
Abstract
Background:
Physician-hospital vertical integration is gaining steam but it is unclear how they affect hospital output.
Objective:
To examine the direct impact of vertical integration on hospital output.
Design:
A pooled design with 6-year data using linear regressions was used. Then, panel data design with hospital fixed effects was used.
Methods:
We linked American Hospital Association data (2016-2021) with AHRQ Comparative Health System Performance Initiative’s Compendium (2018, 2020, 2021; 34 987 hospital-year observations) to develop new measures of vertical integration and assess its relationship with several measures of hospital output including annualized total admissions, total number of inpatients days, and total number of emergency department (ED) and outpatient visits.
Results:
We find that a hospital’s entry into a vertical integration has little or no impact on a broad set of metrics capturing hospital output.
Conclusion:
Our findings suggest that vertical integrations as currently structured may not yield meaningful gains in output or productivity and hospitals faced with declining productivity need to carefully consider the expected gains from vertical integration strategies.
Introduction
Hospitals have been seeing a decline in productivity. 1 To deal with losses incurred by low productivity and depressed margins, hospitals employ different strategies including diversifying in different markets, or merging with other hospitals, or fostering closer ties with physicians. 2 Physicians have clout over resource usage, and organizational costs at hospitals. 3 As hospitals attempt to improve revenues by increasing patient occupancy and admissions, binding closely with physicians can determine where resources are diverted and how they are used. Involving physicians in decision making may lead to better operational decisions and policy shifts that can subsequently influence hospital output.
Hospital output is also understood as hospital productivity in terms of the number of patients admitted, discharged, number of outpatient visits, number of patient days, and the amount of revenue generated. 4 Hospital output has been studied in the context of inputs such as number of Full Time Equivalent (FTE) physicians, number of non-physician personnel, capital, beds, and other non-labor inputs. 5 Ample evidence exists to suggest that output of a hospital may vary based on variations in patients’ acuity and resource intensive needs.4,6 Several organizational characteristics can influence hospital output. For instance, a teaching hospital may have a higher number of FTE residents as compared to a non-teaching hospital, leading to difference in outputs between the two. 7 Ownership status determines the external environment pressure related with payment and reimbursement policies, which can also affect hospital output. 8
Direct ownership of physician’s practices by hospitals (also known as vertical integration) has gained prominence in recent years. 9 Vertical integration at hospitals is defined as the affiliation under a canopy of organizations that offer different levels of care, with the purpose of enhancing efficiency and coordination of care. 10 Vertical integration brings a unified ownership which makes organizational coordination and efficiency easier. 11 Some researchers believe vertical integration should be implemented only if these actions help in increasing revenues, improving quality and physician hospital relationships, while others have contended that the effects of regulation and physician competition have made hospital physician integration almost a necessity.3,12
Existing literature evaluating impacts of vertical integration on hospital outcomes reveals several conflicting patterns. For instance, there is evidence that vertical integration raises hospital costs by enhancing physician involvement in administrative roles, especially for non-profit hospitals. 3 Hospitals could absorb the higher costs if vertical integration helped improve patient revenues. A recent study showed that physicians’ services reimbursement from Medicare would be approximately $114 000 higher if vertical integration was present. 13 However, the same study showed that vertical integration reduced primary care physician’s clinical activity among Medicare patients and integrated physicians saw fewer patients and fewer claims were billed as a result. Studies have also shown that vertical integration is largely motivated by hospitals’ desire to integrate with physicians so that hospitals can augment their ability to contract with managed care plans. Through vertical integration, providers enable a single point of contracting to exert leverage over managed-care payers for substantial price discounts. Vertical integration’s impact on hospitals’ overall financial performance has been extensively studied and the existing literature generally shows that financial performance improves with affiliations due to integration.2,10 Since hospital output or productivity as measured by patient discharges is an important determinant of hospital operating margins, it becomes important to examine the direct impact of vertical integration on hospital output.
