
Abstract
Background:
Traditional Health System has been reported to be the most accessible, affordable, and acceptable in resource-poor settings, particularly in Sub-Saharan Africa. It is utilised for different health needs, including pregnancy management. This study sought to explore traditional and Nurses’ perspectives on traditional medicine utilisation during antenatal care in Bulilima District, Plumtree, Zimbabwe.
Methods:
A qualitative survey was conducted on purposively selected nurses’ and snowballed traditional health practitioners who responded to unstructured interviews. Data were collected using a digital tape recorder, transcribed, and thematically analysed on Max Qualitative Data Analysis.
Results:
A total of 6 superordinate and 10 subordinate themes emerged from the collected and analysed data on both traditional practitioners and nurses. The superordinate themes associated with Traditional Medicine utilisation during pregnancy by women were: protective role, beliefs, shortening of labour, cleansing, accessibility, and collaboration between traditional practitioners and modern health practitioners. Nurses expressed their skepticism on the safety and efficacy of traditional medicine utilisation during pregnancy.
Conclusion:
Women utilise traditional medicines and remedies during pregnancy for different reasons, such as protection from evil spirits, foetus growth and shortening labour. There are concerns regarding their safety from the health service providers, although traditional practitioners share a different view. There is a need for investing in research that would ascertain the safety of these traditional medicines as this system has been a cheaper alternative for those who cannot afford or access modern health services.
Background
In developing countries, over a million women die of maternity-related causes each year regardless of well-known interventions to curb most pregnancy complications. 1 Despite the availability of modern health systems in developing countries, women continue seeking care from traditional practitioners during pregnancy. 2 These services are popular in Sub-Sahara African (SSA) countries because of accessibility, affordability and being readily available in the communities where people live. 3 Policymakers have raised negative publicity towards pregnant women who use traditional medicine, government officials, orthodox health professionals and researchers on the efficacy, quality, reliability and safety.4,5 Although there are concerns, Traditional Medicine (TM) continues to be widely used (prevalence >70%) by African women for maternal and reproductive health care. 6 Frequent traditional medicine users are pregnant women with no formal education, low income and living far from public health facilities. 7
Zimbabwe has two recognised health systems adopted after independence in 1980. 8 These are the Traditional Health Systems (THS) that are mannered by herbalists, traditional healers and traditional attendants as guided by different cultural norms and practices:8,9 the modern health system that is mannered by professionally trained health service providers and services obtainable in designated health facilities.3,8,9 It has been reported that most health service users prefer to utilise the traditional health system particularly in rural areas and other resource poor settings in the country as it is cheap and readily available at their local communities. 10
In Zimbabwe, most traditional health systems are in rural areas where there is a limited number of health facilities and inequity as far as the health service provision is concerned.11,12 Over 60% of the Zimbabwean population resides in rural areas characterised by underdevelopment compared to the urban setup.11,12 There has, however, been conflict between traditional health practitioners and modern health service providers about the boundaries and concerns of safety in as far as traditional medicine utilisation by patients is concerned, leading to differing views and the parallel running of these services.8,13,14 This study, therefore, seeks to explore Traditional Practitioners’ and Nurse’s perspectives on traditional medicine utilisation during antenatal care among women in Bulilima District, Plumtree, Zimbabwe.
Methods
Study area
Bulilima is located in Matabeleland South province and bordering with Botswana to the west in Region 5, prone to severe drought. 15 It has 16 clinics, 22 wards, and 94 361, with 54% females, with Kalanga and Ndebele being the dominant tribes. 16 The district has 1 main referral hospital with 16 clinics that usually refer pregnant women with complications to the district hospital and have an average household size of 5. 16 The average distance that women walk to the nearest clinic is estimated to be 5 to 10 km. The study area is illustrated in Figure 1.

Map of Bulilima District in Zimbabwe.
