
Abstract
Introduction:
Over the last decade, hypertension (HPT) is among the leading causes of death and morbidity in Ghana. In recent past, most health policy research in Ghana and Africa focussed on communicable diseases. In recent times, Ghana and other developing nations have shifted their attention to non-communicable diseases because most of these countries are going through an epidemiologic transition where there is a surge in the prevalence of HPT. This paper was therefore set out to estimate the cost of treating HPT in Ghana from the patients’ and health system’s perspectives.
Method:
We used a cost of illness framework to simulate the cost of HPT management in Ghana taking into account 4 of the common target organ complications with the most mortality implication. A decision analytic model (DAM) was developed in Microsoft® Excel to simulate the progression of HPT patients and the Markov model was employed in simulating the lifetime cost of illness.
Results:
The results show that by 10 years from diagnosis, the probability of death from any of the 4 complications (ie, stroke, myocardial infarction, heart failure, and chronic kidney disease) is roughly 41.03%. By 20 years (or 243 months) from diagnosis, the probability of death is estimated to be 69.61%. However, by the 30th anniversary, the probability of death among the cohort is 82.3%. Also, the lifetime discounted cost of treating HPT is about GHS 869 106 which could range between GHS 570 239 and GHS 1.202 million if wide uncertainty is taken into account. This is equivalent to USD 119 056 (range: USD 78 115-164 723).
Conclusion:
By highlighting the lifetime cost of treating HPT in Ghana, policies can be formulated regarding the cost of treating HPT by the non-communicable disease unit and National Health Insurance Authority (NHIA) of the Ministry of Health.
Introduction
Hypertension is a non-communicable disease recognized as an essential public health concern, affecting both developed and developing countries globally.1-4 Despite the policy agenda implemented by both economically developed and developing nations to kerb the menace, 5 hypertension remains a significant predisposition for the development of cardiovascular diseases (CVD). 2 It has also been reported that hypertension accounts for 50% of total cardiovascular heart disease (CHD) morbidity and mortality worldwide. 6
Significantly 40% of the adult population in the African continent is estimated to have hypertension making it the commonest non-communicable disease. 7 Extant literature has also shown that the prevalence of hypertension has increased substantially over the years ranging between 19% and 40% in Sub-Saharan Africa.8-10 More so, studies in other locales, including Nigeria and Kenya have suffered a major setback in the management of hypertension due to the rising cost of treatment.11,12 Furthermore, a cardiovascular risk factor such as hypertension if not well controlled is a recipe for cardiovascular complications. 13
Within the Ghanaian society, hypertension has steadily seen an increase in prevalence making it an important public health issue even in poor rural communities. 10 Recently published systematic reviews in Ghana reported a prevalence between 24.0% and 30.1% in adult populations.1,14 In 2017 hypertension was reported as the third leading cause of hospital admissions and the leading cause of morbidity and death in Ghana. 14 Besides the debilitating complications associated with hypertension, it poses a huge health expenditure on sufferers of the disease and the health care system. 15 Also, some studies conducted in the Democratic Republic of Congo (DRC) and Ethiopia revealed that 15.4% and 46.6% of patients had their blood pressure poorly controlled and the plausible explanation could be attributed to the cost of treatment for hypertension. 16 This phenomenon of poor hypertension control owing to the cost of treatment with its catastrophic consequences puts enormous pressure on the individual and the already burdened health care system. 17 Despite considerable gains made by the National Health Insurance Scheme (NHIS) since its inception, the transitioning of Ghana away from development-assisted funds, co-payment has now become the order of the day in our health facilities and this has worsened the plight of hypertension patients.15,18
Most studies on hypertension in Ghana have examined the prevalence, risk factors, awareness, adherence, challenges, and management.2,5,10,14,16,18-20 It is against this backdrop that this study seeks to model the lifetime cost of managing hypertension in Ghana considering the paucity of data in the area. This will provide empirical evidence on the lifetime cost of managing hypertension in Ghana for policy formulation. This paper provides a modelled estimate of the lifetime, annual, and monthly cost of managing hypertension in Ghana.
