
Abstract
Background:
Assessing the financial burden of COVID-19 is important for planning health services and resource allocation to inform future pandemic response.
Objectives:
This study examines the changing dynamics in healthcare utilization patterns and costs from a public healthcare perspective during the COVID-19 pandemic in Alberta, Canada.
Design:
Population-based descriptive study.
Methods:
All adult patients over the age of 18 years who had a laboratory-confirmed COVID-19 diagnosis in Alberta, Canada from March 1, 2020 to December 15, 2021. We described demographic information and community- and hospital-based healthcare utilization and costs. We compared changes in each outcome throughout the first four waves of the pandemic.
Results:
Among 255,037 patients, hospitalization incurred significantly higher costs (N = 20,603; aRR = 755.51; marginal cost: $21,738.17 CAD; P < .01). Wave 2 recorded the highest cost for Emergency Department (ED) visits (aRR = 1.10; marginal cost: $79.19 CAD; P < .01). Compared to Wave 1, Waves 2-4 all recorded significantly lower costs for out-patient visits. Wave 2’s in-patient cost for patients that required ICU admission was significantly lower than Wave 1 (aRR = 0.75; marginal cost: −$24,142.47 CAD; P = .02).
Conclusion:
COVID-19 exerted a heavy toll on healthcare services, and the dynamics of this continue to evolve. Utilization of ED and in-patient services were particularly high. Severe infections requiring hospitalization and ICU admission are more expensive than non-hospitalized and non-ICU hospital admits. Future studies should clarify specific factors, such as sociodemographic determinants, that contribute to evolving patterns of health services consumption and changing trends in cost to holistically inform responses to future pandemics.
Introduction
The COVID-19 pandemic has imposed an unprecedented pressure on healthcare systems worldwide. Treatment costs vary between $15,750 CAD to $22,010 CAD for hospitalizations and up to $65,828 CAD for ICU stays. 1 Most of these expenditures originate from ancillary costs and treatment fees, but higher direct medical costs have been observed for up to 6 months post-infection as a result of re-hospitalizations and complications.2-6
Alberta’s public healthcare system faces severe challenges around access to primary care services and has the highest cost per inpatient case among all Canadian provinces.7,8 Examining how this system responds to a pandemic generates insights to assist other similar systems respond to and plan for future pandemics. Our results are relevant to health systems facing similar challenges around access and reach.
Currently, published reports on HCU and costs during COVID-19 vary widely between studies, and often hospital charges instead of costs are used. Using population-based data across the entire province, our study investigates the following question: what were the costs of hospitalization and outpatient visits associated with COVID-19 during the first four waves of the pandemic in Alberta, Canada? Understanding HCU patterns and costs specific to COVID-19 and how these parameters changed as the pandemic evolved is important for healthcare providers, insurance payers, and hospital systems. Our results provide regional data to inform future COVID-19 analyses.
Literature review
Most studies noted a drop in HCU during COVID-19, especially immediately after the onset of the pandemic. In South Korea, pediatric services recorded nearly 43% decrease in service utilization while outpatient services saw 15.75% drop in monthly volume and inpatient services saw a 11.6% decline. 9 Across the U.S., all-cause medical care visits demonstrated a steep decline particularly in outpatient and homecare settings; conversely, inpatient spendings increased. 10 Sweden similarly observed a decline in utilization of primary care services. 11 In Peru, among patients with chronic diseases or infectious diseases other than COVID-19, there was also a decline in HCU, with the most significant decline observed among those with uncomplicated diabetes and chronic lung conditions. 12 Furthermore, the pandemic resulted in a decrease in utilization of maternal and child health services at a regional hospital in Kenya. 13
Among patients with Type 2 Diabetes Mellitus, there was a drop in HCU of routine medical services but simultaneously an increase in telemedicine utilization. 14 In Canada, Zeitouny et al. 15 focused on British Columbia and Ontario, noting the largest decline in HCU in the first week of the pandemic and among ED visits. To et al. 16 found that among Canadian children with asthma, the pandemic was associated with a significant decrease in the number of physician visits and hospitalizations as well as significant decreases in asthma prescriptions. Another population-based study from Alberta found that the pandemic lead to a significant drop in the number of ED admissions for surgical and medical reasons. 17 This study focused on the number of admissions through the ED; our present study differs from this by broadening the scope of analysis to consider costs and HCU for a community-based, ED, and in-hospital service consumption during COVID-19.
