
Abstract
Objectives:
Residency training is important worldwide and recent studies have put more emphasis on its quality evaluation. This study aims to first explore the impact of educational backgrounds on the quality of gynecology and obstetrics (OB-GYN) standardized resident training (SRT) program in China, which may provide crucial evidence for policy considerations to improve SRT quality.
Methods:
A total of 397 OB-GYN resident graduates were enrolled in this retrospective cohort study. They were divided into three groups according to their educational background, that is Bachelor of Medicine (BM), Master of Medicine (MM), and Doctor of Medicine (DM) groups. The characteristics and the results of SRT graduation examination and annual assessment of these residents were collected and compared using one-way analysis of variance or Pearson’s chi-square test. A multivariable logistic regression analysis was performed to identify the association between sociodemographic variables and pass rates of SRT graduation examination. Besides, a subgroup analysis on training time for the DM group was performed. Strobe protocol was followed.
Results:
The residents were older in DM group than that in BM and MM groups (P < 0.001). There was significant difference of the training length and the proportion taking part in SRT graduation examination among three groups (P < 0.001). Although the written test scores of SRT graduation examination were the lowest in BM group (P = 0.015), there was no significant difference in other results among three groups. No significant variable was found associated with the pass rates of SRT examination. No significant difference was found in the subgroup analysis of DM group.
Conclusion:
Overall, the SRT quality of OB-GYN residents with different educational backgrounds was good and comparable. However, residents with BM degrees had lowest written scores and need to be strengthened during training. The training time of residents with DM degrees can be shortened according to their own conditions.
Introduction
Residency training programs are important worldwide in preparing doctors to practice in their designated specialties.1,2 Since the implementation of this program in Germany at the end of the 19th century, it has been vigorously promoted and continuously improved by the United States, and has been recognized by the medical community in the world. 3 As a main part of post-graduation medical education, studies have put more emphasis on quality assurance for both Canadian and American training programs in recent years. 4 However, there is a lack of study about the standardized resident training (SRT) quality evaluation in China, for SRT was launched in 2014 under the leadership of National Health and Family Planning Commission (NHFPC) and has been mandated nationwide since 2020.5-7 At the end of 2014, 8500 residency programs had been established in 559 hospitals enrolling 55,000 resident physicians. 8 The SRT tracks residents into 36 specialties, the quality of which may vary duo to different specialties specificity and complex medical degree system in China. 9 Because, the inconsistency of the various training tracks and teacher levels have led to uneven quality of physicians. Particularly, lower ranked hospitals and unprofessional doctors had negative effects on the forming of high quality of SRT and reliable medical system. 10 So far, there is no research on SRT quality of gynecology and obstetrics (OB-GYN) among residents with different educational backgrounds at home and abroad.
In general, China’s SRT programs were set at 3 years in length and residents had to comply with guidelines from Chinese national government issued curriculum document for each specialty in details. 11 However, the training base can adjust the specific time and content of the training for the personnel who have the corresponding professional degree in medicine and who have engaged in clinical medical work according to their clinical experience and diagnosis and treatment ability.12,13 As for China’s medical degree system, a three-level medical degree system, that is, Bachelor of Medicine (BM), Master of Medicine (MM), and Doctor of Medicine (DM), was adopted in 1981.14,15 A 7-year program which can lead to the award of the MM after successful completion of the 7-year course was adopted in 1988 but replaced by “5 + 3 model” in 2015.14,16 Besides, an 8-year program leading to the degree of DM was initiated in 2001.14,17,18 Moreover, master’s degree and doctor’s degree program both include professional degree and research degree. For example, the 7/8-year program nearly belongs to professional degree. As a result, residents with different educational backgrounds may experience different training length and arrangements. Before 2020, in Zhejiang province of China, OB-GYN residents with BM degrees and residents with MM research degrees must receive 3 years of training, while residents with MM professional degrees only need 2 years of training. However, the situation of residents with DM degrees was a little complicated: residents with DM research degrees as well as MM research degrees required 3 years of training, but residents with DM research degrees as well as MM professional degrees required 2 years of training. Besides, 8-year program residents or residents with DM professional degrees as well as MM professional degrees required only 1 year of training. From 2020, 1 year of training was cancelled, and at least 2 years of training was required, regardless of academic qualifications. Despite all that, every resident physician must demonstrate adequate competencies and pass the SRT graduation examination, before a nationally recognized certificate is issued.19,20
