
Abstract
Background:
In developing nations, almost two-thirds of people with active tuberculosis (TB) remain undetected and untreated. Delays in seeking treatment increase the severity of the illness, the likelihood of mortality, and the risk of the infection spreading to others in the community. Thus, this study aimed to assess the magnitude of delay in treatment-seeking and its associated factors among new adult pulmonary tuberculosis patients attending public health facilities in Habro District, West Harerge Zone, Oromia Region, Eastern Ethiopia.
Methods:
A health facility-based cross-sectional study design was conducted among 420 randomly selected patients with pulmonary tuberculosis who visited public health facilities in Habro District from September 5 to October 5, 2022. Binary logistic regression analysis was used to determine the relationship between the dependent and independent variables, and a 95% confidence interval was used to select significant variables.
Result:
Twenty-one days after the start of their illness, 62.38% (95% CI: 57.4%, 66.6%) of the patients sought an initial consultation. Being female (AOR = 2.14, 95% CI: 1.26, 3.65), having poor knowledge about TB (AOR = 3.10, 95% CI: 1.77, 5.43), having no contact history with TB patients (AOR = 3.52, 95% CI: 1.29, 9.58), having clinically diagnosed pulmonary tuberculosis (AOR = 2.16, 95% CI: 1.26, 3.67), and living a long distance from the nearest health facility (AOR = 2.87, 95% CI: 1.31, 6.23) were important predictors contributing to TB patient treatment delay.
Conclusion:
In the current study, more than three-fifths of TB patients delayed seeking treatment. Thus, awareness of tuberculosis should be created, especially targeting females and communities found at a distance from the health facility. Additionally, health professionals should emphasise the importance of getting medical attention early and knowing how to suspect and identify tuberculosis symptoms.
Introduction
Tuberculosis (TB) is an airborne infectious disease caused by the rod-shaped acid-fast bacillus Mycobacterium tuberculosis (MTB) that typically affects the lungs (pulmonary TB) but can also affect other parts of the body (extrapulmonary TB). 1 It is a major global health problem that a quarter of the world’s population has Mycobacterium tuberculosis infection and is at risk of developing TB disease, and it is one of the top 10 global causes of death and the primary cause of death, in which an estimated 10.0 million people contracted TB in 2019 2 and an estimated 10.6 million people fell ill with TB, with a total of 1.6 million deaths in 2021. 3 Among the top 30 high-TB-burden countries, Ethiopia ranked 12, with the incidence and mortality from TB remaining high. 4
According to the 2020 Global TB Report, Ethiopia is among the top 30 countries with high TB and TB/HIV burdens, with an estimated annual TB incidence of 132/per 100,000 population and a death rate of 19 per 100,000 population. 2 The study revealed that approximately two-thirds of patients with active tuberculosis remain undiagnosed and thus untreated, and more than 81% of TB cases and deaths occur in developing countries. 5 The first national prevalence survey in 2011 reported that 55% of cases were first identified and were not on treatment until the survey. 6 The TB case detection rate in Ethiopia was 67.3% in 2015, which was higher than the 2014 achievement (53.7%) but below the target set by the FMOH and WHO. 6 However, TB remains a major public health problem in Ethiopia, with approximately 29% of TB cases still missing each year. 3 People with tuberculosis who go undiagnosed and untreated may die from the disease or develop a chronic illness that makes them more likely to spread, which would keep the epidemic going. 3
The main problem in controlling TB is improving the detection of sputum smear-positive TB cases, which depends on passive case findings and self-presentation to a health facility.7 -9 Failure to promptly detect and treat active TB cases affects patients, the community, and the healthcare system. 10 Extreme delays exacerbate disease severity, advance dissemination, prolong patient suffering, increase fatality, cause adverse treatment outcomes, such as failure and drug resistance, and fuel disease transmission to close contacts.11 -13
In Ethiopia, almost 50% of all patients with suspected pulmonary tuberculosis have a history of delayed treatment seeking. 5 Hence, the remaining half will continue to transmit TB infection in the community until it is detected and treated by another healthcare provider. 14 A single untreated case of smear-positive tuberculosis can infect up to 15 individuals annually and over 20 individuals during the natural course of the disease.15,16 Since the smear-positive index patient is found to infect between 30% and 40% of his contacts without detection, identification of transmission factors, such as the number of incident infectious cases and the length of their infectiousness, is necessary for successful control. 17
In Ethiopia, like most TB control programs, TB case-finding relied mainly on passive and community-based enhanced TB case-finding as the main strategy, with a focus on diagnosing TB among people who actively sought medical care with TB symptoms or were identified from the community through health extension workers. With this strategy, the program achieved its goal of detecting no more than two-thirds of the estimated annual TB cases. 6 In addition, Ethiopia launched a second-generation health extension worker (HEW) program intending to deliver health information and bring behavioral changes to communicable diseases to the community. 18 However, the burden of the disease and poor treatment-seeking behavior among patients are still high.5,19,20 By enhancing active case discovery, boosting access to TB care, offering early treatment, and reducing the duration of infection in the community, determining the extent and factors that are linked to patient delay in treatment-seeking will assist in enhancing TB control. 21 Therefore, this study aimed to assess the magnitude of delays in treatment-seeking and associated factors among new patients with pulmonary TB in the Habro district of eastern Ethiopia.
