those that escalated within the first 12 hours (mean RI = 53). Admission types varied between patients who had an escalation and those who did not and differed across the admission groups (P < .0001). The proportion of patients with elective admissions was lower in patients transferring 48 hours or more after admission (8.3%) than in patients transferring to ICU in less than 12 hours (33.93%), between 12 and 48 hours (12.5%), or without an escalation to ICU (21.5%). Additionally, emergency admission rates were much lower in patients escalating to the ICU within the first 12 hours of admission.
Population characteristics.
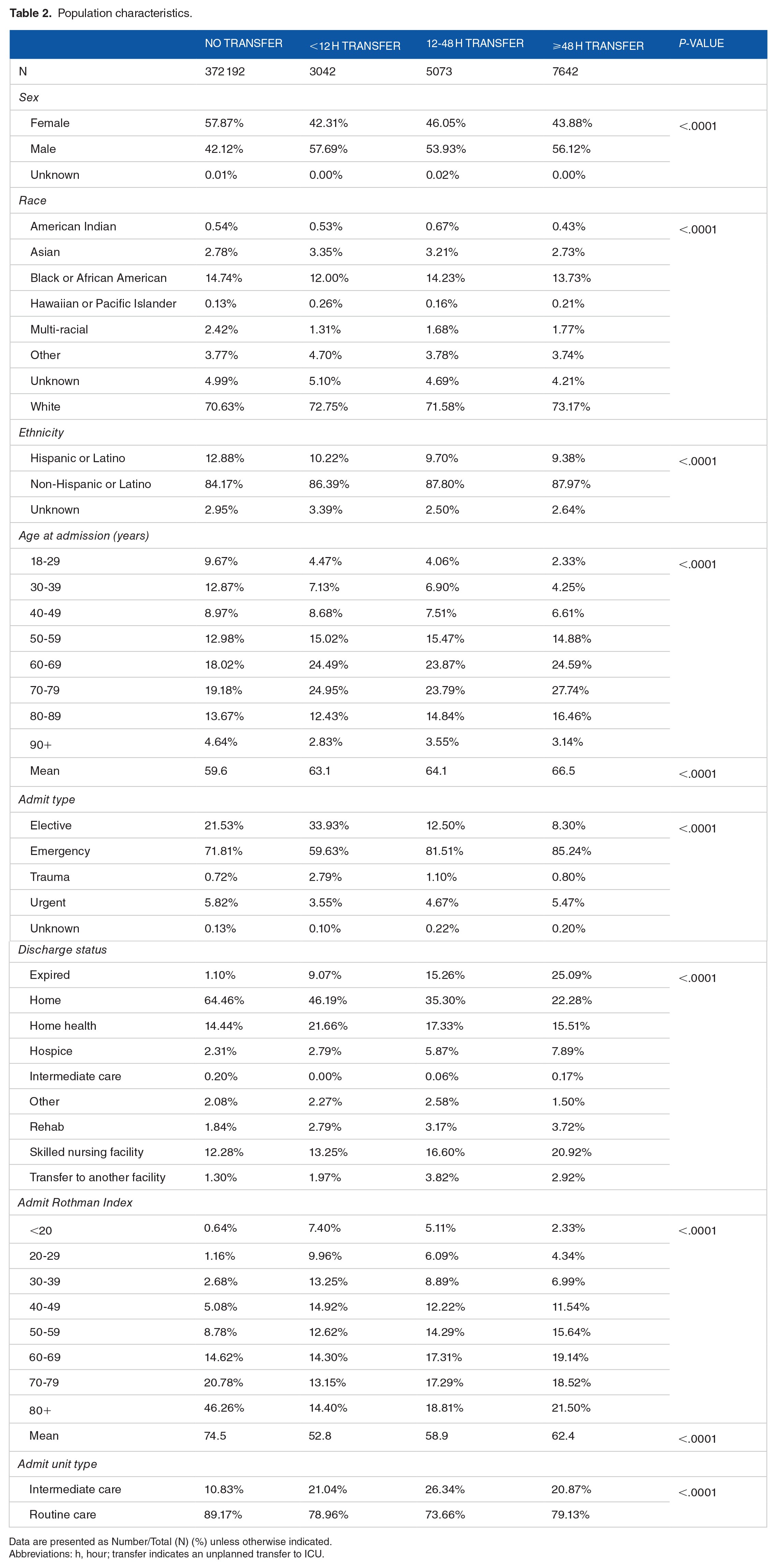
Data are presented as Number/Total (N) (%) unless otherwise indicated.
