
Abstract
Several targeted medication reconciliation (MR) initiatives have been introduced to reduce the number of medication discrepancies (MDs). The real-life quality of medication lists at hospital admission has however not been comprehensively investigated in the last decade. We aimed to examine the frequency and potential clinical relevance of MDs at hospital admission and investigate whether certain characteristics are associated with MDs. Patients ⩾18 years old admitted to medical wards at 4 hospitals in Norway were included. MR was performed, and discrepancies between the reconciled medication list and the medication chart were identified. The potential clinical relevance was assessed in a short-term and long-term perspective. We included 250 patients and 201 (80%) had 1 or more MDs, mean 3.2 (SD 2.9) per patient. Out of 824 identified MDs, 171 (20.8%) and 362 (43.9%) were of moderate, major, or extreme potential clinical relevance in short- and long-term perspective, respectively. The risk of MDs increased with increasing age, increasing number of medications, and the use of multidose drug dispensing. Although several targeted MR initiatives have been launched, the frequency of MDs upon hospital admission is still high. However, the potential clinical relevance of the MDs seems less severe, which indicates an improvement.
Keywords
Background
Inaccurate medication lists have been, and still are, a challenge for patient safety internationally, especially in transitions of care.1-6 Importantly, an inaccurate medication list is a poor decision basis for the prescriber and causes a risk of incorrect treatment to the patient. 7 Medication reconciliation (MR) is an acknowledged method for obtaining a complete and correct medication list that reflects what the patient actually is using. 8 A Norwegian multicenter study from 2011 revealed a disconcerting statistic: as many as 8 out of 10 hospitalised patients had 1 or more medication discrepancies (MD) upon admission. 3 Furthermore, the study showed that most of the MDs could potentially harm the patient in a long-term perspective. 3
In the last decade, several targeted MR initiatives have been developed and implemented.6,8-13 In Norway, a National Patient Safety Strategy was launched in 2011, in which MR was one of the targeted areas. 12 Subsequently, this campaign has evolved into a more comprehensive framework, the National Action Plan for Patient Safety and Quality Improvement, signifying a continued commitment to enhancing patient care and safety, including medication safety. Nationally shared medication lists have been implemented in several countries.9,14,15 The Norwegian National Summary Care Record (SCR) was launched by the end of 2017.10,16 This digital tool serves to provide both primary and secondary healthcare practitioners with uniform access to critical healthcare data concerning individual patients, including an overview of current prescriptions, and information about which medications have been recently dispensed by pharmacies. 16 Furthermore, as MR is a main initiative for reducing MDs, hospitals have implemented local procedures for conducting MR.7,17
Despite numerous measures aimed at reducing MDs, the real-life quality of medication lists at hospital admission has not been investigated comprehensively in the last decade. Furthermore, the authors of a recent Cochrane review on medication reconciliation call for research on high-risk populations and with multicenter designs. 18 Therefore, the aim of this multicenter study was to examine the frequency and potential clinical relevance of MDs revealed by MR when medical patients are admitted to a hospital, and furthermore investigate whether certain medications or patient characteristics are associated with MDs.
Methods
Study team and preparations
The study team consisted of 7 data collectors; 3 master’s students in pharmacy and 4 pharmacists. This team was responsible for the inclusion of patients and data collection. All data collectors had training in conducting medication reconciliation (MR), in adherence to Integrated Medicines Management (IMM).19,20 Additionally, 5 physicians from various hospital wards participated in assessing the potential clinical relevance of the identified MDs.
Patients and study design
The multicenter study took place across 4 different hospitals in South-Eastern Norway. We included medical patients ⩾18 years admitted to different internal medicine wards: 1 acute geriatric ward, 1 internal medicine ward, 2 nephrology wards (including 1 focussed on diabetes), and 1 emergency department. To best align with the 2011 study, 3 we aimed to include the same number of patients in the current study, that is, 50 patients from each ward and in total 250 patients. Patients were consecutively included after written, informed consent from October 2021 to May 2022. Terminally ill patients, patients isolated due to infections, previously included patients, and patients who were not able to communicate in either Norwegian or English and where a translator was not available, were not eligible for inclusion.
