
Abstract
Objective:
This study aimed to use the Person-Centered Coordinated Care Experience Questionnaire (P3CEQ) to assess the experience of person-centered coordinated care among people with long-term conditions in the Balearic Islands, Spain.
Methods:
Over 1300 participants receiving treatment for chronic conditions or HIV pre-exposure prophylaxis were invited to complete the P3CEQ and a socio-demographic questionnaire, both administered electronically via the Naveta app. The P3CEQ assesses the key domains of the P3C through an 11-item questionnaire. Items 1, 2, 3, 4, 5, 8, 9 and 10 assess specifically person-centredness (PC subscale), while items 5, 6, 7, 8 and 9 measure care coordination (CC subscale; question 7 includes 4 sub-questions to specifically assess care plans). Descriptive statistics were used to summarize patient characteristics and P3CEQ items scores. Data analysis included chi-squared test of independence, Student’s t-test and analysis of variance test. Pairwise comparisons were adjusted by Bonferroni correction.
Results:
The P3CEQ and a socio-demographic questionnaire were sent to 1313 individuals (651 men, 657 women, 5 ‘other gender’). A response rate of 35.34% was achieved, with 464 P3CEQ responders (223 men and 241 women). Significant differences in response rates were observed by age, smoking status, alcohol consumption, membership of patient organizations, and use of alternative medicine. Care planning was rated significantly lower than other measured domains. Women experienced less person-centered care than men (16.64 vs 17.91) and rated care coordination worse than their male counterparts (9.18 vs 10.23). There were also differences in scores between medical condition types, with cancer and inflammatory bowel disease patients rating highest for both person-centered care (21.20 and 19.13, respectively) and care coordination (10.70 vs 10.88, respectively). Patients with skin and rheumatic diseases rated lowest their experience of person-centered care. People with higher education and those employed or studying experienced better person-centeredness.
Conclusion:
Using the P3CEQ, we detected significant differences in the care experiences of people with chronic conditions, suggesting the need to address potential gender biases, social inequalities, and the poorer ratings observed for certain conditions in the study population.
Keywords
Introduction
As medical treatments improve and life expectancy increases, the incidence of chronic disease is globally rising.1,2 In Europe, more than 50 million people live with multiple long-term conditions, and almost 55% of the population aged ⩾ 65 years have reported having one or more chronic disease (almost 60% in Spain).3,4 People with multiple chronic conditions (multimorbidity) tend to experience lower quality of life, reduced functionality and more dependnce.1,3,5,6 These patients are often poly-medicated and require multi-disciplinary care and long-term support.2,6-8 Providing high-quality, comprehensive, and cost-effective care to this large group of patients may present conflicting goals for healthcare systems and providers.1,9,10 To meet this challenge, there is a current trend in healthcare systems to move toward value-based care models.11-13 Value-based health care strategies focus on creating value for patients—improving outcomes that matter to them and their experience of care—while reducing costs.11,14 A key requirement for delivering value to patients is a good understanding of their general and specific healthcare needs.12,14
Disease-centered and compartmentalized models of care tend to focus on clinical outcomes. 7 In such settings, chronical patients often experience care as fragmented and discontinuous, and feel that their needs and preferences are ignored.7,15,16 In disease-centered models, people with multimorbidity are at risk of receiving impractical, irrelevant, or even inappropriate treatments, while lack of coordination can lead to unnecessary duplication and/or conflicting treatments and recommendations. 7 Delivering effective care that addresses the needs of these patients requires coordination and collaboration across integrated care settings and a focus on the person, rather than the disease.2,16 With a particular focus on the chronically ill people, researchers agree on the need to move toward more integrated and patient-centered approaches, such as the person-centered coordinated care (P3C).15,17,18
In several European countries, including Spain, efforts are being made to implement P3C models for people with multiple health and social care needs.2,19,20 To guide the transition to a P3C model and assess its impact on outcomes and quality of care, evidence and policies recognize the importance of measuring patient experience and perspectives.15,21-23 Several patient-reported experience measures (PREMs) have been developed to assess healthcare from the patient’s perspective. 2 However, many of these PREMs focus on care provided by a single discipline or on medical interventions for a specific condition, and are not well suited to assessing the complexity of care for multiple chronic conditions. 19
The Person-Centered Coordinated Care Experience Questionnaire (P3CEQ) is a PREM designed in the United Kingdom (UK) to explicitly assess P3C from the perspective of people with long-term conditions.15,22 Its development involved commissioners, healthcare professionals, and patients with chronic conditions, the latter contributing as patient representatives and expert co-designers. 15 The P3CEQ was created to reflect the 5 core domains of the P3C: information and communication process, care planning, transitions, goals and outcomes, and decision making. 22 It is a concise, efficient and user-friendly questionnaire suitable for routine practice and capable of providing feedback during service development.15,22 It has been assessed in both the United Kingdom and the Netherlands as a valid and reliable measure of P3C in people with long-term conditions, and has shown strong face, construct, and ecological validity, with sensitivity to change.22,24 Two major studies (SELFIE and SUSTAIN) have used the P3CEQ to evaluate integrated and tailored care for adult patients in Europe, and the questionnaire has been translated into several European languages, including Spanish and Catalan.2,22,25
We conducted a study to assess the quality of global health care using the P3CEQ with more than 1300 people who were receiving either treatment for chronic conditions or HIV pre-exposure prophylaxis (PrEP) and who regularly visited the pharmacy outpatient clinics of different hospitals in the Balearic Islands (Spain). The aim of the study was to capture the P3C experiences of people with different types of long-term conditions and to identify potential biases in care related to gender, education level, addiction, and other socio-demographic characteristics, in order to improve person-centered and coordinated care for this population. To our knowledge, this is one of the first published studies to use the P3CEQ to assess patients’ P3C experiences in the routine clinical practice in Spain and the first to compare P3C experiences among people with different chronic conditions.
