
Abstract
Introduction:
A timely integrated diagnostic and care trajectory for children with a developmental disability may prevent severe problems in later life. In Flanders, Belgium, different types of governmental regulated and subsidised settings offer diagnostic evaluations, as (part of) their mission. However, they operate in a non-coordinated way inducing severe accessibility problems for the public. This article studies the factors impacting on interorganisational collaboration and proposes an interorganisational conceptual model improving accessibility.
Methods:
Focus groups were performed per type of organisation. Qualitative data were categorised thematically in an iterative process of data- and researcher triangulation. A member check validation was organised.
Results:
Fifty-nine individuals participated in 6 focus groups. Structural and agency-related barriers for interorganisational collaboration were identified at micro, meso and macro level. Participants provided suggestions for better interorganisational collaboration.
Discussion:
To improve accessibility adapted to patients’ needs, a patient-centred, integrated and interorganisational network model grounded in a stepped care logic is proposed to adapt the current organisation-centred model.
Conclusion:
A timely, integrated, diagnostic and care trajectory for children with a developmental disability preventing severe problems in later life requires an integration of services during the overall care trajectory of children by means of interorganisational collaboration.
Introduction
Early detection, timely diagnostic evaluations, and early intervention for children with a neurodevelopmental disability (DD), may prevent academic failure, school behaviour problems, dropout, delinquency and the development of more severe mental health issues in later life.1,2 A diagnostic evaluation can have different goals: (1) make an inventory of the symptoms, (2) classify a disorder or syndrome, (3) assess disorder related needs, (4) indicate needs for care and support, (5) facilitate access to care and support and (6) grant access to financial support.1-7 All areas of development need to be evaluated by a multidisciplinary team.1,3,8,9 As DD vary in severity and complexity,3,4 the diagnostic team can vary in composition and level of specialisation. The health care trajectory10,11 of children with a DD identifies the events, turning points and phases in the diagnostic, treatment, rehabilitation, or support processes. 12 Diagnostic evaluations are not ‘one shot’ events at the start but iterate along the care trajectory. A general diagnostic evaluation of the overall functioning and the needs of the child can be sufficient to start the supportive trajectory, while in other phases more in depth and specialised expertise might be needed. A needs-based diagnostic evaluation to support the child and his context are preferred to a categorical diagnosis. 12
In Flanders, Belgium, different types of public organisations, programmed, regulated and financed by the government, offer diagnostic evaluations of DD besides private practices: Centres for Ambulatory Rehabilitation (CAR), Autism Reference Centres (ARC), Centres for Developmental Disabilities (CDD), Mental Healthcare Centres (MHC), Pupil Guidance Centres (PGC) and Ambulatory Hospital Services for Paediatric Psychiatry (APP). There are more than 150 individual centres, geographically distributed over the Flemish Region. The number per type of centre varies between 2 (CDD) and 61 (PGC). Except for CDD, all types of organisations combine diagnostic activities with activities of care or support. The formal target group of each type of organisation is defined by governmental regulations. All organisations are limited in diagnostic capacity, determined by the governmental planning and financing. However, in practice, accessibility problems emerge characterised by long waiting times, financial inequalities, exclusion of certain age and pathology groups and an unequal regional distribution of diagnostic services. 9 Coordination and integration of the different types of services is lacking 9 resulting in long waiting periods, even a lack of diagnostic activity for certain age and pathology groups (with regional differences).
The field of organisations offering (subsidised) multidisciplinary diagnostic evaluations for children with a DD in Flanders is heterogeneous and characterised by subregional differences. Activities are fragmented, with non-necessary patient referrals and transfers between professionals and organisations inducing a real risk of decreasing quality of care, problematic continuity and accessibility of care and increasing societal costs. 13
Integrated care aims theoretically at an improved coordination of services at the micro, meso and macro level of a health system. The micro level focusses on interprofessional collaboration, participation of patients and informal care along the trajectory; The meso level considers how collaborative interorganisational networks address the needs of a population along the care continuum14-17 and across organisational and disciplinary boundaries. 18 The macro level focuses on the integration of different sectors and policy domains.14,19,20 But many barriers to coordinate and integrate care are identified in literature: rigid organisational boundaries, poor interorganisational communication, a lack of mutual understanding, competition, cultural differences, and rules, diverging regulations and financing mechanisms for health organisations also lacking incentives to collaborate and improve public health goals.15,21
This paper aims (1) to identify the determinants of collaboration between organisations providing diagnostic evaluations for children with a suspected DD in Flanders and (2) to develop a conceptual model to support the provision of accessible and integrated diagnostic evaluations along the care trajectory of the child, taking into account the particularities of the institutional field. 22
Methods
This is a qualitative policy support research project funded by the Flemish government, performed in 2021 and 2022. We focus on the experiences and opinions of stakeholders in the field of multidisciplinary diagnostic evaluations for children with a DD on barriers and facilitators for interorganisational collaboration during the diagnostic activities.