Methodology
Overview of Ghana’s health system
Ghana is politically and administratively organized into sixteen (16) regions and 260 districts. Each district is further divided into health sub-districts and communities, and the delivery of health services is operationally and administratively coordinated with these organizations. The Ghana Health Service (GHS) and Teaching Hospitals (THs) are semi-autonomous entities tasked with providing public health services under an act of parliament (Act 525 of 1996). In addition, there are various faith-based, private-for-profit, and quasi-governmental institutions, as well as mental health facilities. The Ministry of Health (MOH) oversees all of these institutions, with a focus on policy creation, resource mobilization and allocation, and monitoring and evaluation. Community-Based Health Planning and Services (CHPS) are at the bottom of the primary health care hierarchy, functioning as the health system’s initial point of contact for a set population of 5000 people or 750 families, which is sometimes coterminous with electoral zones. These are tasked with providing preventative health services and treating minor ailments in the community using over-the-counter medications. Health Centres (HCs) serve persons in a sub-district’s catchment area and are responsible for providing basic curative and preventive health services. They are the first point of contact between the communities and CHPS. 19
Although health centres are required to serve catchment populations of 20 000 or fewer, in metropolitan areas they can be extended (in size and staffing) and designated as polyclinics to service bigger populations.19,20 According to one assessment, several metropolitan polyclinics were working at the level of hospitals, despite their designation, due to increased population demand for services. The district/primary hospitals are at the apex of the primary health care hierarchy, serving as district-level referral centres for preventative, curative, and emergency health care to populations ranging from 100 000 to 200 000. However, it is estimated that at least half of the districts were without these primary/district hospitals, resulting in additional strain in other facilities that run beyond their capacity.19,20
Overview of model type, structure, and assumptions
Using a cost of illness framework,21,22 we simulated the cost of hypertension management in Ghana taking into account 4 of the common target organ complications with the most mortality implications. A decision analytic model (DAM) was developed in Microsoft® Excel to simulate the progression of hypertension patients in Ghana for a hypothetical cohort of 30-year-old patients. Since hypertension and its associated complications are long-term in nature, we employed a Markov model in simulating the lifetime cost of illness. 23 Hypertension is well documented as a significant risk factor for several life-threatening conditions, including stroke, coronary heart disease, heart failure, kidney failure, and myocardial infarction. Other complications of concern from hypertension are eye problems (retinopathy) and erectile dysfunction among others.2,24
Based on standard treatment guidelines for hypertension management in Ghana and expert opinion of internal and family medicine physicians, 25 we focussed the modelling efforts on target organ complications that are associated with intensive resource use: stroke, heart failure, kidney failure, myocardial infarction.26,27
Markov transition states were identified and represented in the schematic diagram (Figure 1) in which it is assumed that persons with hypertension would have a risk of progression into 1 or more of the 4 possible states—stroke, heart failure, chronic kidney failure, or myocardial infarction, each of which could lead to death. Based on the literature, we also assumed interactions between these states, in that myocardial infarction could lead to stroke and heart failure, which could also result in chronic kidney failure.26-29 The cohort of patients is assumed to enter the model following a diagnosis of hypertension without any target organ complication, where they face the respective probabilities of transitioning from one of the above-mentioned states to another.

Model structure (Markov Model for hypertension).
The typical Markovian assumption was made where it was assumed that the transition probability from one state to another remains fairly constant throughout the patients’ lifetime. Although this ‘memoryless assumption’ of a typical Markov model may seem strong, the absence of age-specific morbidity and mortality rates for hypertension in Ghana and other neighbouring countries 15 limited us from implementing time-or age-dependent transition probabilities, which are recommended as solutions to the memoryless assumption.23,30,31 The model tracks a cohort of 30-year-old patients until death, or they are up to Ghana’s average life expectancy of 63 years. Box 1 provides simple mathematical expressions of the state transitions assumed in the model.
Mathematical expressions of the Markov model.

Cycle length, discounting, and half-cycle correction
In Ghana’s standard treatment guidelines, 25 patients with hypertension or the associated target organ complications are usually scheduled for monthly reviews and/or refills of medications. Also, as patients with the target complications are associated with high mortality rates, a 1-month cycle length is assumed in this model. The Ghana Government does not have an official discount rate for analysis but the Bank of Ghana periodically publishes a reference rate for planning. Accordingly, we discounted the long-term cost by 10% per annum in line with the average annual reference rate at the time of modelling as published by Ghana. 32 Given the ongoing discourse about the added value of half-cycle correction, 33 we made no adjustments for half-cycle correction in the simulation.