Methods
Study design and sample selection
We conducted a multicenter, cross-sectional, observational study involving people with at least 1 serious chronic condition and a small subset of people at high risk of HIV. All of them were recruited from the pharmacy outpatient clinics of 6 public hospitals in the Balearic Islands (Spain), where they were regularly treated with hospital-only medicines, including biologics, selective immunosuppressants, antiretrovirals, monoclonal antibodies, oral cytostatic drugs, and pre-exposure prophylaxis (PrEP). The PrEP is a high effective HIV prevention treatment (eg, emtricitabine /tenofovir) implemented in several European countries for HIV-negative people with high risk of HIV acquisition.26,27 Patients under 18 years of age were excluded.
Participants were recruited between January 2021 and January 2023 from the following study centers: Hospital General Mateu Orfila (Menorca), Hospital Universitari Son Espases (Mallorca), Hospital de Manacor (Mallorca), Hospital Universitari Son Llàtzer (Mallorca), Hospital Comarcal d’Inca (Mallorca), Hospital Can Misses (Ibiza). All study subjects met the following criteria: aged ⩾18 years old; either diagnosed with 1 or more serious chronic conditions or HIV-high risk individuals receiving PrEP; agreed to participate in a telehealth project linked to e-health questionnaires through the Telehealth Naveta platform (https://navetahealth.com/).
Participants were categorized according to their diagnosis as follows: psoriatic arthritis, rheumatoid arthritis, asthma, breast cancer, prostate cancer, lung cancer, ulcerative colitis, Crohn’s disease, atopic dermatitis, multiple sclerosis, spondylitis, hidradenitis suppurativa, migraine, eye conditions, psoriasis, urticaria, HIV-positive, HIV-high risk requiring PrEP, and other conditions.
In order to make meaningful comparisons between larger groups, the above categories were later aggregated into the following types of medical conditions: rheumatic diseases (psoriatic arthritis, rheumatoid arthritis, and spondylitis), cancer (breast, prostate, and lung cancer), inflammatory bowel disease (IBD: ulcerative colitis and Crohn’s disease), skin diseases (atopic dermatitis, psoriasis, urticaria, and hidradenitis suppurativa), neurological disorder (multiple sclerosis and migraine), HIV-positive, HIV PrEP users, and other conditions (asthma, eye diseases, and other conditions).
P3CEQ and sociodemographic characteristics questionnaire
The P3CEQ assesses the key domains of the P3C through an 11-item questionnaire. Items 1, 2, 3, 4, 5, 8, 9, and 10 assess specifically person-centeredness (PC subscale), while items 5, 6, 7, 8, and 9 measure care coordination (CC subscale; question 7 includes 4 sub-questions to specifically assess care plans). Item 11 is an optional question measuring self-care management and was not included it in our statistical analysis. Each question contains checkboxes (for scoring) and an open field (for comments). This study analyzed only scores. We used the Spanish version of the P3CEQ, developed as part of the EU-funded SUSTAIN project. 25 This version was translated and culturally adapted from the original English version by local experts associated with the SUSTAIN project in collaboration with the P3CEQ developers. 2
Two questions of this instrument (6 and 7a) are dichotomous (0 or 3), and the rest of the questions are Likert-scored (from 0 to 3). 22 The score for item 7 was calculated by averaging the scores for questions 7a, 7b, 7c, and 7d. Higher scores represent better experiences of person-centered coordinated care. The minimum total score is 0 and the maximum is 30.
