
Abstract
This retrospective population-based analysis assessed variations in urgent healthcare use by children and young people (CYP) across UK nations (England, Scotland and Wales) between 2007 and 2017. The study focused on urgent hospital admissions, short stay urgent admissions (SSUA) and Emergency Department (ED) attendances among CYP aged <25 years, stratified by age groups and Index of Multiple Deprivation (IMD) quintile groups. A linear mixed model was used to assess trends in healthcare activity over time and across deprivation quintiles. Urgent admissions, SSUA and ED attendances increased across all deprivation quintiles in all studied nations. Increasing deprivation was consistently associated with higher urgent healthcare utilisation. In England, the rise in urgent admissions and SSUA for CYP was slower for CYP from the quintile of greatest deprivation compared those from the least deprived quintile (respective mean differences 0.69/1000/y [95% CI 0.53, 0.85] and 0.25/1000/y [0.07, 0.42]), leading to a narrowing in health inequality. Conversely, in Scotland, urgent admissions and SSUA increased more rapidly for CYP from all deprivation quintiles, widening health inequality. Understanding the differences we describe here could inform changes to NHS pathways of care across the UK which slow the rise in urgent healthcare use for CYP.
Background
Urgent admissions of children and young people (CYP, including individuals aged up to 25 years) in the UK have risen by at least 40% since 2000,1-4 with a temporary halt in the rise in admissions during the SARS-CoV-19 pandemic. 5 Many ‘urgent’ admissions may not be truly ‘urgent’; up to 60% of Emergency Department (ED) attendance in CYP is for non-urgent 6 and 90% of CYP presenting to ED are not admitted for inpatient paediatric care. 6 Between 25% 7 and 50% 8 of urgent admissions might be managed outside the hospital setting. Given the increased pressure on the NHS post pandemic, there is an urgent need to understand and then address the increasing demand on ED and paediatric NHS services for acutely unwell children.9-11
Health inequality, defined as an unfair difference in health existing between individuals and groups, 12 are evident in CYP urgent admissions in the UK since urgent admissions are strikingly higher for those from deprived communities.2-4 Between 2007 and 2017, CYP from the most deprived quintile for deprivation in England had the highest urgent healthcare use of all quintiles. 2 Across England and Wales in 2015-16, CYP from the most deprived communities were 50% to 70% more likely to present to ED compared to those from the least deprived communities. 3 In Scotland, during the period 2000 to 2013, 27% of all urgent hospital admissions were CYP from the lowest quartile of deprivation compared to 15% from the least deprived. 4 Reasons for unscheduled healthcare use being greater in CYP from communities with greater deprivation are complex and include a higher burden of illness and lack of access to scheduled care.
Health policy was devolved to the four UK nations in 1999, and the different nations have subsequently applied diverging health policies.13,14 For example while NHS England focus on choice and competition, with money following the patient, NHS organisations in other nations have retained more simple models where regions are funded to provide care for their population. 13 A second difference between UK nations is their different strategies to integrate health and social care. 15 These differing policies may have had different impact on urgent healthcare use by CYP and the impact of different policies on patient outcomes could give insight into which policies are more effective in providing healthcare. Here we used data collected by the Royal College of Paediatrics and Child Health as part of a project which sought to model clinical demand on child health services through to 2040 16 to describe the change in the health inequalities gap, as evidenced by higher urgent healthcare use by CYP from the most deprived communities, in UK nations between 2007 and 2017.
