
Abstract
Background:
With the advancement of childhood cancer therapy, long-term survivors are on the rise. Reports on childhood cancer survivors in Saudi Arabia are scarce. This study aims to assess the spectrum and burden of long-term complications among survivors of childhood cancer in Saudi Arabia.
Methods:
This cross-sectional study, conducted at multiple cancer centers in Saudi Arabia, enrolled survivors who had been diagnosed with cancer before the age of 14 and had completed at least 5 years after completion of cancer therapy. The primary outcome was to estimate the prevalence of chronic health conditions (CHC) among these survivors. The secondary outcome was to assess the impact of primary cancer diagnosis and cancer therapies on the occurrence of CHC.
Results:
A total of 305 survivors met the inclusion criteria as of July 2022. Females were 165 participants. The median follow-up and age at evaluation were 8.5 and 14 years, respectively. Leukemia was the most common cancer type (49.3%), followed by lymphoma (16.7%) and solid tumors (15.7%). Chemotherapy was administered to 287 survivors. Radiotherapy and surgery were used in 29.2% and 22.3% of cases, respectively. Seventy-eight percent of participants experienced at least 1 CHC, with 31.1% and 14.2% having 2 and 3 CHC, respectively. A multivariate logistic regression identified significant association between CHC and solid tumors compared to hematological malignancies (OR 2.2; 95% CI: 1.1-4.3; P = .023). Growth impairment was the most common CHC, followed by endocrinopathy. Radiotherapy was significantly associated with short stature (95% CI: 1.2-3.6; P = .008). The majority of CHC, 77.3%, were mild in severity, while 19.3% were moderate, 2.9% were severe, and .5% were life-threatening.
Conclusion:
The long-term complications of childhood cancer have revealed a prevalent concern. To optimize health outcomes, it is essential to implement well-structured and long-term follow-up tailored to risk profiles, utilize cost-effective screening methods, and promote prospective clinical research and establishment of a registry.
Introduction
Based on recent data, the incidence of childhood cancer in Saudi Arabia is on the rise. A report indicates a rate of 99.8 per million population.1,2 Advances in curative therapies for many malignancies have significantly improved the survival rate of childhood cancer over the past 5 decades. Currently, more than 85% of children with cancer are cured.1,3-5 This has led to a significant increase in the number of adults who are childhood cancer survivors. In fact, it’s estimated that 1 in every 640 adults aged 20 to 39 is a survivor of childhood cancer. 6 The effects of cancer can be either transient, occurring at the initial presentation of the disease, or secondary to cancer treatment. Alternatively, they may be persistent, arising from the cancer itself or its treatment. These long-term sequelae of cancer can affect both the quality and quantity of survival, with childhood cancer survivors facing a higher risk of mortality compared with aged-matched controls from the general population.7-9
Long-term complications of childhood cancer, reported in up to two-thirds of survivors, are defined as any medical conditions that persist or develop 5 or more years after cancer diagnosis. 4 While life-altering long-term effects are frequent, life-threatening conditions are uncommon and seen in patients who had a history of relapse, high risk malignancies or received older treatment. Life-altering long-term effects can be adjusted to achieve as reported a good health in 90% of survivors.8,9 Major cooperative groups in childhood cancer treatment have prioritized reducing the risk of long-term effects through the development of new treatment regimens without negatively reducing the cure rates. 10 The spectrum of long-term complications of childhood cancer is wide, including impaired growth and development, endocrinopathy, cardiopulmonary abnormalities, neurocognitive dysfunction, renal and liver problems, relapse, and second neoplasms.4,9,11
In recent years, several cooperative groups worldwide have examined the outcomes of childhood cancer patients and developed guideline recommendations for long-term complications surveillance, which have improved early diagnosis and management of such complications.12-14 Studies evaluating the spectrum of long-term complications of childhood cancer in Saudi Arabia are lacking. Data addressing the entire spectrum of chronic health conditions (CHC) in childhood cancer survivors from developing countries are limited.15,16 Therefore, the aim of our study is to estimate the burden of morbidity in survivors of childhood cancer from multiple healthcare centers in Saudi Arabia. Moreover, analyzing such data can contribute to the implementation of evidence-based health-preserving care.4,11
Methods and Materials
Study design and participants
The study was conducted using an observational cross-sectional retrospective design across multiple healthcare institutions. The data of childhood cancer survivors, in remission after completing treatment, from 5 pediatric hematology and oncology centers were analyzed. As shown in Figure 1, participants diagnosed with cancer between 2000 and 2015 were consecutively enrolled if they met the following criteria: (1) diagnosis before the age of 14 years; (2) completion of 5 years of follow-up after treatment; and (3) at least 2 follow-up clinic visits after the initial 5-year off-therapy period. Participants whose follow-up or medical data were not complete were excluded. The data analysis cut-off was July 2022. The primary outcome of the study was to estimate the prevalence of long-term effects of childhood cancer among survivors of childhood cancer. Additionally, the secondary outcome was to assess the impact of different types of cancer on the long-term effects of childhood cancer and to evaluate the feasibility of maintaining long-term follow-up for cancer survivors. According to the study aim and feasibility of the data collection, mortality data were not collected. 5 Additionally, based on the expected prevalence from previous studies and a confidence level of 95%, the required sample size was estimated to be 289 survivors. An expected loss follow-up or missing data rate of 5% was added to ensure a sample of 304 survivors.