Participants were also asked to complete a socio-demographic questionnaire, which included questions about their level of education, employment status, partner status, membership of patient associations, smoking habit, and alcohol and drug consumption, among others. The BMI parameter was categorized according to the World Health Organization (WHO) classification: underweight (less than 18.5 kg/m2), healthy weight (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), and obesity (⩾30 kg/m2). 28
Data collection procedures
The P3CEQ and the socio-demographic questionnaire were delivered electronically through the Telehealth Naveta platform (https://navetahealth.com/), a value-based initiative to assess health outcomes in chronically ill patients through electronically administered patient reported measures. Individuals participating in the study were required to sign a written informed consent form before being registered in the Naveta platform, in accordance with the provisions of Law 41/2002 of 14 November, which regulates patient autonomy and rights and obligations regarding clinical information and documentation.
The study participants received the P3CEQ on their own device (computer, tablet, mobile phone) via the Naveta application. They completed the P3CEQ based on their experience with global healthcare, including primary care, intermediate care, acute hospital care, long-term care, day hospital, community and hospital mental health care, dialysis, socio-health care, home rehabilitation, and other services.
Statistical analysis
Descriptive statistics were used to summarize continuous variables as means and standard deviations (SDs), and categorical variables as frequencies and percentages. Sample size as calculated to estimate the response rate of the questionnaire, with a statistical power ⩾80%. The chi-square test (χ2) of independence was applied to compare the frequency distributions of categorical variables. Comparisons of quantitative variables between 2 categories were performed using the Student’s t-test, while the analysis of variance (ANOVA) test was used for comparisons involving more than 2 categories. Pairwise comparisons were assessed using chi-squared or Students t-tests adjusted by Bonferroni correction. Missing values were ot imputed for analysis. All statistical procedures were performed using R software v4.2.2 (www.R-project.org; R Core Team, 2022). For all tests, the statistical significance level was set at P ⩽ .05.
Data protection
The survey was conducted according to current Spanish Personal Data Protection laws (Spanish Organic Law 3/2018 of 5 December on the Protection of Personal Data and the Guarantee of Digital Rights).
Results
Descriptive analysis of the sample
Of the 2307 health service users from the participating centers who were registered on the Telehealth Naveta platform, 994 (43.09%) did not meet the requirements for the study (see Figure 1). The P3CEQ and a socio-demographic questionnaire were sent to the remaining 1313 individuals (651 men, 657 women, and 5 of “other gender”). Some of these individuals (73) were registered for 2 or more chronic conditions and received 1 P3CEQ for each condition, resulting in a total of 1444 P3CEQs being sent. The response rate was 35.34%, with 464 P3CEQ responders (223 men and 241 women). Of these, 4 people (3 men and 1 woman) completed the P3CEQ for 2 different conditions, making a total of 468 completed P3CEQs.

Flow chart of study participants.
The socio-demographic characteristics and distribution of study participants by type of medical condition are shown in Table 1. The number of patients in the medical condition categories varied: the rheumatic diseases, HIV-positive, and skin diseases groups had relatively high numbers of registered patients (372, 295, and 270, respectively), whereas the oncological patients and HIV PrEP user categories included lower number of patients (25 and 28 respectively). Women were predominant in the neurological, rheumatic, and oncological diseases categories (74.86%, 59.68%, and 56.00% respectively), while the HIV PrEP user group was made up entirely of men. The mean age of the study sample ranged from 58.40 years in the oncology group to 38.50 years in the HIV PrEP users group.
Socio-Demographic Characteristics and Distribution of Study Participants by Type of Medical Condition*.

Abbreviations: BMI, body mass index; IBD, inflammatory bowel disease; HIV PrEP, HIV pre-exposure prophylaxis; N, number of available data for each variable; P3CEQ, person-centered coordinated care experience questionnaire; SD, standard deviation.
Demographic characteristics were reported as mean ± standard deviation (SD) for quantitative traits and counts (%) for qualitative variables.
5.55% of participants were registered for more than 1 chronic condition, so the categories are not mutually exclusive.
