
Abstract
Objectives
The impact of posttraumatic cognitions on the development and maintenance of posttraumatic stress symptoms (PTSS) is understudied among children and adolescents who have experienced commercial sexual exploitation/trafficking (CSE/T). The objectives of this study were to (1) explore posttraumatic cognitions among help-seeking young people aged 11-19 who have experienced CSE/T; (2) determine whether experiencing direct violence, witnessing violence, polyvictimization (ie, multiple exposures to different categories of potentially traumatic events), or demographic characteristics differentially affect whether these young people meet clinical criteria for posttraumatic cognitions using established cutoffs; and (3) explore associations between posttraumatic cognitions and PTSS among young people who have experienced CSE/T.
Methods
This study is a secondary analysis of a baseline cross-sectional survey of 110 young people with substantiated CSE/T experiences who started trauma-focused cognitive behavioral therapy (mean [SD] age = 15.8 [1.5]) from August 1, 2013, through March 31, 2020, in a southeastern US state. We used descriptive statistics, adjusted modified Poisson regression, and adjusted linear regression to test study objectives.
Results
Fifty-seven of 110 (51.8%) young people aged 11-19 met clinical criteria for posttraumatic cognitions. Increased age and a greater number of trauma categories experienced were significantly associated with meeting clinical criteria for posttraumatic cognitions. On average, higher posttraumatic cognition scores were associated with higher PTSS scores, controlling for demographic characteristics (β = 0.95; 95% CI, 0.64-1.26).
Conclusions
These findings underscore the importance of assessing comprehensive trauma history and PTSS of young people who have experienced CSE/T, with added usefulness of measuring cognitive appraisals to inform a therapeutic treatment plan. Measuring cognitive appraisals that may influence PTSS and therapeutic success can ensure an effective public health response for this population.
Sex trafficking of minors involves the giving or receiving of anything of value (eg, money, shelter, food) to any person in exchange for a sex act with a person aged <18 years. 1 Commercial sexual exploitation is a related term that includes sex trafficking and other crimes and activities involving sexual abuse or exploitation in exchange for something of value (eg, commercial production of child pornography or a minor [aged <18 y] engaging in sexual activity for money, shelter, protection, or drugs). 1-3 The commercial sexual exploitation and trafficking (CSE/T) of children, adolescents, and young adults is a global public health and human rights issue. 4 -7
Young people who have experienced or are experiencing CSE/T are at increased risk for mental health consequences. 8 -14 Trauma-related symptoms and disorders commonly experienced include posttraumatic stress symptoms (PTSS; eg, experiencing intrusive thoughts, avoidance of stimuli, or alterations in arousal or reactivity associated with the traumatic event that may or may not meet the diagnostic criteria for posttraumatic stress disorder [PTSD]), PTSD (ie, meeting all diagnostic criteria for PTSD), and complex PTSD (ie, a more severe form of PTSD that develops as a result of prolonged or severe trauma). 8 -16 Other common mental health consequences of experiencing CSE/T include depression, anxiety, suicidality, substance abuse, and behavior problems. 8 -14 CSE/T experiences may have a unique effect on the psychological functioning of young people beyond that of their peers who have not experienced CSE/T. 8 Coercion in the context of CSE/T may add to the complexity of the mental health problems these young people experience. 17
Negative cognitions, or appraisals, contribute to maladaptive psychological and behavioral functioning. 18 -22 Posttraumatic cognitions about oneself (eg, “My reactions since the frightening event mean that something is seriously wrong with me”) and the world (eg, “I am a coward”) 23 develop after a traumatic event and may persist if a person continues to process the event as a serious ongoing threat. 24 Emerging literature consistently documents the associations between posttraumatic cognitions and PTSS among children and adolescents who have experienced trauma. 25 -29 Lobo et al 26 found significant associations between posttraumatic cognitions and PTSS among children and adolescents aged 7-17 who were suspected victims of sexual abuse. Similarly, a study of children and adolescents aged 7-17 years with physical injuries found that posttraumatic cognitions contributed to the severity of PTSD symptoms. 27 Ponnamperuma and Nicolson 28 found that negative trauma appraisals predicted PTSS among trauma-exposed Sri Lankan adolescents aged 12-16 years. A longitudinal study among trauma-exposed Taiwanese children and adolescents aged 9-17 years found that maladaptive appraisals of trauma had a direct longitudinal effect on chronic PTSD severity. 29
Despite the importance of understanding cognitions among traumatized populations and their relation to PTSS, research exploring posttraumatic cognitions among young people experiencing CSE/T is limited. To our knowledge, only 1 study has assessed cognitions among young people who have experienced CSE/T 30 ; however, it was a qualitative study. Thus, research to expand our understanding of posttraumatic cognitions using a validated measure among young people aged 11-19 years who have experienced CSE/T is warranted. In addition to understanding this association, it is important to understand how the age, ethnicity, race, and living experiences of young people who have experienced CSE/T, and how previous trauma experiences, by type and cumulatively, may affect cognitions and related PTSS among young people who have experienced CSE/T. Previous research has documented that demographic characteristics (ie, child-welfare involvement, Black or ethnic minority status) 31-33 and trauma experiences (ie, direct violence, witnessing violence, polyvictimization [defined as multiple exposures to different categories of potentially traumatic events]) 34 -42 can contribute to the trauma symptomology of young people exposed to potentially traumatic events.