Methods
Study design
We conducted a retrospective population-based analysis of healthcare activity using routinely collected data in the four UK nations. The following healthcare activity outcomes were sought from each nation for the period 2000 to 2018: urgent hospital admissions (synonymous with emergency or unplanned admissions); short stay urgent admissions (SSUA, defined as where the admission and discharge took place on the same date); ED attendances. Each outcome was standardised per 1000 in the age group per deprivation quintile using national population denominators. Eligible patients were those aged <25 years, stratified by age groups 0, 1-4, 5-9, 10-14, 15-19, 20-24 years. Deprivation was expressed as Index of Multiple Deprivation (IMD) quintile group. In each nation the IMD is calculated by assigning a score to small geographic areas which considers income, employment, education/training, health, crime, housing and living environment. Each geographic area is then ranked from most (rank of 1) to least deprived. Each of the UK nations has its own methodology for deriving IMD but include mostly consistent domains. The supplement provides further details on how IMD is derived in England, Scotland and Wales. The need for informed consent was waived by the North of Scotland Research Ethics Committees, because of the retrospective nature of the study.
Data availability
England. Data for number of urgent admissions, SSUA and ED attendance between 2007 and 2017 were provided by Hospital Episode Statistics. 17 Data were stratified by both IMD quintile group and age (infant, 1-4 years, 5-9 years, 10-14 years, 15-19 years and 20-24 years).
Scotland. Data were available 2000 to 2018 for number of urgent admissions and SSUA, and ED attendances data from 2009 to 2018. Data were provided by Information Services Department of the Scottish Government 18 and were stratified by Scottish IMD quintile group or by the age group categories described earlier.
Wales. Urgent admission and SSUA data were available from 2000 to 2018 and provided by the Secure Anonymised Information Linkage Databank. 19 ED attendance data were available from 2009 onwards. Data were stratified by the Welsh IMD quintile or by the age group categories described earlier.
Northern Ireland. No data were available.
Analysis
