
Abstract
This quasi-experimental study investigated the preliminary effects of a structured education intervention in a pooled sample of cardiovascular rehabilitation (CR) patients in Brazil. Recently enrolled (RE) and long-term enrolled (LTE) patients attended 12 weekly education sessions in addition to three weekly exercise sessions. Patients completed surveys assessing disease-related knowledge, physical activity, food intake, self-efficacy, and health literacy. Functional capacity was assessed by the 6-minutes walking test. All outcomes were assessed at pre-,post-CR, and 6-months follow-up. Bonferroni correction was applied. In total, 69 (69.7%) patients completed all three assessments. There were significant improvements in knowledge pre-to post-test in both subgroups (p < 0.001), and in functional capacity (p ≤ 0.001) and food intake (p ≤ 0.001) pre-to post-test in the RE subgroup. Post-test knowledge was correlated to physical activity, functional capacity and health literacy. This preliminary study suggests the importance of structured education for CR patients. A larger study using a randomized controlled design is needed to determine efficacy.
Keywords
Introduction
Cardiovascular diseases (CVDs) are the main cause of death worldwide.1,2 In recent years the risk of premature death from chronic non-communicable diseases has been reduced in Brazil 3 therefore, more people have been living with CVDs, requiring support to manage symptoms and reduce the risk of future complications. 4 Cardiovascular Rehabilitation (CR) is a widely-recommended treatment for CVDs, with its cost-effectiveness proven. 5 Based on substantive evidence, CR participation is associated with 20–50% reductions in mortality and morbidity.6–8 CR is an outpatient approach to primary or secondary prevention of CVDs, composed of structured exercise, management of risk factors, psychosocial counseling, and patient education.4,9 These components could be delivered in different modes, including remotely. 10
Patient education is not only considered a core component, but a quality indicator of CR. 11 Studies have shown that education increases knowledge and facilitate behavior change of cardiac patients, optimizing quality of life.9,11–18 Patient education programs within CR can vary substantially. This heterogeneity makes it difficult to understand which educational strategy is most effective for cardiac patients.17,19,20 To our knowledge, Cardiac CollegeTM is the only evidence-based and theoretically-informed comprehensive educational program for CR patients available globally.21–23 Although the effectiveness of Cardiac CollegeTM in Brazilian patients was confirmed, the program where it was empirically tested was created for the trial (i.e., it was not tested in a traditional CR program in Brazil). As in most countries of Latin America, patient education is not prioritized and, when administered, there is also no evidence of standardization.24,25
In this study, we aimed to understand the effects of this structured education intervention in a well-established public CR program in Brazil. This program has been serving cardiac patients from low resource settings for 28 years; however, education was never included in its programming in a structured format, although present as part of the important role of physical and rehabilitation medicine specialists. 26 The results of this research can help to understand the potential benefits of including a structured education curriculum in similar programs and settings. In addition, as many programs in Brazil have long-term enrollment (i.e., patients participate in the program as much as they want), the present study makes it possible to evaluate and understand the course of different variables both in long-term enrolled and recently enrolled patients. Therefore, it aimed to investigate the preliminary effects of a structured educational program – Cardiac CollegeTM – in a pooled sample of cardiac patients at different stages of enrollment in a CR program in Brazil.
Methods
Design
This was a quasi-experimental non-randomized study (pretest posttest with no control group), in which a pooled sample of cardiac patients at different stages of enrollment underwent the same education intervention, with assessments carried out at baseline (pre-test), immediately after the education intervention (post-test) and 6 months after the intervention (follow-up). The research was conducted within the standards required by the Declaration of Helsinki and was approved by the Ethics Committee (2.915.892). Data were collected between August/2018 and March/2020 in one CR program (Florianopolis, Brazil).
Participants and Sample Size Calculation
Participants at two stages of CR enrollment were included in this study: recently enrolled (RE; newly admitted patients); and, long-term enrolled (LTE; already attending the CR program for at least 5 months). Patients with clinical diagnosis of CVDs and/or relevant risk factors were included. Those under the age of 18 years old, or any visual or cognitive condition that would prevent them from completing the questionnaires were excluded.
Sample size was based on conservative calculations with an expected small to moderate effect size (d = 0.25) for knowledge, a statistical power of 0.95 and alpha of 0.05. A total sample size of n = 50 was deemed necessary based on these parameters. Calculations were made with GPower 3.1 using the following parameters: F-test, ANOVA repeated measures, within factors, number of groups = 1, number of measurements = 3, correlation among repeated measures = 0.5, nonsphericity correction ε = 0.99. Anticipating a 50% retention rate based on similar studies, a minimum of 100 participants were required to achieve a final sample size of 50. Patients were approached consecutively until the required sample size was achieved, independently of the stages of enrollment they were in.
Intervention and Data Collection Procedures
Patients included in the RE (CR phase II and III) were informed about the research at the time of program enrollment. LTE patients were invited to participate in the study 15 days before the beginning of education sessions. Patients who agreed to participate signed the Consent Form and completed the first assessment. All patients participated in physical exercise sessions (3 times a week, 1 hour each; Supplemental Appendix), which were supervised by a multidisciplinary team. LTE was attending these exercise sessions before the study started. RE started the education and exercise sessions at the start of the study.