Thus far, globally and in Canada, most studies looking at HCU during COVID19 have focused on one specialty (ex. cardiology, mental health, or emergency services), illness, or population. Our study will fill this gap in literature by adding data that showcase how the entire adult population consumed community- and hospital-based medical services during the pandemic in Alberta, Canada.
Methods
This study was a population-based study and used secondary data collected from 110 healthcare facilities in Alberta, Canada. Outcome of interest include demographic as well as HCU and cost data (Supplementary material Figure 1). In Figure 2 of our supplementary material, we outline our process for patient selection and data analysis.
Patient population
This study included adult patients 18 years and older who tested positive for COVID-19 from March 1, 2020 to December 15, 2021. During this time, Alberta’s population was approximately 4.4 million. 18 The population distribution included 19% between 0 and 14 years, 66.2% between 15 and 64 years, and 14.8% over 65 years. 18 The mean age was 39 years. 18 All eligible Albertan residents are covered by the Alberta Health Care Insurance Plan (AHCIP), covering medically-required physician services, including in-patient and ED care. 19 This means that patients are not charged directly for their care for these services.
Only the first incident cases of COVID-19 were included. To be eligible, patients must have received a positive nucleic acid amplification test (NAAT) on at least two specific genomic targets or one positive target with the nucleic acid sequencing at a provincial-level public health laboratory. Patients who had a confirmed positive COVID-19 test result via the National Microbiology Laboratory were also included. Wave 1 occurred between March to June 2020; Wave 2 between July 2020 and February 2021; Wave 3 between March 2021 and June 2021; Wave 4 between July 2021 and December 2021.
No sample size calculation was completed as this was a population-based study that used all data available from the entire population and missing data were excluded in the analysis.
Data sources
Preliminary data was gathered through the Alberta COVID-19 Analytics and Research Database (ACARD), a data collection developed by Alberta Health Services’ Data and Analytics department and the Centre for Health Informatics at the University of Calgary. ACARD includes public health, clinical, laboratory, pharmacy, administrative, and financial data. The Database has previously been used to investigate other COVID-19 related questions. 20 Patients’ personal health numbers (PHNs), birth dates, and sex were used to link data together from the following data sources:
Alberta Precision Laboratories (APL): All laboratory-confirmed positive COVID-19 test results that were reported to APL were included. The Public Health Laboratory (ProvLab), operated by APL, captures all COVID-19 lab test data in Alberta.
AHS Enterprise Data Warehouse (EDW): This study incorporated information from the Discharge Abstract Database (DAD), the National Ambulatory Care Reporting System (NACRS), Vital Statistics, the Alberta Continuing Care Information System (ACCIS), Practitioner Claims, the Paris and Meditech medical information systems and the Pharmaceutical Information Network (PIN) (Supplemental Table 1).
Patient demographics and definitions
Patients were followed for 6 months after their positive COVID-19 test for all outcomes. To ensure accuracy, patient demographics were obtained from all sources and included age deciles, sex, Elixhauser co-morbidities, long-term care status, location of test collection, and symptoms. Socioeconomic status was reported according to the Pampalon Index, which includes material deprivation (based on education, employment status, and average income) and social deprivation (based on the proportion of individuals over the age of 15 years who are living alone; who are separated, widowed, or divorced; and proportion of single-parent families). 21 The individual components within the index are derived from Canadian census data that is linkable to postal code and presented based on quintiles. The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) diagnosis codes from DAD and NACRS and ICD-9 diagnosis codes from Practitioner Claims in the 24 months before the COVID-19 test collection dates were used to clarify the Elixhauser co-morbidities. 22
Incident COVID-19 cases were matched to DAD, NACRS, and ACCIS to categorize cases as originating from hospitals, Emergency Room, or in long-term care settings, respectively. Tests that were not obtained from these contexts were classified as community cases.