Study design
A qualitative survey was undertaken to explore traditional practitioners’ and nurses’ perspectives of traditional medicine utilisation on antenatal care among women in the Bulilima District. This design was adopted to enable rich data to be gathered and answer the research questions by providing in-depth explanations.17,18 Data was collected and analysed guided by the Consolidated criteria for reporting qualitative research (COREQ), a 32-item checklist for interviews and focus groups. 17
Target population
This study targeted traditional practitioners (involved in offering services to pregnant women) within a 3 km radius from the clinics. Traditional practitioners (TP) included but were not limited to traditional psychiatrists, Traditional birth attendants, herbalists, traditional surgeons, or other relevant individuals responsible for pregnancy management with the aid of traditional medicine, faith healers who used prayers, holy water, and other beliefs. 19 The study further targeted trained nurses offering maternal health-related services to pregnant women in the district. Initially, the researchers went to the field to establish the different types of traditional practitioners there and access the health facilities to determine the number of health practitioners that were relevant to the study. Sensitisation was then done in preparation for the actual data collection. The researchers had no relationship whatsoever with the participants.
Sampling
A total of 15 traditional practitioners who met the inclusion criteria were snowballed. The researchers had no prior knowledge of their numbers and that most are not registered with the Zimbabwe National Traditional Healers Association (ZINATHA). Purposive sampling was used to recruit 14 nurses responsible for maternal health service delivery within the 16 health institutions.
Data collection tools
An interview guide was used to guide the data collection process to ensure that sufficient data was gathered to fulfill the aim of this study. The guides were developed in the English language and then translated to isiNdebele, the major language spoken in this district. The structure of the interview guide for traditional practitioners comprised 13 questions probing the demographic characteristics, sources of income, and reasons for TM utilisation and complications associated with their use. The interview guide for nurses comprised six questions that sought to explore the services provided to pregnant women, challenges associated with access to these services by pregnant women and their views on traditional medicine utilisation, and the perceived complications associated with TM utilisation. The interview guides were pre-tested on two health service providers and two herbalists in Mangwe district, the neighbouring district. The findings were meant to be used to refine the tools further to aid accuracy in data collection. However, there were no adjustments that were made to the guide. The interviews (administered face to face) took between 15 and 30 minutes to be administered and were done at a place where the participants were comfortable, that is, at their homes, work places or any area that was convenient to them. The interviews were recorded using a digital tape recorder. The interview guides have been submitted together with this manuscript as supplementary documents.
Trustworthiness
This process is implemented to ensure that the whole inquiry process yields robust and accurate findings. 8 The following were taken into consideration during the conceptualisation and implementation of the research inquiry:
Credibility and dependability
To ensure that the research methods that were used provide trustworthy information, 8 a research proposal was reviewed by the Department of the Environmental Science and the National University of Science and Technology, where the research is affiliated to, independent reviewers reviewed the proposal and made recommendations that were taken into consideration (on the research, data collection, and analysis tools). The proposal was further reviewed by the Ministry of Health and Child Care (MoHCC) of Zimbabwe before permission was granted to conduct the study. Standardised data collection, analysis, and interpretation methods were also adapted from different authors.20,21
Conformability and transferability
In research, the findings of qualitative studies are put into context and confirmed by other authors.8,20,21 Though the findings of a qualitative study are maybe unique, ideas could apply to other different study settings.8,20,21 High levels of objectivity and honesty were observed in collecting, analysing, and interpreting the data.
Data analysis
Data collected were transcribed verbatim, coded, and thematically analysed on MAXQDA Version 14. Thematic analysis and coding were done using a hybrid of deductive and inductive methods as guided by the obtained data. The themes were derived from the data and were not determined upfront. 22 Obtained results were then presented in superordinate and subordinate themes supported by direct quotes from the participants. The theme development process was guided by the questions that were asked in line with the main aim of the study.
Results
Demographic characteristics
From a total of fifteen traditional practitioners, 7 were self-employed, 8 had >10 years treating people and their ages ranged between 40 and 67 years (average age 48). Of the 14 nurses who participated in the study, 7 were married, and all had an experience of fewer than 10 years. Their average ages ranged from 29 to 48 years (average age 37). Data saturation was reached after interviewing 10 traditional practitioners and 8 nurses. The demographic characteristics of the participants are captured in Table 1.
Demographic characteristics.

Traditional practitioners and nurses’ perspectives on traditional medicines
A total of 6 superordinate and 10 subordinate themes emerged from the data that was collected and analysed. The summary of these themes is presented in Table 2.