The education program comprised of 12 1-hour weekly sessions in addition to the exercise sessions. The education intervention was carried out at the rehab center in a classroom with multimedia features, following Cardiac CollegeTM standards and guidelines. 21 The education program was translated and culturally adapted to Brazilian Portuguese, using adult learning principles. 27 Sessions were delivered by a multidisciplinary team trained on adult learning and included lectures and group discussions. The didactic material was composed of nine booklets and each participant received these materials. All content was available online and included education on exercise, diet, psychosocial health, medication, how the heart works and action planning. 28
Measures
Sociodemographic, and clinical characteristics (age, sex, clinical diagnosis, risk factors, educational level and family income) were self-reported. Knowledge, physical activity, functional capacity, food intake, self-efficacy, and health literacy were assessed pre-test, post-test and at follow-up. Adherence to the intervention (i.e. completion of 12 education sessions) was also measured.
Knowledge
Disease-related knowledge was assessed using the Portuguese version of the Coronary Artery Disease Education Questionnaire Short Version (CADE-Q SV). This questionnaire has 20 statements (4 domains: medical condition, risk factors, exercise, nutrition, and psychosocial risk), and a maximum score of 20. 29
Physical Activity
Participants were asked to wear a pedometer throughout the day for seven consecutive days to measure physical activity level. As a cut-off point, 7500 steps a day were considered compatible with the guideline recommendations suggesting at least 150 minutes per/week of physical activity in populations with chronic diseases. 30 To increase compliance of pedometer use, participants were provided with logs to record wake/sleep time and pedometer on/off time. In addition, a detailed instruction was provided on day 1 and frequent contacts with to remind participants of the importance of wearing the monitor correctly were done during the 7-day period.
Functional Capacity
The Six-minutes’ Walk Test (6MWT) was used to evaluate functional capacity, following recommendations of international guidelines.31,32 Each patient performed the test twice, with an interval of 15 minutes between them or until the physiological variables returned to resting levels. The test with the longest distance covered was included.
Food Intake
Food intake was evaluated by the adherence to the Mediterranean Diet, using the Mediterranean Diet Scale (MDS). 33 Scores range from 0 to 13: ≤5 are interpreted as low adherence to the Mediterranean Diet and ≥10 high adherence.