The assessment of SRT is divided into two parts: process assessment and graduation examination. Process assessment involves attendance, completion of training targets, annual assessment and so on. 12 SRT graduation examination is a measure of the overall effect of training and includes practical skill examination and written examination. The written examination is organized by the state uniformly, using computerized question-answering methods, focusing on the assessment of residents’ level of public basic knowledge and professional theoretical knowledge, and the practical skill examination is organized by each province.13,21 The practical skill examination in Zhejiang Province is based on the objective structured clinical examination (OSCE) pattern and includes six modules: medical data interpretation, patient interviewing (medical history taking, physical examination), medical document writing (first course of disease record, complete medical record), clinical reasoning and decision-making, basic life support skills (cardiopulmonary resuscitation, endotracheal intubation), and specialized procedure performing. Only after passing both the written and the practical skill examinations can residents get the certificate of eligibility. If a resident fails to pass one of the two examinations, the result of the passed examination will remain valid and the resident will have to pass the failed examination by a make-up examination. Moreover, if a resident fails in any one of the six practical skill modules, they will be considered to have failed in the practical skill examination. 21
To date, there are limited studies on comprehensive quality data regarding the SRT of gynecology and obstetrics (OB-GYN). This study aimed to fill this gap, by investigating differences of training performance and underlying causes of OB-GYN residents with different educational backgrounds in China. It is the first time to explore developmental trends in SRT for OB-GYN residents with different educational backgrounds. The study may provide crucial evidence to improve SRT quality for OB-GYN residents and contribute to policy considerations underpinning high quality SRT.
Materials and Methods
We conducted a retrospective study of 397 OB-GYN resident graduates in Women’s Hospital, School of Medicine, Zhejiang University between 2018 and 2022. The inclusion criteria: all the OB-GYN resident graduates who had completed SRT in Women’s Hospital, School of Medicine, Zhejiang University and taken part in SRT graduation examination between 2018 and 2022. Any residents who failed to complete SRT on time or dropped in the middle were excluded from the study. This hospital is government-accredited OB-GYN training bases and a tertiary grade-A hospital, which ranks first in Zhejiang province and ranks third to fifth in China in the field of OB-GYN. Therefore, the hospital can well afford in terms of human resources, equipment, financial support, and disease cases and guarantee the consistency and quality of the resident training programs. This study was reviewed and approved by the Institutional Review Board, Women’s Hospital, School of Medicine, Zhejiang University. It should be noted that we submitted an application for exemption from informed consent to the Ethics Committee and it was approved. Because this study did not involve biological specimens, and the research risk was not greater than the minimum risk. There were no additional adverse effects on the subjects of this study. The researchers strictly abided by the confidentiality principle. The relevant research information was only allowed to be used by the researchers/Ethics Committee, and the information of the subjects was anonymous. It was difficult to contact subjects because they had finished their SRT and most of them had left our hospitals. Strobe protocol was followed in the study. STROBE Statement was found in Supplemental Table 1.
Information was collected from the residency office including gender, age, the highest degrees (BM, MM, DM), training time, the year of taking part in SRT graduation examination, the results of SRT graduation examination of each resident. It should be noted that residents who completed SRT between 2020 and 2022 also had written test scores of SRT graduation examination and annual assessment. The annual assessment included written examination and practical skill examination. The written examination, organized by the School of Medicine of Zhejiang University, used the computer to answer questions and focused on assessing the theoretical knowledge of obstetrics and gynecology of residents. The practical skill examination of annual assessment was the same as that of SRT graduation examination, as described above. All the scores were collected for further analysis.
