
Abstract
Introduction:
Persons with disabilities are the most affected by rising pandemics worldwide. COVID-19 has affected people with disabilities in many areas of their lives; however, its impact has been overlooked. This study aimed to assess the effects of COVID-19 on people with disabilities in Plumtree, Zimbabwe, to develop a disability-inclusive approach in response to COVID-19.
Methods:
A concurrent mixed-methods approach was used to collect qualitative and quantitative data from 7 key informants and ninety-two participants with disabilities, from January to May 2023. Quantitative data were analysed using STATA software version 12 and Microsoft Excel. Multiple Logistic Regression, Chi-square test, and paired-sample test were used to test for associations among COVID-19 cases, source of income, key challenges, and demographic characteristics. Qualitative data were analysed and presented in the form of themes.
Results:
We recruited more females (56.5%) than males with disabilities, and more than half were unemployed (56.5%). In contrast, only 3.3% of the respondents were formally employed. The results also indicated a significant relationship between age and COVID-19 positivity (P = .025). The results also indicated that efforts were being made by government and non-governmental departments to assist people with disabilities during the pandemic through finance, food, awareness campaigns, and social support.
Conclusion:
Restriction measures put in place disturbed the livelihood of people with disabilities in Plumtree. Therefore, entrepreneurship programmes targeting vulnerable groups, including people with disabilities, should be introduced to ensure that their sources of income are sustained despite emergencies or pandemics.
Introduction
The COVID-19 pandemic has strained global healthcare systems and the economy. The pandemic impact was felt much more acutely in developing countries with weak economies to deal with its consequences, especially among vulnerable groups in society. 1 In the context of this study, disability encompasses physical, physiological, and psychological abnormalities or loss, such as persons who have had 1 or more arms amputated, are deaf or paralysed, have difficulty talking, and are blind. 2 These factors impair the body or mind, making it harder for the individual to engage in particular activities and interact with the environment around them.2,3 For example, measures necessary to prevent the spread of COVID-19, such as social distancing and hand washing. People with disabilities are left out of decision-making processes during pandemics, making them even more vulnerable to pandemics. 4 According to the Convention on the Rights of Persons with Disabilities, it is a mandate that all persons with disabilities enjoy all human rights and freedoms. As such, they should be included in decision-making and recovery strategies, particularly during humanitarian crises. 5
The world estimates that there are over 1 billion people with disabilities, and the COVID-19 pandemic has profoundly affected the population, causing socioeconomic inequities in communities. 6 People with disabilities face persistent structural disadvantages compared to the general population, such as barriers to accessing healthcare, increased poverty, reduced work, and reduced levels of education, which are further exacerbated by the measures adopted by various governments to combat the spread of the disease, such as restricting movements for a certain period.7,8
Considering that 80% of people with disabilities live in extreme poverty, especially in developing countries, this group remains the most vulnerable in the aftermath of COVID-19 containment measures. 9 Nonetheless, the COVID-19 pandemic has affected the health of disabled people in both developed and developing countries. During the first 2 months of the pandemic, a survey conducted in Wales and England revealed that two-thirds of people who died from COVID-19 had a disability, and it was estimated that disabled people had up to 11 times the odds of dying from COVID-19 compared to non-disabled people.10-12 It has also been mentioned that for all non-disabled women who die, 11 women with disabilities die, and for every man without a disability who dies, 6.5 men with disabilities die.13-15 People with disabilities have underlying issues that make them more susceptible to the virus, such as chronic conditions.16,17 According to WHO, people with other respiratory and chronic illnesses are more likely to contract COVID-19 and face far more health complications if they do. 18 Furthermore, a study conducted in the United States revealed that adults with intellectual and developmental disabilities (IDD) living in residential care settings were 2.6 times more likely to die from COVID-19 than the general population. Owing to the complications they pose, elderly people with disabilities are a distinct group that requires special attention during humanitarian crises.18,19
Although the general population remains at risk for COVID-19, people with disabilities are disproportionately affected. Prevention measures such as hand washing, improved hygiene, environmental and physical barriers, lack of protective clothing, and physical distancing recommendations do not consider that being disabled leaves 1 with no choice but to seek assistance, increasing the likelihood of exposure. 20 As of 2 May 2020 Africa has reported 39 749 COVID-19 cases and 1660 deaths, indicating that the pandemic is fatal. 21
Thousands of people with disabilities in Zimbabwe faced discrimination in different tribes during the pandemic. 22 Their situation was also worsened by the COVID-19 pandemic, which was first recorded in May 2020, when 178, 29 cases, and 4 deaths were experienced, leading to the government implementing the complete shutdown of the country lasting for extended months. 23 This study sought to assess the impact of COVID-19 on people with disabilities in Plumtree Town to ensure that a disability-inclusive approach could be adopted to achieve sustainable development.