The frequencies of P3CEQ responders and non-responders across various socio-demographic categories are shown in Table 2. There were no significant gender differences in the response rate (34.25% men vs 36.68% women; P = .390). However, when comparing by age, there were significant differences in response rates (P < .001), most notably between the youngest participants (18-49 years), who exhibited the highest response rate, and those aged 65 and over (37.83% and 21.18%, P < .001). Additionally, the response rate was significantly lower among smokers compared to non-smokers 59.22% and 79.14%; P < .001), individuals who reported rare alcohol consumption compared to those who reported no alcohol consumption (57.39% and 83.08%; P < .001), members of patient organizations compared to non-members (44.44% and 69.25%; P = .004), and individuals who reported using alternative medicine compared to those who did not (57.98% and 78.51%; P < .001). When comparing categories of different types of medical conditions, HIV PrEP users had the significantly highest response rate (85.19%; see Figure 2 and Supplemental Table S1).
Distribution of P3CEQ Responders and Non-Responders for Subgroups With Different Socio-Demographic Characteristics.

Abbreviations: BMI, body mass index; IBD, inflammatory bowel disease; HIV PrEP, HIV pre-exposure prophylaxis; M, member; N, number of available data for each variable; P3CEQ, person-centered coordinated care experience questionnaire.
This category was not included in the analysis due to its low frequency.
Pairwise comparison across age categories: between 18-49 y and 50-65 y (adjusted P-value = 1), between 18-49 y and >65 y (adjusted P-value <.001), and between 50-65 y and >65 y (adjusted P-value <.001).
Pairwise comparison across Alcohol consumption categories: between Often and Rarely (adjusted P-value = 1), between Often and Never (adjusted P-value = .120) and between Rarely and Never (adjusted P-value <.001).
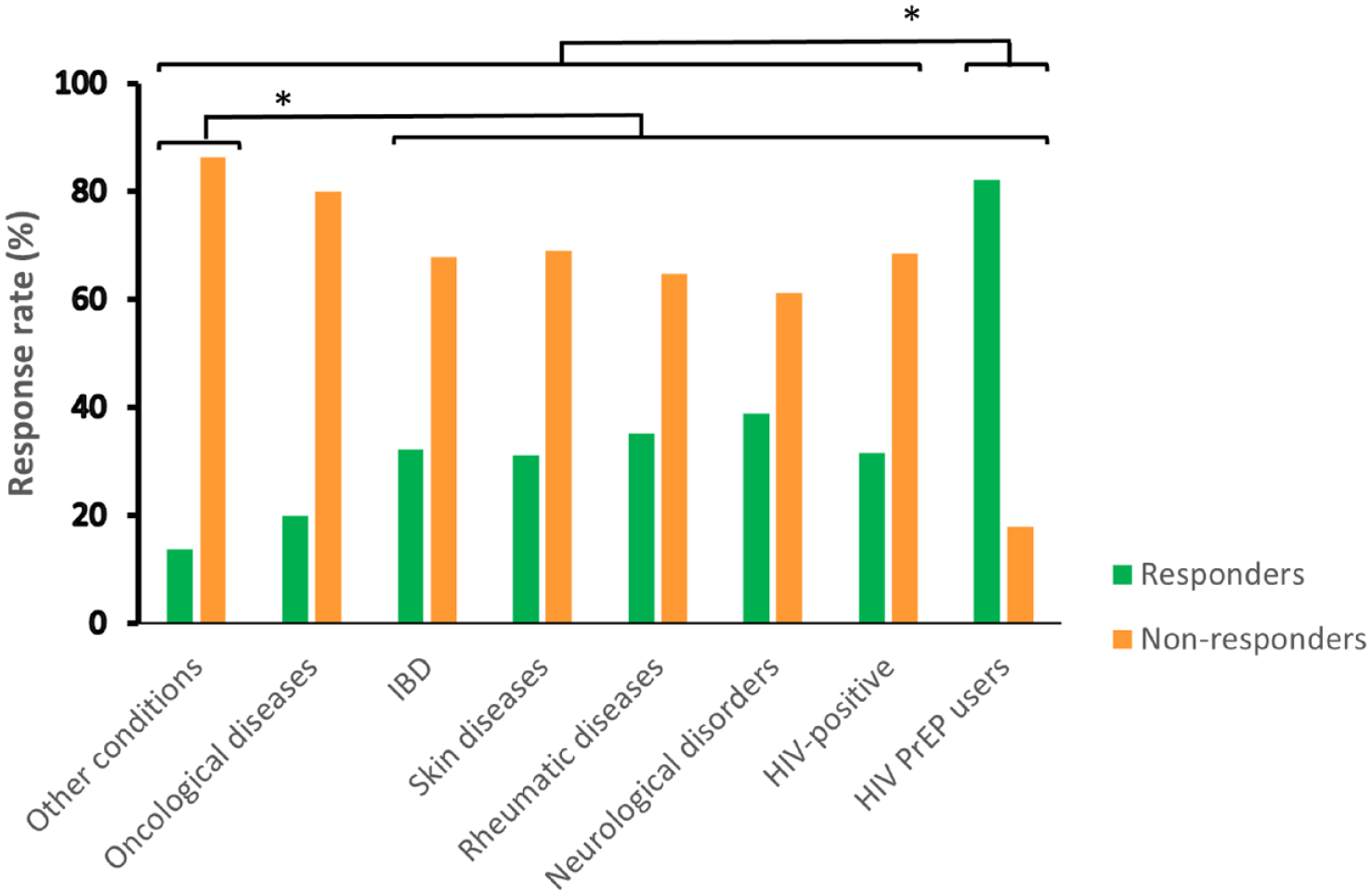
Distribution of P3CEQ responders and non-responders by type of medical condition.