Data collection
Figure 1 describes the steps in patient inclusion and data collection. To ensure a real-life status of the quality of the medication lists at hospital admission, MR was performed according to a predefined inclusion window to give ward staff enough time to complete routine MR according to local procedures. The inclusion window was defined as follows: All patients had to be hospitalised for at least 24 hours before inclusion. When local procedures accepted that routine MR was completed later than 24 hours after admission, the time frame for inclusion was expanded accordingly. Notably, when routine MR was documented to have been performed by ward staff, patients were included consecutively. Patients were included Monday to Friday, and for patients admitted during weekends, the inclusion window was extended. Study MR was conducted within 24 hours post-inclusion.

The steps in patient inclusion and data collection.
Information about the patient’s actual medication use before hospitalisation was collected from a minimum of 2 different information sources. If the patient was capable of giving information about their medication use, a structured interview with the patient was conducted. The SCR was routinely used to validate information regarding prescribed medications. Other information sources, like next of kin and home care nurse, were utilised as needed, such as when patients received assistance with managing their medications. Additional sources could be community pharmacies, multidose drug dispensing (MDD) pharmacies, general practitioners, nursing homes, and patient records.
In addition to the medication chart, the following information was recorded from the patient record or by the patient interview: age, gender, where the patient was admitted from, whether the patients normally administered the medications themselves or received assistance, whether routine MR was documented to have been carried out during the current hospitalisation and if the patient received medications by an MDD system.
Medication discrepancies
A medication discrepancy (MD) was defined as any inconsistency between the patient’s medication chart, that is, the patient’s prescribed medications at the hospital at the time of inclusion, and the patient’s actual medication use before hospitalisation, as revealed by MR.
Only medications classified in the anatomical therapeutic chemical (ATC)-system were assessed for MDs. This approach excluded dietary and herbal supplements. For each MD, the active pharmaceutical ingredient (API), medication formulation and strength, ATC-code levels 3 and 5, administration schedule (regular or on demand), and a short description of the MD were recorded. In addition, for all MDs, whether the actual usage was correctly documented in the physician’s admission note in the hospital record or not was also recorded.
The MDs were classified according to the following categories 3 : (1) Commission of medication (medication prescribed in the medication chart was not being used by the patient prior to hospitalisation), (2) omission of medication (a medication used by the patient prior to hospitalisation was missing in the patient’s medication chart at the hospital), (3) incorrect strength, (4) incorrect medication formulation, (5) incorrect dose (including erroneous documentation of regularly used medications and medications used when needed) and (6) incorrect administration time of day.
Potential clinical relevance
The potential clinical relevance of each MD was assessed collectively by the data collector and 1 physician at each hospital ward. A four-point severity scale for clinical relevance was utilised to characterise the potential implications for the patient if the MD remained undetected and uncorrected. The scale encompassed the following categories 21 : (1) Extreme clinical relevance, including MDs that could cause death or serious or irreversible injury, (2) Major clinical relevance, including MDs that could cause severe or reversible injury, or lack of evidence based treatment, (3) Moderate clinical relevance, including MDs where correction of the MD would give a moderate advantage for the patient and (4) Minor clinical relevance, where correction of the MD would have little clinical relevance for the patient, for example, small deviations in administration time. During the assessments, the patients record including laboratory results (for example renal function) were available and accessible if necessary.
All MDs were assessed for their potential clinical relevance for the individual patient, in a short-term perspective (defined as the MD remaining for a few days of hospital stay), and in a long-term perspective (defined as the MD remaining a permanent part of the patient’s medication list after discharge). 3
Potential risk factors
Patient-related characteristics that were investigated as potential risk factors for MDs were:
Statistics
Data was analysed with IBM SPSS Statistics 28.0.0.0. Descriptive statistics are given as means and standard deviations (SD) for continuous variables and as frequencies for categorical variables. An independent samples t-test was used for continuous variables and Pearson’s χ2 test was used for categorical variables when testing for differences between groups of patients with and without MDs. P-values of <.05 were considered statistically significant.
Ethical considerations
The Regional Committees for Medical and Health Research Ethics (REK) assessed the study and found that approval from them was not necessary. Supplemental Material 1 shows the original study protocol and the protocol amendments. Supplemental Material 2 shows the STROBE Checklist. The study was approved by the Norwegian Center for Research Data (NSD, reference 129324), and the data protection officer at each hospital approved the collection of data at the respective hospitals. Patients, or their next of kin if the patients were unable to consent, gave written informed consent before the patients were included. All data was de-identified and stored on the University of Oslo’s Services for Sensitive Data.
Results
A total of 250 patients were included in the study, see Figure 2. The patients had a mean age of 71.1 years, and used a mean of 8.9 medications after the completion of medication reconciliation. Furthermore, 218 patients (87%) were admitted from their homes. For all patient characteristics see Table 1.