Consort diagram showing the survivors inclusion and exclusion criteria.
The study protocol complies with the Declaration of Helsinki and was granted ethical approval from the institutional research board (IRB) of Prince Sultan Military Medical City (SRC21R/001/01). Moreover, the IRB has approved waiving the requirement for obtaining informed consent from survivors based on the following criteria successfully met by the study: the research involves minimal risk to survivors, data is collected retrospectively from medical records, the waiver does not adversely affect the rights and welfare of survivors, and conducting the study without the waiver would be impractical due to patient visits that occurred a long time ago.
Medical data collection
Electronic health records (EHRs) were utilized to retrieve data from long-term follow-up outpatient clinics focusing on cancer care across the 5 participating hematology and oncology centers. These specialized clinics, managed by senior pediatric oncologists and senior pediatric specialists, functioned 1 to 2 times a week. Clinics in the included centers utilize the Children’s Oncology group (COG) guidelines for long-term follow-up for survivors of childhood cancer. During patient assessments, data points were documented and analyzed, including: (1) Primary cancer diagnosis; (2) comprehensive treatment details; (3) growth assessment based on detailed anthropometric measurements; (4) cardiovascular evaluations for patients exposed to cardiotoxic medications; (5) pulmonary function assessments for patients who had received chest/neck radiation therapy or medications with pulmonary effects; (6) cognitive assessments including auditory screenings for patients treated with central nervous system-directed interventions such as radiotherapy (RT); (7) assessment of gonadal function; (8) hormonal evaluations; (9) transfusion-related viral hazards; (10) social well-being concerns; (11) surveillance for cancer recurrence; and (12) secondary neoplasms.
Outcome measurement
Growth patterns were tracked by comparing measurements to the Centers for Disease Control (CDC) growth charts, with underweight and overweight categories set at below the fifth percentile and above the 95th percentile, respectively. 17 Definitions of short stature (<5th) and tall stature (>95%) were based on height percentiles. Heart function evaluations were based on conventional echocardiography, with a severe reduction in function defined as an ejection fraction (EF) of less than 30%. Lung functions were evaluated through pulmonary function tests (PFT) for specific patients, and intelligence quotient (IQ) assessments encompassed psychosocial evaluations. Auditory evaluations consisted of physical examinations, pure tone audiometry, and brainstem-evoked responses as needed. Hormonal and gonadal function were assessed through Tanner staging, hormonal and renal biomarkers, and bone density testing. Potential transfusion-related complications were monitored by analyzing liver function markers and viral serology. The study researchers graded the long-term complications of childhood cancer in the cohort based on the National Cancer Institute scoring system for common terminology criteria for adverse events (CTCAE) version 5 during medical data collection, ranging from mild to mortality. 18
Statistical analysis
Data analysis was performed using IBM SPSS version 26. Continuous variables were presented as either mean ± standard deviation or median and range or interquartile range (IQR), depending on normality of data distribution, while categorical variables were expressed as frequency distributions and percentages. The Chi-square test and independent t-test were applied for inferential statistics to draw conclusions on categorical and continuous outcomes, respectively. Additionally, a logistic regression model was utilized using odds ratio (OR) with 95% confidence interval (CI) to investigate the association between CHC and the various independent variables, including cancer type, age, gender, and follow-up duration. All statistical results were considered significant at the level of P-value <.05.
