
Abstract
Introduction:
Chronic low back pain (CLBP) is a debilitating condition that affects millions of people worldwide. Healthcare providers play a crucial role in improving access to care for patients with CLBP, but they face numerous challenges in doing so. This study focuses on healthcare provider perspectives of CLBP healthcare access.
Methods:
Semi-structured interviews were conducted with 16 healthcare providers across a variety of disciplines who care for people with CLBP across Saskatchewan, Canada. A qualitative interpretive research approach with inductive thematic analysis was employed.
Results:
Years of experience ranged from 1 to >20 years. Participants represented 11 disciplines across urban, rural, and/or remote settings. Four overarching themes were identified: (1) Challenges for healthcare providers; (2) Anticipating and recognizing barriers and consequences for patients; (3) Facilitators for healthcare providers and patients; (4) Recommendations on improving accessibility to healthcare. Several barriers were identified for healthcare providers to provide optimal, evidence-based care across Saskatchewan, including patient complexity and past experiences, access to resources and coordinating care. Healthcare providers recognized barriers for patients, which ultimately influenced healthcare provider decisions and care provision. Coordinated care and funding were identified as facilitators that support healthcare provider recommendations of multidisciplinary care and improving provider education to enhance provision of care for chronic low back pain.
Conclusion:
Future care models should build on these identified factors, while considering clinical and community-specific contexts.
Introduction
Chronic low back pain (CLBP) is a widespread and costly health problem that affects approximately 80% of adults at some point in their lives. 1 It is the leading cause of disability worldwide 2 and is associated with significant economic burden due to lost productivity and healthcare costs. 1 Although a range of treatments are available, the prevalence of CLBP has remained stable with many people continuing to experience ongoing pain, disability, and reduced quality of life. 3
A wide range of healthcare providers have crucial roles in improving access to care for people with CLBP, but they face numerous challenges that can result in inconsistencies in care delivery. The recommended approach to CLBP management is to discourage use of pain medication, steroid injections and spinal surgery, and instead promote physical and psychological therapies.4-8 Despite the availability of evidence-based guidelines for the management of CLBP, many health systems are fragmented and not designed to support a multidisciplinary approach to guideline concordant care and many healthcare providers face significant barriers in providing optimal treatment for this condition.4,9 Some challenges identified in the literature include lack of access to suitable therapies, lack of time and training, and lack of funding. 4 This is exacerbated for healthcare providers serving in rural or remote communities.
In Canada, the healthcare system has publicly funded universal coverage for essential medical services to all citizens and permanent residents, with each province and territory managing its own healthcare system adhering to the Canada Health Act. 10 However, many services for musculoskeletal conditions and chronic pain do not fall under this universal coverage. Some Canadians have additional health insurance that would help to cover costs of care options like physiotherapy services, which are typically not covered through the public health system. 11 In Saskatchewan, healthcare delivery faces unique challenges due to its diverse geographic landscape, encompassing urban, rural, and remote areas, with 36% of residents living in rural and remote areas, and 17% of the population being Indigenous. 12 In conjunction with reduced access and limited resources to support publicly-funded services, Canadian physicians have identified key challenges in rural settings, including a lack of interprofessional team support. 13
Indigenous peoples are 30% more likely to experience chronic low back pain, 14 while facing unique and substantial barriers to accessing healthcare, including interdisciplinary and rehabilitation care.15,16 Several interdisciplinary care models recommend inclusion of non-medical care providers like physiotherapists or chiropractors, in addition to trauma-informed care strategies within primary care settings17-21 and others are investigating proposed approaches to overcome access barriers.22-25 However, there are few known interdisciplinary care models focusing on addressing the unique needs and context of rural, remote or Indigenous communities in Canada. 24 Development of appropriate models of care and improved access for rural, remote, and Indigenous people requires a deeper understanding of how the various disciplines currently deliver care, including barriers and facilitators to following best-practice interdisciplinary care models.
The objective of this study was to explore the experiences of healthcare providers working with patients seeking CLBP care. We particularly aimed to explore facilitators and barriers to CLBP care (or access to care) and make recommendations to improve access to care.
Methods
This study was approved by the University of Saskatchewan Behavioral Research Ethics Board Beh-REB #1973.