Data collection
We organised focus groups per type of organisation. Participation was limited to 1 person per centre. Inclusion criteria for participants were (1) working in a specialised, governmentally regulated and subsidised multidisciplinary organisation offering diagnostic evaluations of DD, (2) having professional experience in diagnostic evaluations of DD and (3) having practical knowledge on the organisation and practice of the diagnostic activity.
The focus groups discussed the following aspects: (a) a concept (the content) of diagnostic evaluations of DD in children; (b) an illustration (a vignette) of a theoretical diagnostic trajectory and (c) barriers and facilitators in interorganisational collaboration followed by an inventory of suggestions to improve interorganisational collaboration. This article focuses solely on the interorganisational collaboration and its barriers and facilitators problem. The data on the concept of diagnostic evaluations (a) and on the diagnostic trajectory of children with a DD (b), have been published elsewhere. 12
A literature review on diagnostic evaluations of children with a DD, healthcare trajectories and interorganisational collaboration was done to support the development of topic lists for data collection and to support data collection and data analysis.
The focus groups were audiotaped. Participants gave their informed consent at the beginning of the focus groups.
The focus groups were moderated by (EC), supported by a note taker and observer. After each focus group the researchers debriefed on content and process and we discussed on issues to probe in follow up rounds.
To develop the conceptual organisational model, we integrated findings from the focus groups with literature on stepped care, integrated care and integrated health services.
Participation
Fifty-nine persons participated in 6 focus groups (Table 1). The duration varied between 54 minutes (PGC VCLB) and 3h31 (MHC). The planned APP focus group was cancelled because of low participation. The PGC focus group was split up in 2 for organisational reasons, to maximise participation.
Participation in focus groups per type of setting.
Data analysis
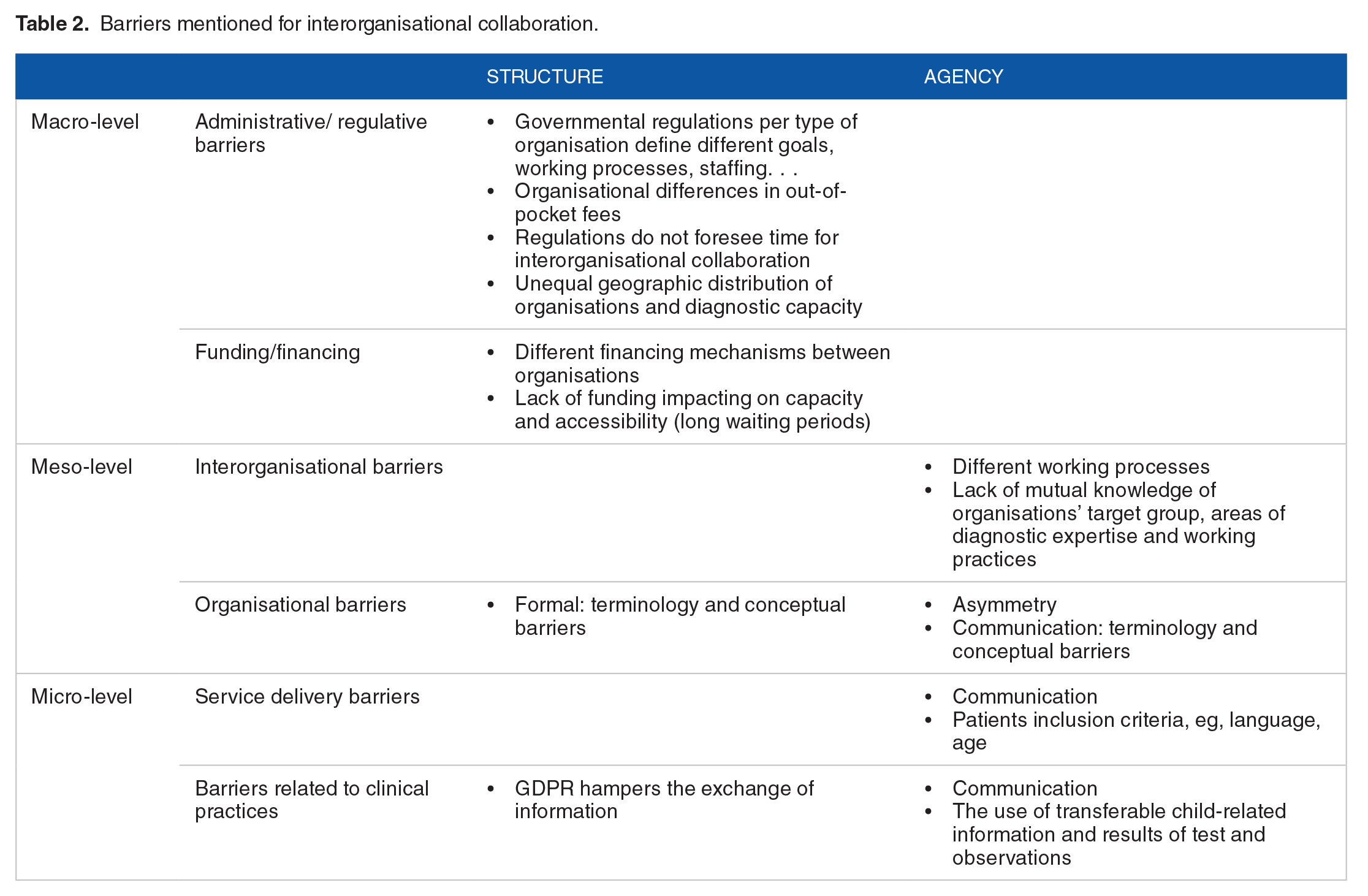