Results
Demographic features
A total of 305 participants met the inclusion criteria, completing a minimum of 5 years of follow-up for post-cancer treatment before July 2022. The participants’ demographic details, clinical profiles, and treatment histories, along with the duration of follow-up, are detailed in Table 1. Female participants constituted 46% of the cohort. The median duration of follow-up post-cancer therapy was 8.5 years (range 5-21 years) while the median ages at cancer diagnosis and evaluation were 4 and 14 years, respectively. The distribution of cancer diagnosis by age showed a prominent percentage falling between 2 and 5 years (36.1%) and those between 5 and 10 years (30.5%).
Clinical characteristics of survivors of childhood cancer.
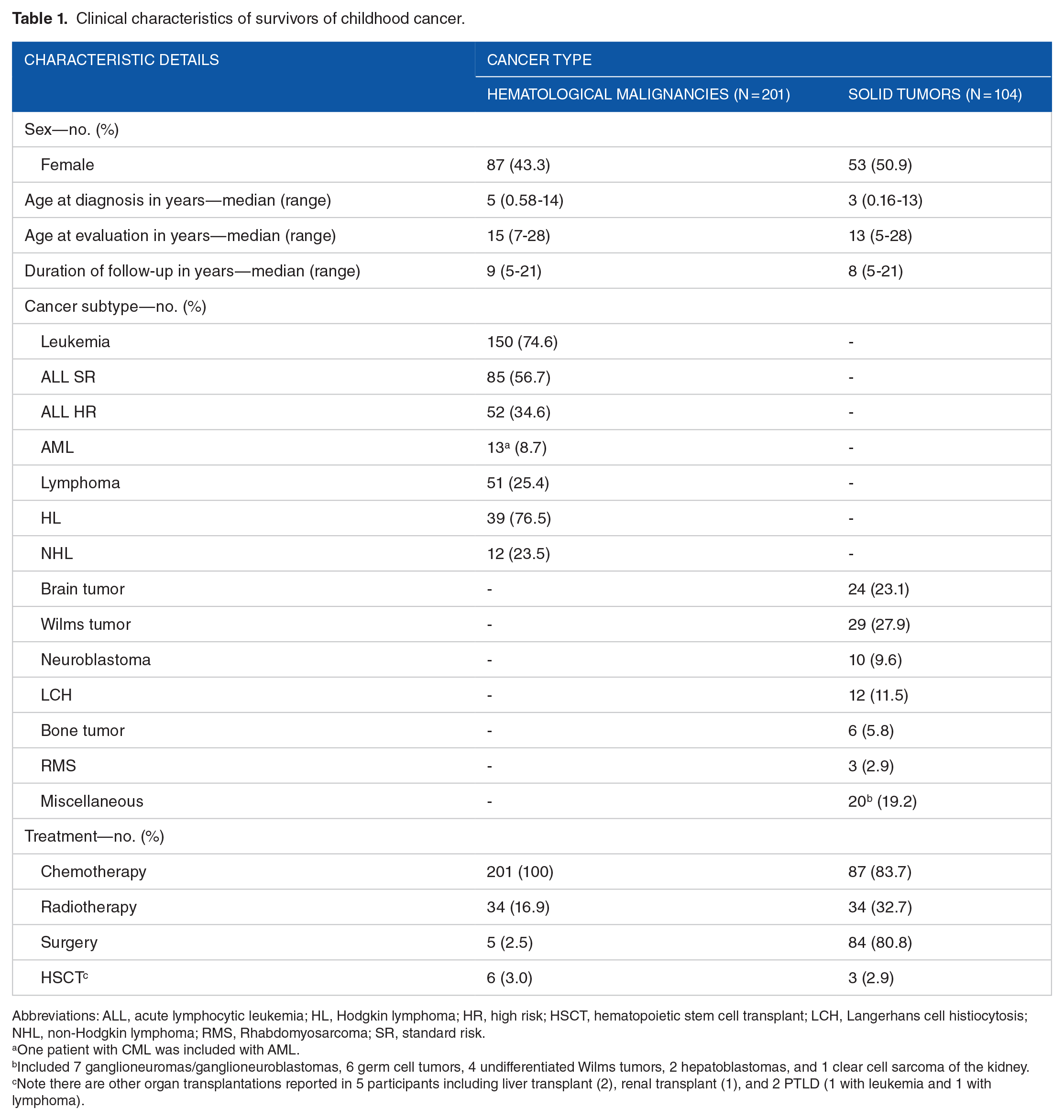
Abbreviations: ALL, acute lymphocytic leukemia; HL, Hodgkin lymphoma; HR, high risk; HSCT, hematopoietic stem cell transplant; LCH, Langerhans cell histiocytosis; NHL, non-Hodgkin lymphoma; RMS, Rhabdomyosarcoma; SR, standard risk.