New medications included all medication dispensations that occurred between −1 and 183 days after a patient’s first positive COVID-19 test were obtained from PIN. Dispensations that occurred in the 183 days prior to the test were excluded. New prescriptions were defined as the first instance of the prescription (ie, only the first dispensation of each drug was considered for the purpose of this study). Dispensations were combined if the same drug had a start date within 3 days of the expected end date of the previous prescription. PIN includes medications dispensed in the community and does not include those dispensed in hospitals. Therefore, these medication costs are not a part of the in-patient costs (ie, they are medication costs that patients pay out-of-pocket).
In-patient and out-patient (OP) costs incurred by the publicly funded healthcare system were determined by multiplying resource intensity weights in DAD and NACRs by the cost of a standard hospital stay from the Canadian Institute for Health Information.23,24 Costs of prescriptions were derived from the Alberta Drug Benefits List. 25 This is an online database that lists prescription drugs and medication products that are covered by Alberta’s government-sponsored supplemental health benefit programs. 25
Outcomes
Outcomes included number of ED visits, number of other patient services, new prescriptions, number of hospital admission, number of ICU admissions, number of days from COVID-19 diagnosis to first hospitalization, number of days to first ICU admission, and hospital length of stay for first hospitalization and for all admissions. We compared differences in community-based (ie, ED visits, OP visits, new prescriptions) costs and healthcare utilization between hospitalized versus non-hospitalized patients and temporal changes between Waves 1 to 4. Differences in hospital-based healthcare utilization and costs were compared between Waves 1 to 4.
Statistical analyses
Descriptive statistics were reported. Frequencies were used for categorical variables; means with standard deviations (SD) were calculated for normally distributed continuous variables. Where relevant, median values with interquartile ranges (IQR) were reported for skewed continuous variables.
We completed univariate and multivariate analysis to summarize healthcare utilization and costs by COVID-19 pandemic wave and by hospitalization status. Total mean costs included in-patient, OP, and ED visits and were reported for the entire cohort and separately for hospitalized versus non-hospitalized patients. Community primary provider visits and costs were excluded because they were not available at the time of data extraction. Prescription costs were reported separately as these are typically patient-borne costs and not from the healthcare payer perspective.
Generalized linear models (GLM) with a Gamma distribution and log link were used to analyze cost outcomes since these models were commonly used for skewed cost data and allowed us to include zero costs. Cost ratios and 95% confidence intervals (95% CI) were reported and average marginal costs were calculated using “R Function Margins: Marginal Effects Estimation”. 26 Poisson regression models were used to analyze the number of hospital admissions, LOS, and number of OP visits given that these outcomes were count data and Poisson regression is specifically designed for count data.
Records with missing sex and Pampalon indices were excluded from the multivariate analyses. Adjusted multivariate analysis included age, sex, LTC resident status, number of hospital admits in the previous year, Pampalon Social and Material Deprivation Indexes, number of Elixhauser comorbidities, and presence or absence of specific comorbidities.
All statistical analyses were performed in R (4.1.0.). 27 P-values < .05 were considered statistically significant. Ethics approval was obtained from the University of Calgary’s Health Research Ethics Board (REB20-0688) and has a waiver of consent. AHS data used in this study is not publicly available but may be obtained via application.
Results
During our study period, 255,037 adult patients who received a laboratory-confirmed COVID-19 test result in Alberta. After excluding those with incomplete data, 227,374 patients (89.2% of the cohort) were included in the multivariate analysis. Demographic data are outlined in Table 1.
Patient characteristics.