Summary of emerging themes.

Protective role
Two sub-ordinate themes emerged from the abovementioned theme: Minimisation of complications and management of diseases and enhancement of appetite. These subordinate themes are discussed in detail below.
Complications and management of diseases
Traditional practitioners cited that TM is utilised for different purposes, some of which are to minimise complications during the entire pregnancy and manage different diseases that occur during pregnancy. Participants reported that many complications arise during pregnancy, labour, delivery and different TM remedies are utilised to ensure no complications and management of diseases. However, on the contrary, nurses cited that TM utilisation by pregnant women brings about many complications as the medicines used do not have guides resulting in some women overdosing. The nurses also cited that the safety of these TMs has not been comprehensively investigated thus there are no guidelines in terms of dosages.
‘We grind the donkey placenta into powder and mix with boiling water, and the woman will drink then after some hours the uterus will come out’. ‘As pregnancy months increase the baby is supposed to turn head facing down but now if it crosses thus when massaging is done using petroleum jelly mixed with white ash till in the right position’. ‘We take white roots of uqethu (runner grass) and drink so that the fetus will turn head facing down’. ‘We use elephant dung as it is burnt, and they stand apart from the burnt dung so that you could sense and feel the smoke of dung. This prevents or eliminates bleeding during early stages of pregnancy’. ‘We have some different types of TM that we use to prevent infection; for example, during childbirth, we use TM such as umthunduluka (sour plum) to sterilize the umbilical code’. ‘Also if they had inyongo they drink Marula (umganu) as they put it in water and they will have running stomach and some come out through urine, there is also a limit of umganu (Amarula) as overdose might lead to complications. A pregnant woman is not supposed to go through ukuphoziswa (enema)’. ‘We use our convectional medicines like Oxytocin, Cytotec and we do fluid replacement depending on how much they have lost; for instance, if they have lost more than 400ml, blood replacement is done as we do cross match and see how much is the hemoglobin then transfuse’. ‘Some traditional medicine is good; it will be just smooth delivery, but you never know what they have taken; some mothers don’t say anything, but we can see as the contraction and dilation doesn’t go hand in hand’. ‘In most cases, African oxytocin make 3Ps (Power, Passage, and Passenger) not to correspond leading to uterus rupture either of too much power affecting dilation’.
Enhancement of appetite
Traditional Practitioners cited that they use TM to enhance appetite in women to increase their food intake. Participants reported that women are very choosy on the food they eat during pregnancy, which might have negative consequences on the foetus’s growth and development, resulting in some TM being ingested to improve the appetite and food intake. Nurses also concurred that some woman take multi-vitamins to boost their appetite. The participants said: ‘Women eat things according to their stomach preferences’, but I recommend food like Okra, dried vegetables and African chewing gum as it improves their appetite’. ‘Yes, some women usually take umdamoyo (multi-vite) to boost their appetite as the majority will not have an appetite’. ‘I think it’s best for pregnant women to eat food with all nutrients preferable vegetables, and they should avoid eating cold food’.
Beliefs
The second superordinate theme comprised 3 subordinate themes: Chasing away evil spirits; Prevention of negative consequences from the smell and Enhancement of embryo growth. These themes are explained in detail below:
Chasing away evil spirits
Participants cited that TM was also used to chase away evil spirits that can derail the pregnancy and lead to complications that may result in the loss of the baby and the mother. They also cited that enemies might use witchcraft and evil spirits to tie the pregnant women to have complicated pregnancies that could then claim their lives. Participants said: ‘We also use Eucalyptus Oil whereby I put 3 drops in water in the “name of the father, son and holy spirit” to chase evil spirits’. ‘We recommend them to buy petroleum jelly and mix with Ivimbela (white/red ointment) to chase evil spirits during the first months and massage the stomach with it so that nurses will not have a negative attitude towards pregnant women’. ‘Firstly, when people haven’t realised that a woman is pregnant, she will take a portion of soil from her footprint and put it in a cloth and tie it. When she is about to deliver thus when she will untie and put in water then drink’. ‘During the first month, pregnant women mix soil and their urine then dry it and tie in a cloth and untie when they are about to deliver to protect a woman from witchcraft and tying during the entire pregnancy’.