One patient with CML was included with AML.
Included 7 ganglioneuromas/ganglioneuroblastomas, 6 germ cell tumors, 4 undifferentiated Wilms tumors, 2 hepatoblastomas, and 1 clear cell sarcoma of the kidney.
Note there are other organ transplantations reported in 5 participants including liver transplant (2), renal transplant (1), and 2 PTLD (1 with leukemia and 1 with lymphoma).
Cancer type and treatment strategies
Among the observed malignancies, leukemia emerged as the most prevalent at 49.2% in 150 patients, followed by lymphoma at 16.7%, solid tumors at 15.7%, and brain tumors at 7.9%. Chemotherapy was the predominant treatment modality, administered to 94.1% of the patients, while surgery and RT were utilized in 22.3% and 29.2% of cases, respectively. Furthermore, 9 patients required hematopoietic stem cell transplant, as outlined in Table 1.
Estimated burden of chronic health condition
A detailed breakdown of the morbidity burden, comparing hematological cancer to solid tumors, including various organ dysfunctions, is shown in Table 2. The estimated burden of CHC reveals a concerning prevalence among cancer survivors, with approximately 78% of the cohort experiencing at least 1 chronic health issue. Moreover, 31.1% and 14.2% of survivors are estimated to have 2 and 3 CHC, respectively. After adjusting for age, gender, and duration of follow-up, the multivariate logistic regression analysis identified a statistically significant association between CHC and solid tumors compared with hematological malignancies (OR 2.2; 95% CI: 1.1-4.3; P = .023).
Long-term complications of childhood cancer categorized by organ system.
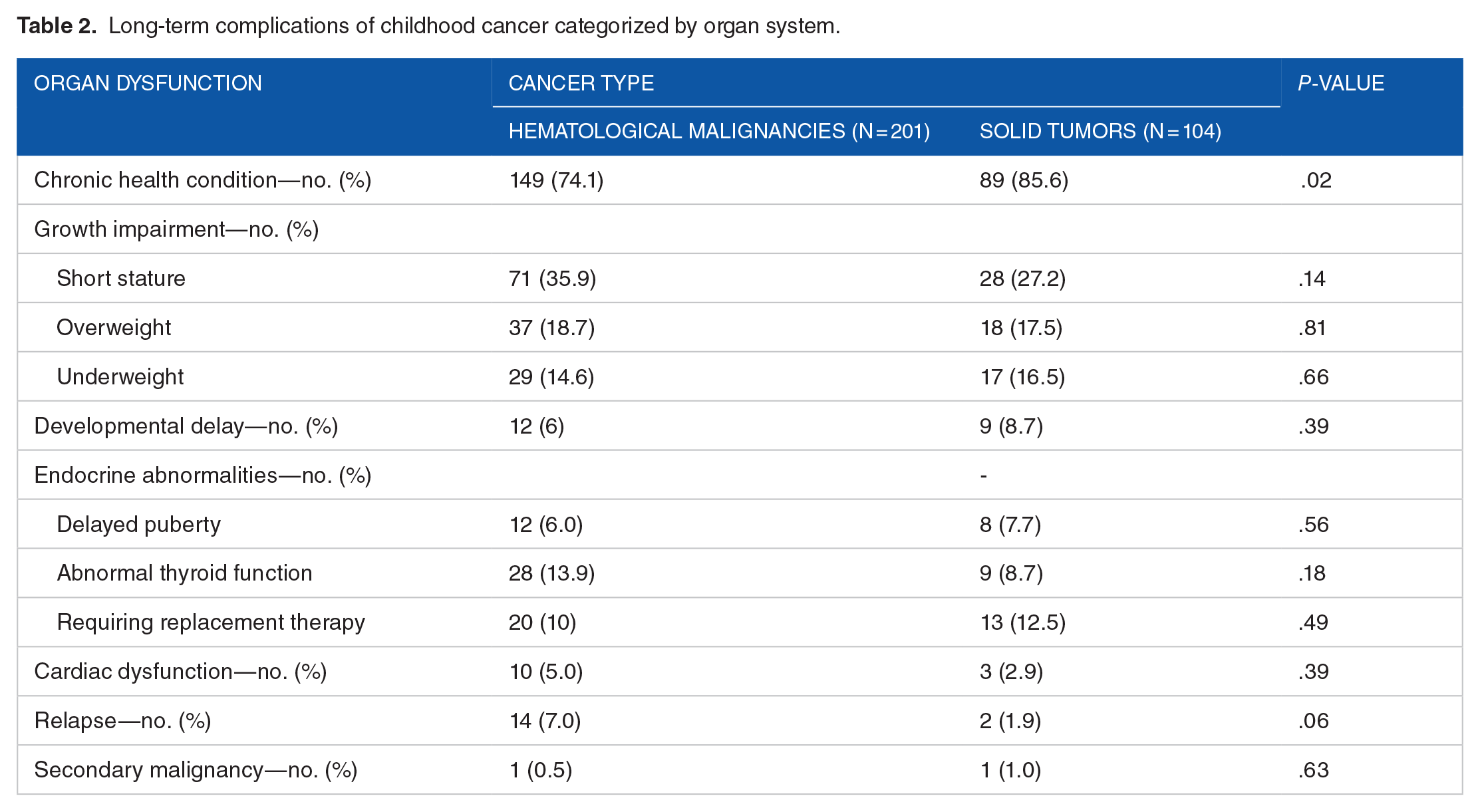
Figure 2 shows the severity scores of CHC based on CTCAE among the survivors. Out of the 384 reported health conditions, 297 (77.3%) had grade 1 (mild) disability, followed by 19.3% with grade 2 (moderate) disability and 2.9% with grade 3 (severe) disability. Two of the survivors had grade 4 (life-threatening) disability, and none had grade 5 or death (Supplemental Table).