Analysis of P3CEQ scores
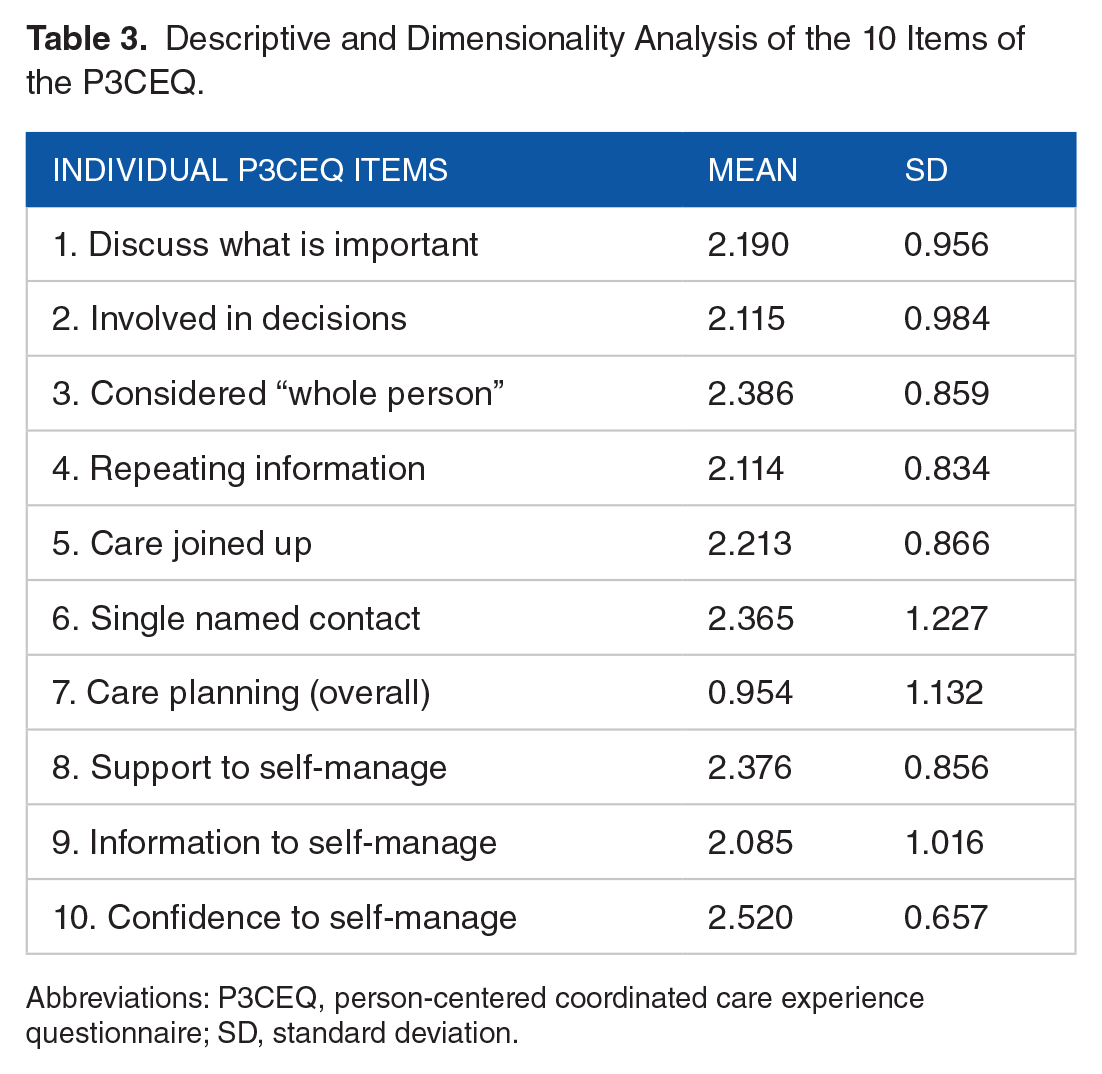
The mean scores and SDs for each P3CEQ item as rated by the study population are shown in Table 3. All items received a mean score of more than 2 out of a maximum of 3, except for item 7 (care planning), which received less than 1. Confidence to self-management was the item with the highest score (2.520 ± 0.657).