Cost data
We employed a bottom-up protocol-based itemized costing approach 22 to estimate the cost of each episode of treatment of hypertension and the related target organ complications. The use of healthcare resources in the treatment of hypertension and the associated target organ complications was guided by the Ghana Standard Treatment Guidelines 25 and the corresponding unit costs were taken from National Health Insurance Scheme (NHIS) price list in Ghana. 34 We considered the direct medical cost such as diagnostics/investigations, consultations, inpatient admissions, and medication, which were all taken from the NHIS price list. From the patient perspective, we also included the cost of transport. All costs are presented in both Ghana Cedis and 2022 equivalent to United States Dollars (USD) using an exchange of 1 USD to 7.31 Ghana Cedis.
The Ghana Standard Treatment Guidelines (2017) provides different lines of treatment options for the diseases considered in the study. For example whereas some hypertensives with no complication maybe put on Thiazide Diurretics, others may be on Calcium Channel Blockers, Angiotension Converting Enzyme (ACE) inhibitors or Angiotension receptor Blockers (ARBs). These classes of medications vary in their cost and are not necessarily prescribed for all persons suffering from hypertension. To adjust the cost to account for these variations, we adopted a weighting approach used by the Ghanaian Ministry of Health in a similar modelling study in Ghana 15 —see Supplemental Material 1. This approach uses the proportion of hypertensives prescribed these medications to adjust the cost. The proportion of patients prescribed the different medications was adopted from the MOH based on the National Health Insurance claims data. Table 1 provides the summary cost data used as model input while the detailed unit cost of items and services are contained in Supplemental Material 1.
Summary of cost data used as model input.

Data source: NHIS price list and service tariffs, 2019.
Also, the lost productivity cost was assumed to be the minimum wage of Ghana for each day of clinic visit. We did not account of reduced productivity across the life of persons suffering hypertension or its cost as we deemed that loss to not be part of the cost of treatment but the wider economic impact of the disease. This may be considered a limitation when interpreting the findings of this study.
Transition probabilities
Conversion of proportions to rates and transition probabilities was done using standard formulae with the aid of Microsoft Excel21,30 (Shown in Table 2 below).
Transition probabilities.

Conversions of proportion to a rate and then to probability were done using standard formulae. 33 (p. 51). The probability of remaining a particular state is the difference been 1 and the combined probability of transitioning away from that state during a cycle.
Sensitivity analysis
In this study, evidence on the transition probabilities was partly obtained from clinical experts as there were no relevant context-specific studies to inform their estimation. Consequently, it was not feasible to represent parameter uncertainty analysis in the form of Probabilistic Sensitivity Analysis (PSA). 5 Hence, we conducted a one-way Deterministic Sensitivity Analysis (DSA) in which ‘parameter values are varied manually to test the sensitivity of the model’s results to specific parameters or sets of parameters’ 38 (p. 724). We reflected the plausible range of the parameter estimates obtained from the clinical experts (Shown in Table 2 above). We simultaneously varied the transition probabilities with their respective lower range to get our best-case (low) estimates and then with their respective upper range to obtain our worst-case (high) estimates. In the results, we presented the uncertainty estimates as ranges around our point estimates of the cost of managing hypertension. Best practice guidelines in medical decision modelling recommend that “...where there is very little information on a parameter because either there are very few studies informing the estimation or there are no data, an expert opinion must be relied on. Usually, a conservative approach [to DSA] should be adopted with an appropriately broad range of possible estimates elicited from each expert, reflected in how opinions are combined across experts and incorporated into the uncertainty analysis” 38 (p. 726). Although our approach is consistent with the best practice guidelines for transparency, 39 future observational studies to estimate the transition probabilities will improve the point estimates of the estimated cost and enhance opportunities to conduct PSA. Also, structural uncertainty was not considered necessary as there were no alternative treatment guidelines used in Ghana that we could use to construct an alternative structure of the model for comparison. Although essential, structural uncertainty analysis is seldomly conducted compared to parameter uncertainty analysis. 30
Results
Probability of progression from one disease state to another
We modelled a hypothetical cohort of 30-years-old Ghanaians diagnosed with hypertension, initially with no complications. Given that Ghana’s average life expectancy at birth is estimated to be 63 years, we modelled the cohort for 33 years (presumably until they die or have reached the life expectancy in the country. As some of the transition probabilities were estimated from expert opinion, we used a wide plausible range as a measure of uncertainty assessment.