Method and Material
Study design and setting
A facility-based cross-sectional study was conducted from September 5 to October 5, 2022, in the Habro district. Habro Woreda is one of the 15 woredas in the western Harerge zone and is found in the eastern part of the Oromia regional state of Ethiopia. It is 75 km from the zonal town of Chiro and 400 km from Addis. Woreda has one general hospital, seven functional health centers, and 32 functional health posts. General hospitals and functional health centers provide services for TB diagnosis and treatment.
Population and sample
The source population for this study was all new adult pulmonary tuberculosis patients attending TB clinics in public health facilities in Habro Woreda, whose age was greater than or equal to 18 years. The study population consisted of randomly selected adult patients with pulmonary tuberculosis attending TB clinics in the public health facilities of Habro Woreda between September 5 and October 5, 2022. Patients with drug-resistant TB, those who had been transferred to another woreda or public health center before data collection began, and those who were unable to respond were not included in the study.
The sample size for this study was determined using a single-population proportion method, and there was a 46% prevalence of delay in treatment-seeking delays in a study conducted in Adama 5 with a 95% confidence level, a 5% margin of precision, and a 10% nonresponse rate. The calculated sample size was 420. The sample size for the second objective (for risk factors) was calculated considering the assumption of a double population proportion formula (80% power of the study, 95% confidence interval, and 1:1 unexposed to exposed ratio), and the sample size was 196, 308, and 372 for the risk factor of rural residence, 22 number of household members, 23 and TB-associated stigma 11 respectively. However, we decided to use 420 as the final sample size because the estimated sample sizes for risk factors were smaller than 420.
Sampling procedure and technique
In Habro District, TB diagnosis and treatment services are offered by public health facilities, including seven health centers and one general hospital. All newly diagnosed cases of pulmonary TB one year before the study period were enrolled in the study. Following a review of the TB unit register from the previous year, a proportional allocation of patients was made according to the anticipated number of new PTB cases in each health facility treatment program (Figure 1). Subsequently, until the desired sample size was reached, all new PTB cases were chosen from all healthcare facilities using systematic random sampling approaches.