Prevention of negative consequences from the smell
One participant elaborated that pregnant women react differently to either bad or good smells and can easily vomit if not prevented and managed. The participant elaborated that there are traditional ways of preventing this from happening. The participant said: ‘They usual smell their armpits or put their hand under the armpit and smell that hand to neutralize bad smell’.
Enhancement of embryo growth
There were mixed feelings as far as this subordinate theme was concerned. Some participants felt that the utilisation of TM enhanced the growth and development of the foetus. In contrast, others felt that the development of the foetus was associated with supernatural powers from God. The participants said: ‘No! No! No! No one knows how to make the baby grow inside that one; it’s “nature from God”’. ‘We usually give them uMqathuva (Red star apple) to make porridge and also bathing close to granaries which are ladies place to stabilize the embryo (ukubamba umthondo). Baobab barks are taken and put in water overnight, and then women drink to make the baby grow and be strong like a baobab tree. Also, if the baby is born slim, we bath him with it to gain weight’.
Shortening of labour
Participants cited that different herbs have been used to speed up delivery and shorten labour, as revealed by traditional practitioners. They also reported that there are herbs that are used to lubricate the vagina to facilitate delivery. Participants said: ‘We burn donkey placenta and mix with water, and we also take roots of isikhukhukhu (snuggle leaf) facing Eastern side, and they drink it for fast delivery’. ‘We also use inkunzane (slippery herb) to wash the vagina to make it slippery during birth, and this herb is strictly not used for drinking’. ‘If pregnant women take that African Pitocin, labor last for 2hours or even 1hour, and sometimes it leads to complications’.
Cleansing
Participants cited that TM is used for cleansing the birth canal later in pregnancy, particularly in women who remain sexually active until the late stages of pregnancy. They cited that this cleansing is meant to prevent a scenario where a dirty baby covered with semen is delivered. Participants said: ‘Sex does not have any effect on pregnancy. . . . . .some man has strong sexual desire and stops even just a few days before labor, which makes nurses complain about dirty babies’. ‘It depends on people, and their sexual appetite differs, but umthunduluka (sour plum) leaves clean everything before birth even sperms as it is believed that the baby will be carrying those using head’.
Accessibility
Two subordinate themes emerged from this superordinate theme: Payment options available for the services and designated huts for delivery. These themes are further explained in the sections below:
Payment options available for the services
Participants reported that not every pregnant woman pays for their services the majority of the time. However, nurses indicated that women are attended to free of charge for 72 hours after their delivery. During pregnancy, women are expected to pay registration fees in health facilities. Participants further elaborated that with the traditional practice, there are varied payment options other than monetary. Participants further reported that these available options and payment flexibility enabled women to have access to the services of traditional practitioners, thereby improving their chances of delivering healthy babies. Participants said: ‘. . .pregnant woman they don’t pay anything since the majority will be stressed as other males deny pregnancy, others being impregnated by others husband and relatives’. ‘They pay isimbo (consultation fee) in the form of money, goats, grains depending on the pocket of a person. Also, they pay umkhonto (token of appreciation) in the form of a goat when the child starts having milk teeth to show appreciation’. ‘They pay money for the eyes of the grandmother but with no specific amount but according to your condition/pocket but it’s just small might be $1 or $2 for appreciation’. ‘We also monitor those women with problems such as high blood pressure. We also monitor post-delivery, usually 72 hours. Still, nowadays, because of circumstances beyond our control, we can no longer keep them for those hours unless they pay for the additional days required to be at the health facilities. You should also note that women are expected to pay the registration fees during pregnancy so that they have medical checkups done periodically’. ‘Maternal health is for free, and currently, there is an NGO (Global Fund) that is funding, us as nurses we are given US$10 per delivery service’.
Designated huts for delivery
One participant highlighted that in the traditional practice, there are huts that are designated for delivering. These are cleaned using TM to ensure that the house does not pose any risks of infecting the mother and the baby during the delivery process. The participant said: ‘. . .grandmothers built huts that are specifically for labor which is polished using dagga and cow dung and no one is allowed to enter that house to maintain its cleanliness’.