Severity score of chronic health conditions among survivors of childhood cancer (n = 305) according to common terminology criteria for adverse events (CTCAE).
Growth impairment
As shown in Table 2, abnormalities in height and weight were identified in 114 (37.4%) and 101 (33.1%) of survivors, respectively. Short stature was the most common growth issue, affecting 99 patients (32.5%), followed by overweight in 55 (18%) and underweight in 46 (15.1%). Exposure to RT was significantly associated with short stature in survivors compared with those without history of RT (95% CI: 1.2-3.6; P = .008). However, survivors of hematological malignancies were found to have no significant difference in the risk of short stature compared with solid tumors (P = .14), as shown in Table 2.
Neuropsychological dysfunction
Among the survivors, 25 patients (8.2%) reported experiencing psychological impairment, either with or without neurological dysfunction. A psychological evaluation of these individuals uncovered a range of disorders, such as anxiety, depression, social withdrawal, and attention deficits. Additionally, 18 survivors (5.9%) were found to have impaired IQ, with 4 of these patients also experiencing psychological impairment. Specifically, survivors with impaired IQ included: 9 with leukemia, 5 with brain tumors, 3 with solid tumors (including 2 with Wilms tumor and 1 with neuroblastoma), and 1 with Hodgkin lymphoma as shown in Table 2. Furthermore, 2 patients had Down syndrome, 3 had attention deficit hyperactivity disorder, and 2 had speech delay. Hearing assessments indicated impairment in survivors with hematological malignancies (10 patients) and solid tumors (4 patients).
