
Abstract
Background:
Despite the known benefits of cardiac rehabilitation (CR), the rate of participation is low following coronary artery bypass graft (CABG). The reasons for this lack of participation are unclear and there have been few studies investigating this, particularly in Asian countries. The present study aimed to address this lack of information and identify reasons for non-participation in phase-2 CR among patients who underwent CABG.
Methods:
We enrolled 42 patients who underwent CABG or CABG combined with valvular heart surgery in a university hospital between October 2016 to September 2018. Patients who participated in phase-1 but not phase-2 CR were interviewed by phone following an 11-item questionnaire.
Results:
The rate of participation in phase-2 CR was only 12.5%. The most frequently reported reason for non-participation was “Did not know that there was phase-2 CR” (61.9%), followed by “Transportation problems” (31%). “Unable to take leave due to work schedule” was fairly frequently reported (19%) as was “Did not participate due to chronic diseases and complications” (14.3%).
Conclusion:
Our study revealed low participation in phase-2 CR, despite its well-known benefits. The primary reason identified was a lack of awareness and understanding among patients regarding phase-2 CR. This highlights the need for targeted interventions aimed at increasing knowledge and awareness of the benefits and availability of CR. Additionally, it is crucial to establish an efficient referral system that ensures seamless transitions from the initial cardiac treatment to the rehabilitation phase. Implementing these strategies is expected to boost CR participation, leading to improved patient outcomes and overall cardiac health.
Introduction
Cardiovascular disease is the leading cause of disability and death worldwide, accounting for one-half of all noncommunicable disease deaths, with 70% of deaths due to the condition occurring in low- and middle-income countries. 1 Cardiac rehabilitation (CR) has been shown to improve exercise capacity and quality of life and to reduce mortality among patients with cardiovascular disease. Therefore, participation in outpatient CR is highly recommended in practice guidelines around the world.2,3 The beneficial effects of CR have also been documented in patients undergoing coronary artery bypass graft (CABG) and CABG combined with valvular heart surgery. Participation in CR after CABG is associated with a significant reduction in risk of cardiac events and readmission 4 as well as a significant relative risk reduction in 10-year all-cause mortality. 5 Most CR programs typically involve patient assessment, exercise training, physical activity counseling, and risk-factor modification. These programs are usually divided into 3 main phases: Phase 1 occurs during hospitalization (inpatient phase), Phase 2 takes place after discharge (outpatient phase, which can be in a hospital- or home-based setting), and Phase 3 is the maintenance phase. Ensuring a continuum of care throughout these phases is crucial to provide patients with ongoing, coordinated support throughout their recovery and to promote lifelong heart-healthy behaviors.
Despite the numerous benefits of CR, the approach is underutilized worldwide, with phase-2 CR reported utilized in only 31% of patients who underwent CABG in the United States in 2007. 6 Additionally, a systematic review found that women have up to 4 times higher odds of non-participation than men, with the included studies being conducted mostly in high-income countries. 7 It is also possible that the utilization of CR is reduced in middle- and low-income countries, where CR remains largely unavailable. 8
Lee et al 9 observed that participation in phase-1 and phase-2 CR was significantly associated with a 20% and 40% reduction in all-cause mortality, respectively. Therefore, encouraging patients to continue to phase-2 CR should be a priority for clinicians. Previous studies have identified factors influencing participation in CR, typically categorized as patient related, healthcare related, socioeconomic, and transportation factors.6,10-14
While certain barriers to participation are commonly identified, such as female gender, lack of knowledge, proximity to CR centers, or low referral rate; the contextual factors and personal aspects influencing CR participation differ among countries, emphasizing the significance of national perspectives. Currently, there is little data on CR participation and the reasons for nonattendance in Association of Southeast Asian Nation (ASEAN) countries. The purpose of this study was, therefore, to define the reasons for nonattendance of phase-2 CR among Thai patients who had undergone CABG.
Methods
This study was conducted in a university hospital in Bangkok, Thailand. We included patients over 18 years of age who underwent CABG and CABG with valve replacement and completed phase-1 CR between October 2016 and September 2018. Exclusion criteria were participation in phase-2 CR at our hospital, as determined through patient records and follow-up data, as well as the inability to complete the phone interview.
Cardiac rehabilitation program
The CR program of our university hospital consists of the standard 3 phases: Phase 1 is carried out during inpatient stay. After surgery, patients are consulted by the attending surgeon regarding the cardiac rehabilitation program. Subsequently, a rehabilitation physician evaluates the patients and prescribes the CR program if there are no contraindications. The CR program is designed to be tailored to each patient’s specific needs. A physical therapist delivers the exercise-based daily CR program. The rehabilitation physician follows up with patients and asked if they want to participate in phase-2 CR; if so, appointments are made within 1 to 3 months of discharge. Phase-2 CR is an outpatient program consisting of an 8-week course comprising once-weekly outpatient sessions of a hospital-based exercise program and at least 2 sessions per week of home-based exercise. The hospital-based sessions include initial assessment, 45 to 60 minutes of circuit training with warm-up and cool-down periods, and patient education on risk and lifestyle modifications. Phase 3 is a maintenance program in which patients will be followed up every 3 to 6 months to ensure that they are adhering to the exercise regimen and modifying high-risk behaviors such as blood pressure control, physical inactivity, smoking, unhealthy diet, and alcohol consumption.