New Contribution
In the past, researchers studied organizational structures based on internal organizational context for instance, leadership and resource availability, but did not necessarily examine changes in organizational structure based on environmental context for example, policy changes, and how those changes impact performance.14,15 We fill this gap by examining vertical integration as a structural change and hospital output as a resulting performance. Our study adds to the existing literature on vertical integration in several ways. First, existing studies on relationship between vertical integration and output are scarce and date back to late eighties, when the organizational context differed sharply from the contemporary era and the vertical integrations were considerably less complex. Recent studies, while focusing heavily on the impacts of vertical integration on quality, output prices, and financial performance, have tended to neglect impacts on hospital output. Second, previous work, much of it based on AHA data, has tended to use simpler proxies for vertical integration, either (1) assigning binary codes to hospitals based on their entry into 1 or more of the 8 types of vertical integration or (2) present a 3 or 4-fold classification that bundles together several distinct types of integrated models into a single fully integrated organization.16,17 Such classifications do not typically rely on independent assessments of factors along which integrated organizations may potentially differ and that may have a direct bearing on how they function (eg, physician autonomy, shared financial risk, shared administrative expenses, or shared bargaining arrangements) but generally assume a crude continuum of integration that runs from less integrated for example, independent practice associations toward a fully integrated organization. 18 We believe our measure of vertical integration leverages several distinct and potentially independent aspects of integration that underlie common physician-hospital arrangements, which allows us to capture more subtle variations in the strength/intensity of integration than available in the existing literature. Finally, in assessing the effect of vertical integration on hospital output, we are better able to control for the size of overall health care system in which the integration between hospital and physicians operates, by linking our hospital data to the AHRQ Comparative Health System Performance (CHSP) Initiative’s Compendium of U.S. Health Systems.
Conceptual Framework
This study uses the conceptual lens of structural contingency theory to guide the examination of the relationship between hospital integration and hospital output. Contingency theory posits that the best way for an organization to organize itself depends on its external and internal environments. 19 Researchers have studied how organizations react to environmental uncertainty through structural changes affecting various aspects of performance. 20 An important proposition of contingency theory is that there is no one best way or approach for management to adapt to situational concerns. 19 In the context of healthcare, contingency factors may include abrupt changes in demands for healthcare services (eg, the COVID-19 pandemic), changes in healthcare policies (eg, the Affordable Care Act and Medicaid expansion), or changes in population health. Hospitals may react to above contingency factors by organizing themselves in vertically integrated structures.
Contingency theory holds that effective organizations adopt structures that fit their context better than the ones that are not as effective. 20 “Fit” usually means that the design or structure of an organization is based on distribution of resources in the environment. 17 Organizational context or environment for hospitals has shifted over the last 2 decades in several major ways that may have propelled their adoption of vertical physician hospital arrangements. First, major policy shifts such as the Affordable Care Act have introduced several incentives that promote vertical integration. 21 As private and public sector payers have been transitioning from fee for service reimbursement models to risk-based models, the distribution of resources from payers has been limited. 21 Contingency theory has also been studied in the context of leadership and management change as organizational response to changing external environments. 22 This is particularly relevant for this study because the integration of hospitals and physicians brings changes to leadership and governance with more physicians expected to be involved in the hospital management. With growing levels of vertical integration in the healthcare industry, clinician leadership has become vital for structural, financial and strategic decision making and such decisions can be fundamental to improving hospital output.23-25
An important tenet of contingency theory is that variations in organizational performance can be best explained as the byproduct of the interaction between an organization’s structure and its context. 26 In other words, as the organizational environment becomes more heterogenous, the organizational structure becomes more complex. 26 Vertical integration is done in many ways. Some types of vertical integration have hospitals and physicians more tightly coupled than others. Organizational context of hospitals can be deterministic of which type of vertical integration hospitals will adopt. Organizational adaptability enhances when the degree of environmental complexity is reflected in the structure of the organization. Relationships between structure and context are higher in high performing organizations. 26 Hospitals that have closer types of vertical integration might encounter a greater complexity in their environment than their counterparts, and thus become more adaptable to environmental changes like policy shifts, reimbursement changes, and population health needs. Hospitals with these types of vertical integration may have an impact on hospital output.