Data were thematically analysed23,24 and categorised using the framework of Auschra. 15 They distinguish structural and agency-related barriers in interorganisational collaboration at different levels: administrative/regulative barriers and funding barriers at the macro level; barriers concerning inter-organisational collaboration and internal organisational barriers at the meso level and barriers concerning service delivery and clinical practices at micro level (see Table 2).
Barriers mentioned for interorganisational collaboration.
EC and ML iteratively analysed the data in a process of researcher and data-triangulation.25,26 A member check validation with a steering committee with representatives of every type of the included organisations was done to increase credibility, relevance and trustworthiness of the findings.27,28
Because of the large amount of data, we only select 1 reference quote per theme in the results section. More quotes are available on request.
Results
Current interorganisational collaboration
All participants report they collaborate with other organisations. However, the meaning given to collaboration as well as collaboration practices vary. MHC describe collaboration as the referral of children with diagnostic needs to mainly CAR and PGC. CDD occasionally collaborate pragmatically and informal when expertise is lacking within their multidisciplinary team. Collaboration is informal, based on trust and individual opinions on the quality of the diagnostic activities of other organisations. Participants of the CAR report 2 aspects: (1) most CAR have agreements with other organisations maintain the first patient contact date to avoid extension of the waiting times when transferring the child, and (2) CAR with less diagnostic capacity and not performing diagnostic evaluations as core business, outsource the assessment (eg, CDD). ARCs collaborate with private psychiatrists. One ARC reports collaboration with a CDD, for a preliminary assessment to shorten waiting times and diagnostic process in the ARC. PGC collaborate by transferring children and collecting feedback on the outcome. Overall Organisations do not engage in shared diagnostic trajectories or shared responsibility.
Barriers for interorganisational collaboration
Structural barriers
Administrative/regulative barriers
Governmental regulations define different goals, working processes, staffing,. . . of organisations
PGC belong to the educational policy domain, ARC, CDD, CAR and MHC to the healthcare and welfare domain. Being regulated by different Ministers and administrations with different responsibilities and policy priorities, hampers collaboration.