Questionnaire and data collection
A questionnaire was developed based on extensive literature review and information gathered from patients who completed phase-1 CR. Two rehabilitation physician who specialized in CR and 1 epidemiologist thoroughly reviewed the validity of the questionnaire. The initial draft of the questionnaire was tested by conducting phone interview with 5 randomly selected patients who participated in phase-1 CR to refine its accuracy and reliability. The final questionnaire included 11-items, designed to be quantitative in nature with closed-ended questions and checkboxes. The questionnaire covered 3 main domains: CR recognition, CR barriers, and CR accessibility. In the CR barriers section, patients could select multiple barriers with some answers leading to follow-up questions for further exploration. The interview was conducted via telephone by the researcher to ensure a higher response rate and provide an opportunity for immediate clarification of any questions. The data was recorded by filling in the responses manually into the questionnaire during the phone call. Baseline demographic, clinical, and procedure data were extracted from medical records.
Ethical consideration
The human and ethics committee of the institute approved the study and all its protocols (IRB number 645/61, date 29/11/2018). Verbal informed consent was obtained from each participant prior to the telephone interviews and was documented in their records. Consent for the use of medical record data was also granted by the hospital. Written consent was not required due to the minimal-risk nature of the study, and verbal consent was deemed sufficient to ensure participants’ understanding and voluntary participation. This approach was approved by the Ethical Committee in accordance with the Declaration of Helsinki. Data extraction was conducted following ethical guidelines to ensure confidentiality and privacy.
Statistical analysis
Continuous variables were assessed for normal distribution and are reported as mean ± SD or median (interquartile range). Categorical variables are reported as numbers and percentage. Data processing and statistical analyses were performed using SPSS Statistics, version 22 (IBM).
Results
We enrolled 42 patients for the present study. Figure 1 presents the flow diagram for study enrollment. Clinical characteristics of the study population are shown in Table 1. Three participants attended phase-2 CR in a center other than our hospital. The first 3 questions of the questionnaire related to CR recognition; 83% of participants said that they remembered following an exercise program during admission, but 66.7% reported not having been invited to participate in phase-2 CR or having the program explained to them. The majority of the patients (83.3%) reported not being informed about phase 2 CR during a follow-up appointment.

Flow diagram of participant enrollment.
Characteristics of the study population. a .
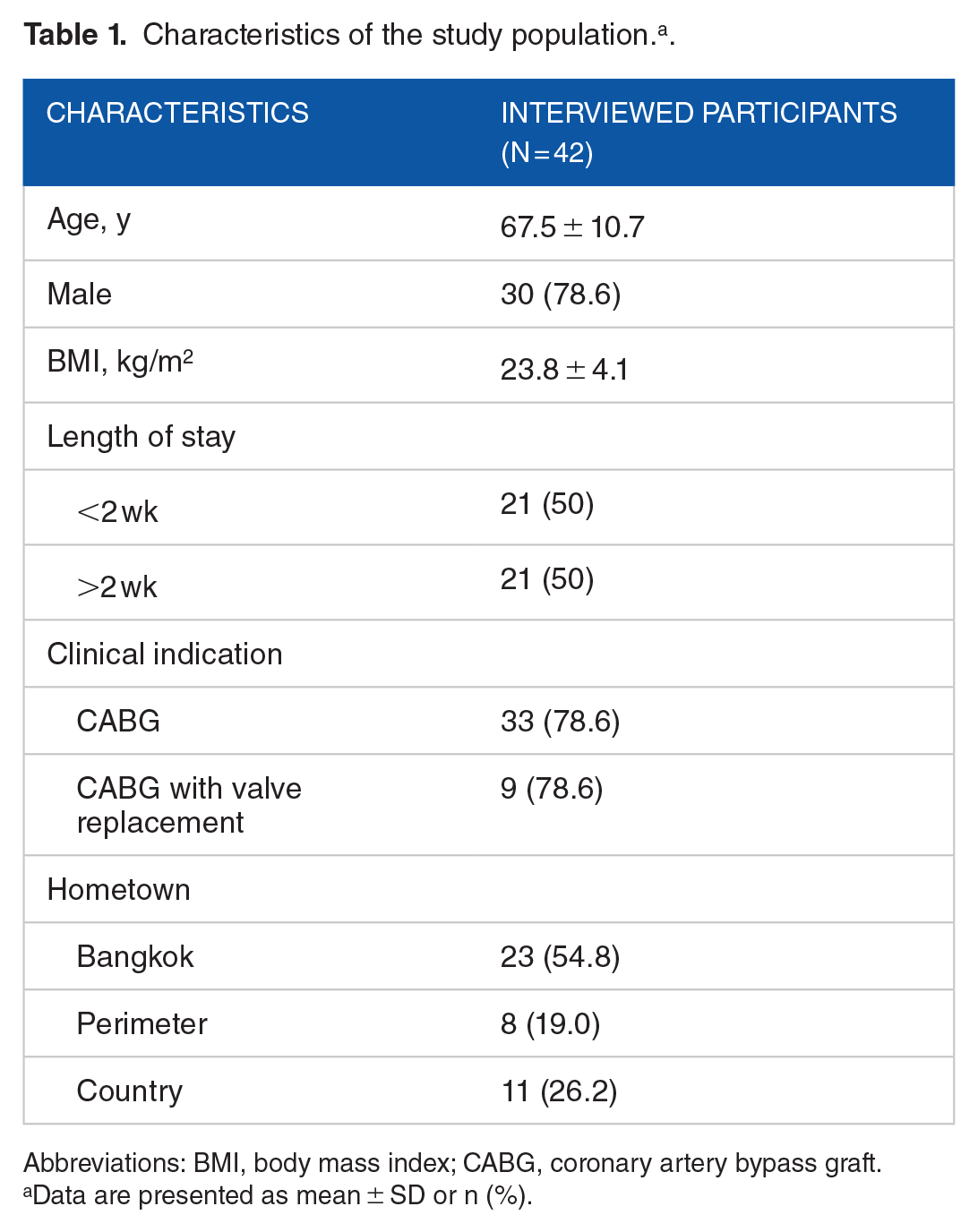
Abbreviations: BMI, body mass index; CABG, coronary artery bypass graft.
Data are presented as mean ± SD or n (%).