Methods
Data, population, and study sample
We linked 6 years of American Health Association data (2016-2021; containing detailed information on key aspects of hospital output and vertical integration) with 3 years of AHRQ Comparative Health System Performance (CHSP) Initiative’s Compendium of U.S. Health Systems (2018, 2020, 2021). The Compendium files identify health systems with at least one hospital and at least one group of physicians that provides comprehensive care (including primary and specialty care) who are connected with each other and with the hospital through common ownership or joint. 27 We first merged Compendium hospital linkage files with health system files for each of 3 years using a unique health system ID developed by AHRQ, and then combined 3 years of data. We subsequently merged 3 years of pooled Compendium data with 6 years of AHA hospital data using the CMS certification number (CCN), assigning Compendium 2018 data to AHA 2016-2019, 2020 to AHA 2020, and 2021 to AHA 2021. We dropped the small number of observations that were missing the CCN in AHA (n = 1747) or were not matched with the Compendium (n = 533). Our final analytic sample consisted of 34 987 hospital-year observations.
Independent variable
We developed a 4-level variable that captures increasing levels of vertical integration in 3 steps. AHA survey solicits information on the 8 types of vertical integration that each hospital currently participates in: Group practice without walls, Management Service Organization, Integrated Salary Model, Equity Model, Foundation, Independent Practice Association, Open Physician-Hospital Organization, and Closed Physician-Hospital Organization. Each hospital may participate in one or more of these vertical integrations. In the first step, we assessed the level of integration involved in each of these PHA models by scoring them on a binary scale for each of a set of 8 criteria which measure several diverse aspects of integration, including financial risk, administrative expenses, bargaining arrangements, governance, and physician autonomy. We identified these criteria from a review of literature and expert commentary on vertical integration.6,10,28,29 We used 2 alternative weighting schemes to sum weighted scores across all 8 criteria and then normalized the summary score to rank the 8 integration models in terms of increasing vertical integration. The 2 weighting schemes assigned differential weights to each of the 8 categories in a slightly different manner, with first scheme weighing all categories equally while the second scheme assigned higher weights to sharing of financial risk and joint ownership of assets, criteria that are universally regarded as indicating a deeper level of integration than other kinds of affiliations. We assigned weights to sum to 1 and estimated total scores for all 8 vertical integrations by each weighting scheme as illustrated in Supplemental Tables S1 and S2 (see formula in footnote for Supplemental Table S1).
As shown in Supplemental Tables S1 and S2, both weighting schemes generated a similar ranking of models. In the second step we used the ranking developed above to assign the 8 vertical integration models into a 3-tier classification as follows (Supplemental Figure S1): high integration category includes Management Service Organization, Integrated Salary Model, and Foundation; moderate integration category includes Group practice without walls and Equity Model; and low integration category includes Independent Practice Association, Open Physician-Hospital Organization, and Closed Physician-Hospital Organization. Finally, since each hospital may participate in vertical integrations belonging to more than 1 of these 3 categories, we developed the final vertical integration variable by using 2 alternative schemes to assign hospitals to 1 of 4 mutually exclusive groupings as described in Supplemental Table S3. We refer to these 2 versions of our final vertical integration variable as primary vertical integration variable and alternative vertical integration variable, respectively, in the remaining text. Our dataset was missing information on participation in vertical integration for 2018 so we filled the missing values for 2018 by assigning the computed 2017 values for vertical integration to the year 2018.
Dependent variable
We tested the effect of vertical integration on a diverse set of hospital output variables reflecting a broad range of hospital function. Specifically, we generated variables capturing annualized total admissions, total number of inpatients days, and total number of emergency department (ED) and outpatient visits. We also captured hospital output for patients admitted through the Medicare and Medicaid programs in the form of total annual Medicare and Medicaid discharges, total annual inpatient days for Medicare and Medicaid patients, and average annual length of stay (LOS) for Medicare and Medicaid patients, respectively. We computed LOS variables as simple ratios of total inpatient days to total discharges for Medicaid and Medicare patients.