‘We work in different sectors. This makes coordination of activities and collaboration between organisations, difficult’. (participant PGC)
Organisational goals
Organisational goals impact on the nature and purpose of the diagnostic assessment. PGC’s primary goal is to support pupils and diagnostic assessments are performed when extra scholarly support seems needed. Diagnostic assessments in a CAR aim at rehabilitation, while ARC specialises in diagnosing autism spectrum disorders. These differences imply that the content of a diagnostic assessment in one type of organisation, is not always considered adapted to the needs of another organisation, hampering the common use of an evaluation.
‘We have to do an assessment to make up rehabilitation goals. A report of a diagnostic trajectory in a CDD or another center, isn’t always useful for us’. (participant CAR)
Working processes
Participants of the CAR consider diagnostic evaluations in private settings not as a multidisciplinary neither as evidence-based which hampers collaboration.
‘We follow evidence-based protocols in our diagnostic work. This is a guarantee for quality of our work, in which we distinguish from private settings’. (participant CAR)
The CAR consider their practice as a more holistic approach compared to other providers.
‘We have the opportunity to include an evaluation of the context of the child in our diagnostic trajectory. That’s a more holistic approach of the child’. (participant CAR)
CDD need input from third parties to evaluate social-emotional components.
‘For a social-emotional evaluation, we often have to collaborate with the hospital service for paediatric psychiatry’ (participant CDD)
Regulations impact on the content of the assessment. Sometimes, specific tests are required for reimbursement of therapy or inclusion in a rehabilitation programme.
‘We need to perform certain tests for inclusion of the child in our rehabilitation program. If this wasn’t as regulated, perhaps we would do other tests’ (participant CAR)
Differences in out of pocket fees between providers of diagnostic evaluations
Out of pocket fees differ and high out of pocket fee in private settings, is reported as a particular barrier for collaboration.
‘Families with better financial capacities laugh with our waiting lists and go to private settings where they get an evaluation within 3 months, while other children have to wait 3 years for the same evaluation’. (participant CDD)
‘Families with financial problems don’t come to an ARC’ (participant ARC)
Regulations do not facilitate interorganisational collaboration
Regulations (and financing) focus on individual organisations and do not support interorganisational collaboration.
‘Our regulations and financing system is based on fee for service. We don’t have the time to invest time in collaboration’. (participant CAR)
Unequal regional distribution of organisations
The geographical distribution of facilities has developed historically and not in a planned programmatic way based on population needs in the area.
‘There is not enough CAR-capacity in Antwerp. In some regions, there are less organisations offering diagnostic evaluations, with a poor capacity’. (participant PGC)
In regions with less organisations, the longer distances are problematic for a vulnerable population.
‘For the most vulnerable group, collaboration with other organisations is not possible because of the physical distance between the settings’ (participant MHC)
Barriers related to funding
Differences in financing mechanisms of organisations
All participants mention the different funding mechanisms as an important barrier for structural collaboration. CAR and ARC are financed by item-of-service, 29 while CDD and MHC are funded per case, offering more flexibility in the organisation and content of the assessments.
Lack of funding impacting on capacity and accessibility
Participants of all focus groups mention diagnostic capacity shortages, resulting in long waiting periods but also in problematic collaboration. With child referrals, organisations are always confronted with a long waiting periods impacting on the continuity of the care trajectory.
‘Waiting lists are the main reason why there is no interorganisational collaboration’. (participant ARC)
Barriers related to clinical practices
GDPR
The General Data Protection Regulation (GDPR) hampers the sharing of information and test results of a child between organisations.
‘I had a meeting with the mum of a pupil and the physiotherapist of the CAR to discuss the results of the diagnostic assessment. I asked for the report, but the physiotherapist said I couldn’t have it. Then I asked the mother for the report, and she said yes, I could have a copy. The physiotherapist passed me over the report. Why does it have to be so difficult?’ (participant PGC)
Agency-related barriers
Interorganisational barriers
Different working processes
The content of diagnostics and the diagnostic test batteries differ between organisations. CDD assess according to the age of the child, the assignment reason and the working hypothesis. CAR uses sector specific evidence-based protocols. The ARC use age-adapted evidence-based protocols but rely more than CAR on the expert opinion of the evaluator.