Our base results show that by 10 years from diagnosis, the probability of death from any of the 4 complications (ie, stroke myocardial infarction, heart failure, and chronic kidney disease) is roughly 41.03% (range: 26.74%-61.54%). By 20 years (or 243 months) from diagnosis, the probability of death (from any of the modelled complications) among the cohort is estimated to be 69.61% (range: 53.02%-85.23%). However, by the 30th anniversary (or 360 months) the probability of death among the cohort is 82.3% (range: 69.23%-93.28%).
Furthermore, our simulation shows that, within 10 years of initial diagnosis of hypertension with complications, the probability of remaining alive but with stroke is 1.74%; 4.80% for myocadiac infarction; 9.04% for heart failure; and 17.59% for chronic kidney disease. Also, by the 20th anniversary of initial diagnosis, the probability of being alive and with any of the 4 complications is roughly 17.88%, while the probability of staying alive, but with only stroke is 0.35%; 1.12% for myocardial infarction; and 12.34% for chronic kidney disease. Finally, by the 30th anniversary of diagnosis, when at least 82.3% of the modelled cohort would have died, the probability of staying alive with no complication is negligibly 0.76%, while the probability of staying alive but with at least 1 of the 4 complications is about 7.72% (See Figure 2).

The modelled probability of being in one of the states (complications) related to hypertension in Ghana.
Estimated lifetime, annual, and monthly cost of treatment
Using cost data collected from the NHIS tariffs (shown in Table 1 and Supplemental Material 1) and resource use according to the National Standard Treatment Guidelines, our simulation shows that the lifetime discounted cost of treating hypertension is about GHS 869 106 which could range between GHS 570 239 and GHS 1.202 million if the wide uncertainty in is taken into account. This is equivalent to USD 119 056 (range: USD 78 115-164 723). This lifetime cost assumes that the cohort is initially 1 or more of 4 complications (ie, stroke, myocardiac infarction, heart failure, and chronic kidney disease).
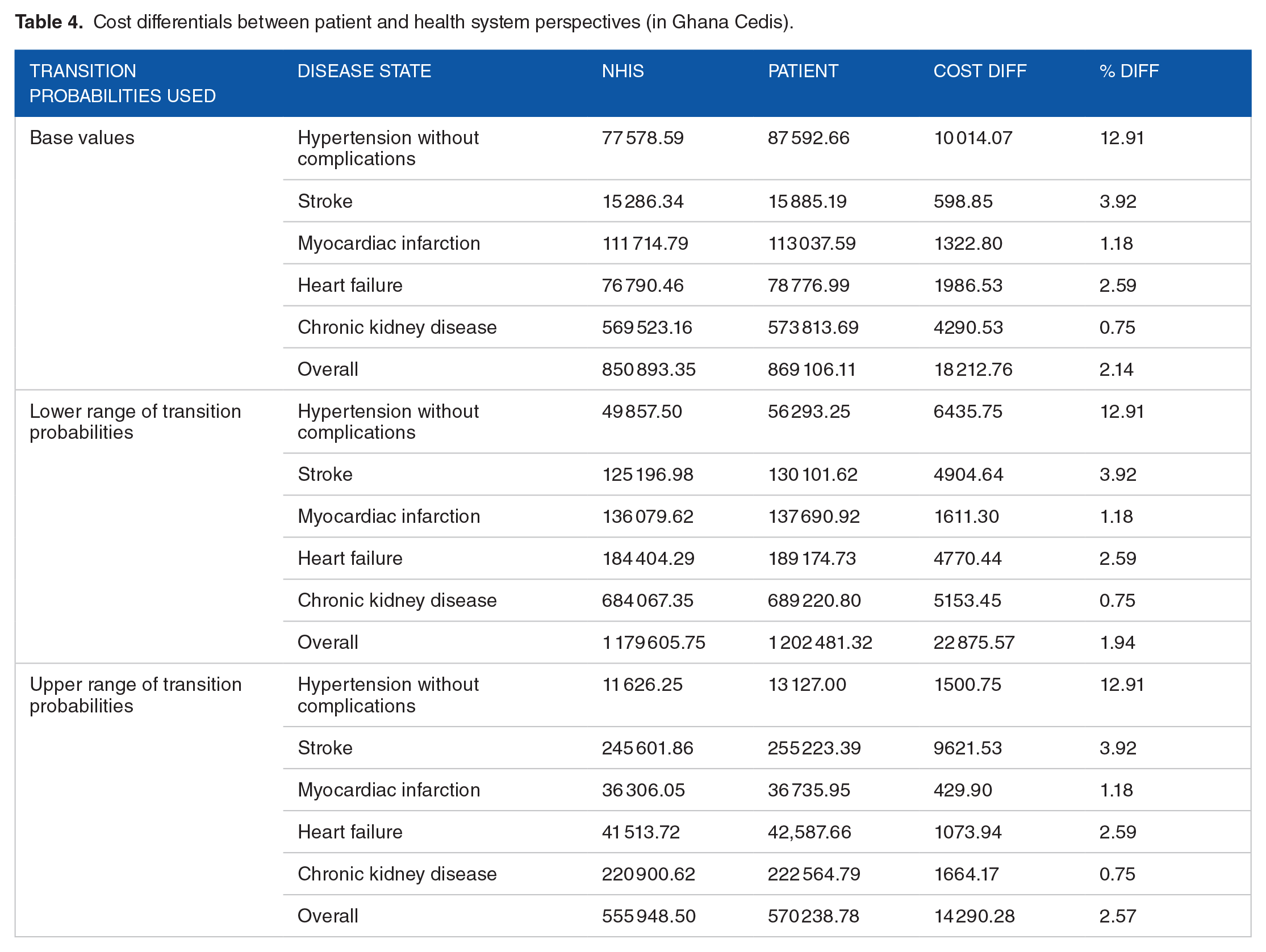
For short-term planning, the undiscounted cost of monthly treatment is estimated to be averagely GHS 3908 but may range from GHS 2091 to GHS 5801, equivalent to USD 535.36 (range: USD 286.40-794.63). However, these costs substantially vary according to the type of complications developed by a patient. For example, hypertensive patients with chronic kidney disease who may require haemodialysis have an undiscounted estimated monthly cost of GHS 