Control variables
Hospital characteristics
We controlled for the confounding effects of a broad set of hospital-related variables including ownership types (non-profit, investor-owned, government/non-federal, and government/general), teaching status, critical access designation, system affiliation, total number of beds, and the total number of nurses, physicians, and hospitalists affiliated with the hospital.
System size
The effect of vertical integration on hospital output may be conditioned by the size of the healthcare system a particular hospital is affiliated with, making it important to control for system size in our specifications. Since AHA data does not provide reliable information on the size of the care system a particular hospital is affiliated with, we developed the system size variable by linking AHRQ Compendium data with AHA data. First, we used the Compendium data to create quartiles for each of 5 system size variables: total number of physicians, total number of group practices, total number of hospitals, total number of beds, and total number of nursing homes. We numbered top quartile as 4, second quartile as 3, third quartile as 2, and bottom quartile as 1. For each system affiliated with a hospital, we then summed the numbered quartiles for all 5 variables to generate a scale ranging from 5 to 20. Hospitals associated with systems that fell between 16 and 20 were classified as belonging to large systems, those between 11 and 15 as belonging to moderate systems, while those between 5 and 10 as belonging to small systems (see Supplemental Table S4 for more details).
Analyses
Our specifications explored whether the effects of vertical integration on hospital productivity are sensitive to specifications that sequentially introduce a series of progressively more rigorous controls for unmeasured confounding factors (ie, system size measurement, panel fixed effects, and lagged predictor variables). To do so, we first ran analysis on pooled 6-year data using linear regressions that regressed each of our 10 outcomes on our primary vertical integration variable, while assessing sensitivity of our estimates to sequential addition of facility-level controls, system-size controls, and yearly trends (using year dummies). We then controlled for hospital fixed effects by running the same regression models with panel data. These are our preferred specifications since it allows us to control for the confounding effects of time-invariant unmeasured factors that may simultaneously impact the likelihood of adopting a vertical integrated arrangement and hospital output (eg, stable but idiosyncratic aspects of hospital governance/leadership). Finally, we tested the sensitivity of our primary estimates in several ways. First, we ran panel regressions with our alternative vertical integration variable (that was estimated by weighting integration criteria differently than the primary variable). Then, we ran similar panel regressions by lagging both types of integration variable by 1 year to account for the fact that vertical integration may have delayed impacts on hospital output that may not be fully realized in the year an arrangement was adopted. However, we dropped controls for number of physicians and hospitalists in lagged regressions to avoid censoring the sample, since a significant number of observations for these 2 control variables were missing.
Results
Table 1 presents the descriptive statistics for our final analytic sample. Almost 58% of hospital-year sample observations did not enter into any type of vertical arrangement, 8% had low vertical integration, 2% had moderate integration, while nearly one-third showed a high level of vertical integration. The hospitals in our sample had on average 5903 annual admissions with 35 711.34 inpatient days, while the number of Medicare and Medicaid discharges were 2602.28 and 1304.11 respectively. About one-third of our observations were teaching hospitals, about a quarter were critical access hospitals, and nearly two-thirds had an affiliation with a hospital system. Slightly more than half of our observations belonged to non-profit hospitals while 27% were investor-owned and rest were government-owned.
Descriptive statistics of all variables (n = 34 987).

Hospitals in our sample had on average 149.59 beds, 228.23 nurses, 370.29 affiliated physicians, and 21.82 affiliated hospitalists. Our system size variable (derived from AHRQ data) assigned 38% of hospitals as unaffiliated with any system while 18% were affiliated with large, 20% with moderate, and 24% with small sized systems respectively. Since we assigned 2018 AHRQ Compendium data to 4 years of AHA data (2016-2019) to generate the system size variable, there was significant discrepancy between system affiliation variable derived from AHA (binary variable) and the AHRQ Compendium data.