Methods
Study area
Plumtree town is 100 km southwest of Bulawayo, the second-largest city of Zimbabwe. Lying in Matabeleland South Province, the town is 10 km from the Zimbabwe-Botswana border and 85 km from Francistown, Botswana. 24 According to council reports, there are 6 wards in Plumtree, with an estimated 8000 households and a total of 11 626 according to the 2012 census. 25 It is estimated that about 2000 travellers on normal days and less now due to restrictions set aside for travellers during the COVID-19 era pass through this border daily. However, despite the restrictions on travel, Plumtree Town residents remain at risk of contracting the virus spread from the border, and thus suffer from its devastating effects. See Figure 1:

Map showing Plumtree District wards.
Study design
A concurrent mixed methods approach was utilised from January to May 2023 for data collection, in which both qualitative and quantitative data were gathered. 26 A qualitative research method was adopted to focus on an in-depth understanding of key informants’ experiences, perceptions, and views on the impact of COVID-19 on disability and to interpret the collected data. The research design allowed for qualitative and quantitative tools to be designed and to assist in answering the broader research questions that this study sought to address. Moreover, the research design provided abundant data about real-life people and situations that gave meaning to the findings as far as the objectives of the study were concerned. Therefore, this research design is appropriate for obtaining a comprehensive overview of the probed variables of interest.
Target population
This study targeted 135 people with disabilities and key informants in Plumtree. This study targeted all persons with disabilities who were above the age of 18 and registered with an organisation called the Zimbabwe Chamber of Informal Economy Associations (ZCIEA), which works closely with people with disabilities in Plumtree. The age of 18 years and above was considered the ideal age group because, in Zimbabwe, anyone aged 18 and above is considered an adult who is capable of making decisions about their life as enshrined in the Constitution. Therefore, parental consent was not required to participate in such studies.27-29 On the other hand, the key informants targeted in this study included representatives of non-governmental organisations that implemented programmes that also targeted those living with disabilities. These included but were not limited to Plan International, and government departments such as Zimbabwe Republic Police, Ministry of Health & Childcare, Women Affairs, and caregivers who assisted in translating the questionnaires for people with disabilities just to mention a few.
Sampling
Rao’s soft sample size calculator (90% CI, 5% width of confidence, and 50% expected value of attribute) was used to obtain a representative sample of 101 people with disabilities from a target population of 135 people with disabilities. Participants were invited to the study by the Chairperson for Disabled People, who successfully mobilised them to provide the necessary information to the researcher. Those who could accept the invitation were used as study participants. However, to comply with COVID-19 regulations, participants met with the researcher in subgroups at a central location, and some participants, particularly older people and the blind, visited their homes. Key informants were purposively sampled.
Data collection procedure and tools
Questionnaire
A structured paper-based self-administered questionnaire consisting of open- and closed-ended questions with 4 sub-divided sections was used. The questionnaire was developed and pretested on 10 respondents and adjustments were made. The findings from the pretest were not included in this study as they were only meant for the validation and fine-tuning of the questionnaire. In cases where the respondents were unable to complete the questionnaire on their own, one of the researchers (involved in data collection) assisted them. The first section focussed on demographic information, age, level of education, form of disability, and employment status. The second section consisted of health-related information about the participants about COVID-19, and the third section included the psychological impact COVID-19 had on them. The last section aimed to assess the emergency response actions taken in Plumtree, which came as a rescue, and the challenges faced by people with disabilities during the pandemic. The data collection tool was translated into isiNdebele and Shona, 2 major indigenous languages spoken in the region. The researchers did not establish any relationship with the respondents and participants prior to this study.