Abbreviations: h, hour; transfer indicates an unplanned transfer to ICU.
The post-match population for patients escalating to the ICU within the first 12 hours of admission included two equal groups of 2943 patients which included 96.8% of all unplanned ICU transfers. Across systems the matching rate of patients with an escalation ranged from 92.9% to 98.8%. For patients with an ICU escalation between 12 and 48 hours the overall match rate was 99.2% resulting in two equal groups of 5032 patients. Match rates ranged from 95.9% to 99.6% across health systems. Similarly, match rates were high in the patients escalating to the ICU more than 48 hours after admission. Across health systems the match rates ranged from 98.1% to 99.9% to create two equal groups of 7607 patients. There were no statistically significant differences in the matching variables of patient age or sex, admit type, admitting unit type or admitting RI score in the post-match population across all study cohorts (Supplemental Table 1).
Univariate analysis of outcomes overall and by admitting unit
As shown in Table 3, patients with an unplanned ICU escalation during their stay had a significantly higher mortality rate than those who did not. Differences between cohorts were greatest in patients transferring more than 48 hours into their stay (25.1% vs 1.9%, P < .0001) compared to those transferring 12 to 48 hours (15.3% vs 3.7%, P < .0001) and less than 12 hours (9.1% vs 5.4%, P < .0001). Rates of patients discharged to hospice were significantly lower for patients escalated within 12 hours (2.2% vs 5.2%, P < .0001) compared to those without an escalation. However, patients with an escalation 48 hours or more into the stay had higher discharge to hospice rates (7.9% vs 4.1%, P < .0001) than their counterparts without an ICU escalation.
Post-match outcomes for unplanned transfers to ICU.

Data are presented as Number/Total (N) (%) unless otherwise indicated.
Abbreviations: ICU, intensive care unit; LOS, length of stay; Transfer, unplanned transfer to the ICU.
Overall and ICU specific LOS was significantly higher for patients with an ICU escalation (Table 3). Differences in overall hospital LOS were more profound in patients with an escalation occurring 48 hours or more into the stay (x¯ = 14.7 vs 5.3, P < .0001) and occurring 12 to 48 hours into the stay (x¯ = 8.0 vs 4.9, P < .0001), however differences were still significant for patients with 12 hours or less transfers (x¯ = 6.1 vs 5.1, P < .0001).
Subgroup analyses revealed that differences in mortality rates were more pronounced in patients admitted to an intermediate care unit than routine units. This difference in intermediate care admissions was most evident among patients transferring to the ICU within 12 hours of admission—these patients had a 15.7% mortality rate compared to 6.2% for those who didn’t escalate care. Routine unit escalations within 12 hours had a 7.4% mortality rate compared to 5.2% for patients without an escalation. However, in-hospital LOS differences were more evident for patients admitted to a routine unit, particularly for patients transferring 48 hours or more into their stay. In this population ICU escalations from routine care units had a median LOS of 14.9 days compared to 5.2 days for patients without an escalation. For patients with ICU escalations from an intermediate unit, escalations had a median 13.7 days LOS compared to their controls who had a 5.8 days LOS. All subgroup analysis results are provided in Table 3.