Our preliminary set of results (without hospital fixed effects) are presented in first 3 columns of Table 2. Having some form of vertically integrated arrangement was associated with statistically significant changes in virtually all forms of hospital output we measured (compared to hospitals that did not report any vertical integration), although there were no clear patterns associated with increasing intensity of vertical integration. Specifically, we found that vertical integration was associated with higher admissions but lower overall inpatient days, higher ED and outpatient visits, greater number of Medicare discharges, more Medicare days but shortening of length of stay, and higher Medicaid discharges but lower number of total Medicaid inpatient days and shorter length of stays. Addition of physician and hospitalist controls and system size controls did not appreciably alter these results (column 4-9, Table 2).
Regression analysis for pooled data with and without system size controls and year dummies.
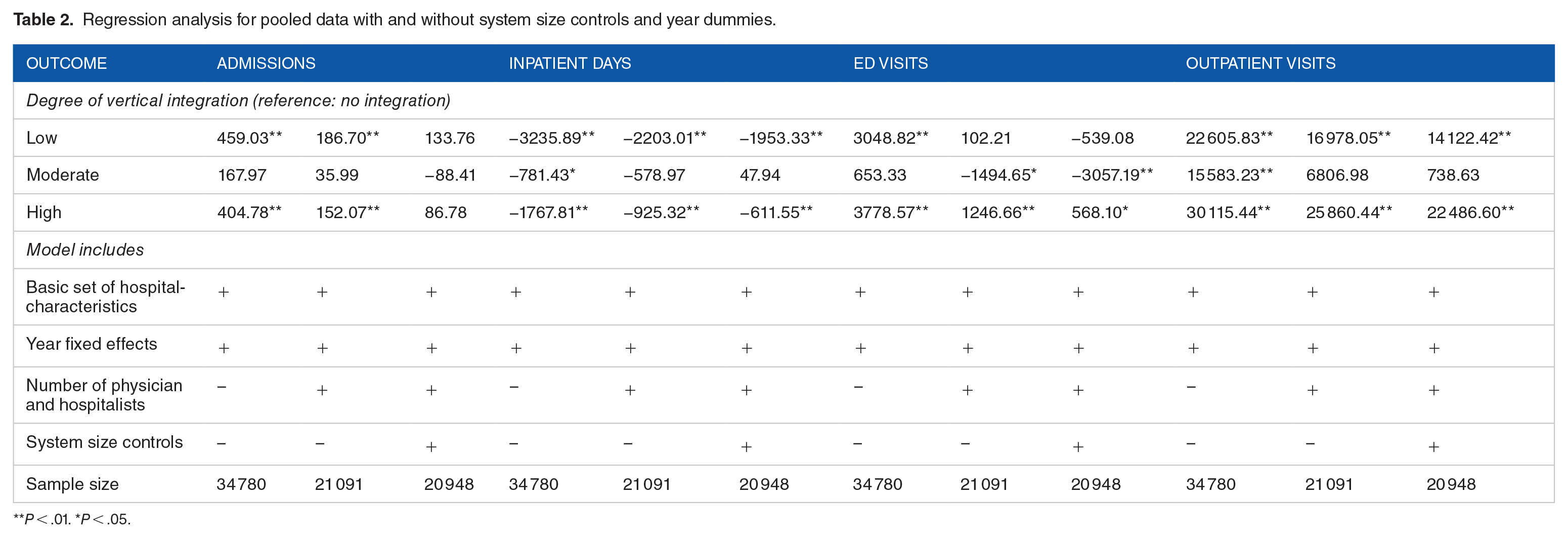
P < .01. *P < .05.

P < .01. *P < .05.

P < .01. *P < .05.