Key informant interviews
The key informant interviews consisted of 6 questions, which were administered face-to-face with the aid of a tape recording device. The information obtained from the respondents was noted in the researcher’s notepad during interviews. The interviews were conducted in English, isiNdebele, or Shona, depending on the participants’ preferred language. Qualitative findings were used to provide more clarity to the quantitative findings; thus, data saturation was not considered a critical issue in this study, as we only sought generalised insight into the trends that we observed in our quantitative survey. 30 The interviews lasted between 30 minutes to an hour on average and the participants were shown the transcripts after transcription for confirmation.
Observations checklists
An observational checklist from the United Nations Country Teams (UNCTs) was adopted to assess the considerations in supporting disability inclusion in COVID-19 response and recovery in Plumtree.
Data analysis
Microsoft Excel was used to enter quantitative data, which were exported to STATA version 12 for further analysis according to the requirements of the objectives. Quantitative data collected using questionnaires were quantified and analysed using descriptive and inferential statistics. The output of the descriptive statistical analysis is presented in tables and graphs to denote key variables such as respondents’ demographic information. Chi-square tests, Paired Samples, Box and Whisker plots, and Multiple Logistic Regression were used to test the significance of the study and determine the associations between the variables of interest. Data collected using the interview guide were transcribed verbatim, categorised, and thematically analysed using MAXQDA Version 14. Coding was performed with the aid of a coding tree, and themes were generated and confirmed by all researchers as independent coders. The findings were then presented as the main and subordinate themes.
Trustworthiness
To establish trustworthiness in COVID-19 and disability studies, we met 4 key requirements: confirmability, credibility, dependability, and transferability. Trust is a critical component of research because it allows the research output to be authentic and reflects the outcomes under study. 31 Once trustworthiness is established, healthcare professionals can determine how qualitative research may affect their daily activities.
Results
A 68.1% response rate to the questionnaire was achieved with the aid of the disability chairperson, who managed to mobilise the respondents to provide the researcher with the information required for this study. The key informant interviews achieved a 100% response rate, as they all showed an interest in the study.
The socio-demographic characteristics of people living with disabilities in Plumtree Town
The findings indicated that a significant proportion of the disabled persons, 38 (41.3%), never went to school then, followed by (23) 25% who went to secondary, 22 (23.9%) went to primary, and only 9 (9.8%) went to tertiary. According to the findings in Table 1, most people with disabilities were unemployed (56.5%), while only 3.3% were formally employed, and 40.2% were self-employed.
Demographic characteristics and challenges faced by people with disabilities.

Cases of COVID-19 among people living with disabilities
The results indicated that 57 (61.9%) respondents did not test positive for COVID-19, while 35 (38.0%) tested positive for COVID-19. Among the people who tested positive for COVID-19, the highest proportion 14 (40%) was made up of those with no/deformed limbs, followed by 9 (25.7%) deaf. The results also indicated a significant relationship between age and COVID-19 positivity (P = .025). The results are summarised in Table 2.
COVID-19 and demographics.

Reference group.
Source of income pre-COVID-19 and lockdown
The results showed that the source of income for the majority of the 39 (42.4%) before the pandemic was vending (selling sweets, airtime, vegetables, etc.), and 16 (17.4%) of the disabled sources of income came from allowances from NGOs. The findings are presented in Table 3 and Figure 2.
Sources of income pre-covid 19 and during lockdown.