The methods used in this study describe phase one of a multi-phase study, in which the protocol and methodology have been published. 26 For this phase, purposive sampling was used to recruit 16 Saskatchewan-based healthcare providers (eg, physician, nurse practitioner, physiotherapist, psychologist, etc). Inclusion criteria included: having any experience in treating CLBP in Saskatchewan across rural, remote, or urban settings. Recruitment aimed for a diversity of healthcare provider types as well as a range of practice settings (rural, remote, urban, Indigenous and non-Indigenous), reflecting Saskatchewan’s geographical dispersion. Recruitment was stopped when provider type became redundant, and data saturation was probable. Healthcare providers went through a screening and informed consent process, followed by an online survey on type of service provided, specialization and years of experience. Initial screening was completed by telephone or e-mail after healthcare providers contacted the research team expressing interest to participate. Healthcare providers received a paper or electronic consent form based on their preference. Consent was verified online prior to completing the online survey, and verified again at the beginning and conclusion of the interview process. Healthcare providers also provided postal codes for the settings in which they provide care. Geographic classification of rural, remote, and urban practice settings was determined by postal code and reference to the metropolitan influenced zone (MIZ) classification developed by Statistics Canada and outlined in our study protocol paper. 26 Survey data was collected using REDCap (Research Electronic Data Capture), a secure online survey tool and research database application hosted by the University of Saskatchewan.27,28 Following REDcap requirements, survey forms were thoroughly pre-tested before moving to production mode. Interviews were conducted virtually (Zoom or telephone) by 2 research team members (KC and AI) to explore experiences in providing care and the perceived access barriers and facilitators for their patients. KC is a postdoctoral fellow with experience and training in patient-oriented research, and culturally responsive care. She is physiotherapist with 11 years of clinical experience, working in urban, rural, and remote communities in Saskatchewan. AI is a research associate with a Masters in Public Health. Her training and work experience over the last 7 years has focused on qualitative community-based Indigenous health research and improving access to care for chronic diseases among diverse populations across Saskatchewan. Semi-structured interviews were conducted between January and August 2021, using an interview guide (Appendix I). Interviews were audio-recorded and transcribed. The average length of the interviews was 37 minutes. Data were analyzed using NVivo 12®. Thematic analysis was conducted following Braun and Clarke’s 29 approach, beginning with preliminary code development for the entire data set (RM and HA), followed by discussion and evaluation with periodic meetings by the research team (BB, SL, KC, AI, RM, HA) to identify patterns and potential themes. Once the themes were identified, a check was carried out to identify adequate representation of the themes with quotes and the entire data set. Subsequent meetings were held with the research team, including patient partners, to further interpret and refine themes with select representative extracts. Trustworthiness was enhanced through an audit trail, as well as member-checking in the context of participant review of transcripts. Participants were provided their written transcript and were able to make alterations to their data prior to data being analyzed.
Results
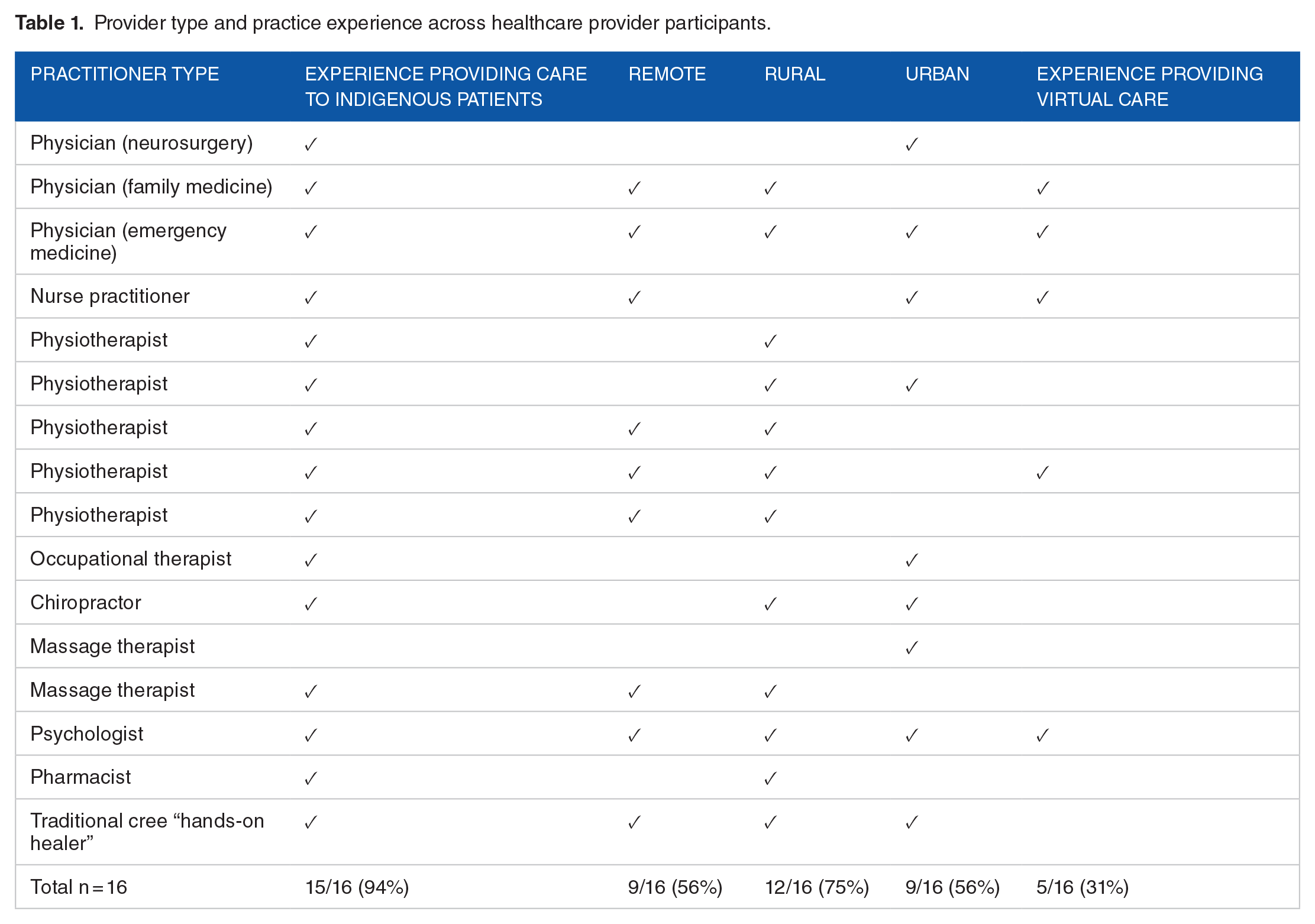
Healthcare provider participant type and experience is summarized in Table 1. Years of experience ranged from 1 year to >20 years. Nine participants identified as women and 7 as men, with an average age of 42 years old (range 30-74 years old).
Provider type and practice experience across healthcare provider participants.
Interview themes
Four overarching themes were constructed from the data collected: (1) Challenges for healthcare providers; (2) Barriers and consequences for patients; (3) Facilitators for healthcare providers and patients; (4) Recommendations to improve accessibility to health care (Figure 1).

Graphic representation of themes.
Challenges for Providers
Access and coordinated care
The majority of healthcare providers working in rural and remote areas spoke of challenges in working in isolated environments and felt that their ability to provide optimal care was often restricted based on access to other providers, availability of resources and capacities of their practices and healthcare system structures.
“But if the physician . . . they’re sitting there thinking, “Okay, this person needs a physiotherapist, but why bother even recommending?” because it’s impossible to even get them one.” (Rural, Remote, Urban practice)
“There’s just barriers on even the provider’s end. . . to make sure that patients are being seen in a timely manner” (Rural practice)
Access to specialists including pain specialists and physiotherapists were sometimes perceived by healthcare providers as not an option and long waiting lists often resulted in patients accessing this type of care in more chronic stages of back pain.
“They just literally don’t have access. Or even the physios that are there, because they’re covering so many communities, if they’re coming in maybe once a week or twice a week, it might be really tough to actually get appointments.” (Rural, Remote, Urban practice)
Healthcare providers spoke about the importance of understanding the realities of their patients, which includes their patient’s ability to access and receive further care. It was evident that these perceived challenges for patients influenced care decisions. Availability of services, cost, travel, and wait times were just some factors influencing access to care.