Descriptive and Dimensionality Analysis of the 10 Items of the P3CEQ.
Abbreviations: P3CEQ, person-centered coordinated care experience questionnaire; SD, standard deviation.
The mean scores for the 2 P3CEQ subscales for different socio-demographic characteristics and type of medical condition are shown in Table 4. Significant differences were observed between men and women. Men had significantly higher scores than women on both the PC subscale (17.91 ± 5.07 vs 16.64 ± 5.31; P = .008) and the CC subscale (10.23 ± 3.53 vs 9.18 ± 3.79; P = .001). No significant differences were found for age on either the PC subscale (P = .670) or the CC subscale (P = .321).
Mean and Standard Deviation of P3CEQ Subscales for Subgroups With Different Socio-Demographic Characteristics and Medical Condition Type.

P value correspond to the analysis of variance (ANOVA) test for each category. Pairwise comparisons between disease type were shown in Supplemental Tables S3 and S4.
The ANOVA test showed significant differences between medical condition types for PC (P = .009) and CC (P = .037), even after adjusting for age and gender. However, the significance disappeared after adjusting for the rest of variables analyzed because of the lower statistical power in the multivariable model due to the missing values in the covariates (Supplemental Table S2). Oncology and IBD patients had the highest ratings for both person-centered care (21.20 ± 1.48 and 19.13 ± 4.22) and coordinated care (10.70 ± 1.57 and 10.88 ± 2.81). Patients with skin and rheumatic diseases rated their experience of person-centered care worst (16.39 ± 5.03 and 16.22 ± 5.44 respectively).
Pairwise comparisons are shown in Supplemental Tables S3 and S4. Significant differences in the experienced person-centeredness were also observed between education levels (P = .031). The highest person-centered experience was reported by individuals in the higher education category (18.15 ± 4.82), followed by those with secondary school education (16.90 ± 5.25), primary school education (16.43 ± 5.62), and basic education (15.38 ± 6.36). Employed individuals and students reported higher levels of person-centeredness compared to those who were inactive (P = .011). Furthermore, the multivariate analysis using the composite score with PC and CC showed that the scores of the 2 subscales were correlated in all medical condition groups (P = .001; Figure 3 and Supplemental Table S2).

Radar chart of the person-centeredness and coordinated care subscales by type of medical condition.
Discussion
The P3CEQ is designed to measure the quality of care from the patient’s perspective to inform health professionals and systems and to guide change toward more coordinated and person-centered care. 22 This shift has been linked to better health outcomes and improved patient experience of care, particularly in the context of long-term conditions.15,29 In this study, we used the P3CEQ to measure the overall care experience of patients with severe chronic conditions who were attended in multiple health care settings and recruited from the outpatient pharmacy services of public hospitals in the Balearic Islands. We also measured the care experience of a small subset of people receiving HIV PrEP in the same services. The mean P3C scores for men and women obtained in our study are consistent with those observed in the UK validation study and higher than those observed in the Dutch validation study.22,24
The significantly lower levels of both person-centeredness and coordinated care reported by the women in our study, compared with those reported by the men, suggest the possibility of gender bias in relation to P3C. This gender pattern has also been observed in the P3CEQ validation studies and others, reinforcing the possibility that women’s care needs may be less well understood and addressed than those of men.22,24,30-32 Several studies have shown that gender biases in health care can affect symptoms, treatment outcomes, and disease progression.31,33-35 A study on the HIV-positive population of Menorca, in the Balearic Islands, showed worse disease management in women, with more advanced disease stages, more symptoms, and a greater use of anticholinergic medications, among other outcomes. 8 Several factors have been suggested to explain gender bias in healthcare, such as gender blindness, stereotyped preconceptions, communication differences between men and women, and the presence of male-oriented care patterns.36-38. Person-centered care for women (PCCW) models have been proposed to address health inequalities affecting women.32,35 However, research on the implementation of PCCW models remains scarce and has not yet fully addressed the specific needs and preferences of women.32,35 Further research is therefore needed in this area.