The outcomes were: urgent admission/1000; SSUA/1000; number of ED attendances/1000. Due to differences between nations in definitions of admissions and derivation of IMD quintiles it was not valid to include data from all nations in a single model. The analysis first described healthcare activity for each nation with stratification by year and IMD quintile. Then a linear mixed model was used to show how each healthcare activity metric changed over time (linear variable) and deprivation quintile (categorical variable). Finally, an interaction term ‘deprivation*year’ was then introduced to the mixed model to describe how outcomes changed by quintile over time (with reference to the least deprived quintile) for each nation. Standard statistical software used (IBM/SPSS version 27.0.1.0).
Results
Data available
Urgent admission and SSUA were analysed using data from England, Scotland and Wales between 2007 and 2017. The ED analysis considered data from England, Scotland and Wales for period 2009 to 2017. Table 1 presents mean outcome data stratified separately by nation, deprivation quintile group and year. Urgent admissions and SSUA were higher in Wales and ED attendance higher in England compared to the other nations.
Mean (SD) values for healthcare outcomes for individuals aged <25 years stratified by nation, deprivation and year.
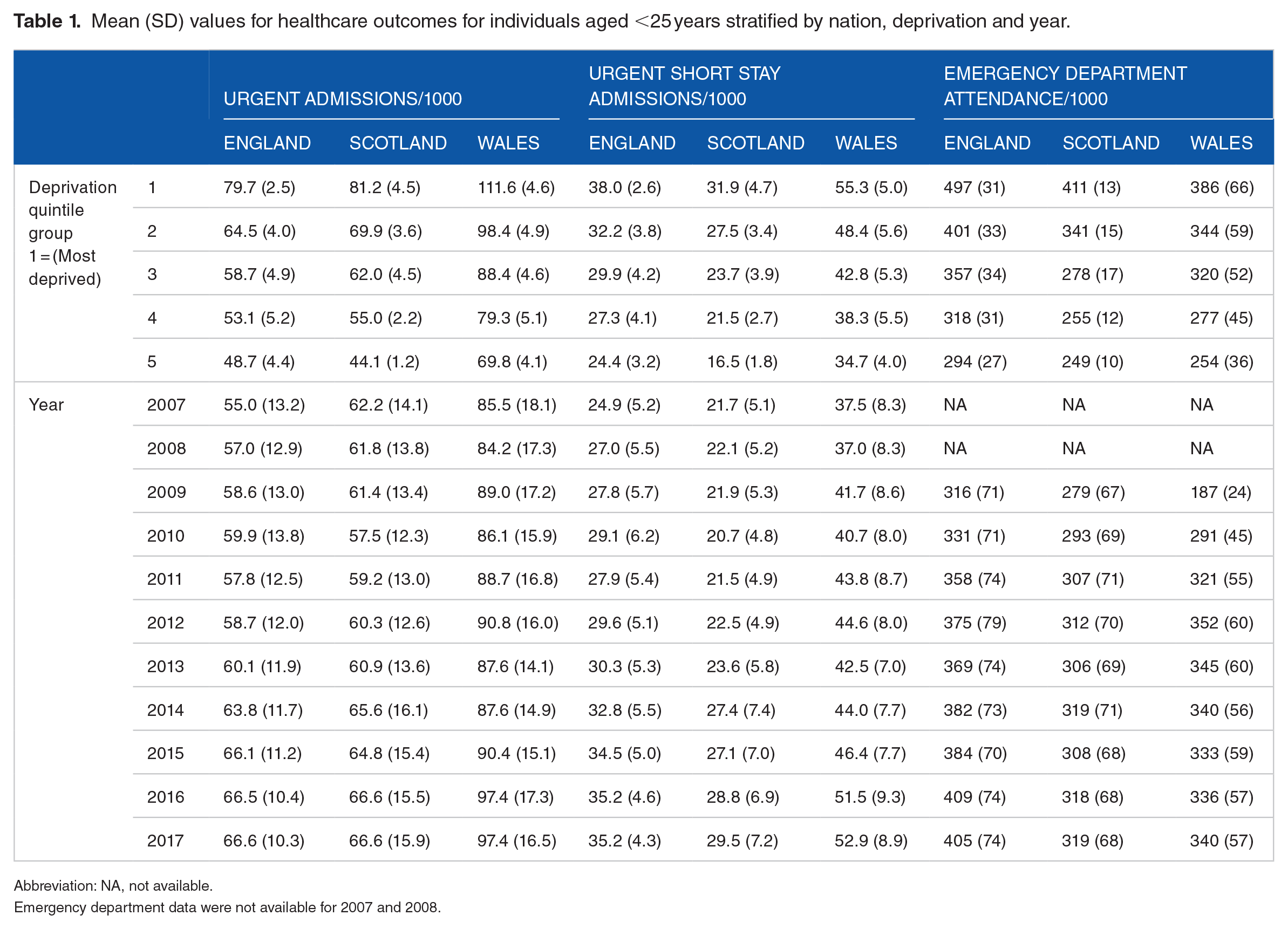
Abbreviation: NA, not available.
Emergency department data were not available for 2007 and 2008.
Outcomes over time with adjustment for deprivation
Urgent admissions
In all three nations, the number of urgent admissions/1000 increased in a step-wise manner from least to most deprived quintiles, Tables 1 and 2. Urgent admissions also rose between 0.6 and 1.2/1000 per year, Table 2 and Figure 1.
Results from main effects general estimating equation where each of the admission outcomes was related to deprivation and time for each nation. The numbers in square brackets are 95% confidence intervals.

Abbreviation: ref, reference.
Differences are significant with P < .001 unless stated otherwise.
P > .05.

Mean of all urgent admissions per 1000 children and young people using data between 2007 and 2017 from England, Scotland and Wales with stratification by quintile of deprivation. Quintile 1 = most deprived quintile.
Short stay urgent admissions
There was an increase in SSUA from least to most deprived quintiles in all 3 nations urgent admissions, Tables 1 and 2. Over time SSUA rose in all nations by between 0.8 and 1.4/1000 per year, Table 2 and Supplemental Figure 1.
ED attendance
ED attendance increased in a step-wise manner from least to most deprived quintiles between 2009 and 2017, Tables 1 and 2. There was a rise in ED attendance in England (mean change 9.7/1000 per year) and Scotland (mean change 2.8/1000 per year) but there was no significant change for Wales, Table 2, Supplemental Figure 2.