“And we just have no other options other than to send several hundred kilometres away, and you’re not gonna get the follow-up, you’re not gonna get that continuity of care. You’re not gonna get a team approach to care. And so we’re sort of [limited] in what we can actually do. Really, the only thing we have access to is pharmacological options, which is not ideal.” (Urban and Remote practice)
It was commonly mentioned by healthcare providers that resources and time are influenced by funding structures for healthcare in both public and private contexts. This often places limitations on either the duration of appointments or the number of times a patient and healthcare provider can interact, and in some cases the ability to interact at all. These limitations not only disrupt relationship building but also restrict providers’ ability to address underlying causes or contributing factors to their patients’ back pain.
“. . .it only allows 20 minutes with a number of patients in a clinic. So, the payment process doesn’t allow that kind of development of relationship. And I think that’s true of all healthcare providers. If they had the time to spend, develop relationships, they’d get better compliance, they’d get better effort and all of those things. (Urban, Rural, and Remote practice)
Publicly available virtual care options for certain treatments for CLBP was also mentioned as being restricted.
“They need that hands-on, they need more time and education than I can offer them than just a handout of, “Here, these are the exercises. Run through it quickly” and then on to the next patient or whatever. So yeah, I think that piece is really missing, and it’s hard to access. Even, like, I tried accessing some virtual care physiotherapy for a couple patients over time, but the only options were private, and I couldn’t get the funding in place for them to be able to access it, so they didn’t access it.” (Rural and Remote practice)
Patient care: Complexities and past experiences
Challenges in access to further care and provider resources coupled with patient specific co-morbidities and realities can create difficulties which healthcare providers said can be frustrating and stressful.
“the frustrating nature of treating chronic pain. It’s sort of draining. And it’s easy to get burnt out if you have a lot of those patients. They don’t get better right away like a sprained ankle or something, if you know what I mean. So, sometimes it’s just challenging, emotionally, to treat those patients.” (Rural practice)
“pain management is certainly a complex issue, and patients with multiple comorbidities, sometimes you’re limited in the pain management options you have available.” (Rural and Remote practice)
Common healthcare provider perceptions of patients with CLBP is that many patients feel hopeless in managing and treating their back pain. Additionally, past care experiences, including challenges with access and differing medical opinions and stereotypes, often make patients apprehensive to move forward with different types and approaches of treatment.
“I found people became just very stoic about it. . . it is just a part of their life. And almost accepting of it or resigned to it as. . .it’s going to be with them for the rest of their lives, “So just give me some medication to deal with it as best I can,” and just sort of get on with it.“ (Urban and Remote practice)
“because they’re having pain they feel that they need medication for the pain. So, unfortunately, right away when they see a provider, the assumption is that they are drug-seeking. And so there’s almost like they’re labelled around that right away, even though they may have very legitimate reasons for having back pain, or that it’s definitely very real. . . . there’s stereotypes that are proliferated right away when they are asking for pain medications.” (Urban, Rural, and Remote, and practice)
Healthcare providers felt patients often did not have realistic expectations regarding management strategies, which created challenges in terms of communication as well as accepting and following management recommendations.
“And so now it became a battle of, we’re being a gatekeeper for pain medications, and ‘you don’t want to help us.’ So it’s taken a lot of work to redirect a lot of that energy into, ‘We want to help you more.’” (Urban and Remote practice)
“There’s sometimes a sense of frustration, and sometimes there’s different expectation of what is good management of chronic pain or persistent pain. And I think that’s shifting over time, but lots of the times, patients are expecting to come and be fixed by the healthcare system.” (Rural and Remote practice)
A lack of appropriate early pain education was suggested as a contributor to patient mindsets.
“I think what’s lacking a lot is the education at the primary level. . . I find there’s still very much a big lack in the education and what’s safe and what’s not safe to do, and just self-management, and making them feel safe with moving again” (Urban practice)
Healthcare Provider Perspectives of Patient Challenges
Healthcare providers mentioned specific challenges their patients with CLBP face that often influence how care is provided and responded to.
Lifestyle changes
Healthcare providers emphasized that lifestyle changes can greatly improve CLBP for certain patients, but the nature of chronic pain is so complex that even the simplest of changes can be challenging for patients to make.