These residents were divided into three groups according to their educational backgrounds, that is, BM group, MM group, DM group. Continuous data of each group were presented as mean ± standard deviation if normally distributed, or as median (25th-75th percentile) if not normally distributed. The normality of distribution was tested using the Shapiro–Wilk test. Categorical data were presented as frequencies and percentages. Continuous variables were compared via a one-way analysis of variance (ANOVA), followed by LSD (Least Significant Difference) test among three groups. Count data were assessed using Pearson’s chi-square test or Fisher’s exact test when appropriate. A multivariable logistic regression analysis was performed to identify the association between sociodemographic variables and pass rates of SRT graduation examination. These variables included gender, age, education background, training time and the year of taking part in SRT graduation examination. The data were presented as odds ratios (ORs) and 95% confidence intervals (CIs). Besides, due to the longest training time span (1-3 years) only existing in the DM group, we performed a subgroup analysis for the DM group. The pass rates of SRT graduation examination (including practical skill examination, written examination and final examination) among different training time residents were compared in this group. The differences were considered statistically significant when the P-value was <0.05. Statistical analyses were conducted using IBM SPSS Statistics 23.0 software (IBM Corporation, Armonk, NY, USA).
Results
A total of 397 resident graduates were identified from 2018 to 2022. Among them, 172 residents had BM degrees, 175 residents had MM degrees and 50 residents had DM degrees. The residents were significantly older in DM group (30(28,32)) than in BM (27(26,28)) and MM (27(26,28)) groups, but no significant difference was found between BM and MM groups. Most OB-GYN residents were female and there was no statistically significant difference in the ratio of male to female residents among three groups. Following the rule above, all the undergraduate residents (100.0%) and nearly three-quarters (72.6%) of master’s degree residents in the study received a 3-year SRT, while the remaining master’s degree residents received a 2-year SRT. Most residents with DM degrees (60.0%) received a 2-year SRT, while the remainder received a 1-year SRT (20.0%) and 3-year SRT (20.0%) respectively. Therefore, there was statistically significant difference of the training length among three groups. At the same time, the proportion of residents with different degrees taking part in SRT graduation examination from 2018 to 2022 was also significantly different. The sociodemographic characteristics of these residents were summarized in Table 1.