Community-based HCU and costs
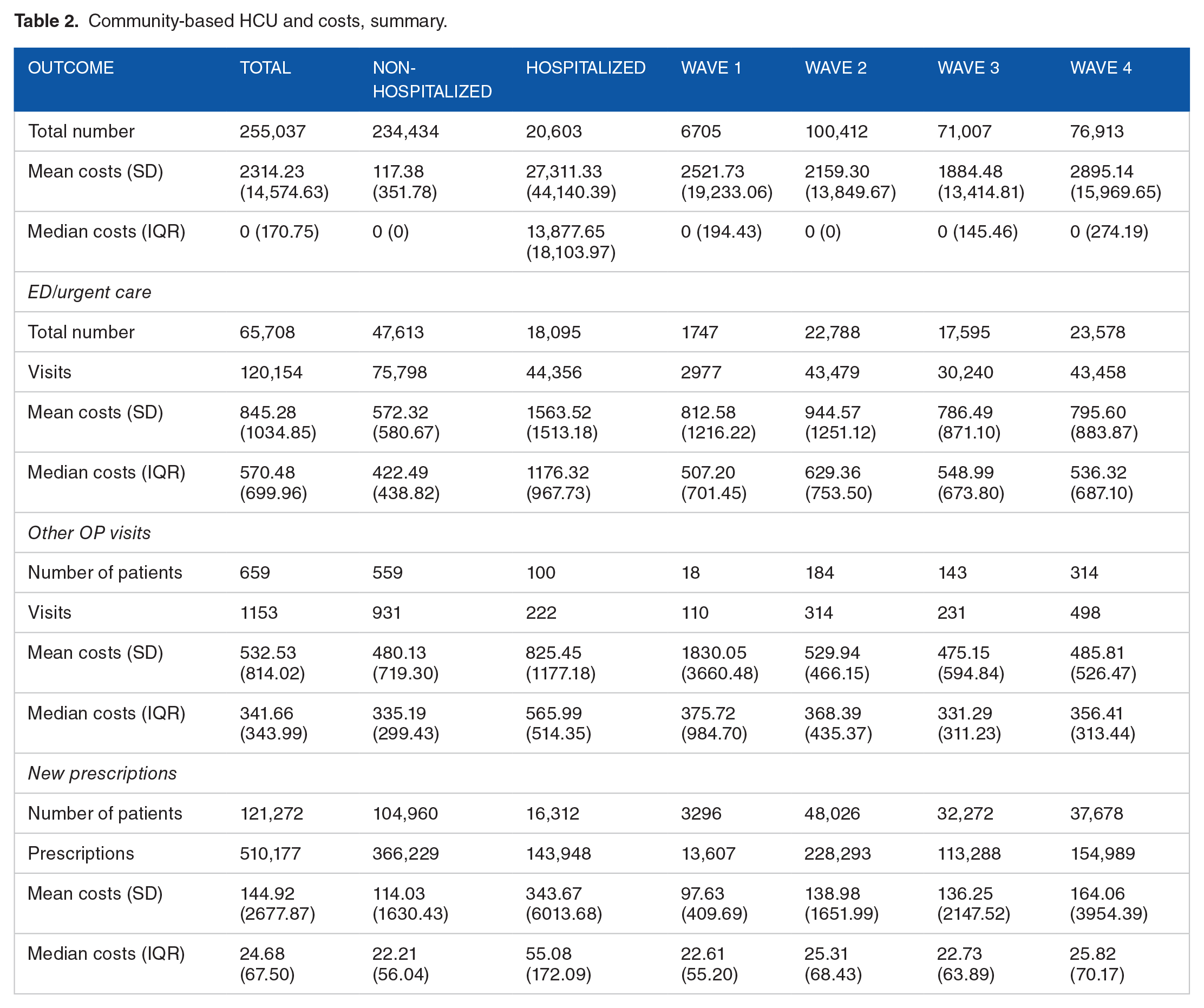
The first four waves of the pandemic recorded a total of 120,154 ED visits with an overall mean cost of $845.28 CAD (Tables 2 and 3). Wave 2 had significantly higher marginal costs for ED visits compared to Wave 1 (marginal cost: $79.19, P < .01). Similarly, Wave 3’s marginal cost was also significantly higher compared to Wave 1 but to a lesser extent than Wave 2 (marginal cost: $47.81, P = .032). Aside from urgent care service use, 659 patients recorded a total of 1,153 outpatient (OP) visits. The overall mean cost for OP visits was $532.53 CAD. Waves 2 to 4 recorded significantly fewer OP visits and lower OP costs. The marginal cost for OP visits was significantly lower in Waves 2 to 4 compared to Wave 1 (marginal cost: −$842.65, −$765.68, and −$761.1; P = .011, .033, and .03 respectively).