Self-Efficacy
The Bandura exercise self-efficacy scale was used. This scale includes 18 items that summarize situations that challenge the individual to maintain their exercise behavior. This is measured using a Likert-type scale ranging from 1 = not confident to 5 = strongly confident.34,35
Health Literacy
Health literacy was assessed using the Medical Term Recognition Test (METER) and the Newest Vital Sign (NVS). METER scores were based on the number of real medical terms that patients correctly identified (range: 0–40) and health literacy is classified as low, marginal and functional. 36 For the NVS, each correct answer (out of 6) equals to 1 point and health literacy is classified as adequate or inadequate. 37
Data Analysis
All statistical analysis was conducted using the Statistical Package for the Social Sciences version 26.0 (IBM Inc 2019, NYC). First, descriptive statistics were used to describe sociodemographic and clinical characteristics. The normality of data distribution was verified using the Kolmogorov-Smirnov test. Second, the Chi-square test was used for association between categorical baseline variables and U of Mann Whitney test was used to compare continuous variables, due to the non-normal distribution of data. The correlation between knowledge after the education intervention (post-test) and health behaviors, self-efficacy and health literacy was analyzed by Spearman’s correlation, since knowledge post-test did not present a normal distribution. For all these analyses, p < 0.05 was considered. To explore the preliminary effects of the education intervention in each subgroup independently, paired t-test or its nonparametric correspondent, Wilcoxon, were used. A Bonferroni correction was applied to control against inflated error due to multiple comparisons for the latter tests, such that a p < 0.002 was considered statistically significant. 38
Results
Respondent Characteristics
In total, 99 patients consented to participate and completed the assessments (Figure 1). Due to the service restriction and laws for risk groups imposed by the Covid-19 pandemic, it was not possible to carry out assessments of follow-up in 16 RE patients. Study sample by subgroups (n = 99). Legend: LTE: long-term enrolled patients; RE: recently enrolled patients. *They could not complete the follow-up evaluations due to the activities being suspended because of the COVID-19 pandemic.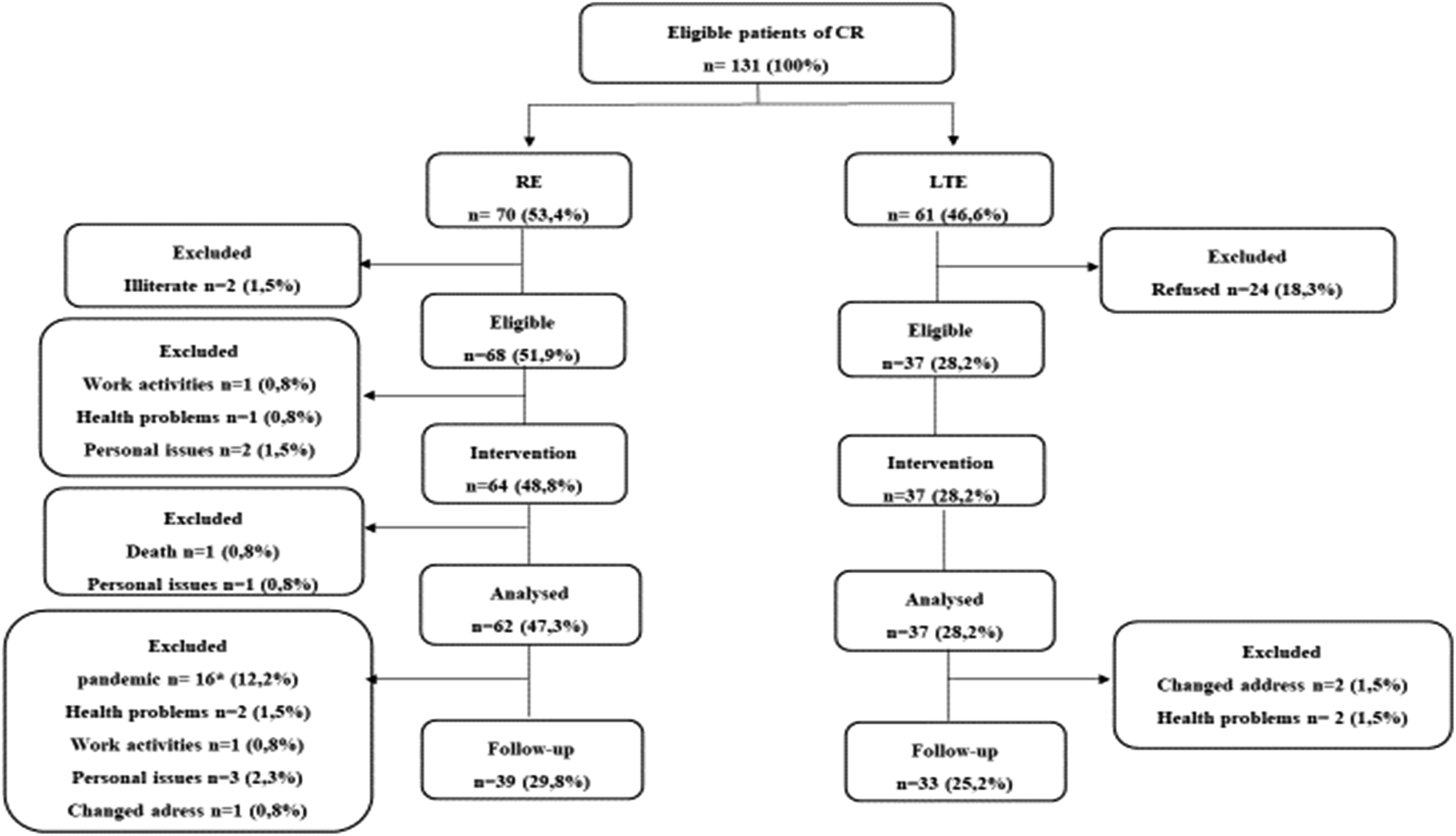
Baseline Characteristics of Pooled Sample (n = 99) and Subgroups.
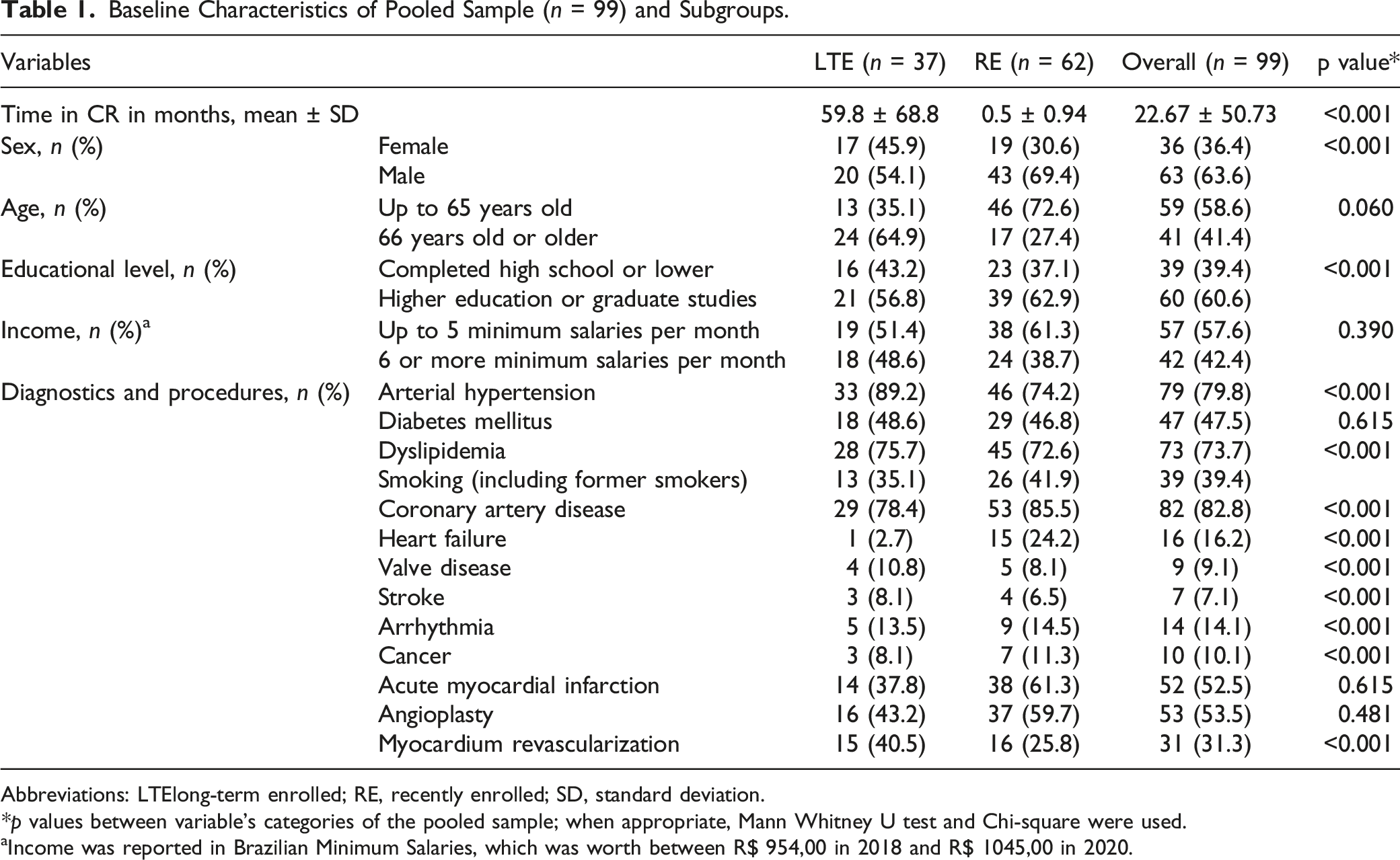
Abbreviations: LTElong-term enrolled; RE, recently enrolled; SD, standard deviation.