To address the dearth of literature on the impact of traumatic experiences on the trauma symptomology (ie, posttraumatic cognitions and PTSS) among young people aged 11-19 years who have experienced CSE/T, this study aimed to (1) explore posttraumatic cognitions among help-seeking young people who have experienced CSE/T, (2) examine whether cumulative trauma experiences (ie, experiencing direct violence, witnessing violence, or polyvictimization) or demographic characteristics (ie, ethnicity, race, living situation, age) differentially affect whether young people who have experienced CSE/T meet clinical criteria for posttraumatic cognitions, and (3) explore associations between posttraumatic cognitions and PTSS among young people who have experienced CSE/T.
Methods
Participants and Data Collection
This study is a secondary analysis of cross-sectional program evaluation data collected through Project Intersect. Project Intersect is a federally funded project that has built a large network of trauma-focused cognitive behavioral therapy (TF-CBT) therapists (N = 133) trained in CSE/T applications. 43 Young people who experienced CSE/T were referred to TF-CBT therapists (licensed or supervised seeking licensure) as part of Project Intersect 43 from August 1, 2013, through March 30, 2020. Therapist training and the process by which young people were referred to Project Intersect are described elsewhere. 43,44 When referred to a therapist, 44 young people aged 11-19 years who experienced CSE/T could participate in program evaluation at 3 time points (intake, midpoint, completion). English-speaking young people aged 11-19 years with substantiated CSE/T experiences could participate in program evaluation. We did not assess continuing CSE/T experiences in the program evaluation. Although labor trafficking substantially affects the mental health of those who have experienced CSE/T, only substantiated CSE/T experiences were a requirement of participating in the program evaluation. Participants received a $20 gift card for completing the evaluation at each time point. We conducted the program evaluation for program and funding purposes and in the context of the clinical services provided by therapists participating in Project Intersect; thus, informed consent was not required. We obtained institutional review board approval from Georgia State University to conduct this study.
Measures
Demographic characteristics.
We collected data on demographic characteristics, including age (11-19 y), gender (female, male, transgender), ethnicity (Hispanic/Latinx, non-Hispanic/Latinx), race, and residential status (living with a caregiver/parent; alone, with friends, or at a homeless shelter; in a group home or other nonjuvenile detention setting; in a foster home or temporary placement; or in another setting [including Department of Juvenile Justice]). We included data on ethnicity in the models as a binary variable based on 1 item asking, “Are you Hispanic or Latino?” (yes/no). We did not include data on ethnic group in analyses because of the small number of participants belonging to each ethnic group. Possible responses for race included Black or African American, Asian, Native Hawaiian/Other Pacific Islander, White, American Indian, or “other” (open-ended response), according to the program evaluation reporting standards set by the grant funder. We then created a variable for race for inclusion in the models with the categories Black or African American, White, or “other” (ie, Asian, Native Hawaiian/Other Pacific Islander, American Indian, “other,” or >1 race [ie, multiracial]). We assessed the residential status of participants in the past 30 days with 12 possible responses, which were combined into 5 categories based on the distribution of the data. To develop parsimonious regression models that considered sample size, we created a dummy variable to indicate whether the young people lived with a parent/caregiver or had another living situation for use in the regression models.
Trauma Categories and Polyvictimization
Next, we identified 7 trauma categories (ie, natural disaster, accident, war, direct violence, witnessing violence, medical trauma, and loss/separation) based on previous literature 21,44 using 14 items from the trauma history screen of the University of California, Los Angeles PTSD–Reaction Index (UCLA PTSD-RI), one of the most widely used validated instruments for assessing trauma symptoms among children and young people (Table 1). 46 We excluded from analyses 1 item in the UCLA trauma history screen that assessed CSE/T experiences, because Project Intersect participants had substantiated CSE/T experiences. During the process of coding the open-ended item, the theme of loss/separation emerged; thus, we grouped responses to this item in the loss/separation trauma category. When participants experienced at least 1 item in a trauma category, we considered them to have experienced that category. We created a summary variable (polyvictimization) to indicate the total number of trauma categories experienced (possible range, 0-7). Respondents were considered to have experienced polyvictimization if they had a polyvictimization score ≥1 (ie, had experienced trauma in >1 category).