Community-based HCU and costs, summary.
Community-based healthcare costs changes from Wave 1 to 4.

Variables included in multivariate analysis: age, sex, LTC resident status, number of hospital admits in the previous year, Pampalon Social and Material Deprivation Indexes, number of Elixhauser comorbidities, and presence or absence of specific comorbidities.
In the community, 121,272 patients required a total of 510,177 new prescriptions. Overall mean cost associated with new prescriptions was $144.92. Compared to Wave 1, the marginal cost for new prescriptions during Wave 3 was significantly higher ($40.04, P = .047) and was the highest among Waves 2 to 4. Wave 3 incurred significantly higher new prescription costs while OP visits were significantly lower than Wave 1 with a significantly lower marginal cost of −$842.64 (P = .011). These findings may be attributable to the highly transmissible Alpha (B1.1.7) COVID-19 variant during Wave 3.28,29
Hospital-based HCU and costs
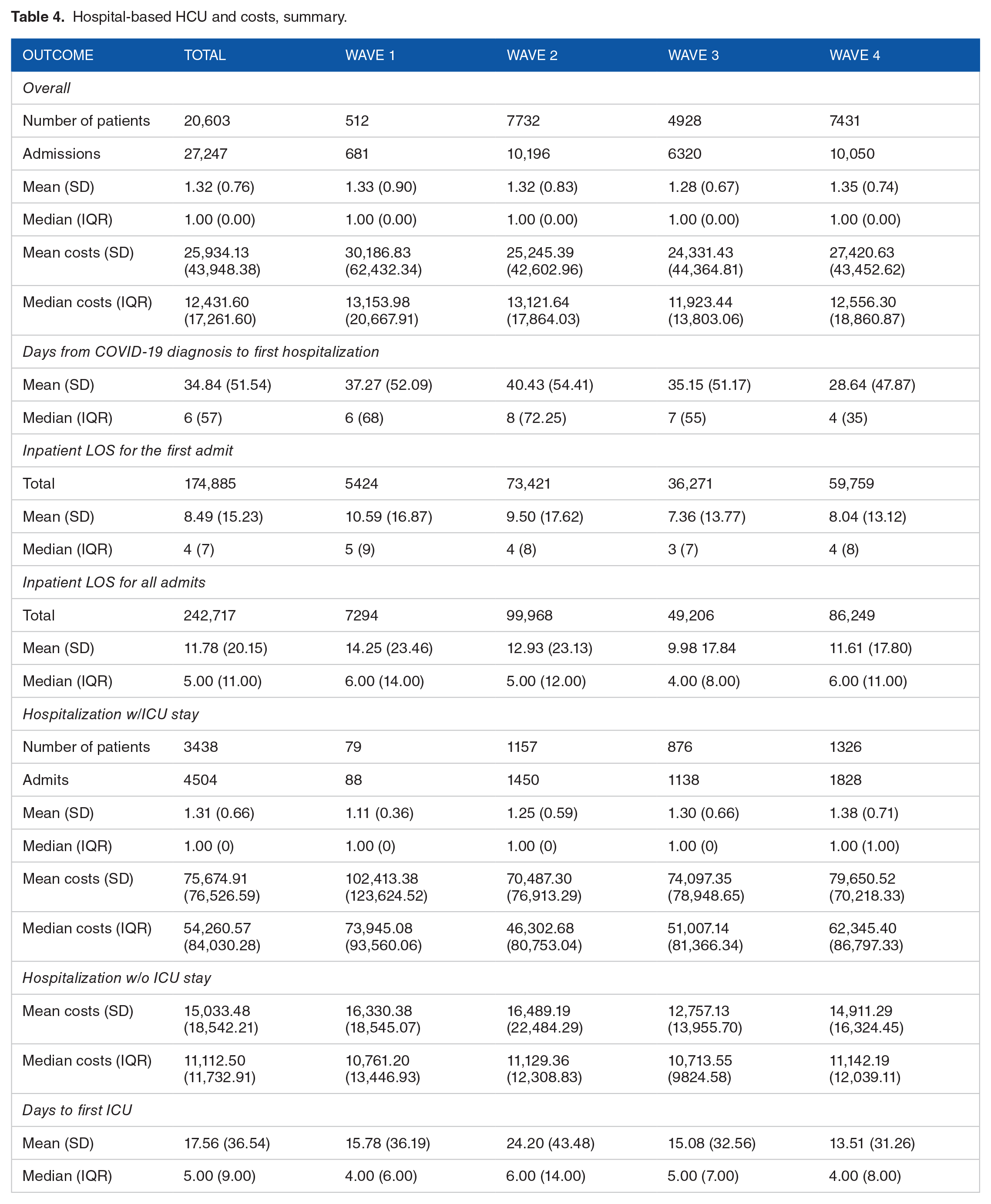
27,247 hospital admissions were recorded among 20,603 patients (Tables 4 and 5). As the pandemic progressed, the duration between COVID-19 diagnosis and first hospitalization decreased significantly. Compared to wave 1, index admission in-patient LOS was significantly lower in all succeeding waves and was lowest in Wave 3 (mean: 7 days vs 11 days; aRR = 0.70; P < .01). As the pandemic progressed, the total marginal cost for inpatient admissions decreased (marginal costs: −$6181.78, −6098.69, and −2646.53; P = .058, .064, and .445 for Waves 2 to 4 respectively) Compared to Wave 1, cost of hospitalization with ICU admission during Wave 2 was significantly lower (aRR = 0.75; marginal cost = −$24,142.47; P = .02).