Multivariate results
In the multivariate analysis unplanned ICU escalations were associated with increased odds of mortality. Among the 12-hour escalation cohort escalations were associated with 87% increase in mortality (OR = 1.87, 95% CI = 1.51-2.31). The impact of an unplanned transfer on mortality odds increased to a 5-fold increase (OR = 5.21, 95% CI = 4.39-6.19) in the 12-48 hour cohort and a nearly 19-fold increase (OR = 18.97, 95% CI = 15.91-22.62) in the 48 hour or greater cohort. Admission to an intermediate care unit was associated with a 31% increase in mortality odds (OR = 1.31, 95% CI = 1.03-1.66) in the 12-hour escalation cohort. Admission unit type was not significantly associated with mortality in the 12-48-hour or greater than 48-hour analysis cohorts. Compared to males, females in the greater than 48-hour cohort had higher odds of mortality (OR = 1.14, 95% CI = 1.02-1.26). All odds ratios are shown in Table 4. Note to address model convergence issues visits with Unknown admission types were excluded from this analysis and patients with Hawaiian or Pacific Islander race were combined with the Other race category.
Logistic regression estimating in-hospital mortality.

Abbreviations: RI, Rothman Index; Transfer, unplanned transfer to the ICU.
Patients with an unplanned ICU escalation were predicted to have a 21% longer LOS for escalations occurring in the first 12 hours (IRR = 1.21, 95% CI = 1.16-1.26), a 58% longer LOS for escalations occurring 12-48 hours (IRR = 1.58, 95% CI = 1.53-1.63), and more than a 2-fold increase (IRR = 2.54, 95% CI = 2.48-2.60) for escalations occurring after 48 hours of admission. Consistent across all three cohorts, increased patient acuity at admission, as measured by the RI, was associated with a longer LOS. In terms of patient demographics, females were predicted to have a 4-5% shorter average LOS than males across all three cohorts. Black or African American patients were predicted to have longer average LOS for the greater than 48 hour (IRR = 1.16, 95% CI = 1.12-1.20), 12-48 hour (IRR = 1.15, 95% CI = 1.10-1.20) and less than 12 hour (IRR = 1.11, 95% CI = 1.04-1.18) cohorts compared to White patients. Incident rate ratios for LOS analyses are shown in Table 5.
Negative binomial regression model estimating overall and ICU length of stay.

Abbreviations: ICU, intensive care unit; IRR, incidence rate ratio; LOS, length of stay; RI, Rothman Index; Transfer, unplanned transfer to the ICU.
Bold represents statistically significant at P < .05.
Sensitivity analysis comparing ICU transfers to direct ICU admits
The sensitivity analysis included 15 757 patients admitted to a routine or intermediate care unit who had an unplanned ICU escalation during their stay and 47 331 patients directly admitted to the ICU. Matching rates for patients escalated to the ICU ranged from 96.7% to 98.7% across the three analysis cohorts. There were no statistically significant differences in patient age or sex, admit type, or admitting RI score in the post-match population in any of the post-match cohorts. Supplemental Tables 2 and 3 report the patient demographic, visit, and clinical characteristics of the study population prior to and after the matching process.
Table 6 shows the post-match univariate comparisons between cohorts for the sensitivity analysis. Mortality rates were significantly higher for patients escalating to the ICU in the 12-48 hour (15.3% vs 7.6%, P < .0001) and greater than 48 hour (25.1% vs 5.1%, P < .0001) cohorts compared to patients who were directly admitted to the ICU. No significant differences were found in mortality between direct ICU admissions and those admitted to a lower level of care and escalated to the ICU within 12 hours. Median LOS was higher in patients with care escalations across all cohorts. However, these differences were more pronounced in patients with escalations occurring later in their stay. Specifically, patients escalating 48 hours or more had 8.9 day longer median LOS (14.7 vs 5.8 days, P < .0001) compared to their direct ICU admit controls, while patients escalating to the ICU within 12 hours had a 0.8 day longer median LOS (6.1 vs 5.3 days, P < .0001).