The most common reason for not participating in phase-2 CR was “Did not know that there was phase-2 CR,” followed by “Transportation problems,” then “Unable to take leave due to work schedule” (Figure 2). “Did not participate due to chronic diseases and complication,” was the fourth most frequent reason for non-participation, and the majority of participants who gave this response reported a condition that limited their ability to ambulate independently. We also asked participants to specify the transportation problem, and the most common reason given was distance or time consuming, followed by transportation dependency (Figure 3).

Reasons for non-participation in phase-2 cardiac rehabilitation after completing phase-1 cardiac rehabilitation.

Sub-reason of transportation problems.
Discussion
There is evidence that patients undergoing CABG are more likely to attend CR than other cardiac patients.6,15 However, we found the rate of attendance for phase-2 CR to be only 12.5%, which is lower than the rate in western countries but equivalent to a study conducted in Singapore which reported that 12.3% of patients who underwent percutaneous coronary intervention agreed to participate in phase-2 CR. 13
All participants in the present study completed phase-1 CR, and the majority reported an awareness of the exercise program they were receiving. However, the patients may be unaware that the exercise was part of the CR program with the continuum of care to the outpatient component. Our finding that only a small proportion of patients were aware of phase-2 CR upon discharge is consistent with a systematic review published in 2012, which reported a lack of personal insight and knowledge to be a common barrier to attendance. 16
Our findings together with previous studies highlight the importance of healthcare related and intrapersonal factors in determining CR attendance. Healthcare-related factors that can reduce the likelihood of CR attendance include a lack of effective communication during the inpatient program and after discharge, and a well-functioning referral system. Although CR is a class 1 recommendation for every patient undergoing CABG, only 72% of participants were consulted for phase-1 CR, and about 10% of the interviewed patients reported being informed of phase-2 CR at a follow-up appointment. A systematic review 17 reported physician recommendation to be the primary physician factor affecting CR enrollment. Therefore, increasing specialists’ and primary care physicians’ awareness of the importance of outpatient CR is crucial. The CR referral system in the present study is not automatic, and thus is entirely dependent on the healthcare provider. Grace et al 18 demonstrated that implementation of automatic referral strategies significantly impact access to CR. A combination of automatic referral methods and thorough discussions with healthcare providers should be encouraged in order to remove this barrier.
Intrapersonal factors relate to patient awareness and understanding of the information offered by the staff. A lack of understanding of the illness itself may contribute to non-participation in therapeutic programs; a systematic review published in 2006 revealed that patients are less likely to see the relevance of behavioral interventions such as CR if they do not understand the underlying chronic process that leads to coronary artery disease. 19 Hence, effective comprehensive education is needed to help patients understand the nature of the disease and the benefits of CR, and to encourage them to seek further help when necessary.