2790 as compared to GHS 57 for those with stroke, but not needing hospital admission. Thus, the average monthly cost of chronic kidney disease is at least 8 times higher than that of heart failure; 6 and a half folds that of myocardial infarction and as much as 10 times that of hypertensive patients without complications. When the plausible range of uncertainty associated with the transition probability is taken into consideration, the cost differential between hypertensive patients with chronic kidney disease compared with those with heart failure is 6.7 to 7.4-folds and as much as 22 to 24-folds for patients without any complication. Table 3 provides the simulated cost from the patient perspective. The overall cost difference between the patient’s perspective of cost and that of the NHIS perspective is 2.14% (range: 1.94%-2.57%). This translates into a discounted value of GHS 18 213 over a lifetime (ranging from GHS 14 290 to GHS 22 876). Table 4 provides the simulated cost from the NHIS perspective.
Estimated cost of treatment for hypertension and related complications (patient perspective of cost in Ghana Cedis).

Exchange rate: 1 USD = 7.31 GHS.
Cost differentials between patient and health system perspectives (in Ghana Cedis).
The estimated cost of treatment for Ghana’s burden of hypertension
Extrapolating the cost of illness estimates for the overall burden of hypertension in Ghana, we used the most recent estimates of prevalence from a systematic review and meta-analysis. 1 The systematic review estimates the prevalence of hypertension in the general population to be 30.3% (95% CI: 26.1%-34.8%) (See Table 5 below). We used the point estimate as the base estimate and used the confidence interval as a measure of parameter uncertainty. The results show that the undiscounted cost for treating hypertension and related complications from the patient perspective (assuming all patients were diagnosed and received treatment is about GHS 438.124 million (USD 60.017 million). This translates into a monthly cost of 36.5 million (USD 5 million). When the associated uncertainty in the prevalence of hypertension is taken into consideration, the estimated monthly cost is between GHS 31.4 million (USD 4.3 million) to GHS 41.93 million (USD 5.744 million). A total amount of 71% of the estimated cost will likely be due to treatment for chronic kidney disease with 7%, 9%, and 11% for hypertension without complications, heart failure, and myocardial infarction, respectively.
Estimated cost of treatment for hypertension in Ghana based on the prevalence rate.

Exchange rate: 1 USD = 7.31 GHS as of April 2022.