Post-match outcomes for ICU transfers compared to direct ICU admissions.
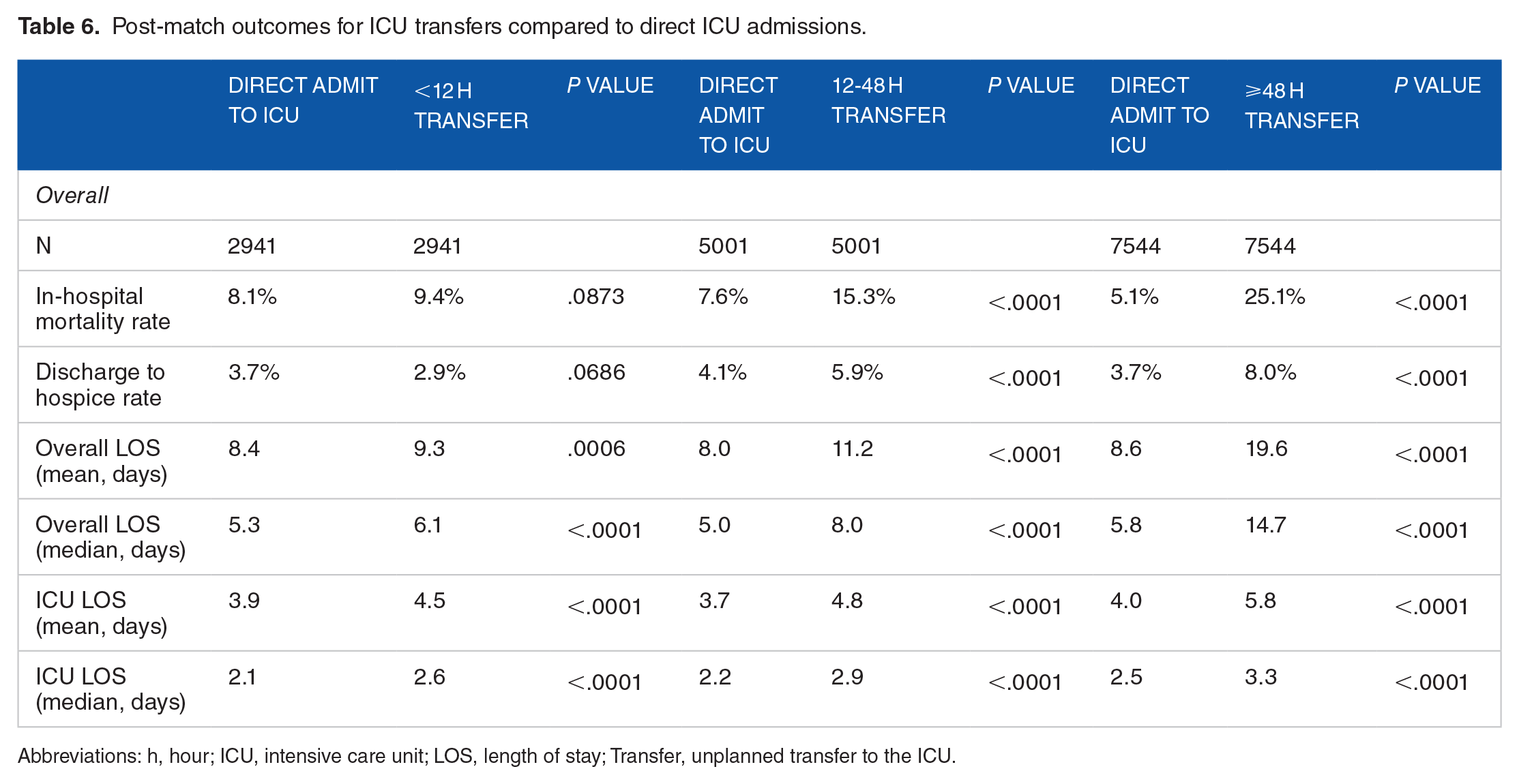
Abbreviations: h, hour; ICU, intensive care unit; LOS, length of stay; Transfer, unplanned transfer to the ICU.