*p values between variable’s categories of the pooled sample; when appropriate, Mann Whitney U test and Chi-square were used.
aIncome was reported in Brazilian Minimum Salaries, which was worth between R$ 954,00 in 2018 and R$ 1045,00 in 2020.
Sociodemographic and Clinical Characteristics of Patients by Retention Status.
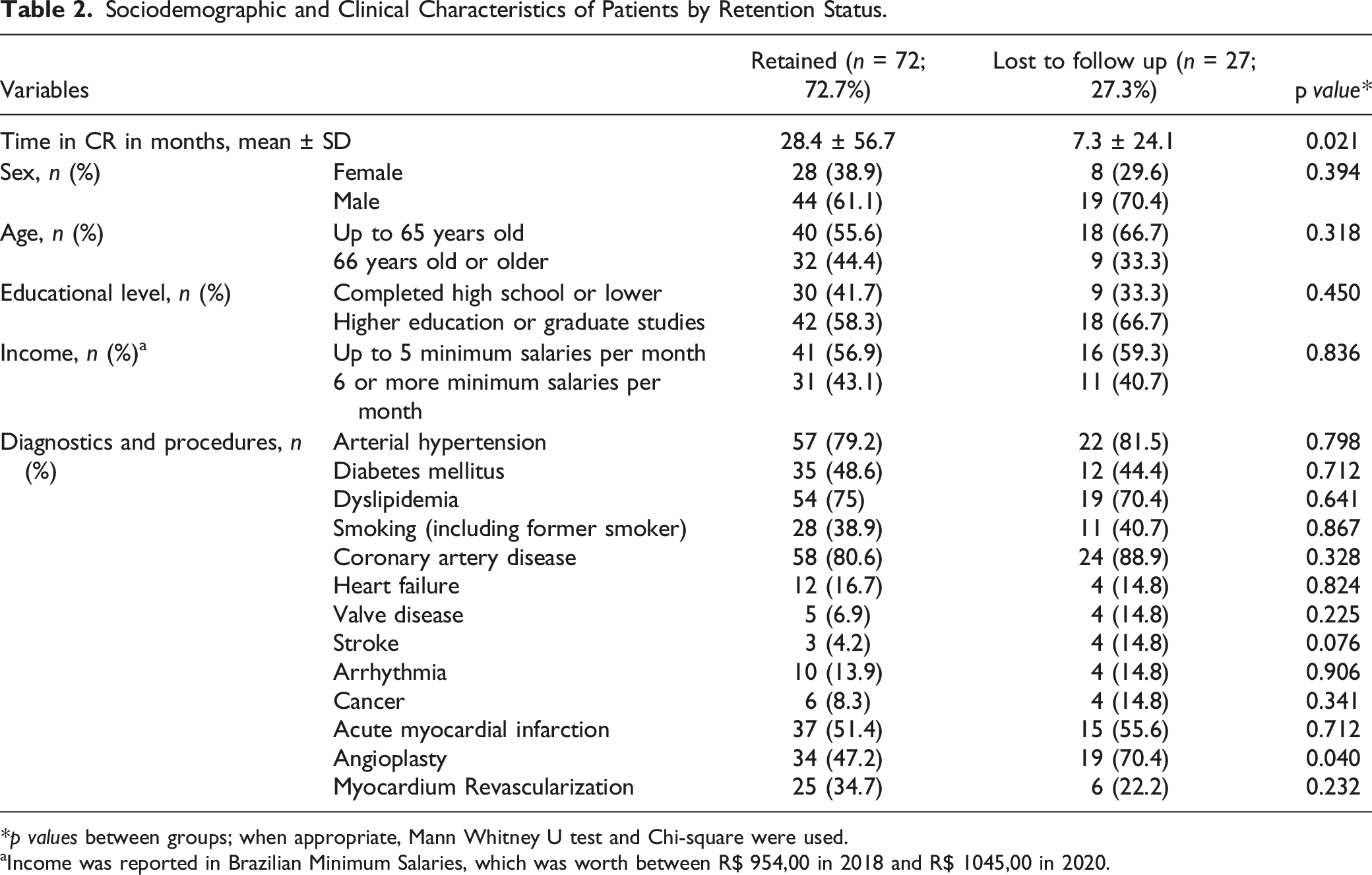
*p values between groups; when appropriate, Mann Whitney U test and Chi-square were used.
aIncome was reported in Brazilian Minimum Salaries, which was worth between R$ 954,00 in 2018 and R$ 1045,00 in 2020.