Flow chart describing the inclusion of patients.
Patient characteristics in the 250 patients included in the study.
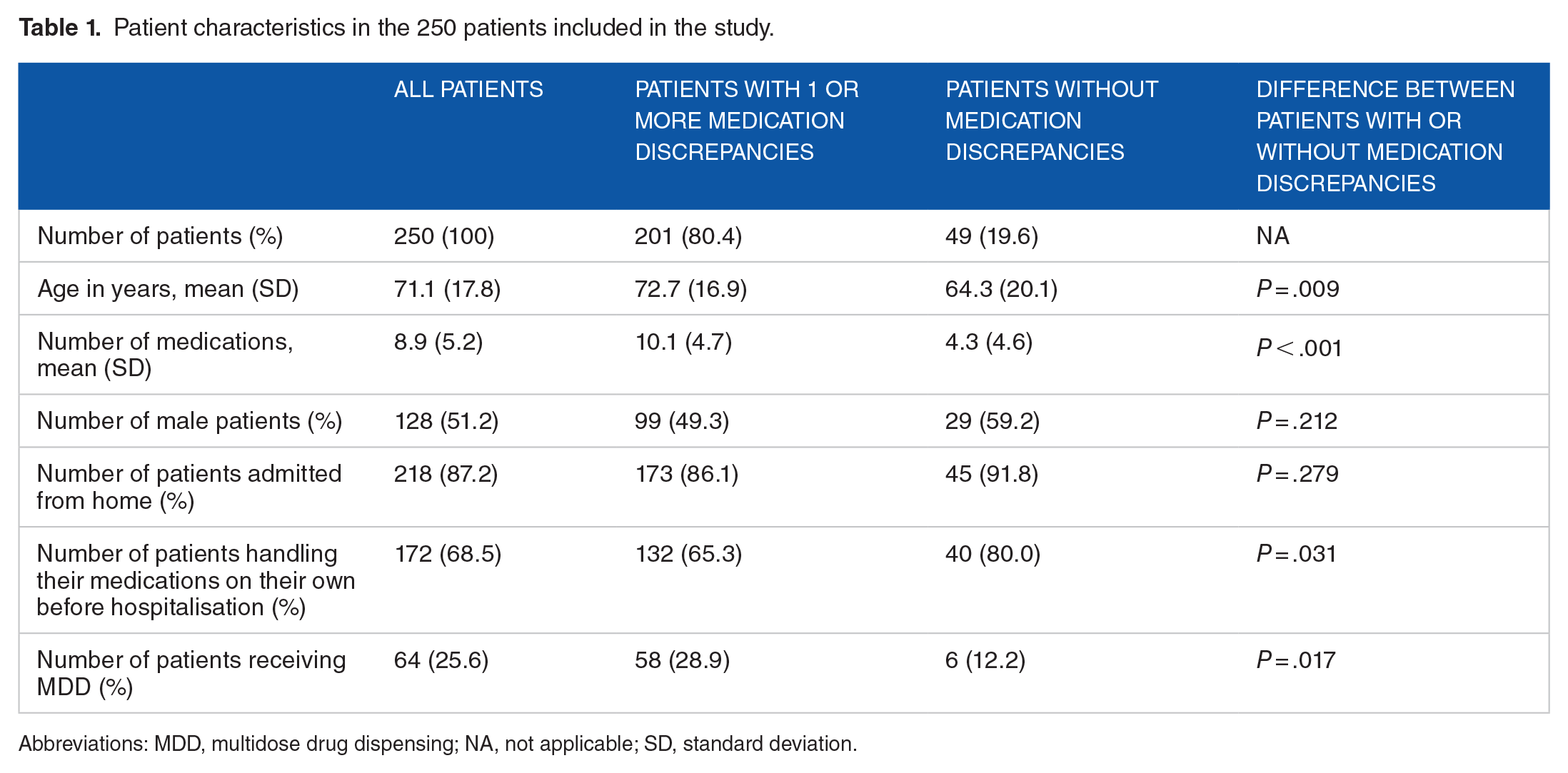
Abbreviations: MDD, multidose drug dispensing; NA, not applicable; SD, standard deviation.