Collaboration between traditional practitioners and modern health practitioners
A total of 2 subordinate themes emerged under this superordinate theme. These are explained in-depth below.
Potential for collaboration
Traditional practitioners indicated no problem working in collaboration with the modern health system as they noted that some problems are beyond nurses/doctors’ capabilities that need their intervention. The participants highlighted that both the Traditional and Modern Health systems are recognised; however, they faced challenges in renewing and legalising their practice. On the contrary, some nurses felt there is no need to infuse these 2 systems. They did not believe in the TM’s efficacy that these women utilise during pregnancy, while others advocated for the collaborative efforts as they felt some TMs work. Participants said: ‘I can work with hospitals because in most cases, pregnant women that have been failed by the hospitals such as those failing to urinate and those with cancer usually come to me’. ‘I am a registered healer among top eight healers in Matabeleland South and was given the certificate to help pregnant delivery, but now they don’t want to renew it don’t know why?’. ‘Those women who use African Pitocin will be having more complications since they don’t have specific dose; you will find that the patient will come with 500ml bottle of concoction and will drink all’. ‘No, we are not allowed to refer patients from hospitals to traditional healers unless some nurses who are talented they can tell that this problem is beyond their control and recommend secretively even though it’s not advisable’. ‘It is possible to work together with the traditional system, but the problem is that some traditional healers say their knowledge and training comes from Ancestors thereby making their services to be paid for, which makes it difficult to work in conjunction’.
Counselling to discourage TM utilisation during pregnancy
Counselling was noted as one of the activities done by nurses on women who utilise traditional remedies. Participant cited that they usually discourage women from taking TMs as their efficacy and safety are unknown and could potentially introduce complications.
‘We give them counseling and health education but sometimes according to culture, the belief that so there is no way we can prevent it’.
Research
Nurses felt that there is a need for comprehensive research to be done on the efficacy and safety of the TM that women normally use during pregnancy. They felt that this would aid confidence and understanding of the issues surrounding these TMs. As such, the women would be able to make informed decisions, and (nurse) will also be able to make informed decisions on whether or not to recommend the usage of TMs during pregnancy. The participants said: ‘I think if their medicines have a proper dosage and also a lot of research is done on their use, it can be used, but I think for now they need thorough research’. ‘I think on safety I would not recommend; I say they are not safe for now unless there are proper recommendations as we can see more complications than good things’.