Interaction between time and deprivation
Urgent admissions
In England, relative to the quintile of least deprivation, urgent admissions rose more slowly for CYP from quintile of greatest deprivation (mean difference 0.69/1000 per year [95% CI 0.53, 0.85]), and rose faster for CYP from the middle and next-to-least-deprived quintiles, Table 3. In Scotland, the rise in urgent admissions was greater for all CYP compared to those CYP from the quintile of least deprivation, with no evidence of a step-wise increase with increasing deprivation, Table 3. In Wales urgent admissions rose equally across all quintiles with the exception of a faster rise of borderline significance in admissions for CYP from the next-to-least-deprived quintile relative to the least deprived quintile (0.43/1000 per year [0.01, 0.85)], Table 3.
Coefficient from interaction term between deprivation and time in the general estimating equation where outcomes was related to deprivation and time.

Abbreviation: Ref, reference.
Differences are significant with P < .001 unless stated otherwise.
P > .05.
Short stay urgent admissions
In England, relative to the quintile of least deprivation, the rise in SSUA was less steep for CYP from the quintile of greatest deprivation (0.25/1000 per year [0.07, 0.42]) and steeper for the three middle quintiles, Table 3. For Scotland, SSUA from CYP rose more steeply in all quintiles relative to the quintile of least deprivation with some evidence of a step-wise increase with increasing deprivation, Table 3. In Wales SSUA rose faster for CYP from the middle 3 quintiles of deprivation relative to the least deprivation; rises in SSUA for CYP from the quintiles with most and least deprivation did not differ, Table 3.
ED attendances. In all 3 nations, ED attendances increased faster in the next-to-least-deprived quintile and middle quintile for deprivation relative to the quintile of least deprivation, Table 3. In England, but not Scotland or Wales, the rise in ED attendance was steeper for CYP from the quintile of greatest deprivation relative to the quintile of least deprivation.
Further analyses
Period 2000-2018
Analysis of urgent admission data between 2000 and 2018 for Wales and Scotland yielded results which were consistent that those from 2007 to 2017 presented in Tables 1 to 3, see Supplemental Tables 1 and 2 and Supplemental Figure 3.
Age-group specific trends
Only data from England could be stratified by both age group and deprivation. Results are presented in Supplemental Tables 3 and 4.
Discussion
This study’s main finding was that the difference in urgent admissions between CYP from the most and least deprived quintile became smaller between 2007 and 2017 in England, whilst in Wales the difference was unchanged and in Scotland the gap became greater. This apparent narrowing of the ‘deprivation gap’ in England reflected ‘catch up’ in admission rates for CYP from the least deprived communities relative to the least deprived communities. Generally, the rise in urgent admissions was slowest among CYP from the least deprived quintiles and faster among CYP from quintiles of intermediate deprivation (ie, not greatest or least deprivation). The use of historical data to understand how the natural experiment of devolving NHS across UK nations may identify policies which could reduce (or inadvertently increase) admissions, and this understanding could inform future policy in the UK.
The focus of the analysis was comparing unscheduled healthcare activity between CYP from the quintiles of greatest and least deprivation. When we compared admissions of CYP from the second, third and fourth quintiles with admissions for CYP from the least deprived quintile, the rate of change was similar or greater than for the least deprived quintile. Table 3 shows that in all nations the highest change in number of admissions and ED presentations was most commonly seen for CYP from the middle quintile for deprivation relative to CYP from the quintile of least deprivation. These observations suggest that describing health inequalities as a gap between CYP from the most and least deprived quintiles may not give complete insight into the complex relationship between deprivation and health outcomes.