A total of 201 patients (80%) had at least 1 MD. For all patients, the mean number of MDs was 3.2 with a standard deviation (SD) of 2.9, whereas the mean among the patients with a minimum of 1 MD was 3.9 (SD 2.7). In total 824 MDs were revealed, and of these 515 (63%) were associated with regularly used medications. The number of each type of MD and the most frequently implicated medications can be found in Table 2. The most frequent medications involved in on-demand MDs were paracetamol (35 MDs), salbutamol (19 MDs), ibuprofen (11 MDs) and zopiclone (10 MDs).
Distribution of the 824 medication discrepancies (MDs) according to type of medication discrepancy and medications most frequently involved.
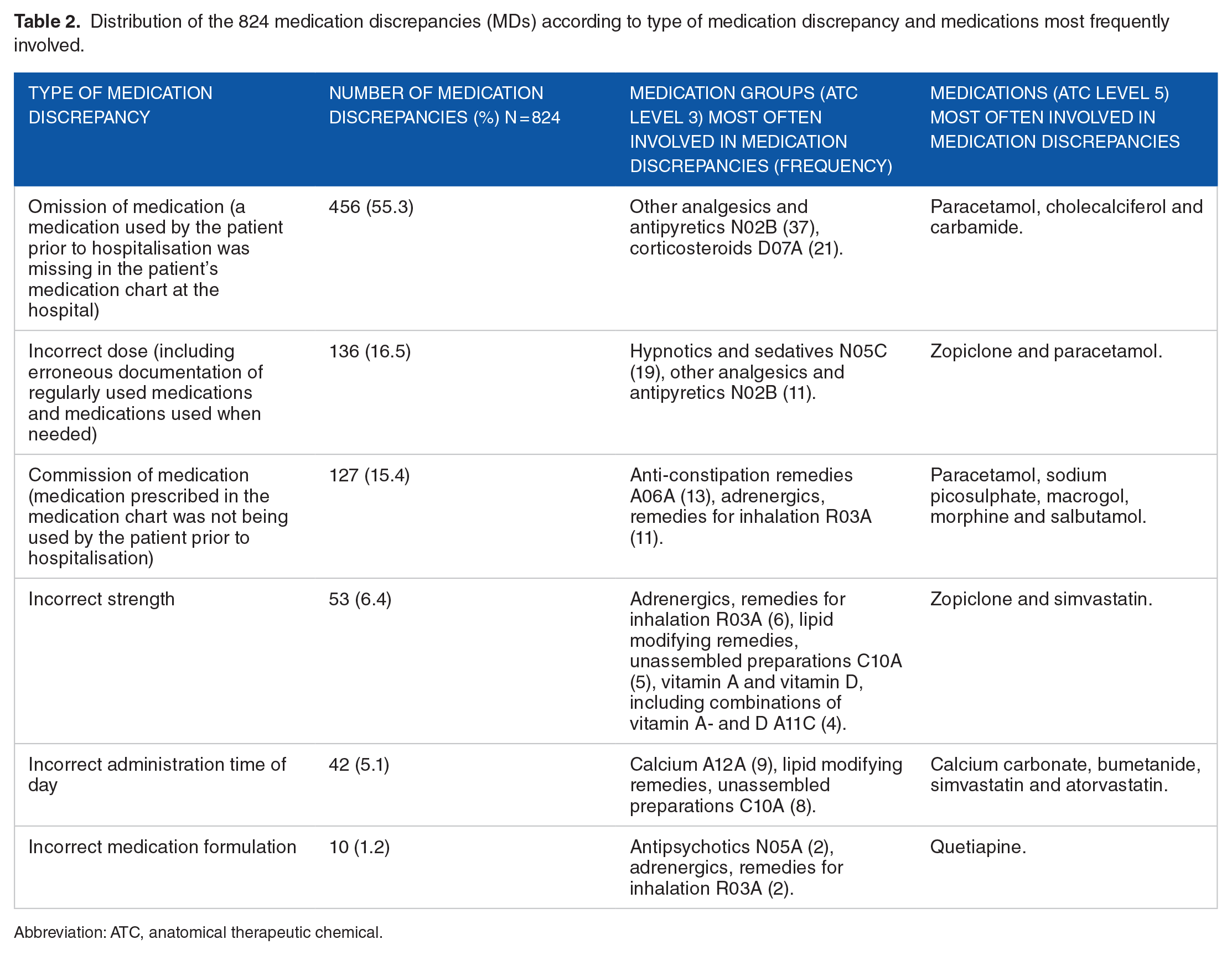
Abbreviation: ATC, anatomical therapeutic chemical.