Discussion
Quantifying the success of programs aimed at identifying and intervening on deteriorating patients in terms of reductions in avoidable mortality and LOS is not straightforward. Causal interplay between mortality and LOS can be hard to disentangle and some organizations perform well in one area and poorly in the other.6,49,50 Raw mortality rates do not distinguish avoidable mortality or FTR events, and LOS may vary by condition or complication. Further complicating matters is the lack of a consensus definition of deterioration (much less a definitive measure of potentially preventable deterioration) that can be used to assess the prevalence of serious deterioration events. 5
Impact of transfer timing on mortality and LOS
Our analysis shows a large and significant increase in mortality rates and LOS associated with patients who experience an unplanned ICU transfer, whether occurring shortly after admission (within 12 hours), within 12-48 hours following admission, or anytime thereafter. Our findings lend credence to the common-sense notion that an inability to identify or mitigate patient deterioration before it has seriously progressed increases the risk of adverse outcomes. While our findings corroborate previous work 27 showing that unplanned ICU transfers within 12 or 24 hours of admission are associated with higher mortality and longer LOS, we additionally find that unplanned transfers occurring more than 48 hours into the patient stay are associated with meaningfully worse outcomes than unplanned transfers occurring earlier in the stay. This is particularly important given that approximately half of all unplanned transfers in our dataset occurred more than 48 hours into the patient’s hospitalization; a finding consistent with other work in this area. 28 We surmise that these later transfers have a high probability of arising from serious progressive deterioration as opposed to being a function of incorrect triage or initial bed placement challenges, both of which are more likely to drive ICU transfer events earlier in the patient stay. This is further supported by the finding that patients with ICU transfers more than 48 hours into their stay have substantially higher RI acuity scores on admission than patients with ICU transfers in the first 12 hours post-admission, suggesting that these later transfer cases were not misplaced at admission but progressed from comparatively low acuity to critical acuity in the course of their stay.
The significantly greater mortality and LOS seen among patients with unplanned transfers occurring more than 48 hours post-admission may reflect both the sequelae of serious deterioration but also, in some instances, the results of serious deterioration exacerbated by a delay in recognition or response. Unfortunately, in this work it is not possible to ascertain the timeliness of ICU transfers. We cannot distinguish transfers that occurred promptly upon the earliest signs of serious deterioration from those that followed significant delays in the identification of deterioration, or that followed a period of unsuccessful interventional activity. Nor can this analysis account for delays due to the lack of bed availability. Numerous prior studies have evaluated the operational obstacles and inefficiencies that cause delays in escalation from inpatient units to the ICU and found worse outcomes associated with these delays, including higher mortality rates and longer LOS.8,20,51-53 Thus, the larger impact on LOS and mortality associated with unplanned transfers more than 48 hours following admission may be a function of both the proportion of transfers arising from post-admission deterioration as well as potentially greater delays in addressing such deterioration, as earlier transfers impose an upper bound on delays in escalation of care (ie, transfers within 12 hours of admission cannot have been delayed by more than 12 hours).
In the matched cohort analysis of patients with unplanned transfers to patients with direct admission to ICU, we see that in the <12 hour timeframe there is no significant difference in rates of mortality and hospice discharge, which stands in contrast to the latter two escalation timeframes. The lack of mortality differences between direct ICU admits and early unplanned transfers supports the thesis that many unplanned transfers in the first 12 hours post-admission reflect patients who should have been admitted directly to ICU, or alternatively, reflects care escalations occurring with minimal delay following the onset of deterioration.