Discussion
This study simulated the cost of treating a cohort of patients with hypertension who have the risk of developing at least 1 stroke, heart failure, myocardial infarction, and/or chronic kidney disease. Our simulation shows that on average, the probability of being alive and without any complications by 30 years of the initial diagnosis is negligibly 0.76%. The 10-year probability of survival with or without any complication is 58.97% (range: 38.46%-73.26%), which significantly declines to 30.39% (range: 14.77%-46.98%) by the 20th year of living with hypertension before plummeting drastically to 17.7% (range: 6.72%-30.77%) after 30 years of initial diagnosis. These findings are consistent with survival analysis conducted in Africa. 40 In the context of Ghana, there has not been a detailed survival analysis of hypertensive patients (to the best of our knowledge) to enable us to compare with our results to further affirm the validity of the simulation. Under the circumstances, we presented the results to internal medicine physicians and epidemiologists who provided consistent opinions in support of the validity of the simulation.
Furthermore, our simulation suggests that the average discounted cost of treatment for hypertension over a lifetime (approximately 33 years after diagnosis) is about GHS 869 106 (USD 119 056), ranging from GHS 570 239 (USD 78 145) to GHS 1 202 481 (USD 164 723), based on the plausible range of transition probabilities in the disease progression. These estimates, which translate into an undiscounted average monthly cost of GHS 3908 (USD 535) appeared to be similar to previous cost-effectiveness studies of hypertension medicines and community-based intervention in Ghana. 15 This estimated cost from the patient perspective is likely to be unaffordable for out-of-pocket paying patients. For instance, our simulated cost of GHS 288 (USD 40) for monthly treatment of uncomplicated hypertension is roughly 71% of the minimum daily wage per month (GHS406) if a person is not covered under the social health insurance scheme, with an estimated coverage of only 40% and with rampant out-of-pocket payments amongst the insured. 41 Additionally, our estimate of approximately GHS 2790 undiscounted monthly cost of treatment for hypertensive patients with chronic kidney disease is also consistent with an average of GHS 2800 estimated by the Tamale Teaching Hospital for patients receiving treatment in that facility but is largely beyond the income levels of most Ghanaian. Ironically, long-term treatment with haemodialysis (life-saving management of chronic kidney disease) is also considered too expensive and excluded from the benefits package of the NHIS. 34 Our simulation shows that up to 71% of the overall cost of treating hypertension with any complication is likely to be due to chronic kidney disease. A recent report of the Ghana renal registry corroborates that most patients on kidney replacement therapy in Ghana resulted from hypertension (38%) and diabetes and that 96.2% of them required haemodialysis (the main cost driver in the cost of treating hypertensive kidney disease in our simulation). 42
Our estimate show that using the recent evidence on the plausible prevalence of hypertension, the economic burden (in terms of treatment cost) is roughly GH¢ 438.124 million (ranging from GH¢ 377.394 million to GH¢ 503.192 million), which represents roughly 0.08% of the gross domestic product (GDP), but ranges from 0.07% to 0.09%) in 2022. In context, Ghana’s health expenditure is estimated at 3.4% of GDP on health, hence comprehensively addressing the treatment needs of hypertension and related complications may require only a small proportional increase in health spending relative to the GDP. Ghana’s per capita health expenditure of USD 75 is lower than the African average of USD128 per capita and signals a need for more and efficient investments in health, including addressing the treatment needs of those living with hypertension and related complications.
Also, the treatments recommended for some hypertension and related complications by the standard treatment guidelines are not readily available in all parts of the country. For example, there are facilities for haemodialysis in patients with kidney disease, but they are only available in 5 out of 16 political and administrative regions of the country. 42 Thus, the cost estimated in this simulation better represents a protocol-based cost of illness rather than the ‘true cost’ experienced by all patients across the country. Similarly, the majority of hypertension patients in Ghana are unaware of their status, and those aware are often not on appropriate orthodox treatment or are non-compliant with the recommended regimen.16,43 A previous study attributed the large degree of treatment non-compliance to the high cost of treatment. 29
Limitations of the Study
The main limitation of the study relates to structural and parameter uncertainties. Structurally, we used only 4 (stroke, myocardial infarction, heart failure, and chronic kidney) amongst numerous plausible complications associated with hypertension. Although the choice of these potential complications was informed by the advice of expert clinicians based on complications that contribute greatest to hypertension-related mortalities in Ghana and tend to require resource-intensive treatment, the omission of other equally important complications such as coronary heart disease and erectile dysfunction must be considered as structural limitations of the model. With the improved availability of data, future simulations should endeavour to include as many complications as feasible.