Demographic characteristics of residents among three groups.

“a” and “b”: same superscript letters mean no significant difference was found between two groups. Different superscript letters mean significant difference was found between two groups.
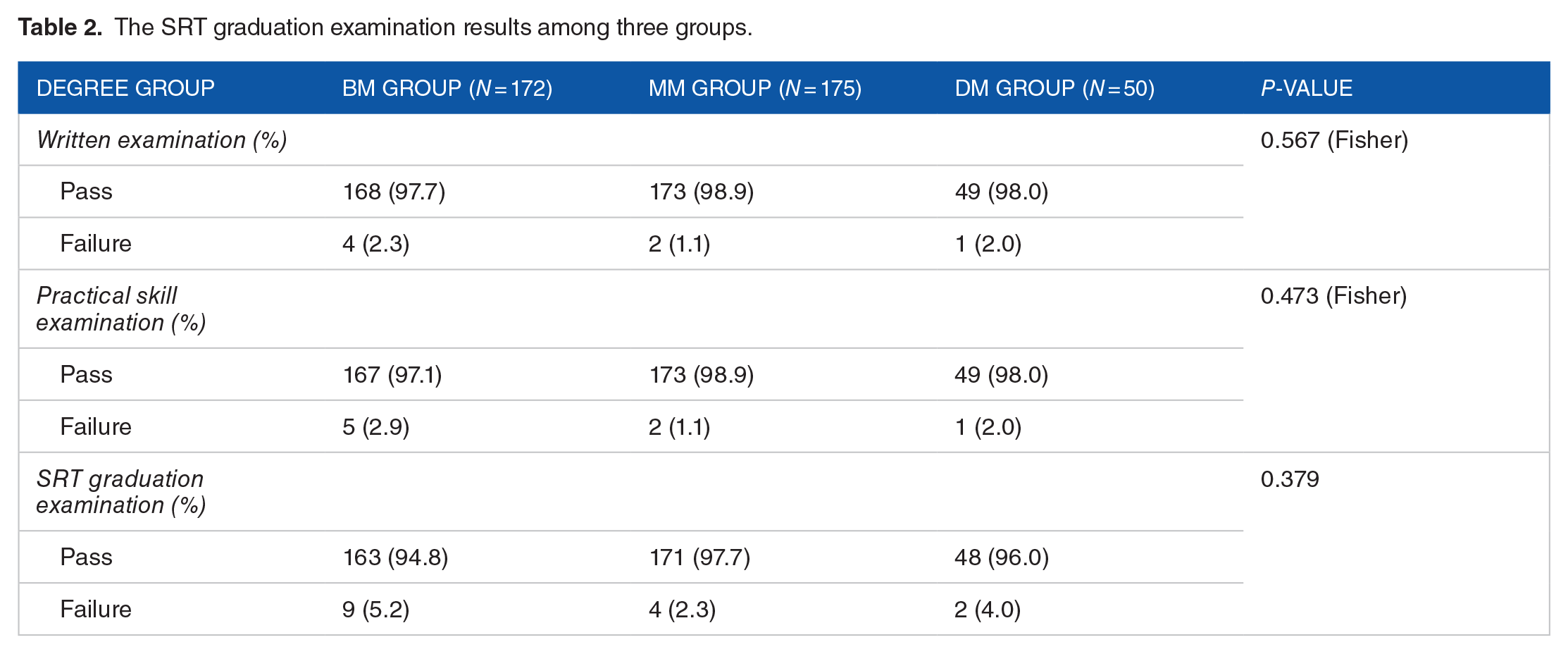
The SRT graduation examination results of all the residents were shown in Table 2. Although residents in the BM group showed raised failure rates of practical skill examination (2.9%), written examination (2.3%), and SRT graduation examination (5.2%), there was no significant difference in the pass rates of these examinations among three groups. Further analysis of written test scores of SRT graduation examination and annual assessment from 2020 to 2022 was shown in Table 3. A total of 222 residents were included during this period. Among them, 120 residents had BM degrees, 77 residents had MM degrees and 25 residents had DM degrees. The written test scores of SRT graduation examination were the lowest in BM group (P = 0.015), while no significant difference was found between MM group and DM group. Meanwhile, there was no significant difference of test scores among three groups in the practical skill examination and written examination of annual assessment. Although the excellent result (scores > 90) rate of annual assessment seemed higher in the DM group, no significant difference was found among three groups.
The SRT graduation examination results among three groups.
Written test scores of SRT graduation examination and annual assessment from 2020 to 2022.

“a” and “b”: same superscript letters mean no significant difference was found between two groups. Different superscript letters mean significant difference was found between two groups.
The results of the multivariable logistic regression analysis for the pass rates of SRT graduation examination were shown in Table 4. However, there was no significant factors associated with the pass rates of the examination in terms of gender, age, educational backgrounds, training time and the year of taking part in SRT graduation examination. The subgroup analysis results of DM group were shown in Table 5, but no significant difference was found. Surprisingly, residents with 1-year training had 100% pass rate in both the practical skill examination and written examination of SRT graduation examination. However, one resident with 2 years of training failed the written examination and one resident with 3 years of training failed the practical skill examination, therefore, the pass rate of SRT graduation examination was 96.7% and 90% respectively.
The results of the multivariable logistic regression analysis for the pass rates of SRT graduation examination.

The subgroup analysis of DM group about SRT graduation examination results among different training time.