“a lot of this pain, in principle, responds best to changes in lifestyle – these are very hard changes to make, and sometimes they’re not very feasible for patients. . ., so I think there’s the frustration aspect, too, with pain. And then just the difficulty side of being able to implement seemingly simple changes, which are actually very difficult, and complex, and multifaceted.” (Urban practice)
Navigating the healthcare system
Healthcare providers felt that many of their patients were unaware of what services were available that could potentially be helpful for their back pain. Spending time educating patients on additional services as well as helping them navigate the healthcare system were common practices among providers.
“I’m advocating with the patients to say, “You should ask your doctor about this. You should ask your doctor about that.” You know, like “These are possibilities, and so you should. . .” you know, trying to educate them in the possibilities” (Urban, Rural, and Remote practice)
Healthcare providers commented on the additional challenges in navigating the healthcare system for Indigenous patients and the potential mismatch between Western and Traditional Indigenous worldviews, recognizing elements of racism that continue to exist.
“. . . (for Indigenous patients) navigating the system is, in many ways, foreign, and unwelcoming, and uninviting, and fear-instilling.” (Urban practice)
“so much of the Western medicine mentality is really on individual’s agency. And so we’re going to tell you what to do, and if you don’t get better it’s your own fault for not following what we’ve told you to do. But that doesn’t put into any context the situation that they’re living within, including cultural values and beliefs.” (Urban and Remote practice)
“I think that there is definitely an element of racism involved with the interest of how people are labelled. And in a couple different key areas where people would be getting, or trying to seek care, and leads to negative outcomes.”(Urban, Remote and Indigenous practice)
For Indigenous patients, reliance on things like medical taxis or having to follow Non-Insured Health Benefits protocols to receive funded care are often not acceptable, timely, reliable, or appropriate.
“[when] they [Indigenous patients] can’t afford to travel, they don’t have someone to drive them, they don’t have a vehicle and they rely on a medical taxi, and there’s zero reliability with the medical taxi service.” (Rural and Remote practice)
Needing ongoing care
Healthcare providers reported that people with CLBP may need long-term management and ongoing care, often with multiple approaches including medication, mental health and lifestyle changes, which requires involvement from interdisciplinary providers.
“Sometimes patients are reluctant to buy into having kind of mental health assistance for helping manage a musculoskeletal issue. But if you’re able to help them make that connection between stress and mental health, it can be very helpful.” (Rural and Remote practice)
Facilitators for Healthcare Providers & Patients
Direct facilitators for healthcare providers and anticipated facilitators for patients were intertwined, and ultimately influenced care provision.
Coordinated care
Healthcare providers that worked in a team-based environment felt supported and that they were able to provide comprehensive care to their patients as well as more timely care.
“We are all in the same space together. There’s a lot of collaboration back and forth that patients feel as if they’re supported and having multiple individuals on their team.” (Urban and Rural practice)
“But, we can access a physiotherapist because we have one. He’s not there full-time, but we actually have three or four within the clinic. So I can get, sometimes, an immediate appointment for them. Or sometimes I can get an appointment within days.” (Urban and Remote practice)
Communication among different care providers was emphasized as imperative to ensure patient care was being assessed from a multi-disciplinary perspective.
“ they’re coming into a centre that they’re already comfortable with. They’re not having to go somewhere else. The care is all integrated together. And we can really have a team approach to managing the care safety and effectively, that is patient-centred, but also does resemble adapted best practice guidelines. . .” (Urban and Remote practice)
Funded care
Funded care in some capacities, including patient third-party insurance, was also identified as a facilitator by some healthcare providers; this was often dependent upon the population demographics of their patient group and the type of care that was being provided.
“I do it all virtually. It’s actually really improved service for my very rural clients, because Health Canada would not pay transportation for them to come from far away, and now they pay – they wouldn’t pay for telephone consultation, but they do now. So, I’m seeing people in very remote places. Even farming people in south-eastern Saskatchewan. People who just are not gonna drive three hours to see somebody.” (Urban, Rural, and Remote practice)
“I think because of the [insured] population that I work with, they tend to have more access to most or expedited appointments and all that, more streamlined a lot more than in the public system . . .I think that they’re the lucky ones, that they have more of a comprehensive team.” (Urban practice)
Care in community
Healthcare providers recognized the benefit to patients when they, or other medical professions, were able to provide care in or near patients’ home community.