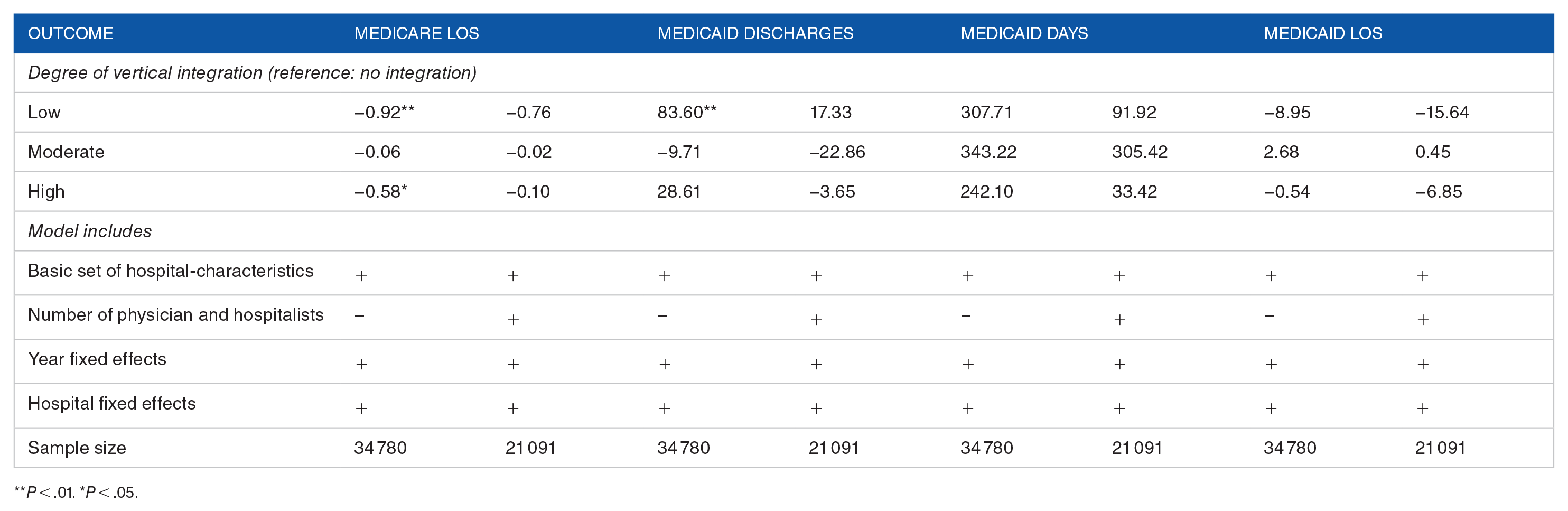
The results from our preferred set of specifications (hospital fixed effects) are shown in Table 3. Addition of hospital fixed effects to the full set of preliminary control variables (aside from system size, which do not enter into panel specifications) eliminates the statistical significance of all hospital output related changes. Our final panel results were not sensitive to an alternative way of measuring intensity of integration (Supplemental Table S5) or to lagging integration variable by 1 year (Supplemental Table S6).
Regression analysis for panel data (preferred specification).
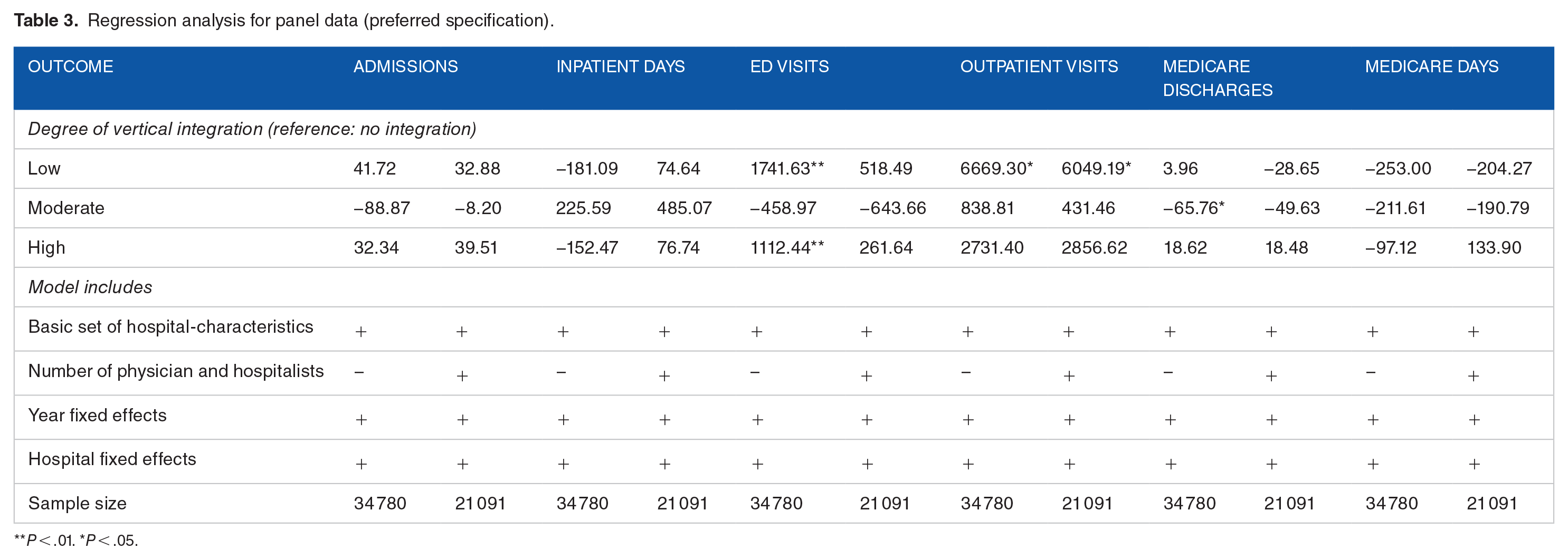
P < .01. *P < .05.
P < .01. *P < .05.
Discussion
The aim of this study was to examine the relationship between hospital physician vertical integration and hospital output. We find that a hospital’s entry into vertical integration between physician groups and hospitals has little or no impact on a broad set of metrics capturing hospital output. Furthermore, there is no clear relationship between increasing degree of administrative/financial coupling between physician groups and hospitals (as measured by higher levels of vertical integration) and hospital output. Our preliminary results without the inclusion of fixed effects show that having some form of vertical integration strongly influences hospital output even after taking size of system affiliation in account. However, these results lose significance upon addition of fixed effects suggesting that differences in output between vertically integrated and non-integrated hospitals likely stem from other time-invariant factors that affect hospital functioning and performance in more stable ways than changes in level of physician-hospital integration.
Our findings add to several strands in recent literature that find uneven associations between vertical integration and several other policy relevant aspects of hospital performance that are distinct from hospital output viz. quality, spending, financial performance, and prices. However, none of recent studies have focused on output per se. Empirical literature on how vertical integration affects hospital output is very scarce and dated. Most of the studies in this strand appeared in late eighties and nineties and typically executed hospital output as a classic Cobb-Douglas production function with case-mix adjusted number of discharges as a salient measure of output. Morrisey et al 2 found little effect of physician-hospital integration on output for urban hospitals but higher number of discharges for rural hospitals. Our study, using a substantially broader array of hospital output measures and a sophisticated metric for more complex contemporary vertical integrations comes essentially to the same conclusion, even though the regulatory landscape and organizational milieu is radically different than in nineties and eighties.