For 213 (26%) of the 824 identified MDs between the reconciled medication list and the medication chart, the patient’s actual use of the medication had been correctly documented in the physician’s admission note within the hospital record. Consequently, these particular MDs were introduced during the hospital stay. Among these MDs, the predominant type was omission of a medication (61%), followed by incorrect dose (13%), as shown in Figure 3.

Description of key results regarding the medication discrepancies (MDs) between the patient`s actual medication use (that is, the reconciled medication list) and the medication chart, where actual use were correctly documented in the physician’s admission note in the hospital record.
Among the 201 patients with at least 1 MD, 72% had 1 or more MDs of extreme, major, or moderate clinical relevance in either a short-term or long-term perspective, Table 3. Of all 824 MDs, 21% and 44% of the MDs were assessed to be of extreme, major, or moderate potential clinical relevance in a short-term and long-term perspective, respectively.
Potential clinical relevance of the 824 medication discrepancies (MDs), if not corrected during a normal hospital stay of a few days (short-term), or if remained part of the patient’s medication list after discharge (long-term), and the most frequently involved medications.

Abbreviation: ATC, anatomical therapeutic chemical.
There were 145 patients (58%) where routine MR was documented to have already been performed by the hospital staff. Of these 107 (74%) had 1 or more MDs. Of these 145 patients, 74 (51%) had 1 or more MDs of extreme, major, or moderate clinical relevance in either a short-term or long-term perspective.
Notably, patients with 1 or more MDs were statistically significantly older than those without MDs, see Table 1. Additionally, a significantly higher percentage of patients managing their own medications was observed in patients without MDs compared to patients with MDs. Lastly, the percentage of patients with MDs who received MDD was higher compared to patients without MDs.
Discussion
This multicenter study uncovered concerning results: despite several initiatives aimed at curtailing MDs, approximately 80% of the patients had at least 1 MD between the medication chart and the actual medication use prior to hospitalisation. Our findings are consistent with the Norwegian multicenter study conducted in 2011, 3 that is, prior to the earlier mentioned initiatives. A similar study conducted in Sweden, encompassing both inpatients and outpatients, found a slight reduction in MDs from 2012 to 2022. 7
Fortunately, despite the high frequency of MDs, the majority were classified as of either minor or moderate potential clinical relevance, and less than 2% of the MDs as of potential extreme clinical relevance in a short-term and long-term perspective. The relatively low frequency of clinically relevant MDs aligns with findings from other studies conducted in settings that have also directed increased attention towards MR in recent years.17,26 However, in the Norwegian multicenter study from 2011, 3 the frequency of potentially extremely clinically relevant MDs was 4.8%, and it is reasonable to infer that the decrease in clinically relevant MDs can be attributed to the increased focus on MR. Moreover, the availability of medication information through the SCR has likely contributed to this finding.11,27
Interestingly, although the SCR was available for ward staff, the most common MD in our study was the omission of a medication, comprising more than half of all identified MDs. This finding is in line with a recent study investigating MDs between medication lists in primary care after implementation of the SCR. 27 Furthermore, omissions commonly were among the most frequent MDs in earlier studies.2,3,7,17,26,28
In the current study nearly 40% of the MDs concerned medications used on demand. The most frequent of these MDs included both paracetamol and ibuprofen that can be bought ‘over the counter’, which may partly explain the high omission rate despite the implementation of the SCR. This underlines the importance of the patient interview to reveal the actual use of medications.
Surprisingly, for as many as one-fourth of all the MDs, the medication list in the physician’s admission note in the hospital record reflected the patient’s actual use of the medication, even if the hospital medication chart did not. This outcome has not been explored before and the finding was unexpected. Possible reasons might be that an intended change in the prescription was not documented in the patient’s record, or that an unintended error occurred during the prescription in the hospital medication chart. The most frequent medication groups involved in omissions were analgesics, antipyretics, and dermatological corticosteroids, and one may wonder if it is a conscious choice by the physician not to prescribe these in the medication chart if they considered there is no need for these medications during the hospital stay. Future studies should aim to explore the reasons for such MDs, for example, are they intended or unintended, to obtain insight and knowledge on how to reduce MDs that are introduced during the hospital stay.