To our knowledge, our study is the only one published to date that has compared P3C in different long-term conditions. In our sample population, patients with cancer and IBD (ulcerative colitis and Crohn’s disease) experienced the highest levels of person-centered and coordinated care. However, the results for cancer patients should be interpreted with caution due to the small sample size of this group. With regards to IBD, a possible explanation for the higher scores could be the recent advances in personalized treatments and the implementation of multidisciplinary holistic care for these patients.39-41 Multidisciplinary care for IBD may involve gastroenterologists, radiologist, specialist nurses, hospital pharmacists, mental health professionals, dieticians, and other specialists. 42 Many initiatives have been developed in several countries to define, establish and evaluate multidisciplinary teams that can provide comprehensive and coordinated care to people with IBD.43,44 In our country, the Spanish Group for Crohn’s Disease and Ulcerative Colitis (GETECCU) has implemented a national program to ensure a high quality of care for these patients by evaluating and certifying IBD units, including those in the Balearic Islands. 45
The poorer outcomes observed in patients with skin, rheumatic and neurological conditions may indicate a need to improve person centered and coordinated care practices for these patients. Several studies have shown that people diagnosed with skin conditions, whose treatment tends to focus only on the physical aspects of the disease, feel that their concerns, insights, and the psychological impact of their condition, such as stigmatization, are often ignored or underestimated by healthcare professionals.46-48 Rheumatic and neurological diseases can also have multisystemic effects that require a holistic and collaborative approach between different healthcare disciplines.49-53 Several strategies have been proposed to enhance care experience for patients with rheumatic conditions, such as promoting an integrated and collaborative multidisciplinary approach, implementing the use of patient reported outcomes measures (PROMs) and PREMs, improving the communication between healthcare providers and patients, and developing shared decision making processes.51,54,55
In our study, people with higher levels of education and those who were working or studying experienced higher levels of person-centered care. The relationship between education and the experience of person-centered care has also been observed in the P3CEQ validation studies.22-24 These associations may reveal social inequalities in care that warrant further investigation, given the limited information in this area. In addition, when we compared the response rates within each socio-demographic subgroup, the categories that responded least to the P3CEQ were smokers, frequent drinkers, drug users, members of patient organizations, and users of alternative medicines. HIV PrEP users, who were significantly younger, had a higher response rate of the P3CEQ compared to the groups of chronic patients. We hypothesize that the association between higher response rates and younger age may be related to the electronic administration of the questionnaire, but this requires further research.
The domain with the lowest score in our study was care planning (item 7). This finding is consistent with the results of the Dutch validation of the P3CEQ and a Norwegian study on the psychometric properties of the same questionnaire.23,24 Individualized care plans for chronic patients are still not widespread in some countries, in contrast to the United Kingdom, where initiatives to develop person-centered and coordinated care are very common.22-24 In Spain, the development of individualized care plans has been considered in some models to improve the management of chronic patients, but these plans often do not take into account patient’s preferences.56-59 Care planning is one of the 5 core domains of person centered and coordinates care, and an individualized care plan should ensure that holistic care is tailored to the needs, preferences, and values of the person.7,22,29 Health goals that are important to patients should also be included in care plans to guide the process of shared decision making. 7 Our findings suggest that more emphasis should be placed on care planning to improve this P3C domain for all patients. Moreover, it should be noted that the term used in Spanish to refer to an individualized care plan may differ among the various models of care for chronic patients established in different regions of Spain.57-59 This lack of consistency reflects the fact that the individualized care plan is a relatively new concept in Spain, and patients may be unfamiliar with it or refer to it by other names.
Our study is one of the first published experiences of implementing the P3CEQ administration in clinical practice and had the largest sample size of the few studies that have used this questionnaire in Spain.2,16,60 Our response rate was similar to the response rate of the UK validation study, but considerably lower than that of the Dutch study.22,24 We hypothesize that the higher response rate observed in the Dutch study may have contributed to the lower mean scores reported. Furthermore, we speculate that a higher response rate within our own sample population may have provided a different perspective on patient experience. There is evidence that response rates to patient-reported measures are influenced by both socio-demographic factors and the methods by which the questionnaires are administered.61,62 In the UK study, patients were sent an envelope with written information and a paper questionnaire to complete, whereas in the Dutch study respondents could choose to complete the questionnaire online or on paper.22,24 Moreover, the Dutch study recruited the sample from the National Panel of people with chronic illness or disability (NPCD), which has an established history of conducting health surveys.24,63 The discrepancy in response rates across various socio-demographic categories in our study suggests that it may be necessary to devise strategies to engage groups with lower participation rates, such as older people who are less familiar with digital tools. Possible approaches for this group of people could include providing additional guidance from nurses or user support specialists or involving family members or caregivers to help them to complete the questionnaires. 2
Our findings offer valuable insights into the quality of care provided to chronically ill patients and shed light on the required improvements to enhance patient satisfaction and the overall healthcare experience. One of the areas that should receive more attention and research is the socio-demographic biases in healthcare and how to correct them. Strategies are needed to improve person-centered and coordinated care for patients with certain chronic conditions, such as skin disease. Another goal for health system should be the implementation of individualized care plans, which should be created with the participation of patients.