Influence of demographic characteristics
We found it interesting to consider the findings in terms of different patient characteristics. While we matched our analysis cohorts on several health equity dimensions, including sex and age, we had insufficient patient volume to match across race categories. However, we see that the proportion of patients in each race category is comparable between each set of matched cohorts and similar to the proportions reported in the raw pre-matched populations. Notably, regression analyses revealed a statistically significant increase in hospital LOS among Black patients relative to White patients over all three escalation timeframes. This raises interesting questions about potential disparities with respect to care plans and discharge management in this population.
Pre-match data indicates that across all timeframes analyzed proportionally more males had unplanned transfers than females. Similarly, being female served as a protective advantage in the LOS regression analysis across all timeframes but resulted in higher risk for mortality in the patient cohort matched for 48 hour or later transfers. This finding may be an artifact of including labor and delivery patients in the study dataset since these patients are not intrinsically medically compromised and are less likely to have unplanned ICU transfers or protracted hospital stays relative to patients who are admitted for pathological reasons. Without further analysis we can only speculate if there might also be social-factor considerations influencing this difference.
Not surprisingly, we see from the regression analysis a consistent increase in mortality risk for higher age groups within each analysis time frame. However, we also note a tendency for age greater than 90 to imply a statistically significant reduction in LOS across all three transfer timeframes; an anomaly we attribute to goals of care in this much older population reducing the probability of ICU treatment.
Influence of patient acuity
Regression analyses show that mortality risk increases monotonically for patients with lower admitting RI scores for each of the three time frames, consistent with other research comparing RI to mortality risk.54,55 We also see that the importance of the admitting RI acuity score to mortality risk is greater in the populations transferring closer to admission than in the patient transferring after more than 48 hours. This observation is complicated by the fact that the higher mortality risk associated with lower admit RI scores will result in population attrition altering the composition of the population remaining eligible for analysis more than 48 hours after admission. In contrast, the consistent decrease in the importance of the admitting RI on LOS as the analysis timeframes are further from the point of admission is quite clear-cut.
Study strengths
Our study has a number of strengths, including a large and diverse population of patients, and multiple analytical approaches including descriptive analysis of matched cohorts and multivariate regression to confirm the impact of unplanned ICU transfer on patient mortality and LOS. The diversity of our study data and our analytical approach suggest that our findings regarding the impact of deterioration-associated unplanned transfers at hospitals can be generalized to most US hospitals. Another key component of this work is our use of the RI acuity score to ensure patients of similar physiologic acuity were matched between our study cohorts. Notwithstanding the numerous factors that influence a decision to transfer a patient to ICU, severity of patient condition is usually a core consideration. 56
Study limitations
Our study also has limitations. As previously noted, we could not evaluate the timeliness of patient transfer to the ICU, nor could we ascertain the actual motivation for each transfer, such as hospital bed capacity constraints. We also did not have diagnosis details available in our data to support matching or sub-population analysis on the basis of diagnostic groups or comorbidities. We would encourage future analyses to include risk-stratification that also incorporates the primary reason for treatment and comorbidities. Furthermore, our programmatic definition of unplanned transfer is susceptible to errors or omissions in ADT data—for example, if a patient went from an acute care floor to the operating room followed directly by a planned ICU admission, it is possible in some instances our data would not reflect the surgical procedure leading us to incorrectly classify a (potentially high risk) case as an unplanned transfer to ICU. Our data also lack indications of which patients were restricted to comfort care measures, had do-not-resuscitate orders, or other advanced directives which may have influenced their course of care and affected LOS or mortality.