Among patients for whom routine MR was documented as performed by ward staff, more than half still had 1 or more MDs of extreme, major, or moderate clinical relevance, in either a short-term or long-term perspective. This result is in accordance with previous studies showing that the quality of documented routine MR might be uncertain. 29
Increasing age, number of medications, and the use of MDD were revealed as potential risk factors for MDs. These findings align with previous research.17,22,30 Although MDD is an acknowledged aid to securing correct medication use, it may also be a potential source for MDs. 31 Conversely, patients who managed their medications independently displayed a lower risk of encountering MDs. This insight could potentially guide hospital staff in prioritising patients for MR.
One notable strength of this study lies in its alignment with the 2011 study, 3 being conducted with a similar method and with 1 exception at the same hospitals. This facilitates comparisons of the 2 sets of findings, relating them to proposed changes and improvements that have been made over the years. Additionally, the study benefits from the inclusion of many patients across various hospitals, thereby enhancing the representativeness of the results within this regional healthcare context. The risk of selection bias is regarded to be low as the data collectors did not have access to the hospital record before inclusion.
The fact that the clinical relevance of the MDs was evaluated by a physician often involved in the patient care, might be considered as a limitation to the study as this method could potentially have raised the threshold for considering the MDs as clinically relevant. The MDs were evaluated for clinical relevance together with a representative from the study team with an uneven balance of power, potentially favouring the opinion of the experienced physician, which is not unfamiliar. 32 However, it is considered a strength to have 2 different professional perspectives represented by the pharmacist and physician in the evaluation of clinical relevance.
The future holds various digital solutions, possibly reducing medication errors in the healthcare system, for instance, the Shared Medication List which is being launched in Norway these days. 9 The Shared Medication List and similar systems are considered useful tools to improve communication regarding medication use across different levels of care. Importantly, the results of the current study underline the importance of conducting the patient interview, since digital tools will not provide information about for instance adherence. A concern revealed in this study is MDs seemingly being introduced in the hospital’s internal system, where the medication list in the admission note differed from the medication chart. This needs further investigation and may suggest a need for improved training for the hospital staff in these systems to minimise medication errors in the future.
Conclusions
Although several targeted measures on MR have been launched in Norway, the frequency of MDs upon hospital admission is still high, especially among elderly, patients with polypharmacy or the use of a multidose drug dispensing system. Despite the high frequency of MDs, the potential clinical relevance seems less severe, which indicates an improvement.
Supplemental Material
sj-docx-1-his-10.1177_11786329241254202 – Supplemental material for Medication Discrepancies in Hospitalised Medical Patients – Status After a Decade With Targeted Medication Reconciliation Measures, a Cross-sectional Multicenter Study
Supplemental material, sj-docx-1-his-10.1177_11786329241254202 for Medication Discrepancies in Hospitalised Medical Patients – Status After a Decade With Targeted Medication Reconciliation Measures, a Cross-sectional Multicenter Study by Helena Zaitzow Mikaelsen, Ingeborg Hjalland Ulla, David Karimi, Liv Mathiesen, Kirsten Kilvik Viktil, Malin Olsen Syversen, Lilli Minh Nguyen, Kajsa Rebecka Bengtsson, Marc Vali Ahmed, Krystina Parker, Anja Fog Heen, Anne Mette Njaastad, Rehman Qazi and Marianne Lea in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241254202 – Supplemental material for Medication Discrepancies in Hospitalised Medical Patients – Status After a Decade With Targeted Medication Reconciliation Measures, a Cross-sectional Multicenter Study
Supplemental material, sj-docx-2-his-10.1177_11786329241254202 for Medication Discrepancies in Hospitalised Medical Patients – Status After a Decade With Targeted Medication Reconciliation Measures, a Cross-sectional Multicenter Study by Helena Zaitzow Mikaelsen, Ingeborg Hjalland Ulla, David Karimi, Liv Mathiesen, Kirsten Kilvik Viktil, Malin Olsen Syversen, Lilli Minh Nguyen, Kajsa Rebecka Bengtsson, Marc Vali Ahmed, Krystina Parker, Anja Fog Heen, Anne Mette Njaastad, Rehman Qazi and Marianne Lea in Health Services Insights
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
HZM, IHU, DK, LM, KKV, and ML conceptualised the study and developed the design. Material preparation was performed by HZM, IHU and DK. Data collection was performed by HZM, IHU, DK, MOS, LMN, KRB and ML. MA, KP, AFH, AMN and RQ conducted the assessments of clinical relevance together with the data collectors. Data analysis was performed by HZM, IHU, DK, LM and ML. The first draft of the manuscript was written by HZM and IHU. HZM, IHU, LM and ML conducted several revisions of the manuscript. All authors read and approved the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.