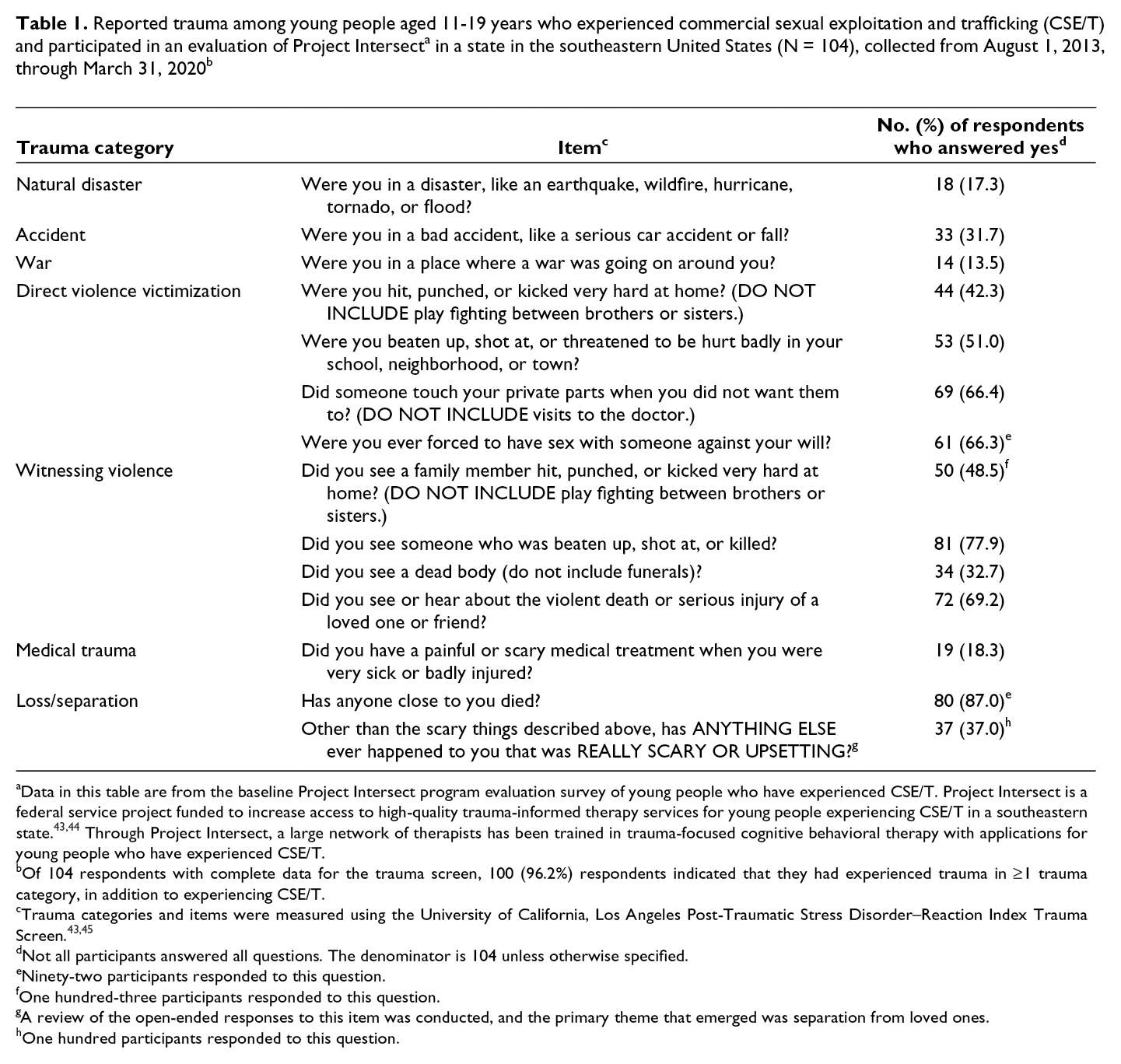
aData in this table are from the baseline Project Intersect program evaluation survey of young people who have experienced CSE/T. Project Intersect is a federal service project funded to increase access to high-quality trauma-informed therapy services for young people experiencing CSE/T in a southeastern state. 43,44 Through Project Intersect, a large network of therapists has been trained in trauma-focused cognitive behavioral therapy with applications for young people who have experienced CSE/T.
bOf 104 respondents with complete data for the trauma screen, 100 (96.2%) respondents indicated that they had experienced trauma in ≥1 trauma category, in addition to experiencing CSE/T.
cTrauma categories and items were measured using the University of California, Los Angeles Post-Traumatic Stress Disorder–Reaction Index Trauma Screen. 43,45
dNot all participants answered all questions. The denominator is 104 unless otherwise specified.
eNinety-two participants responded to this question.
fOne hundred-three participants responded to this question.
gA review of the open-ended responses to this item was conducted, and the primary theme that emerged was separation from loved ones.
hOne hundred participants responded to this question.
Posttraumatic Cognitions
We assessed posttraumatic cognitions using the Child Post-Traumatic Cognitions Inventory (CPTCI). 45,47 The CPTCI is a validated, 33-item self-report questionnaire that measures maladaptive cognitions among trauma-exposed young people aged 6-18 years. 45,47 Participants were asked, “Tell us how much you agree or disagree with the following statements.” Statements that followed included, “Anyone could hurt me” and “I am no good.” Responses to each item ranged from don’t agree at all (1) to agree a lot (4). The criterion score for clinically significant posttraumatic cognitions ranged 45 from 46 to 48 (possible range for total score, 33-132). If a young person’s CPTCI total score was ≥46, that person was considered to be experiencing clinically significant posttraumatic cognitions at the time of data collection.
Posttraumatic Stress Symptoms
We used the UCLA PTSD-RI to assess PTSS using a 27-item validated subscale. 46,48 For the first 11 participants, we used the UCLA PTSD-RI based on the Diagnostic and Statistical Manual of Mental Disorders-IV diagnostic criteria for PTSD 49 ; the remaining 99 participants (starting in October 2014) completed the UCLA PTSD-RI based on the Diagnostic and Statistical Manual of Mental Disorders-V. 50 During data collection for Project Intersect, the PTSD diagnostic criteria and UCLA PTSD-RI were updated; therefore, we began using the UCLA PTSD-RI for the Diagnostic and Statistical Manual of Mental Disorders-V when it became available. Participants were asked to rate how many days during the last month they had experienced PTSS, such as “I have trouble concentrating or paying attention” or “I have strong feelings in my body.” For each item, participants could choose 1 of 5 response options: none (0), little (1), some (2), much (3), or most (4). We calculated PTSS according to the scoring described in the UCLA PTSD-RI manual (possible range, 0-124). 46
Data Analysis
To address our first objective of exploring posttraumatic cognitions among help-seeking young people who experienced CSE/T, we calculated frequencies and percentages of young people who were considered to have clinically significant posttraumatic cognitions based on a CPTCI score of ≥46. 45 For our second objective of examining the associations between cumulative trauma experiences and demographic characteristics on the posttraumatic cognitions of young people who experienced CSE/T, we developed 3 adjusted modified Poisson regression models. All models included clinically significant posttraumatic cognitions as the dependent variable; ethnicity, race, age, and living situation as covariates; and trauma as the primary independent variable of interest, with separate models for direct violence victimization, witnessing violence, and polyvictimization. To asses our third objective of exploring associations between posttraumatic cognitions and PTSS among this population, we used an adjusted linear regression model using the same covariates that were used in the previous models.