‘We use standardized trajectories adapted to the age of the child and the information gathered in a first interview. The case manager, who is doing this first interview, decides if adjustments have to be done to the standard protocol or not’. (participant ARC)
PGC use diagnostic protocols developed by a PGC expert group .
‘We have our own methods and protocols . . .’ (participant PGC)
Different organisational practices, impact on collaboration .
‘We can perform some QI testings for other organisations, but only when it fits in our specific trajectory and goals’ (participants PGC)
Unclear mutual knowledge about organisations target group, expertise and working practices
Organisations have specialised and do not all address the broad spectrum of developmental disorders, while third parties have no knowledge what centres specialise in what developmental disorder. These ‘de facto’ specialisation shows in inclusion and exclusion criteria used by centres, which impact on waiting times and trajectories of children and is a key factor in communication with parents.
‘Sometimes parents are disappointed because referring doctors not always give them the right information about what PGC do and how they work, resulting in false expectations. Clear communication and giving the right information, is important in a collaboration’. (participant PGC)
Moreover, prejudices and poor knowledge on the management of the waiting lists by other organisations hampers interorganisational collaboration.
‘There are many prejudices about the waiting lists of the CDD. Referrers always suppose they are very long, but they are not familiar with the prioritization of specific age and target groups’. (participant CDD)
CDD & CAR participants mention organisations are not always well informed on their practice and activities.
‘Perhaps we don’t communicate enough about internal changes’ (participant CDD)
‘Little is known by referrers to which CAR they have to refer to. There are interorganisational differences between the CAR considering the specific target group they work with’. (participant CAR)
Organisational barriers
Communication: terminology and conceptual barriers
Clear communication and mutual adaptation reduce the risk of misunderstandings or unaddressed expectations.
‘The paediatric psychiatrist needs ‘this’ information and a CAR needs ‘other’ information. . . it is not always clear who needs which information, what makes collaboration difficult’. (participant PGC)
Clinical autonomy, distrust and quality of the assessment
The lack of trust in the quality or usefulness of diagnostic activities of other organisations hampers clinical continuity of care. Professionals and organisational teams tend to rely on ‘their’ diagnostic practices, not necessarily as an explicit value judgement about others, but to keep control of a diagnostic process by the ‘own’ group. PGC experience distrust, even a lack of respect by other (healthcare) organisations in their diagnostic work. This lack of mutual (clinical) trust reinforces the practice of ‘we will do it on our own’ hampering management continuity of diagnostic evaluations between organisations.
‘Collaboration is not always a possibility. I had contact with a private centre lead by a psychiatrist, and they clearly communicate they don’t accept test assessments done by other organisations’. (participant PGC)
Trust is mainly determined by hands-on professionals’ collaboration experience.
‘Collaboration depends on individuals, not on organisations’. (participant ARC)
There are concerns about and distrust in the quality of diagnostics in private settings, mainly the multidisciplinary character or ‘integral’ assessment of the child. Especially private settings are not (considered as) interdisciplinary, or (if any) the composition of the multidisciplinary team is questioned as well as the quality of the diagnostic process.
‘There are diagnostic settings with which we won’t collaborate because of the lack of quality and the distrust in those centres’. (participant PGC)
Asymmetry
The differences in expertise and knowledge between types of diagnostic centres, sometimes induce doubt and a lower perceived value. 34 Collaborators of the PGC remark about their collaboration with an ARC ‘Who am I? They are the experts, though?’ (participant PGC GO!), and ‘collaborators sometimes experience a threshold in contact considering diagnostic activities with other organisations’ (participant PGC).
This mechanism plays on a personal as well as organisational level.
‘On behalf of diagnostic evaluations, PGC has a bad image’. (participant PGC)
Barriers related to service delivery
Communication
False (eg, ‘ask the PGC to do the IQ, over there it’s for free’), unclear (eg, diagnostic reports to be translated to plain language for parents) or loss of information and poor communication (eg, lack of feedback after referral) hamper interorganisational collaboration.