Traditional medicine and concoctions used during pregnancy
Participants stated many traditional medicines used and their reasons. The most predominant are Nyeluka (water snake/fish), donkey placenta, elephant dung, holy water, and holy tea, as indicated in Table 3.
Traditional medicine used during pregnancy.
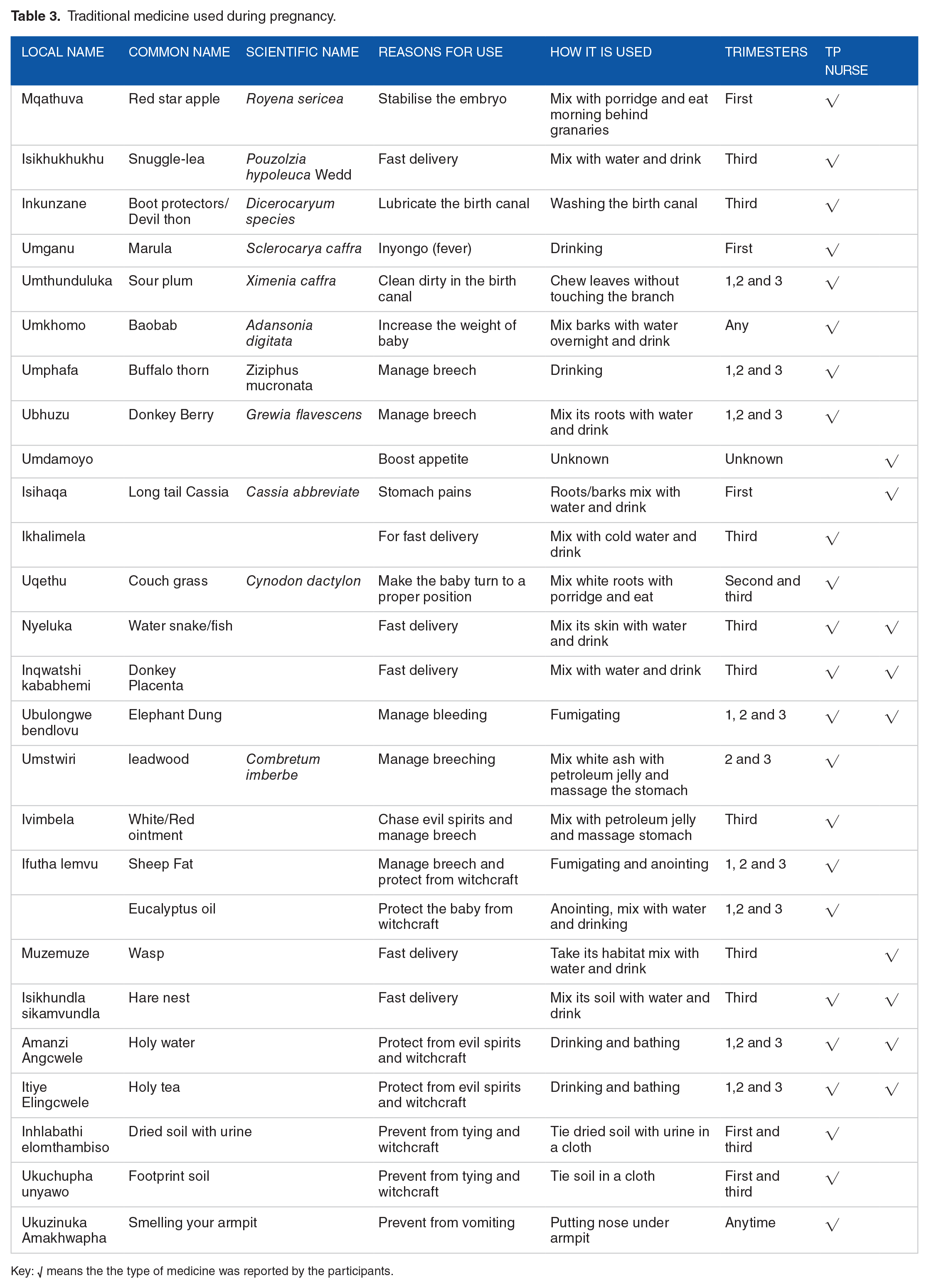
Key: √ means the the type of medicine was reported by the participants.
Discussion
Most traditional practitioners had attained at least an ordinary level and have >10 years of healing. In comparison, nurses majority have <20 years of experience in the health sector. Literature reveals that traditional practitioners’ educational level varies as some have attained primary, secondary and tertiary level.23,24 Our findings contrast with other studies that showed the experience of traditional health practitioners ranges from 5 to 10 years. 25
Bleeding was one complication that traditional practitioners manage through fumigating elephants dung as pregnant women stand apart from the smoke naked under their observation. In addition, the study noted that elephant dung was mixed with water and drank to quicken delivery among pregnant woman. These findings are similar to different scholars who revealed that women use elephant dung to manage bleeding or quicken labour.26,27 Also, traditional practitioners (TP) highlighted that pregnant woman easily vomit due to bad or good smell, which is prevented by smelling their armpits. Studies are against the notion revealed by the results as they suggest that they are chemical methods used to control odour rather than smelling of armpits.28,29
The study noted that traditional practitioners could chase away evil spirits that usually make nurses have negative attitudes towards pregnant women affecting the delivery process. Some mechanisms of chasing evil spirits from the study are similar to studies conducted by Aziato et al 30 and Mudonhi and Nunu 31 who highlighted anointing oil, blessed water, sticker, blessed white handkerchief, blessed sand, Bible and Rosary. Furthermore, studies conducted in Islamic tradition revealed that prayer is a weapon to chase away evil spirits. 32 Findings show that witchcraft in the form of tying constantly appears, which is prevented by taking dried soil mixed with urine or footprints and tying in a cloth and untie during labour. 33 This is supported by studies conducted by Chamisa 27 who found out that urine with soil and footprint mixed with other herbs prevent pregnancy tying.