Impact of Education Intervention in the Pooled Sample
Pre-Test and Post-Test Comparisons of Knowledge and Behavior Change in the Pooled Sample (n = 99). a
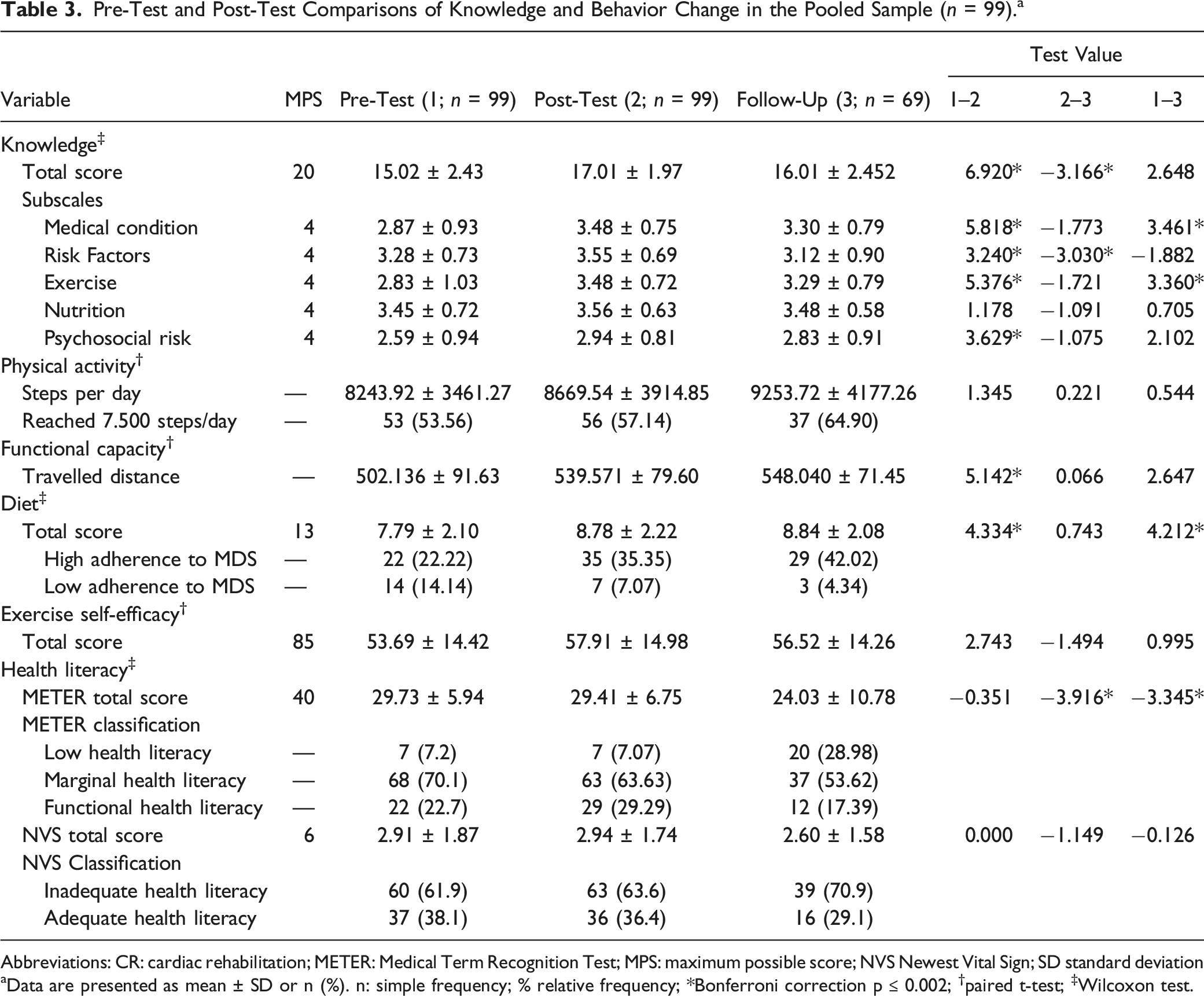
Abbreviations: CR: cardiac rehabilitation; METER: Medical Term Recognition Test; MPS: maximum possible score; NVS Newest Vital Sign; SD standard deviation
aData are presented as mean ± SD or n (%). n: simple frequency; % relative frequency; *Bonferroni correction p ≤ 0.002; †paired t-test; ‡Wilcoxon test.
Regarding the level of physical activity, there was no significant difference between the three assessments. However, it was observed that functional capacity measured by the 6MWT increased significantly post-test (p < 0.001).
The MDS score significantly improved post-test and this improvement was maintained in the follow-up. It was also observed that the proportion of participants that scored 10 or more in the Mediterranean diet increased over time, which indicates high adherence to this food pattern.
Finally, when health literacy was assessed using the METER instrument, there was a significant reduction of health literacy levels over time (p < 0.001). When health literacy was assessed by the NVS instrument, no significant differences between the three assessments were found. In regards to health literacy, more than 60% of the sample presented low health literacy at pre-test and there was no statistical difference over time.