“. . .in some of the rural settings is that some of the orthopedic surgeons actually will go out into the smaller towns and do consultations there. And I think that’s been very helpful in order to bridge those people so they’re not having to come into the city or wait an x amount of time that they’ve been trying to bridge that gap.” (Urban and Rural practice)
“I think providing some education to the nurses has been beneficial in providing that continuous care so that the patients are supported when there isn’t a physician in the community.” (Rural and Remote practice)
Patient education & agency
Healthcare providers mentioned the importance of building trusting relationships and focusing on education and self-management strategies (eg, engaging in appropriate exercise, movement mechanics including postural considerations, positions of relief, and avoidance of prolonged positioning, etc). There was a strong consensus that patient agency and education contributes to better outcomes. More specifically, when a patient understands their back pain and treatment or management rationale, they are more likely to buy-in to making changes and supporting themselves.
“ (if) they feel more empowered of how to manage their condition, that it would decrease the overall use of healthcare, and surgeries, and visits to the emergency room, and opioids that they might be using, and just even their health in general.” (Rural practice)
“with many of my patients (it) is that nobody’s really told them. So when you actually explain they’re like, “Oh! Okay, I get it.” And so then that helps figure out what to do about it or why what you’re recommending might be really helpful.” (Urban, Rural, and Remote practice)
Virtual care
The perceived value of virtual care ranged across the various disciplines. Some healthcare providers reported this as a major facilitator for patients to access care, particularly during and after the COVID-19 pandemic. Others saw value in virtual care for components of care provision, but not as a sole approach to care, and others were unable to provide virtual care (ie, – massage therapy). Some disciplines, such as physiotherapy, reported that some components of care could be conducted virtually, but some components required hands-on assessment and treatment strategies.
“That’s one of the things I like about virtual stuff, is being able to access when you need it. And I always prefer to have people come in earlier rather than waiting ‘til it gets to be a crisis.” (Urban, Rural, and Remote practice) “There’s still such value in hands-on care and manual therapy and biomechanical treatment that you can provide an education piece to it, but there’s still such a significant importance to seeing someone in-person. But yes, I think it has given us the ability to at least see somebody in-person, and then if we needed to carry on any education or exercise progression, and they can’t make it into the location that we’re in, at least we can try to set that up in a virtual appointment and provide that in that aspect.” (Urban and Rural practice)
Recommendations on Improving Accessibility to Healthcare
Multidisciplinary care
Most healthcare providers indicated that having more available options for multidisciplinary care, with an emphasis on patient education and infrastructure, would improve outcomes.
“As a local provider, having access to specialists, physiotherapists, or otherwise, really helps reduce professional isolation. . .not just that there’s another provider that we can talk to, but that there’s more options, there’s more tools. And it really helps us know that we can provide the standard of care that we would want to have provided to ourselves or our family or loved one.” (Urban and Remote practice)
Healthcare providers were aware of ideal models of care and offered solutions for underserved areas, such as virtual care components to care.
“to have a multidisciplinary approach like we do have in the city would be ideal in all the rural areas. And maybe that part that has to be done virtually. But for people to have access to that would be critical in managing the back pain.” (Urban and Rural practice)
Provider education
Most healthcare providers reported that improved education for frontline healthcare providers on chronic pain management would be valuable to improve chronic pain management at the primary level of care.
“having healthcare providers being on the same page with the physiology and what are best practices for persistent pain, is important.” (Rural and Remote practice)
“the pain education. . .whether that’s physiotherapy or you’re getting that from a chiropractor or a different discipline, that’s gonna be critical in managing chronic back pain.” (Urban and Rural practice)
Discussion
This study identified several gaps in care for people living with CLBP from the perspective of healthcare providers. These gaps encompassed challenges faced by healthcare providers, whose perspectives influenced their decisions on care provision. These challenges were intertwined with perceived or anticipated obstacles for patients, thereby impacting the care recommendations made by practitioners. The main challenges for healthcare providers were availability of resources and time influenced by funding structures, access to other healthcare providers or specialists, as well as patient complexities and past experiences. Healthcare providers who practiced in rural and remote communities reported additional challenges of access to, and coordination with, other healthcare providers, demonstrating professional isolation is often exacerbated in rural and remote communities. Healthcare providers recognized additional challenges for Indigenous patients, specifically around navigating the healthcare system, complicated by funding structures and travel requirements. Despite the challenges, there were many facilitating factors identified in the current delivery of care across Saskatchewan such as coordinated care, funded care, and providing care in the community, as well as recommendations from healthcare providers on how to improve care for those living with CLBP.