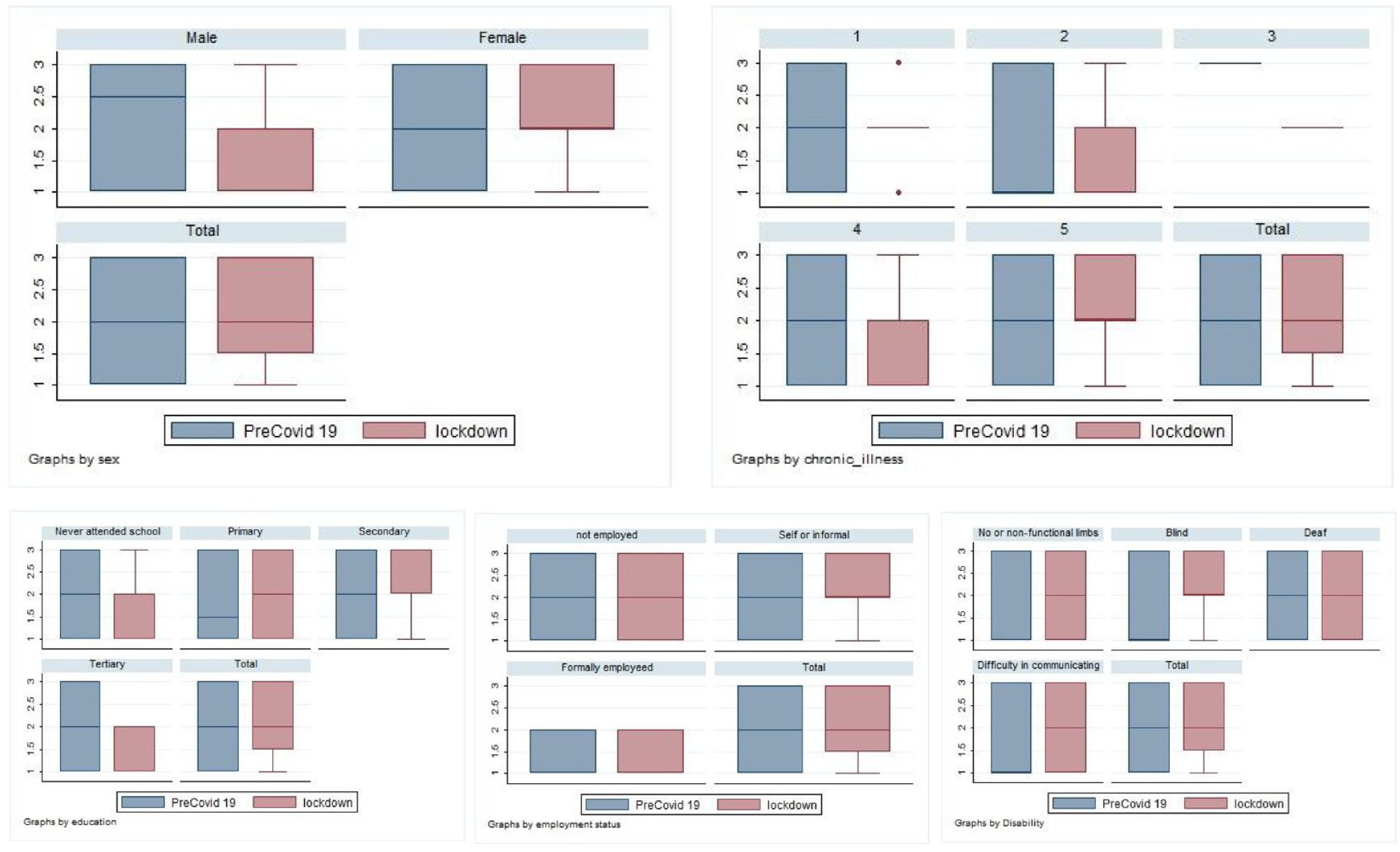
Association between source of income pre and during the COVID 19 pandemic.
Disability inclusion into socio-economic response
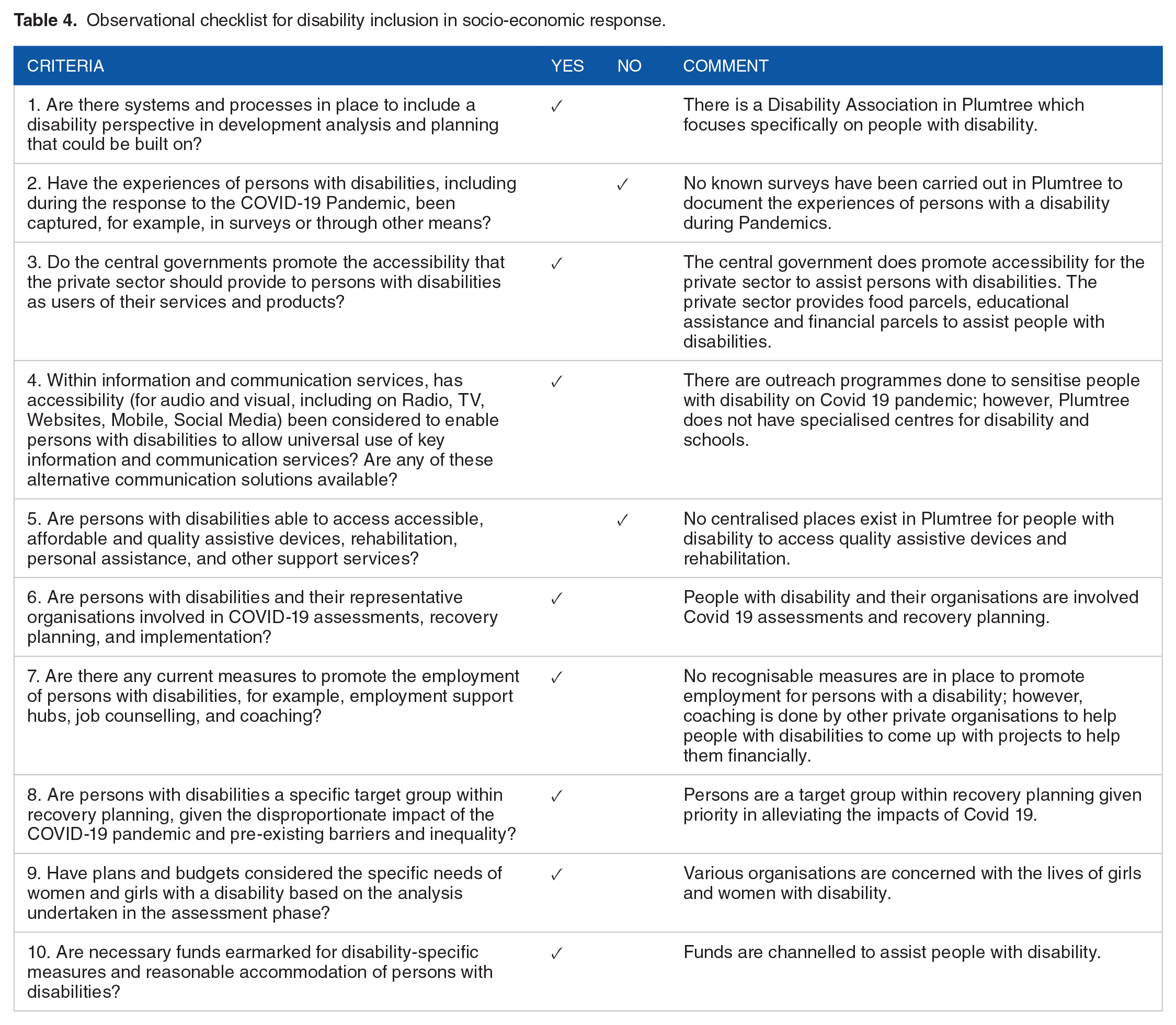
The findings indicated that people with disabilities had funds allocated to them earmarked for disability-specific measures. It should also be noted that various organisations have considered the specific needs of women and girls with disabilities in their plans and budgets. Table 4 presents the results.
Observational checklist for disability inclusion in socio-economic response.
Interventions that were implemented to assist people with disabilities during COVID-19 in Plumtree Town
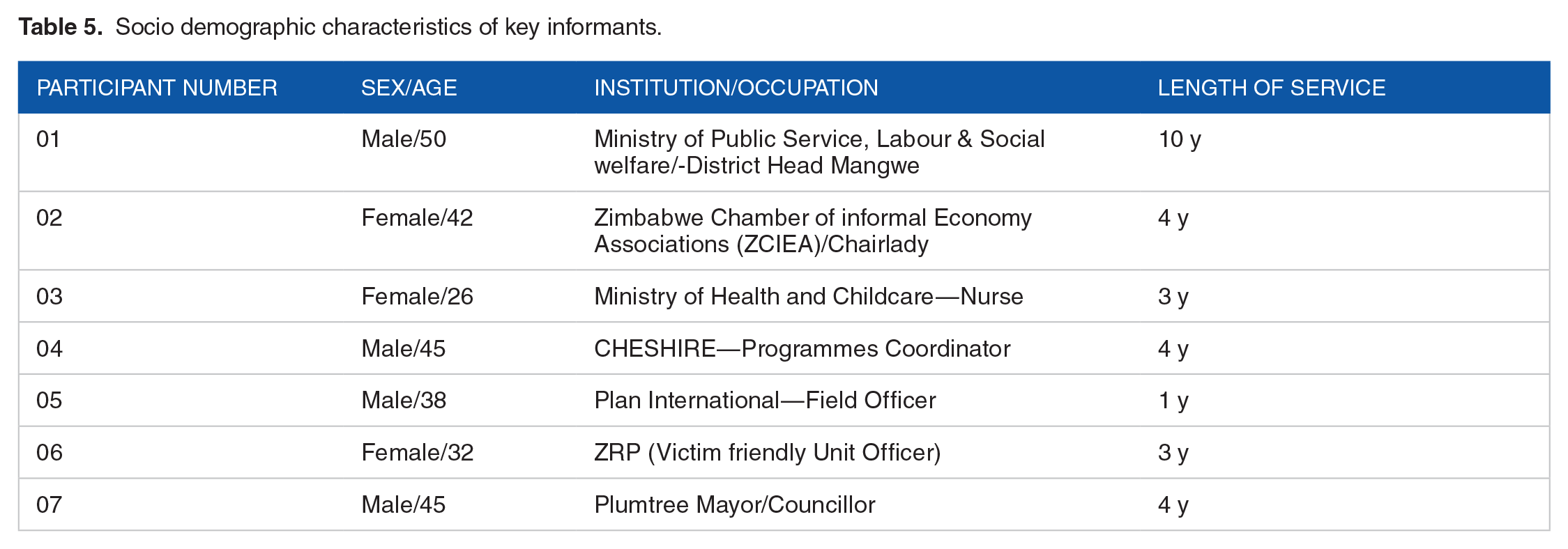
Six themes emerged from the 7 interviews. Of these 7 interviews, 3 were conducted telephonically because the key informants were not stationed in Plumtree and visited the site periodically to monitor the implementation of the programmes. The demographic characteristics of the key informants are presented in Table 5.
Socio demographic characteristics of key informants.
Awareness campaigns
The results indicated that educational campaigns were conducted to sensitise COVID-19 spread and prevention. Both governmental and non-governmental departments conducted these campaigns to protect persons with disabilities from contracting the virus. In an interview, the respondents indicated the following: ". . .we managed to conduct educational campaigns with different governmental departments such as Zimbabwe Republic Police, Ministry of Health and Childcare, and Social welfare to sensitise on COVID-19 spread and prevention among the vulnerable groups including the people with disability.".