Impact of Education Intervention by Subgroup Analysis
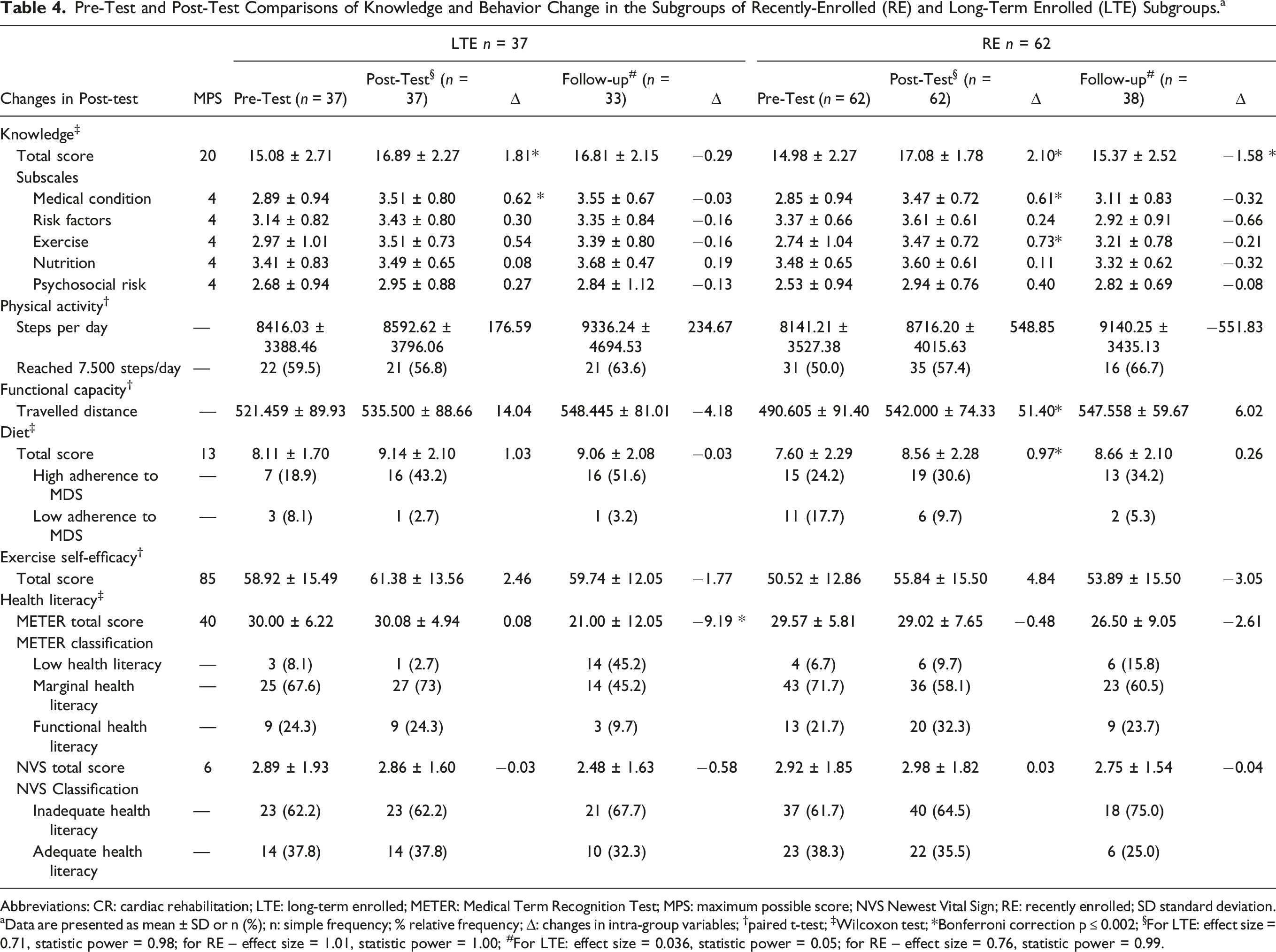
Pre-Test and Post-Test Comparisons of Knowledge and Behavior Change in the Subgroups of Recently-Enrolled (RE) and Long-Term Enrolled (LTE) Subgroups. a
Abbreviations: CR: cardiac rehabilitation; LTE: long-term enrolled; METER: Medical Term Recognition Test; MPS: maximum possible score; NVS Newest Vital Sign; RE: recently enrolled; SD standard deviation.
aData are presented as mean ± SD or n (%); n: simple frequency; % relative frequency; ∆: changes in intra-group variables; †paired t-test; ‡Wilcoxon test; *Bonferroni correction p ≤ 0.002; §For LTE: effect size = 0.71, statistic power = 0.98; for RE – effect size = 1.01, statistic power = 1.00; #For LTE: effect size = 0.036, statistic power = 0.05; for RE – effect size = 0.76, statistic power = 0.99.
In regards to physical activity, there was no significant differences between assessment points for both RE and LTE. It is observed that there was an increase in the percentage of patients who reached 7500 daily steps. Functional capacity increased significantly post-test only for the RE subgroup.
Dietary habits improved significantly post-test for RE only; however, the proportion of participants classified as high adherent to the Mediterranean diet increased in both subgroups. Exercise self-efficacy did not change significantly in any assessment point for both subgroups.
Finally, when health literacy was assessed using the METER instrument, a significant reduction was observed between post-test and follow-up for LTE participants, with no changes for RE ones. As for the classification, the number of participants in LTE and RE who presented marginal health literacy decreased in the follow-up, followed by an increase in the number of patients with low health literacy. No differences were found in the assessment of health literacy by the NVS.