There are some plausible explanations for our findings. First, the physician utility maximization model posited by Pauly and Satterthwaite 5 suggests that utility maximizing physicians may exhibit behaviors regarding input choice and consumption that, while rational from an individual physician’s perspective, may hamper cooperation toward collective goals and lead to unwanted results for the integrated organization. For instance, physicians may overuse hospital inputs that in the short term tends to spread out the costs across all their patients, but can incur higher costs to the hospitals. Subsequently, patient output may fall as a result of declining revenues. According to this model, measuring hospital input by counting the number of hospital personnel may be imperfect. Instead of personnel, payroll and wages should be used. Our study attempts to demonstrate a relationship between hospital input (measured by vertical integration) and patient output, and does include the number of physicians, hospitalists, and nurses as key predictor variables. However, inclusion of nurse and physician salaries as one of the predictors, which was not within the scope of this study, may have revealed a different conclusion. Second, physicians should be involved in governance and management functions of the hospital’s policy decisions, so that hospitals can attract care providers with a “good fit” thereby enhancing quality and patient output. Merely vertically integrating does not guarantee the involvement of physicians within hospital governance and strategic decision making and it is possible that current arrangements lack optimal governance structures and management protocols to facilitate more effective physician involvement in hospital governance. Third, integration makes the market more concentrated. 30 Classical economics theory suggests that market concentration in less competitive markets may lead to shrinkage in output and increases in product prices. Patients with less generous insurance may face higher out-of-pocket payments or may have to travel longer distance to find out-of-network providers, as their in-network providers diminish especially for specialty care. This may in turn reduce output.