We are not aware of previous work which has combined paediatric healthcare utilisation data from different UK nations. Work published more than a decade ago has compared health outcomes between the UK nations20,21 but there have been no more recent simila analyses. Our work is consistent with studies reporting a rise in the number of urgent admissions and ED attendances in CYP from more deprived communities.2-4 Whilst relatively little insight into improving healthcare outcomes can be gained from comparisons between the UK and other nations due to fundemental differences in healthcare systems22,23 useful information may be gained from comparison of child health outcomes between UK nations following the natural experiment of devolution which commenced in 1999.13,24
This study was not designed to explain the reasons behind the changing gap in urgent admissions and ED attendance among CYP across UK nations, nor the observed steeper rise in admissions for CYP from intermediate deprivation quintiles. The mostly linear upward trend in admissions, seen in Figure 1, suggests that no single policy change is important; policies applied across all UK nations, such as European working time directive 25 and the policy of 4-hour wait in ED, 26 may not be singularly relevant to the observed trend. The worldwide financial collapse in 2008 and subsequent austerity in UK public health spending 27 might be expected to have had a smaller impact on least compared to the most deprived communities, making it seem less likely to explain the relative rise in urgent admissions for the least deprived quintiles in England. Increased attendances from the least deprived quintile might be explained by the healthcare-seeking behaviour, 28 observed in adults across England. However, this increase was not seen in Scotland, so it again seems unlikely that the same pattern fully applies to the healthcare utilisation behaviours of CYP. The training standards for physicians, regulated by the General Medical Council (GMC), 29 and nurses, regulated by the Nursing and Midwifery Council (NMC), 30 are consistent across the UK. As such, variations in the confidence of these healthcare professionals to assess acutely unwell CYP are unlikely to make a substantial contribution to the associations described.
Pathways of unscheduled care for CYP are likely to differ between nations 15 and explain some of our results for those from the most deprived quintile, and such variation is previously described within England bronchiolitis admissions. 31 National and regional pathways may be dependent on deprivation, NHS funding, bed capacity and population density, and such factors are not equally distributed across the UK. 15 For example, funding across the four nations is based on the Barnett formula, and in 2020/21 Northern Ireland, Scotland and Wales respectively received 14%, 11% and 6% above the UK average. 32
CYP are more likely to live in communities with the greatest deprivation, and this may partly explain the increased healthcare use we report for CYP from the more deprived quintile. This unequal distribution of CYP per capita across quintiles of deprivation would not explain the rise in urgent health care use for CYP from the least compared to the most deprived quintiles and may underestimate the magnitude of the rise. Assuming that the unequal distribution of CYP across quintiles of deprivation is mostly consistent between nations and the period 2007 and 2017, this inequity will not explain the change over time we report.
There are at least three stages of decision making along a pathway of a child’s care where deprivation may have influence leading to increased or reduced chance of admission. First, the CYP or their parent/carer’s understanding of how to access the NHS may differ by deprivation, for example, children from more deprived communities are more likely to present to ED compared to OOH or in hours GP. 33 Second a clinicians’ decisions to admit a child may be influenced by deprivation. A study by King et al 34 showed that referring clinicians often consider factors unrelated to the presenting complaint, such as domestic situations (including deprivation) and proximity to the hospital. This introduces a noteworthy consideration: a child from a deprived community might be more likely to be referred to the hospital per se, regardless of their clinical condition. The decision to discharge from hospital is a further stage where deprivation and wider domestic circumstances are considered. Any delay in discharge of a child from a more deprived community, to give more time for symptoms to resolve in hospital, will lead to reduced readmission and thus lead to reduced admissions for children from deprived communities. These factors may partly explain the differences in admissions between deprivation groups, but do not obviously explain why children from the most deprived communities in in England experienced a reduction in admissions between 2007 and 2017 relative to peers from less deprived communities.