Transportation problems significantly impacted CR attendance in the present study. Almost half the patients who reported they were not aware phase-2 CR stated that they would not have participated if they had known because of transportation problems. Our findings are consistent with a study conducted by De Vos et al 20 in Belgium, which also identified transportation problems as the primary reason for non-participation, despite the fact that most patients lived within a 20 km radius of the CR center. Similarly, a study in the Czech Republic highlighted distance as a significant obstacle to CR participation. 21 Other studies have supported the substantial impact that logistics can have on CR attendance,10,14 with the distance between the patient residence and CR center having a significant negative relationship with CR utilization. In Thailand, most patients who are referred for CABG or valve surgery return to their local hospital for follow-up. Tertiary care facilities typically only offer limited CR, and such facilities are often located in Bangkok or the city centers of each province. Only 3 patients in the present study attended CR at a center nearer to their home. Although half of the patients live in Bangkok, the dependency for transportation was highly reported as a transport-related reason for non-participation. A study in 2016 showed that elderly individuals in Bangkok typically travel distances ranging from 3 to 8 km for medical services. Within this distance range, it was observed that they predominantly rely on door-to-door transportation options such as cars and taxis. Notably, more than half of the elderly individuals who use private cars depend on others for their transportation needs, intensifying the transportation barrier for accessing cardiac rehabilitation services. 22
Pardaens et al 23 described dependency for transport as a major predictor for failure to complete a CR program. To address this logistical barrier, a 2019 statement from the AACVPR/AHA/AAC suggested that home-based CR may be a feasible alternative for low-to-moderate-risk patients who are eligible for CR but cannot attend traditional center-based CR programs. 24 Thus, the development of an optimized home-base program tailored for Thai patients could increase participation and improve patient outcomes.
The inability to take leave from work in order to complete CR reflects the influence of socioeconomic factors on patient rehabilitation. Winnige et al 21 found that financial reasons were the significant barrier to participation in outpatient CR, and the most common reason for non-completion was work interference. A further 2 studies carried out in Asian countries found busy work schedules and time conflicts to be significant factors influencing participation in CR.10,13 Offering CR sessions in the evenings or on weekends might be a strategy to overcome this barrier.
We discovered that a considerable number of participants did not participate in CR due to complications or chronic conditions including chronic renal failure, cerebrovascular disease, and other conditions that impede mobility. The presence of multiple comorbidities represents another important intrapersonal factor associated with participation in CR. Listerman et al 25 revealed that, regardless of the medical burden of comorbidities, all patient groups benefited from CR, particularly older patients. Thus, attendance should not be discouraged.
Our study has several limitations which should be acknowledged. First, the data were obtained from a single university hospital. The overall interpretation can be influenced by the specific CR services available as well as by patient characteristics. To improve the generalizability of results, further multicenter studies involving larger sample sizes are required. Second, the study only included participants who underwent CABG or CABG combined with valve surgery. The results may not, therefore, be representative of other cardiac patients with different characteristics, such as those with congestive heart failure. Third, our sample size was relatively small, and no formal sample size calculation was performed as we included all available cases from the study period. While sufficient for initial exploratory analysis, our small sample size may affect the robustness and generalizability of the findings. Larger studies with calculated sample sizes are needed to validate our results and enhance statistical power, providing more definitive conclusions. Fourth, sociodemographic data were not collected in this study, limiting our ability to explore how these factors might influence CR participation. Finally, while using a survey allows for efficient data collection from a larger number of participants and facilitates the quantification of responses, surveys may also be subject to response bias and may not capture the depth of individual experiences. Future research could benefit from a mixed-methods approach, combining quantitative surveys with qualitative interviews to provide a more comprehensive understanding of the barriers to CR.
Conclusions
Despite the proven benefits of CR, we found the rate of participation in phase-2 CR to be low among Thai post-CABG patients. Initial insights showed that a lack of knowledge about the program is the primary reason for non-participation. To address this, clinicians should implement targeted educational interventions to improve patient awareness of CR benefits. Additionally, creating a streamlined referral system can ensure smoother transitions from hospital to outpatient CR. By focusing on these areas, we aim to increase CR participation rates, which may lead to improved patient outcomes and enhanced cardiac health.
Footnotes
Acknowledgements
The authors would like to thank all the patients who participated in this survey.
Author Contributions
S.R. contributed to conceptual design, review and editing the manuscript, T.P. contributed to data collection and analysis, T.W. contributed to conceptual design and supervise the work planning. T.R. contributed to the methodology design, review and editing the manuscript, J.C. contributed to the conceptual design and writing the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research and authorship of this article.
Ethical Considerations
The study was approved by the human and ethics committee of the Faculty of Medicine, Chulalongkorn University. (IRB number 645/61 date 29/11/2018).
Consent to Participate
Verbal informed consent was obtained before commencing each telephone interview.