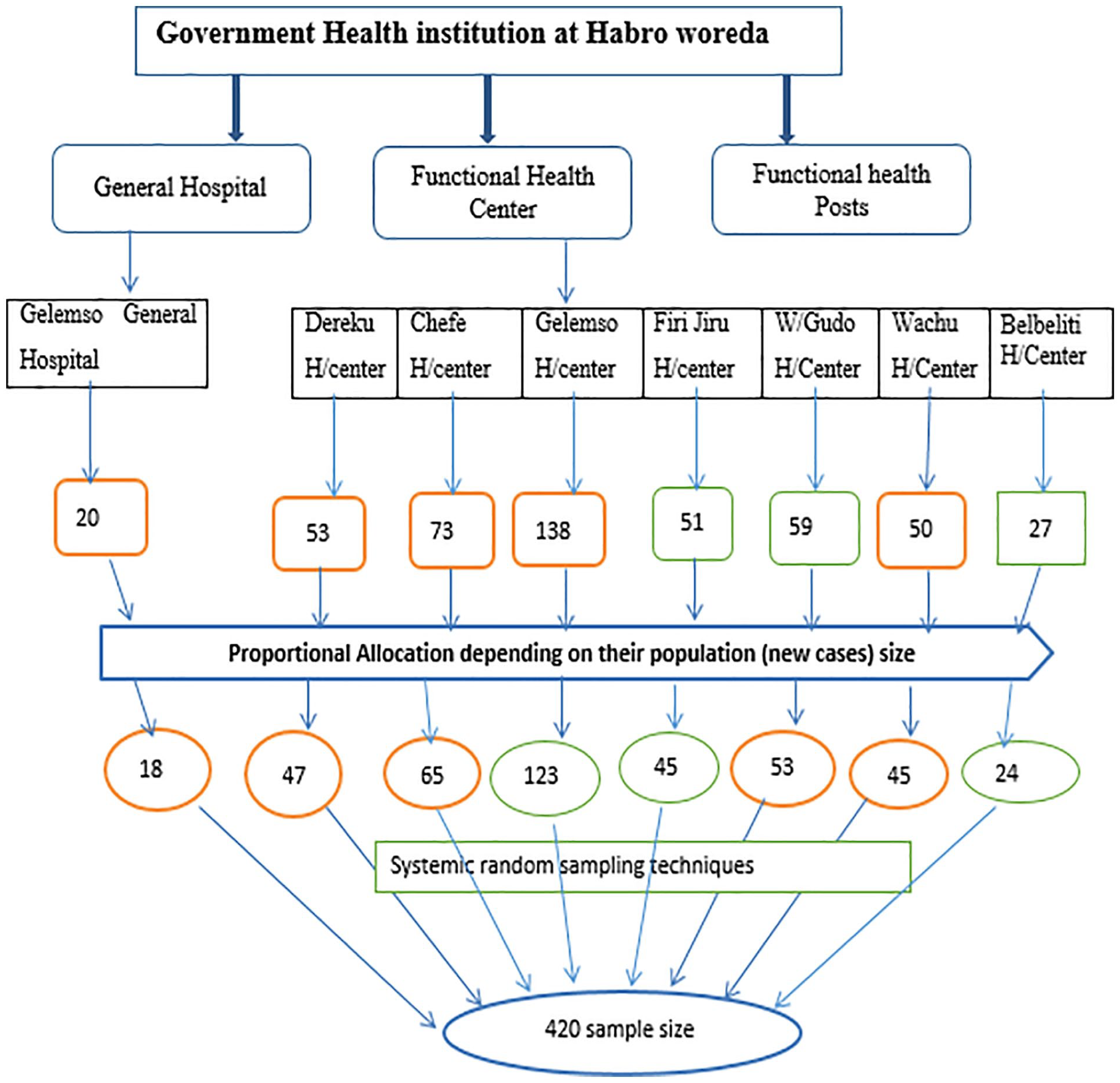
Diagrammatic representation of sampling procedures in public health facilities of Habro District, Eastern Ethiopia.
Data collection methods and quality control
Data were gathered using a structured questionnaire modified from that created by the TB CARE II project. 24 To ensure that the questions were clear and understandable by the respondents, the questionnaire was first prepared in English and then translated into the local language, “Afan Oromo.” It was then translated back into English to maintain its consistency. By providing 2-day training, 8 clinical nurses with data collection experience, along with 2 supervisors (BSC health workers), gathered the data.
To maintain the quality of the data, the questionnaires were carefully designed, a pretest was conducted, and the necessary modifications were made. After data collection, the questionnaires were reviewed and checked daily for completeness, accuracy, and clarity by supervisors and the principal investigator, and the necessary feedback was offered to the data collectors the next day. All the participants’ answers were kept confidential.
Study variables
The outcome variable in this study was TB treatment-seeking delay. The independent variables were
Operational definition
Data management and analysis
Epi Data Version 3.1 was used to enter the data, which was then exported to STATA Version 15 for cleaning and analysis. The patient’s baseline characteristics were described using descriptive analysis and summarized as frequencies, proportions, means, and SD. A binary logistic regression model was used to determine the factors associated with delayed TB treatment. A bivariable analysis was conducted, and independent variables with a value of less than 0.25 were taken as candidate variables and considered in the multivariate analysis. An adjusted odds ratio along with 95% of the confidence interval reported to show the strength of the association and independent variables that have a P value < .05 were declared to be significant tests with an outcome.