As with any retrospective analysis, the potential exists for the unintentional introduction of bias through population selection or an inability to control for biasing factors. Our approach of using matched cohorts mitigates this risk but cannot eliminate it completely; in some instances propensity scoring may exacerbate underlying imbalances in the data. 57 The use of matching excludes certain observations, which may reduce the information available about the diversity within the control population. However, post hoc analyses of the full control population yielded results consistent with those presented here. The matched population was prioritized to mitigate potential selection bias and minimize the risk of overestimating the effect of the study variable in the over-represented group. Our grouping of transfer events into defined time ranges may obscure or amplify subtle differences—for example patients transferred a few minutes apart on either side of our 12 and 48 hour cut-points may be more similar than the aggregate differences between these groups suggest. However, our approach is consistent with recent prior work in this area and aids with clinical interpretability. Additionally, the study utilized a retrospective observational patient population and did not employ power analyses to determine sample size which could limit the statistical power to detect smaller effect sizes. Finally, future work may benefit from examining in greater depth additional health equity dimensions to either tease-out or rule-out potential disparities in care related to the occurrence of unplanned transfers as well as associated outcomes.
Conclusion
Although previous studies have evaluated the connection between unplanned ICU transfers and inpatient mortality and LOS, this is the first work to rigorously examine outcomes between matched cohorts of patients over multiple transfer time windows. Comparing multiple transfer windows elucidates the connection between serious clinical deterioration and escalation to ICU, especially for patients having an unplanned transfer more than 48 hours post-admission—a group that reflects around half of all unplanned ICU transfers. The substantially elevated LOS and mortality associated with unplanned ICU transfers can inform quality improvement programs tasked with improving those same measures, while new insight into outcomes based on transfer timing has a concomitant implication for how organizations understand and prioritize timely and effective intervention on deteriorating patients outside the ICU. Specifically, this work demonstrates that organizations seeking to reduce both avoidable mortality and LOS metrics would benefit by implementing programs aimed at more timely identification and pro-active management of ward-level patient deterioration.
Supplemental Material
sj-docx-1-his-10.1177_11786329241312877 – Supplemental material for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames
Supplemental material, sj-docx-1-his-10.1177_11786329241312877 for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames by Kathy W Belk, Joseph Beals and Samantha J McInnis in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241312877 – Supplemental material for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames
Supplemental material, sj-docx-2-his-10.1177_11786329241312877 for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames by Kathy W Belk, Joseph Beals and Samantha J McInnis in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329241312877 – Supplemental material for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames
Supplemental material, sj-docx-3-his-10.1177_11786329241312877 for Mortality and Length of Stay Implications of Deterioration-Associated Transfer to the Intensive Care Unit over Different Time Frames by Kathy W Belk, Joseph Beals and Samantha J McInnis in Health Services Insights
Footnotes
Acknowledgements
The authors would like to thank Peter Mallow, PhD, Chair of the Department of Health Services Administration and Director of Health Economic and Clinical Outcomes Research at Xavier University for his expertise on analytical methods as well as Michael Rothman, PhD, Advisory Data Scientist at Spacelabs Healthcare for his insightful feedback on the manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: At the time this study was conducted all authors were employees of Spacelabs Healthcare. Neither Spacelabs Healthcare nor Spacelabs Healthcare™ affiliated authors received additional funding or compensation for this study.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM is a current employee and JB and KB are past employees of Spacelabs Healthcare, the commercial entity behind the Rothman Index patient condition score which was used to control for patient acuity in this analysis.
Author Contributions
J.B. and K.B. conceived and designed the study; K.B. performed data extraction and data preparation; K.B. and S.M. conducted statistical analyses and quality assurance review; J.B., K.B. and S.M. interpreted the results and J.B. and K.B. drafted the manuscript. All authors provided feedback and approved the final manuscript.
Data Availability
Due to confidentiality and data use agreements, the datasets analyzed in the current study are not publicly available. Requests to access the datasets for bona fide research purposes should be directed to the corresponding author.
Ethics Approval
The study protocol was reviewed and approved by Pearl IRB (Indianapolis, IN) under IRB ID 2024-0253. Upon review of study materials addressing patient confidentiality, data management, access and protection, the infeasibility of obtaining patient consent as well as risks posed to the welfare and anonymity of study participants this study was determined to be Exempt according to 45 CFR 46.104(d)(4) Secondary Research Uses of Data or Specimens.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.