One of the most significant challenges Saskatchewan healthcare providers faced when trying to improve access to care for patients with CLBP was the professional isolation and siloed environments, which was identified to be more problematic in rural and remote locations. The siloed nature of healthcare, uncoordinated across multiple professions and settings, has been suggested to be one of the greatest challenges limiting delivery system optimization. 9 Primary care physicians undertake the initial evaluation in 65% of low back pain cases and are often the sole provider for these patients. 7 Further, many patients with CLBP may have comorbidities, which is also more problematic in rural locations where rural Canadians have higher healthcare needs but less access to healthcare. 30 Healthcare providers must address these comorbidities in addition to the patient’s CLBP to ensure that they receive comprehensive care. This is challenging given the constraints of current practice models. Lack of interprofessional team support in rural settings are key challenges identified by Canadian physicians, along with high rates of burnout.13,31 Team-based care and equitable access are cited as objectives to optimize healthcare delivery to address these issues and provide comprehensive care. 9 This includes funded care for appropriate services, recommended as a facilitator among the healthcare providers interviewed in this study.
Healthcare providers reported a range of additional perceived barriers affecting access to treatment. These barriers included navigating the healthcare system complicated by lack of insurance coverage for certain treatments, long wait times for appointments, and geographic or financial barriers that limit access to care and understanding of what is available and appropriate to them. For example, approximately one-third of Canadians do not have additional health insurance that would help to cover costs of care options like physiotherapy services, 32 which are typically not covered through the provincial public health system. The anticipation of these complex barriers led to recommending care that seemed more accessible, even if it was not optimal. Healthcare providers reported an additional level of complexity regarding referrals for Indigenous patients covered under Non-Insured Health Benefits, which must follow specific guidelines in terms of how, when, and where to access care. Although patients may rely on primary care providers for guidance through the medical system, referrals may not be made based on perceived barriers of geography or costs and the education on these options for care may not be provided for the patient. This is reflected in the literature where patients feel that there is “nothing that can be done” for their back pain. 33
Communication and coordinated care were noted as barriers, a facilitator, and a recommendation for improving care. Patients with CLBP often have complex medical histories and may be managing multiple health conditions, which can make it difficult for healthcare providers to fully understand their needs and develop effective treatment plans. Further, many CLBP patients require regular care and ongoing follow-up care. To address this challenge, prioritizing patient-centered care, including shared decision-making and active patient involvement in care planning should be considered. In some cases, healthcare providers described how they educated the patient on what they should do next, rather than actively providing the appropriate referrals, putting the burden on the patient to further navigate the fragmented system. True patient-centered care could involve provider-to-provider communication, which would include patient history, coordinated care plans and making sure referrals are appropriate. Alternative models to healthcare delivery that include a broad range of providers to care for people with chronic conditions have been reported, with some models integrating physiotherapists within primary healthcare teams with unanimous sentiment of value from both family physicians and nurse practitioners. 34 Given the Canadian primary care crisis, 35 it is becoming more important to rely on team-based models of care 35 or non-physician led models that have been developed to improve wait times and patient outcomes for low back pain care.18-21
To address perceived challenges in access, practitioners suggested several potential solutions. One solution is to expand access to multidisciplinary care, in line with prior recommendations to provide patients with a more comprehensive and coordinated approach to managing their CLBP.4,8 The problem of healthcare fragmentation and the need for transformation to multidisciplinary care has been known for many years; however, the transformation required to implement these changes requires innovative solutions starting at the local or regional level with co-creation of solutions at the front lines and co-leadership of projects by researchers and clinicians, to provide knowledge for the broader health networks.9,36 Additionally, the implementation of evidence-based treatment guidelines requires educating patients and providers, and changing outdated ideas about CLBP. 4 Solutions are needed to mitigate professional isolation and to provide more effective management for CLBP, including patient and provider chronic pain education, culturally responsive care for Indigenous Peoples, as well as access to community facilities for individuals to take part in active lifestyles and exercise management. Virtual care was a recommendation by healthcare providers to address some of these barriers, and could be utilized to improve access to certain types of care, education for both patients and providers, as well as reducing professional isolation through virtual interdisciplinary and team-based care models.37-39 The way in which virtual care is offered and these potential benefits must be contextualized based on the population that is being served, as well as the type of healthcare that is being provided.