A limitation of our study is that the sample size of some categories of the medical condition types was relatively small, for example, cancer. To strengthen the weight of our findings, further studies with larger sample sizes for each category should be conducted. In addition, although many of our patients were poly-medicated and had more than 1 disease diagnosis, we did not specifically collect this information. In future studies, it will be worthwhile to include these data to clearly determine the experience of care in patients with multimorbidity.
As healthcare organizations around the world transform to adopt the patient-value-based healthcare paradigm, assessing the experience of care from the patient’s perspective is crucial. 13 Initiatives to measure person-centered and coordinated care are relatively new in our country. To implement them more systematically, both healthcare providers and patients need to be well informed about the importance of completing PREMs such as the P3CEQ. 64 Finally, it is essential that the results of these measures reach both healthcare professionals and policymakers who bear the responsibility to facilitate improvements in care. 15 The necessary changes will require coherent leadership, transparency policies, aligned management and clinical commitment, and follow-up. 13
Conclusion
To the best of our knowledge, this is one of the first published studies that employed the P3CEQ to evaluate patients’ experiences of P3C in routine clinical practice in Spain and the first to compare the P3C experiences among people with different chronic conditions. Our results showed that men, those with higher levels of education, those in employment and students had better experiences of care, suggesting the possibility of gender bias and social inequalities that should be further investigated and addressed. Statistically significant variations in P3CEQ scores among patients with different long-term conditions highlight the need for a more comprehensive understanding of the unique needs of patients specific to each condition. The lowest score in the care planning domain highlights that policies and strategies should be developed to implement care plans with patient participation in clinical practice. Given the valuable information gained from patient feedback, it is essential to educate both healthcare professionals and patients about the benefits of using PREMs such as the P3CEQ, and to identify and overcome barriers to patient involvement in completing them.
Supplemental Material
sj-doc-2-his-10.1177_11786329241258856 – Supplemental material for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ
Supplemental material, sj-doc-2-his-10.1177_11786329241258856 for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ by Gabriel Mercadal-Orfila, Salvador Herrera-Pérez, Núria Piqué, Francesc Mateu-Amengual, Pedro Ventayol-Bosch, Maria Antonia Maestre-Fullana, Joaquin Ignacio Serrano-López de las Hazas, Francisco Fernández-Cortés, Francesc Barceló- Sansó and Santiago Rios in Health Services Insights
Supplemental Material
sj-docx-1-his-10.1177_11786329241258856 – Supplemental material for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ
Supplemental material, sj-docx-1-his-10.1177_11786329241258856 for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ by Gabriel Mercadal-Orfila, Salvador Herrera-Pérez, Núria Piqué, Francesc Mateu-Amengual, Pedro Ventayol-Bosch, Maria Antonia Maestre-Fullana, Joaquin Ignacio Serrano-López de las Hazas, Francisco Fernández-Cortés, Francesc Barceló- Sansó and Santiago Rios in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329241258856 – Supplemental material for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ
Supplemental material, sj-docx-3-his-10.1177_11786329241258856 for Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ by Gabriel Mercadal-Orfila, Salvador Herrera-Pérez, Núria Piqué, Francesc Mateu-Amengual, Pedro Ventayol-Bosch, Maria Antonia Maestre-Fullana, Joaquin Ignacio Serrano-López de las Hazas, Francisco Fernández-Cortés, Francesc Barceló- Sansó and Santiago Rios in Health Services Insights
Footnotes
Acknowledgements
The first author, Dr Gabriel Mercadal-Orfila, obtained permission to use the P3CQ for this study. Authors wish to thank Pilar Alba for her editorial assistance (financed by FARUPEIB). INSA-UB Maria de Maeztu Unit of Excellence funded by MICIN/AEI/FEDER, UE (CEX2021-001234-M).
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GM and NP researched literature and conceived the study. All authors were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. NP, GM, and SR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical Approval
The Ethics Committee of Research of the Balearic Islands (Comitè d’ètica de la investigació de les Illes Balears) approved this study (REC number: IB 5117/23 EOm).
Guarantor
NP.
Data Availability Statement
Data are available upon justified request to the correspondence author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.