We used multiple imputation to address missing data. We assumed data to be missing at random. Missingness on CPTCI was related to observed variables in the dataset (ie, ethnicity, race, and living situation), which we controlled for in the models. We determined the number of imputations using the largest fraction of missing information (0.27 for CPTCI score) and a coefficient of variation of 5%, as described by von Hippel. 51 Based on this calculation, the number of imputations was 20. Data were missing for 29 CPTCI variables and 28 PTSS variables. Data on race were missing for 12 respondents. The final analytic models included 109 participants in the linear regression model and 108 participants in the modified Poisson regression models because of 1 participant who was missing data on all variables included in the models and because of 1 invalid value in the Poisson regression models. We conducted all analyses in SAS version 9.4 (SAS Institute, Inc), with α = .05 considered significant.
Results
Most of the sample identified as female (103 of 109; 94.4%) and Black or African American (59 of 98; 60.2% (Table 2). Most respondents reported experiencing direct violence (83 of 100; 83.0%) or witnessing violence (92 of 104; 88.5%). The mean polyvictimization score was 3.3 (SD = 1.5); 100 of 104 (96.2%) young people with complete data for the trauma screen reported experiencing polyvictimization in addition to CSE/T (Table 1; see footnote “b”). Fifty-seven of 81 (70.4%) respondents with complete data had clinically significant posttraumatic cognitions. Fifty-three of 57 (93.0%) respondents who had experienced direct violence and 54 of 57 (94.7%) respondents who had witnessed violence had clinically significant posttraumatic cognitions.
Demographic characteristics of young people aged 11-19 years (N = 110) who experienced commercial sexual exploitation and trafficking (CSE/T) and participated in an evaluation of Project Intersect a in a state in the southeastern United States, collected from August 1, 2013, through March 31, 2020
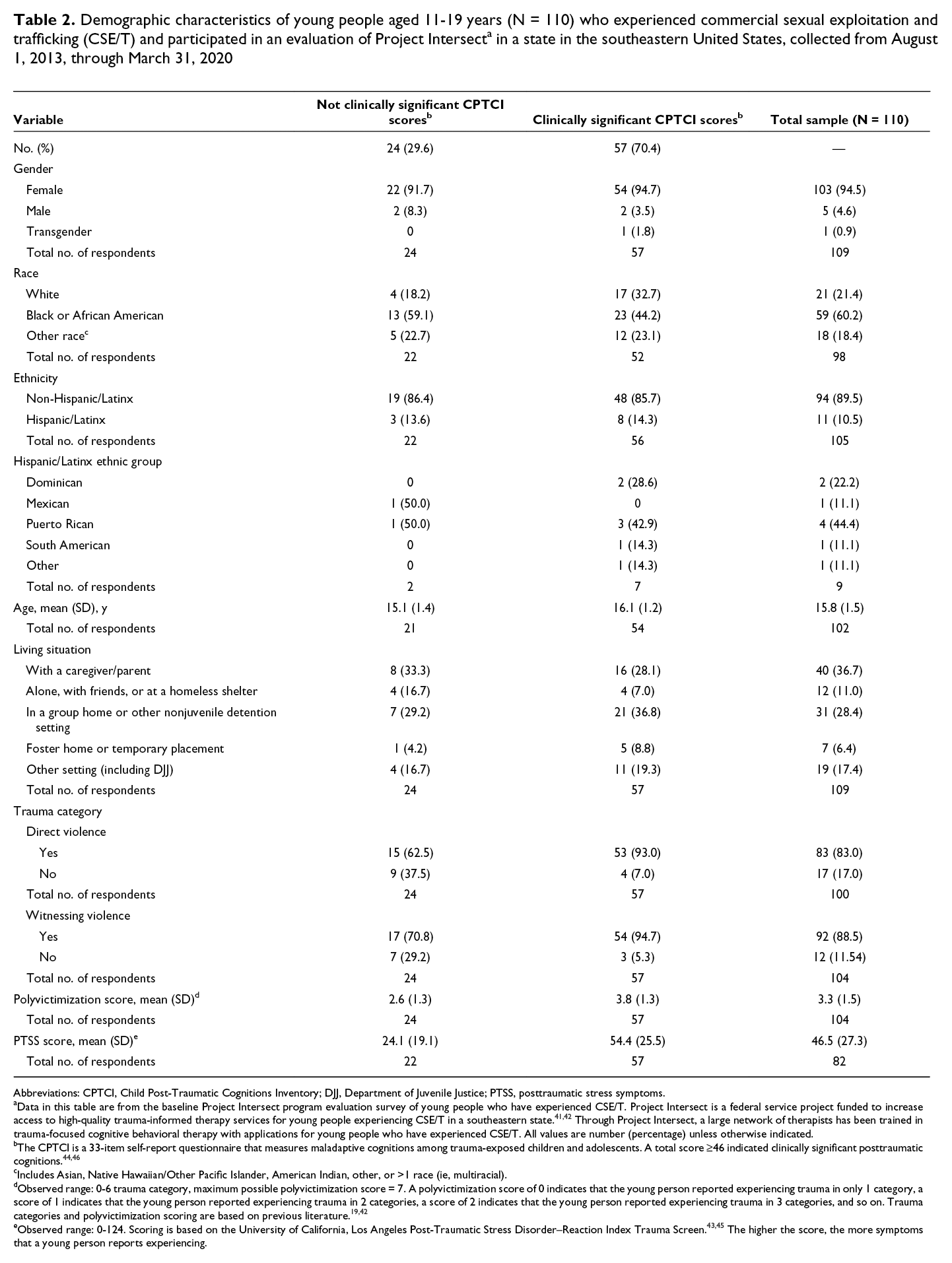
Abbreviations: CPTCI, Child Post-Traumatic Cognitions Inventory; DJJ, Department of Juvenile Justice; PTSS, posttraumatic stress symptoms.