Endocrinopathies
The estimated prevalence for delayed puberty among the survivors was 20 individuals (6.6%), as seen in Table 2. Abnormal thyroid function test estimated in approximately 12.1% (37 survivors). Abnormal thyroid function was more frequent in survivors of hematological malignancies compared to those with solid tumors but did not reach statistical significance (Table 2). The proportion of individuals requiring replacement therapy was 20 survivors (10%) in the hematological malignancies group and 13 survivors (12.5%) in the solid tumors group, with no significant difference between the 2 groups.
Cardiac dysfunction
Abnormal echocardiograms were reported in 13 individuals (4.3% of the total cases), as shown in Table 2. The median age upon cardiac evaluation was 12 years, ranging from 9 to 16 years. Out of the abnormal echocardiography, 8 patients (2.6%) exhibited impaired EF. Within a specific healthcare center, 2 survivors required medical therapy for myocardial dysfunction with an EF below 40%, out of a total of 5 affected individuals. Cardiac dysfunction was associated with hematological malignancies in 10 cases (6 with leukemia and 4 with lymphoma) and with solid tumors in 3 cases (Ewing sarcoma, Wilms tumor, and rhabdomyosarcoma).
Other organ dysfunction
The estimated frequency of survivors with abnormal PFT on follow-up was 8 patients which constitutes 2.6% of the participants. Elevated liver enzymes were rare and reported in 7 (2.3%) of the survivors, while impaired renal function affected 11 individuals (3.6%). Two survivors who had leukemia were found to have transfusion related hazards.
Relapse and secondary malignancy
Out of the 305 patients, relapse post-cancer treatment and secondary malignancies was observed in 5.2% and 0.7% respectively, as listed in Table 2. While the incidence of relapse was higher among patients with hematological cancers (14 patients) compared to those with solid tumors (2 patients), this difference was not statistically significant (P > .05).
Discussion
This study is the first to describe the long-term complications of childhood cancer in Saudi Arabia with reference to long-term follow-up and the prevalence of CHC. Data among 305 survivors of childhood cancer identified a high prevalence of CHC affecting 78% of individuals. Moreover, approximately one-third of these survivors have 2 CHC. Further analysis of the different types of health conditions in comparison with the cancer type showed the main findings: growth impairment ranked as the most common CHC, followed by endocrine dysfunction. Additionally, our findings revealed a notable correlation: survivors with solid tumors faced a significantly higher frequency of CHC when compared to those with hematological malignancies.
The increasing advancements in cancer therapy, aimed at curing patients, along with the growing number of survivors, underscore the high prevalence of long-term complications in these individuals as noted in findings of the current and other similar studies across continents.16,19-21 Therefore, enhancing our understanding to progress specific long-term follow-up care for cancer survivors is imperative. 21 It is crucial to raise awareness and implement long-term follow-up measures for the late effects of childhood cancer. This includes educational efforts, prevention strategies tailored to risks, surveillance plans specific to effects, counseling services, and comprehensive multidisciplinary approaches. 12 These steps are essential to detect early signs of treatment or cancer-related complications and to initiate the appropriate therapeutic interventions. 22 Moreover, survivors of childhood cancer face a substantial risk of developing serious health conditions. A recent comprehensive retrospective study has revealed that cancer survivors face a substantially elevated risk of mortality and life-threatening conditions, 6.2 times higher than that of the general population. 19 These additional findings emphasize the critical importance of implementing a comprehensive long-term follow-up framework to mitigate the heightened risks of morbidity and mortality.
The findings of the ranked CHC in the current study, focusing on growth impairment and endocrine dysfunction, underscore the importance for physicians to address and minimize such complications. To achieve this goal, it is imperative to establish standardized long-term follow-up programs for cancer survivors in Saudi healthcare institutions, incorporating a multispecialty team, particularly within the endocrine service. This approach will enhance the effectiveness of these programs. Moreover, conducting prospective studies to evaluate these Saudi programs, including appropriate patient-reported outcomes, is essential for a comprehensive assessment of interventions. 23
The transition of healthcare services from pediatric to adult care in the context of most chronic diseases such as cancer survivors is known to face multiple obstacles, including the practices themselves, barriers, and healthcare implementation. 24 Studies on survivors of childhood cancer, including the current study, have shown that most of these individuals are in their teenage and early adolescent years, which makes it likely for them to be transferred from pediatric to adult healthcare services. Additionally, teenagers who are cancer survivors have a risk of various health conditions involving most organ systems, including the endocrine system, which require early detection and optimal treatment to ensure normal growth into adulthood. Unfortunately, many cancer centers do not have established standards for survivorship transition, which is a significant concern. 25 Such findings highlight the critical importance of establishing well-structured practices to support the transition of survivors, ultimately ensuring uninterrupted optimal healthcare for adult survivors of childhood cancer.