Nurses revealed that those who utilise traditional medicine resemble more complications than those in conventional medicines. Also, health practitioners acknowledged that some woman who utilises TM deliver safely without any complications. Several studies concur as they highlight that traditional medicine leads to complications that result in maternal morbidity and neonatal death. 34 Others show that they lead to safe and fast delivery. 26
Traditional practitioners noted that if there are no complications, women can deliver safely at home, but they should deliver at the hospital if there are complications. The World Health Organization 35 suggests that delivery at home is safe under a skilled, well-trained birth attendant. On the other hand, health practitioners recommended birthplace to be at the hospital to manage unforeseen complications. This is supported by studies that reveal concerns towards home birth as they advise hospital births even though there is no law restricting home births.3,36
Many herbs were noted in the study that is used during pregnancy, such as umganu (Marula: Sclerocarya caffra) and isihaqa (long-tail cassia: Cassia abbreviate) to cure diarrhoea and inyongo (fever). Still, they indicated that overdose leads to complications. This is supported by the study conducted by Eloff. 37 that found that inner barks of Marula have antibacterial activities towards microbes such as Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, and Enterococcus faecalis which are prime causes of diarrhoea. The study showed that ukuphoziswa (enema) is strictly not allowed among pregnant women. Despite our results discouraging, literature shows that some pregnant women still practice it. 38
Based on the study’s traditional and nurses’ perspectives, isikhukhukhu (Snuggle-lea: Pouzolzia hypoleuca Wedd), donkey placenta and inkunzane (Boot protectors/devil thorn; Dicerocaryum species) where most predominately African oxytocin used to induce and shorten labour. Different studies were obtained, which showed that donkey placenta and isikhukhukhu (Snuggle-lea: Pouzolzia hypoleuca Wedd) were used to induce labour.26,27 Also, nurses revealed that African Pitocin reduces labour to about 1 or 2 hours. In most cases, for those who utilise traditional medicine, the dilation and contraction will not correspond. Studies reveal that these African Pitocin quickens and induces labour but not necessary stating the exact timeframe. 26
It should be noted that indigenous knowledge plays a major role in ensuring that women in poor resource settings have access to health services. However, there are still arguments regarding its safety and efficacy. 39 However, there is a window of opportunity to foster collaborative efforts between the Traditional Health System and The Modern Health System.8,24,40 This could be achieved by eliminating cultural barriers that hinder collaborative efforts between the 2 health systems and improve information sharing and tolerance.8,41,42
Limitations
This study cannot be generalised to the entire country since the study population was rural-based and traditional medicine can differ depending on geographic location. The study was not funded, and as such, there is a need to look at a bigger population.
Conclusion
Traditional and health practitioners acknowledge that traditional medicine is used during pregnancy for different purposes even though their perspective differs regarding their utilisation. Most traditional remedies were used in the last trimester to quicken delivery. Health care professionals should routinely include herbal medicines when asking about the patient’s drug use rather than recognising contraction and dilation that is not corresponding, which aid in determining that someone used traditional medicine. Women are a valuable asset in any nation; therefore, this subject of TM should be treated as something delicate to foster better antenatal health since there are concerns regarding their safety. There is also a need to conduct more research that explores the efficacy and safety of TM and its utilisation during pregnancy.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors Contributions
NM conceptualised the research idea. The author also collected and analysed qualitative data. NM designed the methodology and data collection tools. The author also translated the data collection tool to the Local language (isiNdebele). WNN refined the idea and, together with NM, drafted the manuscript. The author also coordinated the manuscript writing process. WNN performed data analysis on MAXQDA. All the authors read and approved the final manuscript.
Ethical Approval and Consent to Participate
Permission to carry out the study was sought from relevant authorities such as the Provincial Medical Director for Matabeleland South, District Medical Officer for Bulilima, and the National University of Science Technology, particularly Environmental Science Health. Moreover, the research abides by the Nuremberg code and principles stated in the Helsinki Declaration for the safety of participants involved in the study. 43