aData in this table are from the baseline Project Intersect program evaluation survey of young people who have experienced CSE/T. Project Intersect is a federal service project funded to increase access to high-quality trauma-informed therapy services for young people experiencing CSE/T in a southeastern state. 41,42 Through Project Intersect, a large network of therapists has been trained in trauma-focused cognitive behavioral therapy with applications for young people who have experienced CSE/T. All values are number (percentage) unless otherwise indicated.
bThe CPTCI is a 33-item self-report questionnaire that measures maladaptive cognitions among trauma-exposed children and adolescents. A total score ≥46 indicated clinically significant posttraumatic cognitions. 44,46
cIncludes Asian, Native Hawaiian/Other Pacific Islander, American Indian, other, or >1 race (ie, multiracial).
dObserved range: 0-6 trauma category, maximum possible polyvictimization score = 7. A polyvictimization score of 0 indicates that the young person reported experiencing trauma in only 1 category, a score of 1 indicates that the young person reported experiencing trauma in 2 categories, a score of 2 indicates that the young person reported experiencing trauma in 3 categories, and so on. Trauma categories and polyvictimization scoring are based on previous literature. 19,42
Trauma and Clinically Significant Posttraumatic Cognitions
Results of the 3 adjusted modified Poisson regression models indicated a significant association between polyvictimization and clinically significant posttraumatic cognitions (adjusted prevalence ratio [aPR] = 1.21; 95% CI, 1.02-1.44; P = .03; Table 3). Each additional trauma category experienced was associated with a 1.21 times higher likelihood of having clinically significant posttraumatic cognitions. The model for direct violence victimization (aPR = 2.27; 95% CI, 0.91-5.66; P = .08) and witnessing violence (aPR = 2.50; 95% CI, 0.86-7.31; P = .09) found no significant association between these trauma categories and clinically significant posttraumatic cognitions.
Adjusted modified Poisson regression models examining trauma categories of interest and child posttraumatic cognitions among young people aged 11-19 years participating in an evaluation of Project Intersect a in a state in the southeastern United States, collected from August 1, 2013, through March 31, 2020 b
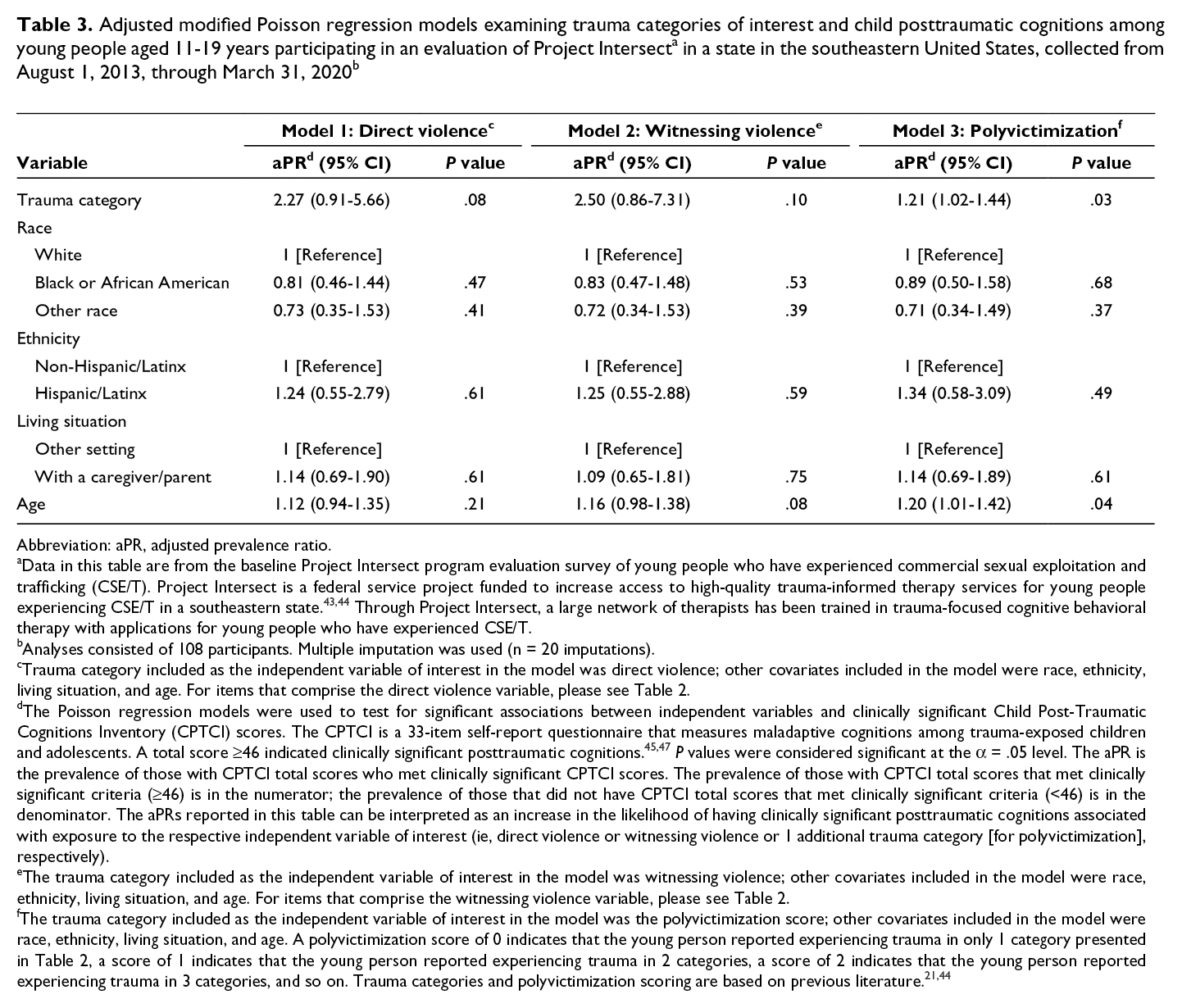
Abbreviation: aPR, adjusted prevalence ratio.