Ethical considerations
This study was approved by the Institutional Health Research Ethical Review Committee (IHRERC) of the School of Public Health of the College of Health and Medical Sciences, Haramaya University. Permission was also obtained from each health facility in which the data were collected, and informed consent was obtained from each participant.
Result
Sociodemographic characteristics of study participants
Out of 8 public health facilities, four hundred and twenty (420) study participants were interviewed, with a response rate of 100% in this study. Among the participants, 213 (50.71%) were females, and 207 (49.29%) were males. Approximately 50.48% of the participants were aged between 18 and 34 years, and the mean age of the participants was 35.89 years (SD ± 15.82).
The majority of participants (87.38%) were Muslims, and 74.52% were married. Almost three-quarters were rural residents, and 73.53% had community health insurance. The average family size of the households was 4.1 (SD ± 2.1). Among the respondents, 85.24% lived within an average distance of 4.14 (SD ± 3.4) kilometers to the nearest health facility from their home (Table 1).
Sociodemographic characteristics of new adult pulmonary TB patients in public health facilities of Habro District, West Harerge Zone, Eastern Ethiopia, September 5 to October 5, 2022 (n = 420).

Abbreviations: ETB = Ethiopian birr.
single, divorced, and widowed.
Individual (knowledge and perception) factors
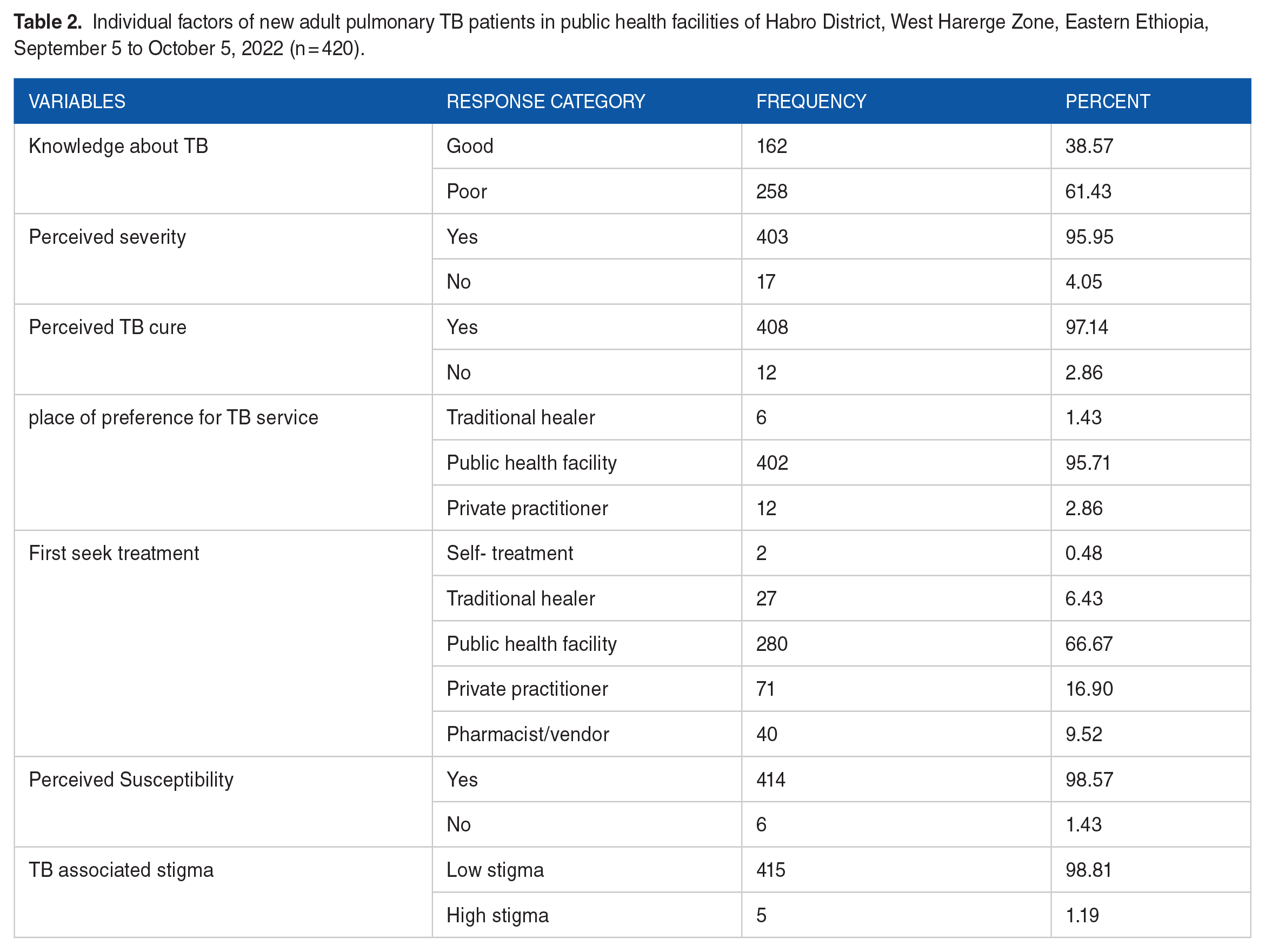
A total of 258 (61.63%) participants had poor knowledge of TB, and 162 (38.57%) had good knowledge about tuberculosis. Most (95.95%) perceived TB as a serious disease and preferred to seek services from public health facilities. Two-thirds (66.67%) were contacted by a public health facility for the first symptom, and 98.81% were perceived as nonstigmatized (Table 2).
Individual factors of new adult pulmonary TB patients in public health facilities of Habro District, West Harerge Zone, Eastern Ethiopia, September 5 to October 5, 2022 (n = 420).
Medical and clinical factors
Approximately 2% of the study participants were HIV-positive, and 256 (60.95%) were clinically diagnosed with pulmonary TB. Approximately 6.67% of the participants had a history of contact with TB patients, and 7.6% had other chronic diseases. Approximately one-fourth (21.19%) of the participants presented with severe illness at first contact, and the majority (94.29%) presented with cough (Table 3).