‘When we refer for a diagnostic evaluation, we sometimes get feedback on the outcome, sometimes we don’t. Or we only receive a written report. But that’s not always feedback corresponding with the diagnostic questions we referred for’. (participant PGC)
‘There is always a loss of client-related information when we collaborate with other organisations’. (participant CDD)
Barriers related to clinical practices
Communication: the use of transferable child-related information and results of test and observations
Diagnostic information sharing barriers are both a logistic question (shared client files, informatics. . .) as well as a content and ‘reporting culture’ matter.
Regarding content there are differences in reporting diagnostic information or information shared in an anamnestic or other interviews. Little attention is currently paid on the different organisational needs.
‘PGC only do diagnostic activities related to learning problems. CAR and we perform other diagnostic activities. We should almost develop a tool in which the used concepts and the applied diagnostic trajectories are explained for other organisations’ (participant MHC)
Suggestions for better coordination and interorganisational collaboration
Participants formulated suggestions to improve interorganisational collaboration (Table 3).
Suggestions for improving interorganisational collaboration.

Structural measures
Administrative/regulative
Include interorganisational collaboration as a mission in the governmental regulations of organisations
Governmental regulations should include interorganisational collaboration as a responsibility of all organisations offering diagnostic evaluations which facilitate the use of resources and taking responsibilities for coordination and collaboration with other players in the field.
‘The MHC are the only type of organisations that can collaborate with other organisations in current regulative frame. CAR can’t. Regulations must change and make it possible’. (participant MHC)
More adapted regional distribution of organisations and capacity
Interorganisational collaboration depends on availability and capacity in the region. Changes in regional distribution are mentioned as a step-up to more collaboration.
‘We certainly may not forget the regional spread of subsidized organisations. An equal spread in function of availability, but also on behalf of specializations’. (participant PGC)
Suggestions related to funding
Besides regulations, funding or allocation of resources for time and activities spend on interorganisational collaboration is proposed
Interorganisational collaboration requires time for coordination, meetings and more mobility of collaborators. This investment of time needs to be financed.
‘Interorganisational collaborations impacts on the management of organisations. Financing has to be foreseen for time and transport to other regions’. (participant ARC)
Inter-organisational suggestions
A common approach of reporting standards for sharing diagnostic information.
When a child is referred, it should be possible to transfer diagnostic information between organisations, and to continue the diagnostic process started by a previous organisation that meets quality standards shared by all.
‘Some agreements on methods and reporting standards of diagnostic evaluations is needed when more interorganisational collaboration should be implemented’. (participant ARC)
Organisational suggestions
Conceptualising a shared, interorganisational vision on diagnostic evaluations and a shared quality framework
To collaborate, a shared vision on diagnostic evaluations is needed.
‘The meaning and significance of diagnostic evaluations should be enlarged and not mainly be restricted to the search for a diagnosis. A shared vision is needed in society and in all diagnostic offering organisations’ (participant MHC)
Additionally, a quality framework for diagnostic evaluations has to be developed and respected by all providers. This will promote mutual respect for the delivered evaluations.
‘Specific specialized expertise and diagnostic activities performed by different types of organisations can be equally evaluated under the condition of working within a shared quality framework’. (participant CAR)
Agency-driven measures
Suggestions related to the inter-organisational domain
Sharing knowledge and developing trust in organisations’ diagnostic expertise
Knowing, recognising and developing trust in each other’s expertise, and recognising the limitations of expertise in their organisation is an important stepping stone for collaboration.
‘Mutual knowledge on expertise and organisational goals is needed for more collaboration’. (participant CAR)
Suggestions related to the organisational domain
Sharing expertise and knowledge in practice
Sharing expertise, competences and knowledge between organisations or professionals by coaching, teaching or formulae of outreaching, to broaden the competences and knowledge in less specialised organisations, is reported as an option to improve interorganisational collaboration.
‘It would help to get additional expertise of specialized collaborators of other centres, so we are also interested in more collaboration’. (participant PGC)
Suggestions related to service delivery
Make ‘practical’ arrangements to enhance collaboration between organisations: e;g. using the first date of assignment of an organisation when referring to avoid double waiting periods, or instal interorganisational team meetings, . . ..