Furthermore, the results indicated that non-governmental organisations also participated in COVID-19 to sensitise girls and women to sexual and reproductive health and rights (SRHR) services and communities to stop gender-based violence against people living with a disability. One respondent said;
“. . .We also managed to provide Sexual and Reproductive Health services to girls through guardians and counselling teachers as well as conducting educational road show to stop gender-based violence among the vulnerable groups including people with disabilities”.
The study findings also indicated that organisations used professional experts to disseminate information against the spread and prevention of COVID-19 among people with disabilities. In an interview, one respondent mentioned the following.
"..we are a Civil Society Organisation (CSO) targeting girls and women with disabilities. During COVID-19, we capacitated girls and women with disabilities with COVID-19 information using Disability Experts to disseminate information.".
Financial assistance
The results revealed that different organisations assisted vulnerable groups, including people with disabilities, with monetary support. The findings indicated that children in primary and secondary schools were assisted by monthly school fees. One respondent said: ". . .. . ..we provided financial support and well-paying school fees to primary and secondary children. We also began distributing PPE, sanitisers in schools in collaboration with other government departments.".
Another respondent from social welfare mentioned the following.
". . .we managed to support vulnerable groups with US$100, transferred into their netone cards".
Food assistance
The results also revealed that food parcels were donated to vulnerable groups including those with disabilities. They were in the form of cooking oil and mealie meal. One respondent stated, "we managed to give the elderly who are disabled food parcels; however, only four(4) managed to benefit from this intervention.".
Health care services
The results also indicate that people with disabilities, such as COVID-19 vaccinations, were provided with medical assistance. In an interview, one respondent mentioned the following: “. . .. . .. All the patients were diagnosed with COVID-19. During the COVID-19 period, we embarked on an outreach program targeting all wards to ensure everyone is accessing the COVID-19 vaccine."
The respondent further elaborated that they provided quarantine places for patients who were tested for COVID-19, as well as counselling.
"We gave medical assistance to patients that would have tested positive for COVID-19 by giving adequate advice concerning the virus or disease and providing quarantine places.".
Use of traditional medicine to treat COVID-19 in people with disabilities
This study revealed that traditional medicine was one of the major interventions used by the population living with disabilities to cure COVID-19 for those who tested positive for the virus. Most of the respondents who tested positive for the virus used traditional medicine. They indicated that;
"We used
Social support
The study findings also indicated that people with disabilities received social support from various stakeholders. During the COVID-19 period, people with disabilities faced gender-based violence, as mentioned in an interview.