aData in this table are from the baseline Project Intersect program evaluation survey of young people who have experienced commercial sexual exploitation and trafficking (CSE/T). Project Intersect is a federal service project funded to increase access to high-quality trauma-informed therapy services for young people experiencing CSE/T in a southeastern state. 43,44 Through Project Intersect, a large network of therapists has been trained in trauma-focused cognitive behavioral therapy with applications for young people who have experienced CSE/T.
bAnalyses consisted of 108 participants. Multiple imputation was used (n = 20 imputations).
cTrauma category included as the independent variable of interest in the model was direct violence; other covariates included in the model were race, ethnicity, living situation, and age. For items that comprise the direct violence variable, please see Table 2.
dThe Poisson regression models were used to test for significant associations between independent variables and clinically significant Child Post-Traumatic Cognitions Inventory (CPTCI) scores. The CPTCI is a 33-item self-report questionnaire that measures maladaptive cognitions among trauma-exposed children and adolescents. A total score ≥46 indicated clinically significant posttraumatic cognitions. 45,47 P values were considered significant at the α = .05 level. The aPR is the prevalence of those with CPTCI total scores who met clinically significant CPTCI scores. The prevalence of those with CPTCI total scores that met clinically significant criteria (≥46) is in the numerator; the prevalence of those that did not have CPTCI total scores that met clinically significant criteria (<46) is in the denominator. The aPRs reported in this table can be interpreted as an increase in the likelihood of having clinically significant posttraumatic cognitions associated with exposure to the respective independent variable of interest (ie, direct violence or witnessing violence or 1 additional trauma category [for polyvictimization], respectively).
eThe trauma category included as the independent variable of interest in the model was witnessing violence; other covariates included in the model were race, ethnicity, living situation, and age. For items that comprise the witnessing violence variable, please see Table 2.
fThe trauma category included as the independent variable of interest in the model was the polyvictimization score; other covariates included in the model were race, ethnicity, living situation, and age. A polyvictimization score of 0 indicates that the young person reported experiencing trauma in only 1 category presented in Table 2, a score of 1 indicates that the young person reported experiencing trauma in 2 categories, a score of 2 indicates that the young person reported experiencing trauma in 3 categories, and so on. Trauma categories and polyvictimization scoring are based on previous literature. 21,44
Posttraumatic Cognitions and PTSS
The multivariable linear regression indicated a significant association between posttraumatic cognitions and PTSS, controlling for age, ethnicity, race, and living situation (Table 4). A 1-point positive difference in CPTCI score corresponded to a 0.95-point positive difference in PTSS score (95% CI, 0.64-1.26; P < .001).