‘We collaborate with a CAR and have the agreement that, in case of mutual referral, the assignment date is taken over. By this agreement, we avoid children have to restart the waiting period when referred’. (MHC participant)
Adapt collaboration to different stages of the trajectory and development of the child.
Interorganisational collaboration is currently mainly limited to referral when specific expertise and competences are lacking in the organisation in charge. Participants plead for an interorganisational collaborative model taking into account (1) the phase in the child’s care trajectory and the goal(s) of the diagnostics and (2) the complexity of the diagnostic needs consulting the adequate level of knowledge and expertise available in different types of organisations.
‘The current organisational model emphasizes highly specialized diagnostic centres, with the consequence that the expertise of less specialised organisations is not used. But sometimes high expertise isn’t needed, developmental problems aren’t always as complex’. (participant ARC)
A more institutionalised model of collaboration identifying the potential role and requested expertise of different types of organisations in different stages of the care trajectory is needed.
‘We need some good agreements on organisations’ responsibilities’ (participant MHC)
Discussion
This research engaged in a dialogue with representatives of different public organisations in Flanders providing diagnostic evaluations for developmental disorders using focus groups. The results learn that currently interorganisational collaboration is mainly informal, ad hoc, on a personal level and is in general limited to referral. Government regulations do not facilitate interorganisational collaboration resulting in an inefficient use of the overall diagnostic capacity. Thinking in terms of trajectories and a system approach for collaboration, using the logic of stepped care and patient centred care15,18,30,31 is considered by the participants as a means to support a public health approach improving accessibility of diagnostic evaluations of developmental disorders.
Stepped Care is a conceptual approach of delivering and monitoring treatment and care so that the most effective, yet least resource intensive treatment is delivered first, only ‘stepping up’ to intensive/specialist services as required and depending on the level of patients’ needs. The most effective yet non resource-intensive care or treatment is delivered adapted to the needs of the client, also aiming at guaranteeing early and better access to health systems. 30 Patient centred puts forward the needs of the patient in different stages of a trajectory as a key starting point. It implies that there is no ‘linearity’ (eg, from low level to high level) in the use of the different levels of specialisation30,32 Moreover, different levels of specialisation of diagnostic evaluations can be provided by different types of organisations in different phases of the trajectory adapted to the needs in that phase or event.18,33 In order to organise work processes according to these principles, collaboration and integration of service providers within and between sectors or domains is needed to enhance continuity of care 34 and integrate health services.14,18,30 Integrated care is a patient-centred approach and requires a multilevel approach in the field of diagnostic evaluations of developmental disorders. At the micro level it focusses on inter-professional (or interdisciplinary) collaboration and participation of patients and informal care along the trajectory of a child. The meso level considers on how collective action and shared responsibility of organisations can be realised to meet the needs of a population across the care continuum. At the macro level the integration of policies and regulations of different policy domains is needed.14,19,20 The focus groups indicate that there is a consensus that developing collaborative networks14-17 across organisational and disciplinary boundaries 18 is the way to move forward. But multiple factors, such as external environment, organisational characteristics, people characteristics, instruments of interorganisational collaboration and relational factors 21 need to be considered.
A conceptual model for system design
Based on these findings we propose a conceptual system design model that could be used as a frame of reference for the future design of de diagnostic field in Flanders. The model focusses on expertise and diagnostic activities rather than on ‘types’ of organisations. Different levels of specialisation can be provided by different types of organisations,18,33 but the type of activity needs not to be limited to one type or organisation. The model addresses the question which expertise and knowledge is available where (in what region) and which diagnostic activities can be taken up by who? Diagnostic activities vary from low to high intensive and specialised and the system design question is to ensure that people can access the appropriate level of diagnostic expertise adapted to their needs along their trajectory. Collaboration and integration within and between organisations and sectors is needed to enhance continuity of care 34 and increase the efficiency of the available diagnostic service capacity.
The conceptual programme of activities model (Figure 1) differentiates 3 expertise levels: level 1 provides specialised diagnostic evaluations and coordinates the diagnostic trajectory of the child, level 2 providing highly specialised diagnostic evaluations and level 3 is the level of dedicated expertise for particular developmental disorder categories.