The rapid advancement of digital medicine has the potential to alleviate the burden of long-term monitoring for childhood cancer survivors. Indeed, artificial intelligence (AI), with its diverse applications, is playing an increasingly significant role in healthcare services. 26 It has the capacity to yield substantial and enduring improvements in the long-term health and well-being of these survivors by facilitating more effective and cost-efficient monitoring and care through advanced screening methods. Recent studies have successfully evaluated the use of AI in analyzing ECG data to predict the risk of late-onset cardiomyopathy in this population.27,28 However, the implementation of such advanced screening methods necessitates evaluation in clinical trials, with careful consideration of the ethical implications surrounding these emerging healthcare technologies.
There are several limitations to our study. First, such a study looking at the prognosis of long-term survival of a certain condition ideally should be reported through a prospective study. However, being time-consuming is an obstacle that can limit the feasibility of these studies. Second, the study is a retrospective study that uses secondary data collection, which can limit the accurate estimation of complications and ultimately increase the risk of information bias. Third, the exclusion of mortality data and participants with incomplete follow-up or medical data may have introduced selection bias; However, it is important to note that participant selection in this study was influenced by the approach of the national healthcare system in treating cancer patients. Moreover, we analyzed most of the data from the last 2 visits from the oncology follow-up clinic, which could obscure the presence of other CHC. Additionally, the population sample size is considered small compared with the available robust data from other similar studies. However, our study was limited because of issues outside the principles of clinical research. Furthermore, the study lacks a comparison with a similar cohort from the general population. 29 Such an analysis can establish the actual risk of CHC in relation to individuals without previous oncological conditions.
Conclusion
The estimated high prevalence of CHC in long-term survivors of childhood cancer in our cohort is in line with reported findings in the literature and encourages the establishment of a well-structured program that uses advanced, tailored to risks, and cost-effective screening methods to ensure optimum healthcare follow-up. The high risk of long-term complications of childhood cancer underscores the importance of clinical trials in developing treatment strategies with minimal long-term adverse events and without reducing the cure rate. Furthermore, most survivors are teenagers, which emphasizes the importance of maintaining uninterrupted programs. Additionally, providing a suitable follow-up strategy that is acceptable for survivors and ensures adherence to lifelong medical check-ups is crucial. Finally, the findings encourage expanding evidence-based knowledge through prospective studies on detailed issues surrounding childhood cancer survivors.
Supplemental Material
sj-docx-1-his-10.1177_11786329241299317 – Supplemental material for Long-term Follow-up for Survivors of Childhood Cancer in Saudi Arabia: A Multicenter Cross-Sectional Study
Supplemental material, sj-docx-1-his-10.1177_11786329241299317 for Long-term Follow-up for Survivors of Childhood Cancer in Saudi Arabia: A Multicenter Cross-Sectional Study by Fahad Alabbas, Ibrahim Alharbi, Naveed Ahmad, Walid Ballourah, Khalid Alnajashi, Ghaleb Elyamany, Nawaf Alkhayat, Yaser Borai, Omar Alsharif, Hasna Hamzi, Amal Bin Hasan, Waleed Ibrahim, Luluah Albahlal, Sara Alnasser, Sulaiman Alajlan, Abdelrahman A Aboush, Reem Al-Sudairy and Abdulrahman Alsultan in Health Services Insights
Footnotes
Acknowledgements
The authors would like to thank the SANAD Children’s Cancer Support Association for helping the research and supporting children with cancer.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the SANAD Children’s Cancer Support Association and the SANAD Research Grants Program, grant number: RGP-2020-13.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors Contributions
All authors contributed equally. All authors contributed to this manuscript accordingly. All authors have read and approved the final manuscript and agreed to the published version of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.