Discussion
Limited research has focused on comprehensive quality data on residency training in OB-GYN compared to other specialties, and each of which stressed on different aspects. For example, Gothwal et al 22 and Boekhorst et al 23 evaluated how the COVID-19 pandemic affected the OB-GYN residency program in India and Europe respectively. Riedel et al 24 analyzed general and gender-dependent factors that influence the decision for or against specialty training in OB/GYN among medical students in Germany. Sami Walid and Heaton 25 investigated the share of minimal invasive surgery in the training of obstetricians and gynecologists in USA. Therefore, further research is needed on the quality of obstetrics and gynecology residency training.
To our knowledge, this is the first study to investigate the impacts of educational background on the quality of OB-GYN residency training program in China. We found that, overall, pass rates of SRT graduation examination for OB-GYN residents with different educational backgrounds were good and comparable. However, residents with BM degrees had lower SRT graduation written scores than those with MM and DM degrees. Residents with DM degrees were generally older and they had significantly different training length when compared with other residents, but further analysis of DM group found that there was no significant difference in the pass rates of SRT graduation examination among different training time.
Previous studies about relationship of educational backgrounds and SRT results focused on surgical and internal medicine residents. In a study of 1387 surgical residents in Beijing, Zhang et al 26 found that residents with MM and DM degrees had significantly higher SRT pass rates than that with BM degrees, while there was no significant difference between MM and DM degree residents. Their findings were similar to ours, namely that residents with BM degrees had relatively poor SRT examination results, which both remind administrators and clinical faculty to pay more attention the quality of SRT in undergraduate residents. However, in another study of 303 internal medicine residents in Shanghai, Yin et al 27 found that SRT pass rates and practical skill scores were lower in residents with DM degrees than those with BM and MM degrees. Their results were completely contrary to our and Zhang’s study. The above conflicting data might be caused by variations in terms of study design, specialties, gender ratio, educational backgrounds and mode of SRT. For example, OB-GYN compared to these surgical and internal medicine specialties, has the highest percentage of women trainees and active physicians. 28 Previous study had revealed that the “female factor” significantly decreased the self-confidence of practical and surgical skills among OBGYN residents, 29 which would have impact on the different outcomes of SRT among different studies.
China has developed unique and well-structured medical education system. For residents with BM degrees, they only completed 5-year clinical medical major program before SRT, which is the basis of clinical medicine education. The clinical medical major program includes theoretical knowledge of internal medicine, surgery, obstetrics and gynecology, pediatrics, and basic medicine such as anatomy, histology, etc. The training plan includes basic and clinical medicine courses and internships. 14 For residents with MM and DM degrees, they should complete postgraduate education after undergraduate education in China, which includes postgraduate courses, standardized residency, general practitioner training, specialist training or research training according to different types of postgraduate programs. 19 The postgraduate courses cover a variety of subject areas, mainly dividing into two parts: basic medicine and clinical medicine, for example, topics in pathophysiology, topics in endocrine and metabolic diseases, topics in OB-GYN, etc. They have a greater depth and breadth of knowledge than undergraduate courses, which includes the latest literatures and the most advanced researches. Therefore, on one hand, residents with BM degrees were generally younger than those with MM and DM degrees, on the other hand, they may not obtain sufficient scientific and clinical training compared with those with MM and DM degrees. Moreover, residents with MM and DM degrees can receive scientific guidance and empirical knowledge from their supervisors more or less, which all contribute to better SRT results compared with residents with BM degrees. Thus, administrators, educational leaders, and clinical faculty should pay more attention to SRT quality of residents with BM degrees, for example, holding more academic lectures and increasing one-to-one support activities by teachers. These measures would improve their ability to adequately perform with solid theoretical knowledge, which can be incorporated into their future practice. This would also contribute to an increase in the residents’ confidence and capability in performing gynecology surgeries, leading to enhanced quality of patient care. 30
It is worth noting that the subgroup analysis results of DM group showed no significant difference among different years of training. This finding may promote us to consider whether every resident with DM degree needs at least 2 years of training, especially for 8-year program residents or residents with DM professional degrees. These medical education programs vary but mainly include basic science and medical education together with scientific research training. 17 During the years of pursing their degrees, they had conducted in-depth research on certain diseases of OB-GYN and accumulated some clinical experience. Even if after graduation, they still face high demands of academic research besides clinical training, such as publishing articles in English journals with a high impact factor or applying for grant program. 31 It is hard to balance clinical training and academic research. 32 From this respect, it is necessary to reduce their training time as much as possible. Recently, most objectives of Council on Resident Education in Obstetrics and Gynecology have attempted to address some of these realities by identifying core topics that all practitioners should know and emphasizing critical thinking more than memorization. 33 Therefore, for doctoral residents, administrators and clinical faculty should fully assess their work skills and abilities before they participate in SRT, and if some of them have had solid medical knowledge and clinical practice skills, they could enter clinical practice directly or only need 1-year training after completing their education. In this way, doctoral residents can become independent obstetricians and gynecologists in the shortest possible time.