Correlations Between Health Behaviors, Self-Efficacy and Health Literacy with Post-Test Knowledge
Correlations Between Health Behaviors, Self-Efficacy, Health Literacy and Post-Test Disease-Related Knowledge.
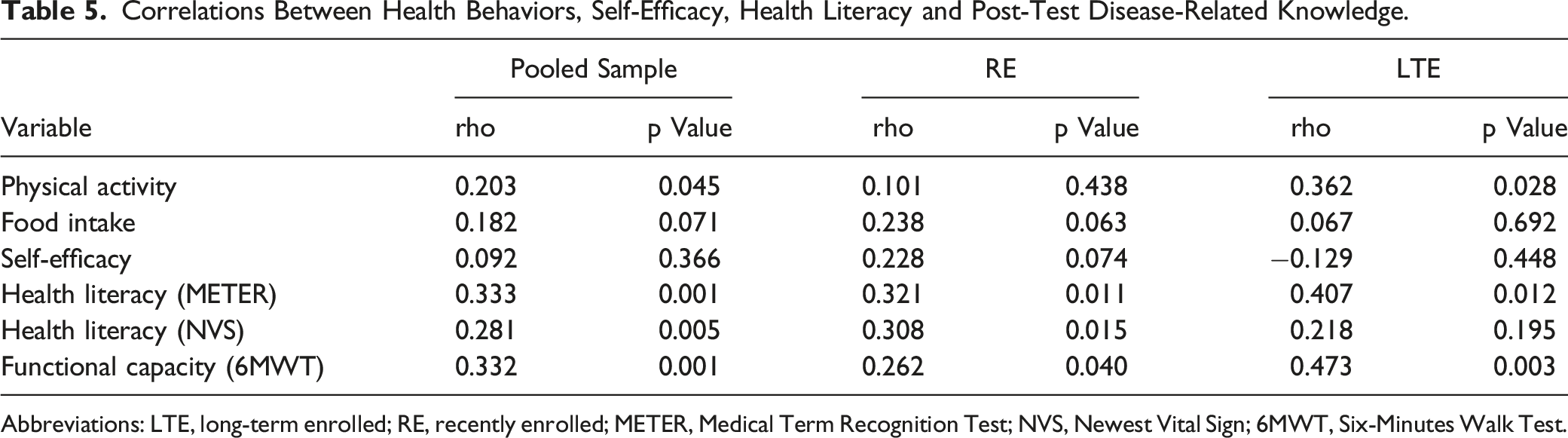
Abbreviations: LTE, long-term enrolled; RE, recently enrolled; METER, Medical Term Recognition Test; NVS, Newest Vital Sign; 6MWT, Six-Minutes Walk Test.
Discussion
The present study provides preliminary results that a structural educational program delivered to a pooled sample of RE and LTE CR patients can increase disease-related knowledge, functional capacity, and dietary habits in Brazil. Post-test knowledge was correlated to physical activity, functional capacity and health literacy. Results also showed that depending on the enrollment of patients in these programs, their responses to the education intervention are different, but mainly positive: even if patients are enrolled in the program for a certain period before the education was delivered an increase in disease-related knowledge and behavior change is observed. The lack of a control group is a limitation of this study; however, the relevance of these findings should be highlighted since there are few studies that address the effects of a structured education intervention for patients in CR programs in Latin America or low-income settings. To our knowledge, none of the previous studies in this area have analyzed the effects of a structured educational program in cardiac patients at different stages of CR enrollment.
The increase in knowledge post-test in the pooled sample as well as in each subgroup suggests that a structured education intervention may be needed to improve patients' knowledge about their disease, which can be one of the first steps for behavior change, along with intention, motivation and other types of self-efficacy. 11 Even patients in the LTE subgroup – which were coming on-site frequently for at least 5 months – improved their disease-related knowledge significantly, which shows that informal education may be insufficient to this purpose.22,39 However, considering that after the follow-up, knowledge of the pooled sample and RE decreased in relation to post-test, it is possible that the time of immersion in the educational program (3 months) may have been insufficient. Longer education programs (i.e., more than 3 months) or other strategies to promote retention of knowledge gained during the 3-months education program are warranted. In this context, Liu et al. 40 showed that prolonged educational programs, with at least 6 months of duration, can be more effective for cardiac patients.