Hospital-based HCU and costs, summary.
Hospital-based HCU and costs—univariate and multivariate analysis between Waves 1 to 4.

Variables included in multivariate analysis: age, sex, LTC resident status, number of hospital admits in the previous year, Pampalon Social and Material Deprivation Indexes, number of Elixhauser comorbidities, and presence or absence of specific comorbidities.
Our hospitalized cohort recorded a mean cost of $27,583.42 CAD versus $168.42 CAD for the non-hospitalized group. Internationally, the median costs for hospitalization range from $11,260 USD in Brazil to $21,752 USD in the U.S.30,31 The mean cost for hospitalizations with ICU admit was five-times higher than those without ICU admit ($75,674.91 CAD with a median of $54,260.57 CAD vs. $15,033.48 CAD with a median of $11,112.50). This aligns with data showing that ICU admission was associated with higher treatment costs for COVID-19 in Colombia, where the median cost for COVID-19 hospitalization with ICU was three-times higher than those without. 32 In Brazil, the mean cost for treating an ICU patient with COVID-19 was $17,709 USD versus $21,222 USD in the U.S.33,34 The cause for these variations is likely multifactorial. Different approaches to treatment, cost of resources, and healthcare settings are important to consider.
Discussion
We completed a population-based study to compare community versus in-patient healthcare utilization and costs among incident adult cases of COVID-19 in Alberta, Canada between March 1, 2020, and December 15, 2021, stratified by changes between consecutive “Waves” of the pandemic.