There has been a gradual shift in integration strategies within the health care sector moving from horizontal integration toward vertical integration, especially because current U.S. health policy trends that emphasize patient centered care also drive the need for better coordination of care. Many policymakers find these trends salutary and believe they will yield significant benefits over time. Our findings add to the growing body of evidence suggesting a more nuanced and mixed view of the advantages of vertical integration. Earlier cost studies showed that vertical integration may be associated with higher costs per discharge, even though the conventional wisdom is that integration may reduce costs. 2 More recent research suggests that vertical integration may significantly improve only a limited set of measures of quality, but does not impact cost or resource utilization.21,31 Vertical integration’s lack of a clear signal of effectiveness in terms of quality, and processes of care, as well as on reducing costs implies that like any other business decision, involving physicians in hospital administrative functionalities is a strategic decision that warrants a careful cost-benefit analysis. Hospitals need to carefully consider the expected gains from vertical integration strategies especially if they view it as a key lever for achieving their output enhancement goals.
This study has some limitations that are worth noting. First, our study does not measure the involvement of physicians in hospital governance, or their commitment toward the hospital which may be indirect results of vertical integration in affecting patient output. Studies in the future should include physician involvement, payroll, clinician morale, and patient insurance status as factors in studying the same associations. Second, our AHA dataset was missing information on vertical integration data for the year 2018, for which we had to impute the 2017 results. Similarly, compendium data was not available for all study years so we had to use 2018 data to assign system size variables for years 2016-19. These methodological choices may have introduced some measurement error in our measures for vertical integration and system size. Third, we assessed only vertical integration between physicians and hospitals. Our results may have limited validity for more comprehensive integrated arrangements that include other healthcare organizations (such as long-term care facilities) and managed care organizations that provide health insurance. Future studies should attempt to include metrics capable of capturing the depth and quality of physician engagement with hospital management and strategic decision-making. Finally, it is possible that some hospitals that adopted vertical integration also initiated collateral changes in management practices or operational restructuring that independently impacted output-related outcomes. Due to data limitations, we are unable to segregate such simultaneous impacts from the result of vertical integration. However, to the extent that these changes stem from stable but unmeasured differences amongst hospitals (idiosyncratic leadership practices), our fixed effects methodology can partially account for these effects.
Conclusion
Vertical integration has been a major shift in the healthcare policy landscape leading to greater ties between hospitals and physicians. Integration may improve coordination of care and efficiency. However, integration alone may not increase the involvement and commitment of patients toward hospitals. Also, integration can increase market concentration and patients may have to deal with higher payments or travel far to seek specialty and expensive care. In the years to come, it is yet to be seen if vertical integration can positively influence patient output.
Supplemental Material
sj-docx-1-his-10.1177_11786329241304619 – Supplemental material for Does Physician-Hospital Vertical Integration Affect Hospital Output?
Supplemental material, sj-docx-1-his-10.1177_11786329241304619 for Does Physician-Hospital Vertical Integration Affect Hospital Output? by Soumya Upadhyay and Neeraj Bhandari in Health Services Insights
Footnotes
Funding:
The publication fees for this article was provided by the UNLV Open Article Fund. We thank UNLV libraries for their support.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Only publicly available secondary datasets were used for this research project.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.