Although nutrition-specific knowledge was not significantly improved during this study, MDS scores increased post-test and were maintained in the follow-up overall and in the RE subgroup. These findings are important since it has been observed that dietary behavior has a beneficial impact both on general health 41 and cardiovascular health.42,43 In addition, there was an increase in the proportion of patients considered highly adherent to the Mediterranean diet post-test in both subgroups. Whereas the Mediterranean diet has been indicated as one of the healthiest eating patterns, 44 the high adherence to the diet by post-test patients could be a reflection of the educational process, since education can influence patients’ food choices.15,33,45 However, such results cannot be corroborated by this study, since there was no correlation between MDS and knowledge post-test. In addition, the adherence to this dietary pattern at follow-up was not high, which has been shown in another study. 35
Functional capacity, a predictor of morbidity and mortality for CR patients,9,12,46 improved only in the RE, with maintenance of gains in the follow-up assessment, which corroborates with a previous study. 22 Although it was not observed significant changes of traveled distance between the two subgroups, the RE obtained an average increase of 52.17 meters, compared to 14.04 meters of the LTE. In this case, only the RE reached the clinically important minimum difference of 25 meters for coronary artery disease patients. 47 This can be justified by the fact that LTE participants were already trained for several months and the 6MWT measure was not taken from the start of CR, but the start of the education intervention. In untrained individuals (i.e. participants from the RE subgroup) the potential for evolution in functional capacity measurements is greater when compared to trained individuals (i.e., participants from the LTE subgroup). 22
Although it is already established in the literature that improvements in functional capacity is predominantly due to the physical exercise component of CR,48–50 our study provided some evidence that education may also contribute to these changes. Post-test knowledge was correlated to functional capacity. Knowledge may influence CR adherence, 51 and consequently improve functional capacity. A previous study in Brazil observed that both patients attending an exercise-based CR program and a comprehensive program had significant increases in functional capacity. 24 However, only the ones in the comprehensive program demonstrated a significant difference in relation to the control group. 24
Although it is well established that education interventions can promote changes in physical activity levels,15,18 this result was not found in the present study. However, it is noteworthy that the average daily steps of patients in both subgroups at pre-test was already high (7500 steps per day), 30 and that this condition was maintained, which can be considered a positive result, since the maintenance of beneficial physical activity levels is also an important objective of CR and not always achieved. 9 There was a positive and weak correlation between post-test knowledge and physical activity for the general sample and for LTE, which reinforces that disease-related knowledge can be a determinant for behavioral change. 15 In addition, the education level of the sample must be considered, since several factors can influence adherence and increases in the practice of physical activity, with individuals with higher education being more likely to exercise. 52
Health literacy, evaluated by the NVS, showed no significant difference post-test in the general sample and between subgroups. However, when evaluated by the METER, health literacy decreased at follow-up overall and in the LTE subgroup. It was also noted that most patients in both subgroups presented marginal or inadequate health literacy. In this context, other authors claim that patients with chronic diseases do not necessarily improve health literacy as during CR programs.53-55 Conceptually, adequate health literacy in the context of chronic diseases includes a constellation of skills that are critical to patients for managing their condition and navigating the health care environment and different contexts and potential causal linkages could exist. This is a complex relationship that needs further investigation, specially for patients in a middle-income country. In addition, health literacy of this subgroup is fragile, regardless of their length of stay in the program, in addition to being influenced by factors such as socioeconomic level, which may also have corroborated the lack of improvement in health literacy.56,57
Finally, the information generated by this study can serve to encourage the implementation of comprehensive programs. 4 Although we have not assessed patients’ satisfaction, it was possible to note a high interest in the education intervention from participants. They were very participative during the group classes, mainly on sessions related to diet, asking questions and making notes often. In addition, informal positive feedback was received and program had few absences. Adherence was assessed: in LTE was 100%; and in the RE, of the 68 participants, 64 (94%) completed the entire education intervention (i.e., attended all 12 sessions). Reasons for non-adherence included health problems, work activities and personal issues.
Caution is needed when interpreting these results since the present study has some limitations. First, there was no control group, which presents several threats to internal validity (history, maturation, testing). Therefore, a larger study using a randomized controlled design is needed to determine efficacy. Second, the study was carried out in a single CR program. It was not possible to reach the necessary number of individuals evaluated according to the sample calculation. Such restrictions limit the generalization of the results. In addition, discrepancies between number of participants in each enrollment subgroup could be associated with bias towards the much larger RE subgroup. Differences in disease profile and study retention could also reflect selection bias (e.g., LTE participants could be predisposed to superior retention because they have already demonstrated adherence to CR). Third, the evaluators were not blinded to the subgroup in which patients were inserted, due to insufficient staff on the team. Fourth, in addition to the fact that the follow-up was carried out after just 6 months, which may have influenced the assessment of the maintenance of the behaviors and knowledge of the subjects, the number of subjects evaluated in the segment was significantly lower due to the pandemic of the new coronavirus, which may also have influenced the results. Fifth, the MDS tool used to assess dietary behavior was not psychometrically validated in Portuguese at the moment of the research. In addition to including a control group, assessment of different education durations and outcomes (e.g., motivation) should serve as the basis for future research with other characteristics such as religion included to understand factors that influence outcomes and mixed methods used to assess impact of education interventions.
Conclusion
This preliminary study suggests the importance of structured education for patients attending CR programs. Significant increases and maintenance of knowledge in patients that were enrolled for a long term highlights the need for these interventions. Different stages of CR enrollment must be considered when designing education interventions. Overall, although more research is needed, the inclusion of the LTE subgroup in this study aimed to show that all patients can benefit from education while participating in CR and this core component should be offered to everyone, at any stage of CR enrollment.
Supplemental Material
Supplemental Material - Preliminary Effects of a Structured Educational Program in Cardiac Patients at Different Stages of Enrollment in Cardiovascular Rehabilitation
Supplemental material for Preliminary Effects of a Structured Educational Program in Cardiac Patients at Different Stages of Enrollment in Cardiovascular Rehabilitation by Rafaella Zulianello dos Santos, Andrea Scheafer Korbes, Christiani D. Batista Bonin, Ariany Marques Vieira, Marlus Karsten, Magnus Benetti, Paul Oh, and Gabriela L. d. M. Ghisi in Community Health Equity Research and Policy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by internal funds from Toronto Rehab Foundation.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.