Clinical characteristics of new adult pulmonary TB patients in public health facilities of Habro District, West Harerge Zone, Eastern Ethiopia, September 5 to October 5, 2022 (n = 420).

Diabetes (5.24%) and hypertension (2.38%).
The magnitude of treatment-seeking delay
The magnitude of patient delay for seek-Tb service was 62.38% (95% CI: 57.4%, 66.6%). The overall mean and median number of days of patient delay were 36 and 30 days, respectively. In addition, the maximum patient delay was 120 days when seeking TB services.
Factors associated with a delay in seeking treatment
In the bivariate models, sex, age in years, educational status, occupation, income, residence, knowledge, perceived severity, perceived cure, previous exposure to TB, types of TB, loss of appetite, and distance were found to be significantly associated with the dependent variable (less than 0.25) and were considered for the multivariable model. Finally, knowledge of TB, sex, contact history or exposure to TB patients, type of TB, and distance to the nearest health facility were significantly associated with delayed seeking of TB treatment.
Female patients were 2.15 (AOR = 2.15, 95% CI: 1.29, 3.58) times more likely to delay seeking TB treatment than their male counterparts. Clinically diagnosed pulmonary tuberculosis patients were 1.27 (AOR = 1.27, 95% CI: 1.23, 3.43) times more likely to be delayed than the study participants with bacteriologically confirmed pulmonary tuberculosis. Participants from a distance ⩾10 km were 2.92 (AOR = 2.92, 95% CI: 1.39, 6.15) more likely to delay seeking TB treatment than those from the nearest health facility. When compared to participants with good knowledge of TB, respondents with poor knowledge were 3.08 (AOR = 3.08, 95% CI: 1.79, 5.32) more likely to delay seeking treatment (Table 4).
Factors associated with a delay in seeking treatment among new pulmonary TB patients in Habro District, West Harerge Zone, Eastern Ethiopia, September 5 to October 5, 2022 (n = 420).

P value < .05. **P value ⩽ .001. 1 = reference of the variable.
Discussion
This study found that 62.32% of the patients delayed seeking TB services. Female sex, poor knowledge of TB, no history of TB contact, type of TB diagnosis, and distance from the facility were significant factors associated with delays in seeking TB treatment services.