A main finding from our analysis of community-based HCU is that while consumption of OP resources and costs decreased as the pandemic progressed, pressure on EDs remained high. We observed that, in Alberta, the number of ED visits in subsequent waves of the pandemic were higher than Wave 1, peaking in the second wave. These are similar to findings from other studies that noted an initial decrease in the number of ED visits starting in March 2020.35-39 This was followed by an increase in the proportion of critical patients assessed in ED and in mortality and morbidity.40-42 During this same period, Alberta’s total number of outpatient visits significantly decreased. One contributor to this may be the severe lack of family physicians in Alberta. Between 2020 and 2023, Alberta recorded a 79% decrease in the number of family physicians accepting new patients. 43 Not having a family physician is associated with more annual ED visits and hospitalizations as well as denying patients timely access to treatment for chronic illnesses, which in turn may result in ED attendance or hospital admissions. 44 Alberta has mostly independent provider-run clinics that receive minimal resource and infrastructure support compared to acute care services. 45 There is insufficient funding to implement interdisciplinary care and limited integration with social services. 45 These factors may result in an over-reliance on hospital and EDs for health complaints that may otherwise be managed in the community. 45
In terms of inpatient outcomes, we noted that later Waves recorded shorter duration between COVID-19 diagnosis and first hospital admit, and overall LOS decreased, dropping to its shortest duration in Wave 3. Data from Ontario and Quebec during the first three Waves found that, over time, the mean hospital LOS decreased from 17 to 19 to 12 days, respectively. 46 Our data from Alberta was similar, showing a decrease from 14 to 13 to 10 days, respectively. Internationally, however, studies have generated variable results. Mexico, India, and Brazil recorded an average of 9 days, which is similar to our result, while the Republic of Korea recorded 29.4 days.30,47 The level of infection, local regulations, COVID-19 variant, and vaccination uptake and availability are all important to consider.
In Alberta, starting in March 2021, people under the age of 75 were eligible for vaccination, and by the end of June 30, all adults in the province were offered at least one dose of the COVID-19 vaccine. 48 This phased rolled-out approach is an important consideration when case numbers may not have demonstrated a notable drop, but this could be due to the fact that vaccination efforts were still ramping up and not everyone had access to a vaccine. Moreover, it is possible that vaccines that were administered were not in the same locations where COVID-19 infections were spreading the fastest. However, in general, we observed that in-patient LOS for patients’ first admission was significantly shorter as the pandemic progressed, implying that vaccination may have contributed to less severe COVID-19 infections. The marginal cost for hospitalizations with ICU admission for Wave 2 compared to Wave 1 was significantly lower. Contributing factors may include the severity of infection, treatment protocols and differential costs associated with resources used.
While our findings for in-hospital HCU and costs demonstrated variability as the pandemic progressed, our results emphasize previous international results on the financial toll of hospitalization and intensive care management of COVID-19 as well its toll on ED services.
Policy Implications
It is imperative to improve access to family physicians and support acute care services in the community. Policies that can meet this gap in demand include directing more funding and resources to hire and retain more primary care providers where there is greatest need; creating more “care networks” to boost the capacity of physicians to provide greater coverage for more patients; and expanding primary care teams to establish satellite sites in remote and rural areas. 49
Alberta covers a large geographic area with differential access to health resources in urban versus remote regions. To adequately meet a diverse set of needs, it may be worthwhile to design specific healthcare delivery plans or models of care for different areas to agilely respond to evolving needs, particularly during high-pressure periods. Also, it is important to invest in technology as well as capital and human resources for EDs to efficiently manage increased influx of patients. Findings from this study may inform a more demand-driven approach to resource allocation particularly for community health services as these HCU and cost parameters remained consistently high throughout the pandemic. HCU and costs for ED services were especially high throughout the four Waves we examined. This result emphasizes the importance of sustaining acute care services during pandemic situations.
Strategic advisories or bridging programs to strengthen the linkage between acute and primary care may be beneficial in coordinating care for complex patients. Effective local regulations around social activities and access to medications and vaccines is important to mitigate overburdening inpatient services. As we demonstrated changes in HCU and cost as a pandemic evolved, it is important that in future pandemics, there is ongoing evaluation, data monitoring, and assessment of resource consumption and costs.
Strengths and Limitations
One limitation of our study is that our analysis is limited to the first four Waves of the pandemic. This could have potentially limited our understanding of the dynamics of the pandemic over time. In addition, we were unable to obtain vaccination data and therefore could not report rates of vaccination within our study population, which could have impacted disease severity and course. Our data did not examine testing variability over time. While we reported a broad spectrum of HCU parameters, our data did not report the specific causes for these, which may be an area of interest for future studies to gain a deeper insight into the influential factors contributing to COVID-19 HCU and costs.