We conducted an extensive literature search but did not find context-specific high-quality evidence from clinical trials and observational studies to precisely estimate the probabilities of moving from one disease state to another (transition probabilities). As guided by the Society for Medical Decision Making (SMDM) guidelines, we elicited the transition probabilities from expert opinion. In doing so, we also elicited the plausible range of the parameter estimates which was used to test the sensitivity of our base results. This also resulted in a wide range of cost estimations to reflect the level of uncertainty in our data. In this regard, future studies should explore the rate of developing complications among hypertensive patients in Ghana, which will contribute to more precise cost estimates in future simulations.
Furthermore, the unit cost data were taken from NHIS price and tariff list, which some industry players opine that, may be less than the ‘true cost’ of drugs and services in the market. Also, the NHIS service tariffs are differentiated for the public, private for-profit, and private not-for-profit, as well as the different levels of care although the medicines list, has uniform prices. For simplicity, we used the service tariffs for primary hospitals for common procedures and services as the primary hospitals provide more than 95% of the care required by hypertensive patients in Ghana. 44 The treatment protocol for hypertension treatment in tertiary hospitals which are assessed by less than 5% of the population also tends to slightly differ from the national Standard Treatment Guidelines. Against the backdrop of the aforesaid, we decided to use the tariffs for primary hospitals which represents to a large extent, the usual practice for hypertension management in Ghana, but this should be considered a limitation as our simulation does not provide a differentiated cost of treatment based on the type of health facility accessed by patients in the country.
Implications for Health Policy and Research
In terms of health policy, it will be imperative for Ghana to initiate comprehensive healthy lifestyle interventions aimed at delaying the onset of hypertension (HPT) and encouraging routine blood pressure monitoring. Such measures are crucial for the early detection and effective management of pre-hypertension and hypertension. Research indicates that these interventions significantly mitigate the development of complications, most notably chronic kidney disease (CKD)—which our study highlights that CKD is the complication that could account for approximately 67% of the lifetime treatment costs associated with hypertension. Therefore, it is essential for future health policies to prioritize community-based hypertension prevention and management strategies.
Additionally, the Government of Ghana need to address the impoverishing out-of-pocket payments associated with hypertension-related complications, particularly CKD treatment costs substantially exceed the average income levels in Ghana and are not covered by the National Health Insurance Scheme (NHIS) benefit package. Hence, future health policies must incorporate strategies to alleviate the economic burden posed by these complications.
Also, the Ghanaian health system should emphasize the establishment of wellness centres and non-communicable disease (NCD) clinics within all primary healthcare facilities. This strategic move will enhance the capacity of the healthcare system to deliver comprehensive and effective care for hypertension and its associated complications, thereby improving public health outcomes.
Lastly, future studies should also focus on the rate of developing complications among hypertensive patients in Ghana. This will contribute to more precise cost estimates in future simulations.
Supplemental Material
sj-docx-1-his-10.1177_11786329241241909 – Supplemental material for Estimating the Lifetime Cost of Managing Hypertension in Ghana: A Modelling Study
Supplemental material, sj-docx-1-his-10.1177_11786329241241909 for Estimating the Lifetime Cost of Managing Hypertension in Ghana: A Modelling Study by Fidelis Atibila, James Avoka Asamani, Emmanuel Timmy Donkoh, Rob Ruiter, Gerjo Kok and Gill Ten Hoor in Health Services Insights
Supplemental Material
sj-xlsm-2-his-10.1177_11786329241241909 – Supplemental material for Estimating the Lifetime Cost of Managing Hypertension in Ghana: A Modelling Study
Supplemental material, sj-xlsm-2-his-10.1177_11786329241241909 for Estimating the Lifetime Cost of Managing Hypertension in Ghana: A Modelling Study by Fidelis Atibila, James Avoka Asamani, Emmanuel Timmy Donkoh, Rob Ruiter, Gerjo Kok and Gill Ten Hoor in Health Services Insights
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Ethical Consideration
This study was part of a larger study in Ghana with ethical approval from the Institutional Review Board of the Christian Health Association of Ghana (CHAG) (PIN -15052019).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.