These magnitude results of this study are almost identical to those of studies conducted in Ibadan, Nigeria (61.8%) 26 ; the North Wollo Zone of Amhara (62.3%) 27 ; and North Showa, Ethiopia (59.9%). 15 However, the magnitude of the current study is greater than that in previous studies conducted in Zimbabwe (48%), 14 Adama (46%), 5 Addis Ababa (42.1%) 11 and Tigray, Northern Ethiopia (52%). 28 However, the magnitude of the present study was lower than those in studies conducted in Iran (65.5%) 29 and the Bale Zone (96%). 25 This gap may be due to sample size, sociodemographic status, and knowledge of TB. Another reason might be the difference in study settings and geographic inaccessibility to healthcare facilities. 15
The proportion of delays in seeking care for TB was significantly higher among female patients. This result is consistent with studies conducted in Iran, 29 Ibadan, Nigeria, 26 Adama Town, 5 the North Wollo Zone of the Amhara Region, 27 Wollega, 30 and Tigray. 28 Female delays may be caused by a variety of factors, including work overload, the submissive role of the family, women’s limited decision-making authority, unemployment, accessibility, a low level of education, and female involvement in domestic duties. 31
The proportion of delays in seeking treatment was high among participants with poor knowledge of TB. This result is in line with those of studies conducted in Peru, 32 Italy, 33 Mekelle, 22 the Oromia Special Zone, the Amhara Region, 20 Adama Town 5 and North Wollo. 27 This might be a result of the respondent’s awareness of tuberculosis, as those who are well informed about the disease might be more motivated to seek treatment at an early stage. 27
In this study, respondents who had no close contact or household members who had tuberculosis were 48% more likely to delay seeking treatment than those with a household member or close contact exposure to tuberculosis. This may be the result of community-wide health education about TB that emphasizes the signs and symptoms of the disease, as well as the benefits of early detection and TB infection prevention. As a result, these activities to raise awareness may increase household contact and TB screening among the general population to reduce treatment delays.
This finding indicates that respondent patients with clinically diagnosed pulmonary tuberculosis were more likely to delay seeking treatment compared to bacteriologically confirmed pulmonary TB patients, which is contrary to the findings of the study by Mekelle. 22 The observed difference can result from a range of symptoms, gradual progression, or a less severe clinical manifestation at the beginning. 11 Additionally, patients clinically diagnosed with pulmonary tuberculosis are less likely to cough and expectorate sputum, prompting them to seek medical attention.
When compared to short walking distances to health facilities, patients who had long walking distances between a public health facility and their home were 14.18% more likely to delay seeking treatment. This result is in line with those of studies conducted in the Bale Zone. 25 This could be because it is difficult to get to a medical institution due to distance or a lack of roads. 34 Additionally, it is difficult to get to a medical center because of the topography and because the population is dispersed around the area. 25
Although this study included all public health facilities that provide TB treatment services, it has some limitations. There may have been some recall bias when respondents were asked questions about past events because of the cross-sectional design used in this study.
Conclusion
The prevalence of delays in seeking treatment among patients with new pulmonary TB was high in this study. Being female, having poor knowledge about TB, having no previous contact with TB patients, having clinically diagnosed pulmonary TB, and having a distance of ≥ 10 km were significantly associated with patient delay. Therefore, addressing the significant factors is needed to prevent delays in seeking treatment among patients with pulmonary TB in the study setting. Together with health extension workers, health professionals should focus on raising public awareness of tuberculosis symptoms, especially among females, making free diagnostic and treatment services available in the nearest area, and encouraging people to seek early care and treatment. Health professionals should also emphasize the value of early health-seeking and how to suspect and recognize TB symptoms.
Footnotes
Acknowledgements
The authors are grateful to the data collectors, supervisors, West Hararghe Zonal Health Department, Gelemso General Hospital, Habro Woreda Health Office, administrative authorities who took part in the study, and Haramaya University for their valuable assistance.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations and acronyms
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; FMOH, Federal Ministry of Health; MDR, multidrug resistant; PTB: pulmonary tuberculosis SD: standard deviation; TB: tuberculosis, WHO: World Health Organization
Authors Contributions
This idea was developed by Assefa Getiye, who made major contributions in terms of data evaluation, rough drafts, and final writing. Data analysis, drafting, and manuscript preparation were performed by all coauthors. The final draft of the manuscript was read and authorized by all authors who agreed to the details of this work.
Consent to Publication
Not applicable