Moreover, since we stratified our data based on hospitalization status, we were unable to determine the temporality of events. Also, our results did not include HCU and cost data for family physician visits, which is an important outcome to evaluate. Also, we were not able to confirm whether any hospitalization after the initial COVID-19 admission was due to COVID-19 amongst our patients. Given that this was a population-based study that used administrative data, there is a possibility of human error in coding. At the same time, conducting a similar study not using administrative data would have been very costly and difficult to access the same amount of data.
Our study was population-based, including patients from across Alberta. This allowed us to consult multiple data sources. Therefore, our results are based on a comprehensive assessment and have wide geographic coverage to ensure that patients from different settings across Alberta are represented.
Conclusion
We completed a population-based analysis of COVID-19 HCU and costs in Alberta, Canada and summarized changing trends across the first four Waves of the pandemic. We noted that overall utilization of community-based health services decreased during this period while ED visits and costs remained high, underlining the pandemic’s persistent pressure on acute care services. Consistent with findings from other regions, our results demonstrate that hospitalization, especially those that required ICU admission, incurred significantly higher costs. We highlighted the importance of strengthening our primary care system to build a strong backbone for our healthcare system. Greater support and engagement between acute and primary care services prepares our health system for future challenges.
Future studies may examine sociodemographic factors that contribute to changing HCU and costs. It would also be worthwhile to contextualize HCU and cost data withing clinical outcomes to more thoroughly understand whether these parameters impact recovery and health post COVID-19.
So what?
What does this study add to existing knowledge? Among the limited number of Canada-based healthcare utilization studies on COVID-19, this study examines the overall cost and evolving trends of healthcare utilization during the pandemic to better inform policymaking and service delivery pathways. Our community-versus-hospital analysis compares healthcare utilization and cost in different settings.
What are the key implications for public health interventions, practice, or policy? This study identified that hospitalized COVID-19 patients requiring ICU admission were significantly more costly (marginal cost exceeding $20,000 CAD) and that, throughout the pandemic, urgent care remained heavily burdened while other HCU outcomes fluctuated. These results encourage more engagement with primary care providers and coordination-of-care with community-based emergency medical service providers to enhance future response to pandemics.
Supplemental Material
sj-docx-1-his-10.1177_11786329241306390 – Supplemental material for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study
Supplemental material, sj-docx-1-his-10.1177_11786329241306390 for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study by Kathy Liu, Elissa Rennert-May, Zuying Zhang, Adam G D’Souza, Alysha Crocker, Tyler Williamson, Reed Beall and Jenine Leal in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241306390 – Supplemental material for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study
Supplemental material, sj-docx-2-his-10.1177_11786329241306390 for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study by Kathy Liu, Elissa Rennert-May, Zuying Zhang, Adam G D’Souza, Alysha Crocker, Tyler Williamson, Reed Beall and Jenine Leal in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329241306390 – Supplemental material for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study
Supplemental material, sj-docx-3-his-10.1177_11786329241306390 for Evaluation of In-Hospital and Community-Based Healthcare Utilization and Costs During the Coronavirus 2019 (COVID-19) Pandemic in Alberta, Canada: A Population-Based Descriptive Study by Kathy Liu, Elissa Rennert-May, Zuying Zhang, Adam G D’Souza, Alysha Crocker, Tyler Williamson, Reed Beall and Jenine Leal in Health Services Insights
Footnotes
Acknowledgements
We wish to acknowledge Alberta Health Services for their provision of the data used for this study.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internal funding from the University of Calgary was provided to JL and ERM for this work.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Concept and design: KL, JL, ERM. Acquisition of data: AD, AC. Analysis and interpretation: ZZ, KL, JL, ERM. Drafting of the manuscript: KL. Critical revision of the paper for important intellectual content: KL, JL, ERM, AD, AC, TW, RB, ZZ. Obtaining funding: JL, ERM. Administrative, technical, or logic support: N/A. Supervision: JL, ERM.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.