There are several limitations to this study, and the available data. First, the analysis was mostly limited to the years 2007 and 2017 who were living in England, Scotland and Wales; however, our further analyses show that the results for urgent admissions were similar for those nations where data were available for 2000 to 2018 and for those aged 0 to 14 years. Second, and did not include data form Northern Ireland the data for prescribing outcomes were limited by both a relatively short duration, by applying different definitions (ie, number of prescriptions vs number of items prescribed) and by not having knowledge of the clinical context (ie, urgent or planned), but in the absence of any comparable data we provide them whilst acknowledging these limitations. Third, each of nations has applied slightly different methodologies to derive their index of deprivation thereby limiting comparability across the nations. 35 Fourth, we have assumed that the effect on admissions of factors other than those we have included in our analyses (ie, nation, age and deprivation) remained constant between 2007 and 2017.
A further limitation is that we report absolute rate of change in unscheduled health care use, and this does not place the change in context of baseline activity; for example, an annual rise of 0.5/1000 in urgent admissions is proportionately different from a baseline of 44.1/1000 (Scotland, least deprived quintile) compared to 111.6/1000 (Wales, most deprived quintile). Therefore, the absolute difference between deprivation groups and the relative change may be partly explained by different burden of disease in more deprived quintiles, different health seeking behaviour and clinical decision-making differing by deprivation, amongst other reasons. Finally, the higher urgent admissions for Wales compared to England and Scotland may reflect difference in pathways of care and deprivation but also may reflect differences in how data are recorded in the UK nations. Importantly, our study focused on changes within nations and therefore differences between nations in data recording will be constant and not affect our results.
In summary, we find that deprivation is related to urgent admissions and ED presentations of CYP across the UK and, perhaps unexpectedly, urgent admissions are rising less slowly for CYP from the most deprived quintile in some UK nations and more quickly for CYP from intermediate quintiles of deprivation. Future work could usefully link hospital and ED data to primary care activity to determine whether health seeking behaviour has changed post COVID and parents are presenting to ED instead of in hours and out of hours GP. Additional analyses could also consider whether the trends described here are seen across all conditions, including ‘primary care sensitive’ ones. Our findings might also be of relevance to services providing urgent heath care for older populations.
Supplemental Material
sj-docx-1-his-10.1177_11786329241245235 – Supplemental material for Rising Unscheduled Healthcare Utilisation of Children and Young People: How Does the Rise Vary Across Deprivation Quintiles in UK Nations?
Supplemental material, sj-docx-1-his-10.1177_11786329241245235 for Rising Unscheduled Healthcare Utilisation of Children and Young People: How Does the Rise Vary Across Deprivation Quintiles in UK Nations? by Josip Plascevic, Joseph Ward, Russell M. Viner, Dougal Hargreaves and Steve Turner in Health Services Insights
Footnotes
Acknowledgements
We are grateful for Jonathan Cushing who helped collect data as part of the Paediatrics 2040 programme. We are also grateful to colleagues in the four nations for their assistance in providing data including Deborah Brown (Pharmacy Statistics, HSC Business Services Registration, Northern Ireland), Ashley Akbari (Secure Anonymised Information Linkage Databank, Wales) and colleagues at Hospital Episode Statistics and Public Health Scotland.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
List of Abbreviations
CYP - Children and Young People
ED – Emergency Department
IMD – Index of Multiple Deprivations
NHS – National Health Service
SSUA – Short Stay Urgent Admission
UK – United Kingdom
Author Contributions
ST and RV conceived the idea. ST and JP undertook the analysis and wrote the first draft of the manuscript. All authors made meaningful contributions to the interpretation of the data and the final manuscript.
Ethics Approval and Consent to Participate
The need for informed consent was waived by the North of Scotland Research Ethics Committees, because of the retrospective nature of the study.
Consent for Publication
Not applicable (see above).
Availability of Data and Materials
Data are available on application to Hospital Episode Statistics (for English data), Secure Anonymised Information Linkage Databank (for Welsh data) and Public Health Scotland (for Scottish data). Data custodians are: for Scotland
All methods were carried out in accordance with relevant guidelines and regulations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.