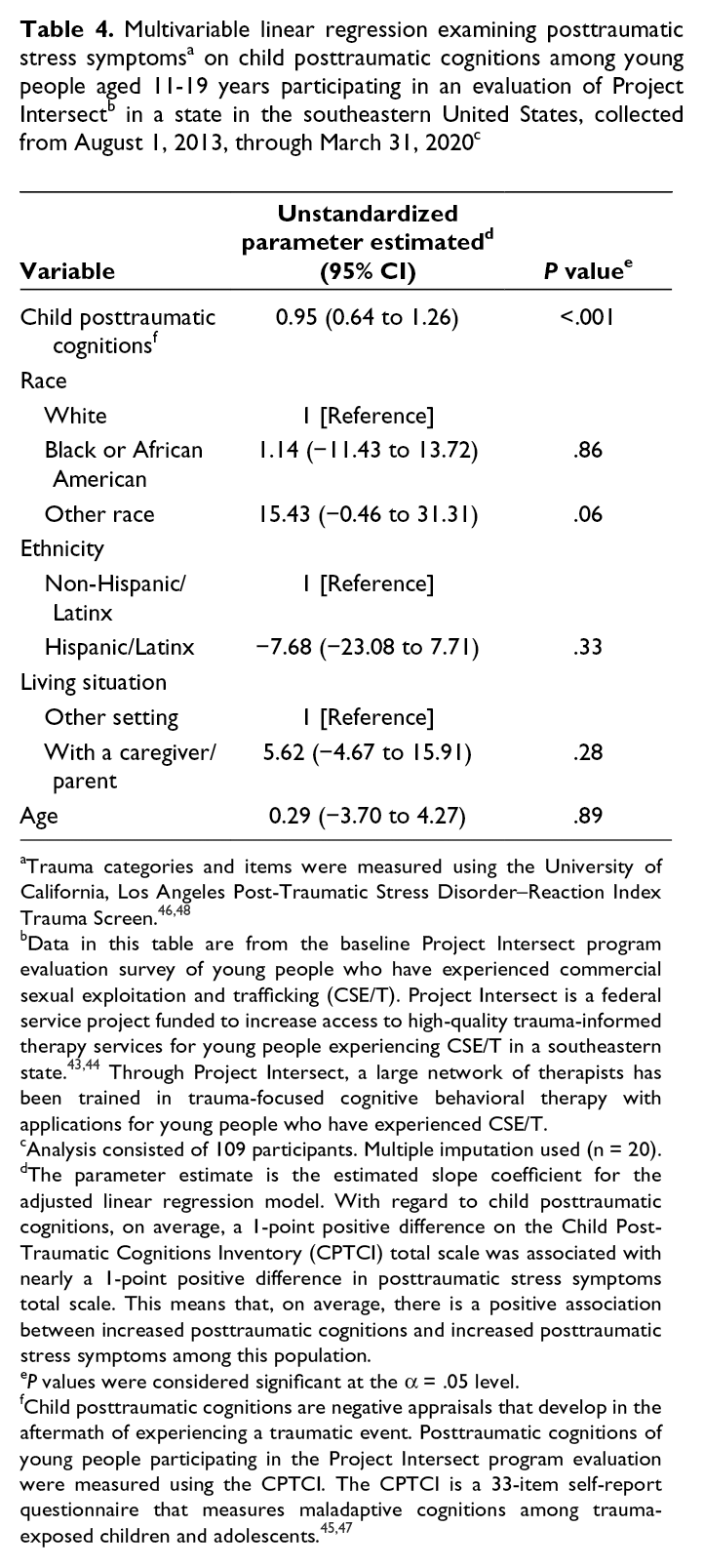
aTrauma categories and items were measured using the University of California, Los Angeles Post-Traumatic Stress Disorder–Reaction Index Trauma Screen. 46,48
bData in this table are from the baseline Project Intersect program evaluation survey of young people who have experienced commercial sexual exploitation and trafficking (CSE/T). Project Intersect is a federal service project funded to increase access to high-quality trauma-informed therapy services for young people experiencing CSE/T in a southeastern state. 43,44 Through Project Intersect, a large network of therapists has been trained in trauma-focused cognitive behavioral therapy with applications for young people who have experienced CSE/T.
cAnalysis consisted of 109 participants. Multiple imputation used (n = 20).
dThe parameter estimate is the estimated slope coefficient for the adjusted linear regression model. With regard to child posttraumatic cognitions, on average, a 1-point positive difference on the Child Post-Traumatic Cognitions Inventory (CPTCI) total scale was associated with nearly a 1-point positive difference in posttraumatic stress symptoms total scale. This means that, on average, there is a positive association between increased posttraumatic cognitions and increased posttraumatic stress symptoms among this population.
e P values were considered significant at the α = .05 level.
fChild posttraumatic cognitions are negative appraisals that develop in the aftermath of experiencing a traumatic event. Posttraumatic cognitions of young people participating in the Project Intersect program evaluation were measured using the CPTCI. The CPTCI is a 33-item self-report questionnaire that measures maladaptive cognitions among trauma-exposed children and adolescents. 45,47
Discussion
Posttraumatic cognitions feature prominently in the development of PTSS among traumatized people. 22,52 Our study builds on previous research suggesting a strong association between posttraumatic cognitions and PTSS among trauma-exposed children and adolescents. 26 -30 To our knowledge, our study is the first to examine posttraumatic cognitions using a validated measure among a population experiencing CSE/T. Understanding posttraumatic cognitions among this population is especially important, because previous research has documented that maladaptive cognitions can affect treatment progression 52 and contribute to revictimization risk broadly. 22
More than half of participants in our study met the clinical criteria for posttraumatic cognitions, suggesting that the young people in our study who experienced CSE/T commonly experienced posttraumatic cognitions or negative trauma appraisals. A deeper exploration of factors associated with clinically significant posttraumatic cognitions indicated that polyvictimization placed respondents at greater risk of meeting clinical criteria for posttraumatic cognitions compared with respondents who did not experience polyvictimization. However, no other trauma category was associated with increased posttraumatic cognitions among respondents. This finding is surprising in light of previous research that found associations between experiencing direct violence and witnessing violence and increased posttraumatic cognitions. 34,36,37,53 All participants in our study were substantiated as having experienced CSE/T, and the trauma included experiences that happened either in conjunction with, or in addition to, CSE/T experiences. Thus, there may be something unique about the CSE/T-related trauma experiences and related cognitions among young people who have experienced CSE/T that may distinguish them from other young people who have experienced non–CSE/T-related trauma. Future comparative studies may help elucidate these potential differences.