Limitations
Although our study addresses an area of research with limited data, it has several limitations. First, only one institution with limited sample size was included in the study, which may be underpowered to identify potential significant differences. Due to a retrospective study, we did not perform the calculation and justification of the sample size selected in this study, so the selection bias inherent in the design of this study was unavoidable. Second, the study only analyzed the impact of educational backgrounds on the pass rates of SRT examination and scores of the written examinations as well as annual assessment. It did not analyze the impact of other factors such as training time and the year of taking part in SRT examination on the examination results. Nor did it compare the performances of the different modules of the practical skill examination. Third, some studies have shown that marital status has a significant impact on resident performance.34-36 However, this study did not include marital status as an independent variable due to personal privacy. Finally, the representativeness of the data was not enough, which limited the generalizability of our results. After all, the scale of the training programs and the number of residencies is huge and the level of training quality is mal-distributed and imbalanced in China. Meanwhile, the results of this study cannot be compared internationally due to the differences in the contents and forms of residency training programs in different countries. 21 Therefore, further study at multiple institutions with variations in geographic distribution, sample sizes, and characteristics of the SRT programs is necessary.
Conclusion
On the whole, the SRT quality of OB-GYN residents with different educational backgrounds in China was good and comparable. However, residents with BM degrees had lowest SRT graduation written scores and their medical knowledge needs to be strengthened during training. Meanwhile, the training time of residents with DM degrees can be shortened according to their clinical practice skills and abilities. Our findings may provide a theoretical basis for administrators, educators, and clinical faculty members to develop advanced teaching and evaluation methods for OB-GYN SRT residents with different educational backgrounds.
Supplemental Material
sj-docx-1-his-10.1177_11786329241306392 – Supplemental material for Impact of Educational Background on the Quality of Standardized Residency Training Program: The Case of China, a Cohort Study
Supplemental material, sj-docx-1-his-10.1177_11786329241306392 for Impact of Educational Background on the Quality of Standardized Residency Training Program: The Case of China, a Cohort Study by Xiaoyu Tu, Xiaoquan Ding, Wanru Huang, Xiangrong Xu, Paulo Moreira and Runju Zhang in Health Services Insights
Footnotes
Acknowledgements
We gratefully acknowledge the staff of the department of Gynecology and Obstetrics Women’s Hospital, School of Medicine, Zhejiang University for their support.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Nature Science Foundation of China (No. 82001626).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
XT was involved in the design of the study and performed data analysis, interpretation and manuscript drafting. DX contributed to data analysis, manuscript drafting and editing. HW were responsible for data collection and checking. XX, PM and RZ was involved in the design, supervised the data analysis, and revised the manuscript. All authors read and approved the final manuscript.
Ethics Statement
The study was reviewed and approved by the Ethics Committee of Women’s Hospital of Zhejiang University (reference: IRB-20240231-R).
Data Availability Statement
Data are available upon justified request to the correspondence author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.