"..we recorded three cases of sexually abused mentally challenged persons. However, the victims refused to go to the hospital for assistance.".
Discussion
The research findings showed that most of the disabled population in this study ranged between 45 and 59 years of age, and a few were aged 60 years and above. It has been reported that all age groups are at risk of contracting COVID-19. According to World Health Organization, 8 it is reported that older people face significant risks due to the physiological changes that occur with ageing. The results also indicated a strong significant relationship between age and COVID-19 positivity. This is supported by several studies indicating that the older an individual is, the higher the likelihood of contracting COVID-19. 32 As humans age, their immune systems deteriorate and they become vulnerable to infections. 33 This is generally exacerbated by living with disabilities, which further heighten vulnerability in various ways, ranging from limited mobility, limited access to services, and reduced reliance on oneself. The findings also showed that most people living with disabilities had never attended school. Other studies also reveal that people with disabilities are denied enrolment in schools in early childhood, which, however, has a direct link to employment in later stages.34-36 Only 3.3% of people with disabilities in this study were formally employed, which is in line with the findings of a study conducted by the National Association of Societies for the Care of the Handicapped 37 ; only 2% of people with disabilities work in the public sector, and less than 7% work at all.38,39 This is a cause for concern, as most organisations do not have inclusive policies that allocate certain quarters to people with disabilities, as they are often overlooked in the recruitment process.
The results indicated that only (38%) of the people with disabilities tested positive for COVID-19. The study findings are supported by other studies that reported that people with disabilities have a greater risk of being infected with COVID-19; they are less exposed due to reduced mobility. 18 This indicates that living with a disability limits mobility, depending on the nature of the disability, thus reducing exposure through contact with other individuals who might be infected in the communities. Among the respondents who tested positive for COVID-19, those with no limbs or deformed limbs constituted the highest percentage (40%). This generally might be explained by the fact that those with deformed limbs have challenges as far as mobility and performing their own tasks are concerned, as they must rely more on other people to assist them in getting by with their day-to-day chores and activities. This results in interaction which in turn increases the risk of infection. It should also be noted that some studies have supported this assertion, as they indicate that social distancing and self-isolation can be difficult for some people with disability.40-42 Furthermore, they need to be cared for and assisted in their day-to-day lives, rendering social distancing impossible, thus heightening their risk of contracting COVID-19. 43
According to the findings, before COVID-19, most people with disabilities (42.4%) earned their living through vending activities and received less from allowances (NGOs). The study further showed that people with disabilities were limited in terms of education, with the majority having no formal education, thus limiting their career prospects. In Zimbabwe, most organisations recruit employees with at least 5 ordinary level passes, including mathematics and English. This forces a significant proportion of people with disabilities to be informally employed or to rely on handouts or donations. According to Livermore and Bardos, 44 people with disabilities rely on informal activities to generate income because their illiteracy prevents them from being admitted to the formal sector. The findings of Ranabahu and Tanima 45 indicate that COVID-19 disrupts livelihood activities of people with disabilities, supporting research findings.
The study findings indicated that approximately 35% of people with disabilities had difficulty accessing healthcare services during the lockdown. During the lockdown period there were serious challenges associated with transportation and navigating these challenges with limited mobility could have been one of the factors that led to healthcare services being inaccessible to people with disabilities. People with disabilities may have other conditions that require regular visits to healthcare facilities for checkups and management. In this study, gender-based violence was noted as a challenge for people with disabilities during COVID-19. People with disabilities are the most vulnerable to violence during humanitarian crises. 46 According to some scholars, girls, and women with disabilities are more likely to be abused than their male counterparts. 47
Findings from this study indicate that the risk of contracting COVID-19 increases with age, and women are more likely to contract COVID-19 than their male counterparts. This finding needs to be considered during programming for the management of future pandemics, as a significant number of studies have found a correlation between age, sex, and susceptibility to communicable diseases.48-50 This would enable different stakeholders to strengthen their health systems through anticipation of inequalities that might increase the susceptibility of the different communities and create an environment (at individual, community, and institutional levels) that can decisively manage health risks and ensure access to health services for those in need. 51 This would ensure adequate preparedness to comprehensively and effectively deal with any future eventuality.