The findings presented here offer valuable insights for clinical practice, emphasizing the importance of maintaining patient-centered care, culturally responsive approaches, and enhancing education and training opportunities for healthcare providers in early back pain management. Implementing innovative solutions to address healthcare fragmentation and improve access to CLBP care requires collaboration between researchers, clinicians, and community stakeholders. Future research should prioritize co-creation of solutions at the local level and evaluate the effectiveness of innovative care delivery models in diverse healthcare settings, focusing on community needs and strengths.
Strengths and limitations
This study used a patient oriented research approach, engaging patients living with chronic low back pain in all stages of the research, including shaping the research questions. The qualitative nature of the research provided insights of healthcare provision that quantiative methods may not capture; however, the study does have several limitations. Healthcare provider experiences presented in this paper are specific to reported disciplines in the Saskatchewan context and therefore not applicable broadly. Healthcare providers were prefaced to speak about their overall experiences; however, interviews were conducted during the height of the COVID-19 pandemic and public health restrictions, thus experiences shared may be shaped by this context.
Conclusion
Improving access to CLBP care across Saskatchewan requires considerations on the different systems, networks of support, and community contexts in which healthcare providers are working. Building trusting relationships and focusing on patient agency were identified as being beneficial and in-line with current CLBP guidelines. Providers working in rural, remote, and Indigenous communities face unique and additional challenges in the type of care they can realistically provide or recommend but also how it is provided; this includes navigating additional barriers to accessing appropriate and timely care.
Supplemental Material
sj-docx-1-his-10.1177_11786329241265861 – Supplemental material for Healthcare Provider Perspectives on Access to Healthcare for Chronic Low Back Pain Across Urban, Rural, and Remote Settings
Supplemental material, sj-docx-1-his-10.1177_11786329241265861 for Healthcare Provider Perspectives on Access to Healthcare for Chronic Low Back Pain Across Urban, Rural, and Remote Settings by Katie Crockett, Stacey Lovo, Alison Irvine, Catherine Trask, Sarah Oosman, Veronica McKinney, Terrence McDonald, Nazmi Sari, Rosmary Martinez-Rueda, Harini Aiyer, Bertha Carnegie, Marie Custer, Stacey McIntosh and Brenna Bath in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241265861.docx – Supplemental material for Healthcare Provider Perspectives on Access to Healthcare for Chronic Low Back Pain Across Urban, Rural, and Remote Settings
Supplemental material, sj-docx-2-his-10.1177_11786329241265861.docx for Healthcare Provider Perspectives on Access to Healthcare for Chronic Low Back Pain Across Urban, Rural, and Remote Settings by Katie Crockett, Stacey Lovo, Alison Irvine, Catherine Trask, Sarah Oosman, Veronica McKinney, Terrence McDonald, Nazmi Sari, Rosmary Martinez-Rueda, Harini Aiyer, Bertha Carnegie, Marie Custer, Stacey McIntosh and Brenna Bath in Health Services Insights
Footnotes
Acknowledgements
We would like to sincerely thank and acknowledge all of the participants who shared their experiences of providing care for those living with chronic low back pain for this research.
Author Contributions
KC and AI performed the measurements (survey data collection and interviews) and drafted the manuscript. KC and HA designed the figure. BB supervised the work. RM and HA processed the data, and performed the initial analysis. KC, SL, AI, RM, HA, and BB contributed to ongoing data analysis. All authors aided in development of survey questions and interview guides, interpretation of the results and contributions to the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study provided by the Canadian Institutes for Health Research, Saskatchewan Centre for Patient-Oriented Research, and University of Saskatchewan College of Medicine.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.