Age was the only demographic characteristic that was significantly associated with posttraumatic cognitions in the model with polyvictimization, with increased age being associated with an increased risk of clinically significant levels of posttraumatic cognitions. Although exposure to violence has been found to increase with age, 54 research on age-related differences in PTSS 33,55,56 and posttraumatic cognitions 23,26,53 is inconsistent. An association did not emerge between living situation and posttraumatic cognitions nor with PTSS. The lack of sufficient evidence to detect an association between living situation and posttraumatic cognitions and PTSS is surprising, because children and adolescents with higher levels of trauma are more likely than children and adolescents with lower levels of trauma to have disruptions in foster care placement. 31,32,57 Furthermore, neither ethnicity nor race was associated with posttraumatic cognitions or PTSS. Commensurate with other research, 58 -62 more than half of the young people in our sample identified as Black or African American. Given the overrepresentation of children and adolescents of color among young people who have experienced CSE/T, 63 future research should explore how experiences of marginalization, race-based objectification, and racial/discrimination trauma contribute to the development of posttraumatic cognitions. 64
Lastly, as with previous research, 25 young people in our sample with higher levels of posttraumatic cognitions reported higher levels of PTSS. This finding was expected because “negative mood and altered cognitions” is 1 domain of the PTSD diagnosis. 50 Collectively, these findings suggest the importance of a comprehensive trauma screening (ie, identification of the full range of traumas experienced) and quality assessment at multiple timepoints during treatment (ie, trauma symptoms, posttraumatic cognitions), given the associations of these factors with more severe trauma-related symptomology, 22,25,65 interpersonal trauma revictimization, 22 and the effect of mental health treatment. 66,67 The therapeutic treatment plan should also focus on incorporating evidence-based cognitive processing treatments and strategies. 68 Addressing these cognitions in the treatment plan may provide added therapeutic value for young people who have experienced CSE/T.
Notably, the participants in our study have the opportunity to participate in TF-CBT 69 as part of Project Intersect. 43 TF-CBT is a components-based model of psychotherapy with a strong evidence base for treating a broad array of trauma-related mental health outcomes, including trauma-related cognitions 52,67 that young people with trauma exposures may experience. 70 Although our study was limited to data collected at the start of treatment, it will be important to examine whether young people who have experienced CSE/T and who complete TF-CBT report reductions in their posttraumatic cognitions and related PTSS after completing treatment, and whether differential treatment outcomes emerge among young people who report clinically significant posttraumatic cognitions at the start of treatment. Currently, there is no collective, deep understanding of how posttraumatic cognitions are differentially affected by trauma categories that young people experience and how posttraumatic cognitions contribute to the risk of revictimization. There may be unique cognitions among young people who have experienced CSE/T, especially among those who may not consider the CSE/T experience a trauma, perhaps as a result of the manipulation tactics of exploiters. 17,71 Future research should explore how posttraumatic cognitions contribute to the vulnerability of young people to such tactics and young people’s perceptions of power and control during trafficking experiences.
Limitations
This study had several limitations. First, these data were collected as part of a program evaluation of young people with substantiated CSE/T experiences referred for therapy. Thus, the data are indicative only of help-seeking, English-speaking young people who have experienced CSE/T and may not be representative of the larger population of young people who have experienced CSE/T in the United States. Self-selection into the evaluation introduces selection bias, thereby further limiting generalizability. Other factors that limit the generalizability of these findings are the lack of variability in some of the covariates and the small sample size. It is unclear how young people with substantiated CSE/T experiences who engage in mental health treatment may differ in their posttraumatic cognitions compared with young people who have experienced CSE/T who are not identified or who are identified but do not engage in therapeutic services.
Second, 103 of 109 participants in our study identified as female. Little observed variability in gender is likely the result of difficulties in identifying male and non-cisgender young people who have experienced CSE/T. Third, assessment data collected were self-reported and limited to the clinical measures implemented as part of the program evaluation. Thus, we were unable to ascertain exposure to adverse childhood experiences beyond violence or community- and societal-level factors that may influence posttraumatic cognitions and PTSS. We were also limited in our assessment of participant race and ethnicity, because these domains were defined by the grant funder.
Fourth, the trauma assessment measures do not distinguish between events that occurred before or during the period of exploitation, nor whether multiple events within a trauma category affected outcomes. Thus, some of the victimization experiences that were reported may have been experienced as part of the CSE/T experience. Furthermore, we did not differentiate between trafficking and exploitation, and we did not assess ongoing CSE/T. Another measurement issue was that the posttraumatic cognitions measure had the most missing data compared with other program evaluation measures, perhaps as a result of being located at the end of the survey. Although data were appropriately imputed, when we examined data on respondents who completed this measure, >70% of the sample met the clinically significant criterion. Thus, the results are likely highly conservative. Lastly, the items in the CPTCI measure were limited to asking about one frightening event, which may not capture the extent of the cognitions that may be related to cumulative experiences of trauma.
Conclusions
This study supports the importance of and critical need for quality assessment and evidence-based mental health treatment that incorporates a focus on cognitions for young people who have experienced CSE/T, given the high rates of trauma experiences and the clinically significant levels of posttraumatic cognitions and PTSS. Randomized controlled trials are necessary to document how evidence-based programs, such as TF-CBT, affect the short- and long-term mental health of this population. Studies examining whether posttraumatic cognitions are a mechanism or mediator of treatment progress among this population, and the best approaches for cognitive processing as an element of trauma-informed, evidence-based interventions, are needed. As our understanding grows about best practices for the mental health treatment of PTSS and posttraumatic cognitions among young people who have experienced CST/E, these findings and strategies must be disseminated and implemented broadly to ensure that young people receive the greatest benefit from clinical interventions in community settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Program evaluation findings reported in this article were from Project Intersect, a service grant funded by the Substance Abuse and Mental Health Services Administration (SAMHSA) as part of the National Child Traumatic Stress Network (SM061107-03; to principal investigator K.K.). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of SAMHSA.