Strengths and Limitations
This study utilised a mixed-method survey that allowed for triangulation of findings and provided clarity on observed trends, thus providing a comprehensive outlook on the impacts of the COVID-19 pandemic on persons with disabilities. On the contrary, the researchers faced communication barriers with some of the participants during data collection, especially with people who were deaf or hard of hearing; however, caregivers helped the researchers communicate with the respondents. The questionnaire that was used in this research was developed and pretested by the researchers and it was not adapted or adopted from other standardised tools.
Conclusion
The findings of this study suggest that COVID-19 has affected people with disabilities in Plumtree. Most people with disabilities rely on the informal sector to make ends meet; however, the government’s measures to combat the spread of COVID-19 disrupted their operations and had a significant impact on their sources of income. Access to critical healthcare and education services is particularly difficult for people with disabilities during pandemics.
Supplemental Material
sj-docx-1-his-10.1177_11786329241274484 – Supplemental material for Effects of COVID-19 Among People With Disabilities in Plumtree, Zimbabwe: A Mixed-Method Survey
Supplemental material, sj-docx-1-his-10.1177_11786329241274484 for Effects of COVID-19 Among People With Disabilities in Plumtree, Zimbabwe: A Mixed-Method Survey by Lindiwe Ndlovu, Nicholas Mudonhi, Nomathemba Sibanda, Wilfred Njabulo Nunu and Norman Manyeruke in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241274484 – Supplemental material for Effects of COVID-19 Among People With Disabilities in Plumtree, Zimbabwe: A Mixed-Method Survey
Supplemental material, sj-docx-2-his-10.1177_11786329241274484 for Effects of COVID-19 Among People With Disabilities in Plumtree, Zimbabwe: A Mixed-Method Survey by Lindiwe Ndlovu, Nicholas Mudonhi, Nomathemba Sibanda, Wilfred Njabulo Nunu and Norman Manyeruke in Health Services Insights
Footnotes
Acknowledgements
Not applicable.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NM and L.N. conceptualised the research idea. L.N. crafted the objectives and developed the methodology and data-collection tools. L.N. collected data. N.M. coordinated the research process and drafted the manuscript. N.S. translated the data collection tools into Local Language (Isi Ndebele), captured the data into EPI DATA, and cleaned it in preparation for analysis. N.S. and WNN coded the data and performed the data analysis using SPSS version 23. L.N. produced the map of the study area. NM translated the data collection tool into Shona, conducted Key Informant Interviews, transcribed the data, and coded transcripts. All authors have read and approved the final manuscript.
Authors Information
LN was a former undergraduate student in the Department of Environmental Science and Health at NUST. NM is a Lecturer in the Department of Environmental Health at the National University of Science and Technology (NUST) in Bulawayo Zimbabwe. The author holds an Msc Degree in Environmental health and is a PHD in Public Health student at the University of Kwazulu Natal. NS is a Research Fellow in the Department of Environmental Health at NUST and holds an MPH and an MA. WNN was an Executive Dean and associate professor in the Faculty of Environmental Science at the National University of Science and Technology in Bulawayo, Zimbabwe. The author holds a PhD in Public Health and is an Associate Professor in the School of Public Health at the University of Botswana. Furthermore, the author is a Post Doctoral Researcher at the University of the Free State in South Africa. NM is a chairperson in the Department of Environmental Science and a PhD holder at the University of KwaZulu Natal, South Africa.
Ethical Statement
Ethics clearance was sought and granted by the Institutional Review Board at the National University of Science and Technology in Bulawayo, Zimbabwe. As required by the Declaration of Helsinki, a letter was granted to seek consent and voluntary participation from all the respondents. The participants were free to decide whether to participate or decline and were reminded that their participation was voluntary; refusing to participate while the interviews were in progress would not affect their care. Participation agreement was obtained only after the study was well explained to the participants. Consent forms were provided for participants to sign (written consent), indicating that they were willing to participate in the study. One of the principles of social research requires researchers to protect the integrity, right to self-determination, privacy, and confidentiality of research subjects’ personal information. Therefore, the anonymity and confidentiality of the participants were preserved by keeping their names and identities away from the research findings and reporting of the study. All principles of the Helsinki Declaration on studies involving human participants were observed and adhered to.
Consent for Publication
Not applicable.
Availability of Data and Material
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.