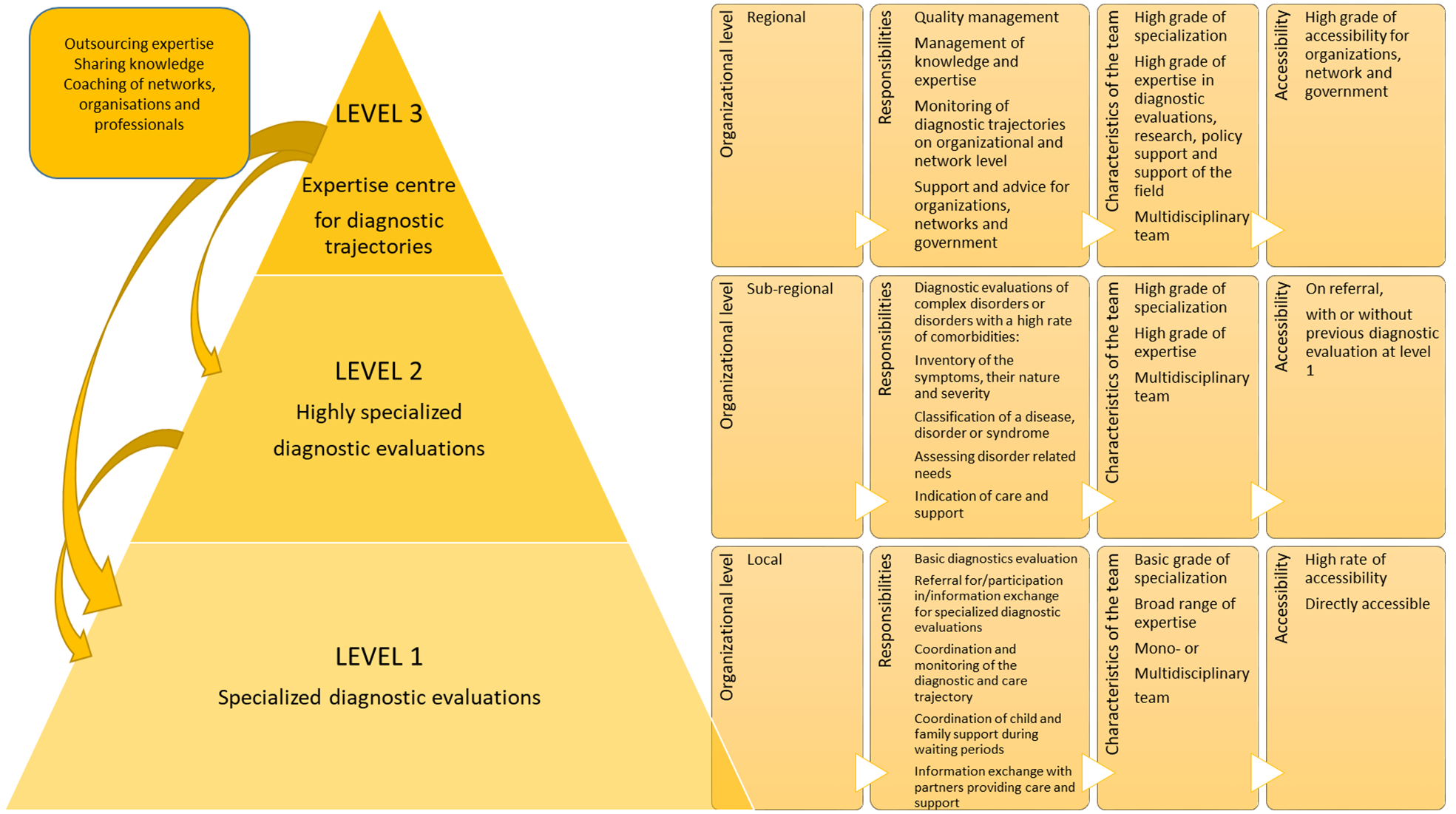
A stepped care model for diagnostic evaluations for children with a suspected developmental delay or disorder.
Developmental disorders vary in severity and complexity with major impact on developing a diagnosis.3,4 A general, overall evaluation of the functioning of the child can be done on level 1. Professionals and teams at this level need knowledge and expertise in the broad range of DD and evaluations are performed by an interdisciplinary team.12,35,36 Only exceptionally monodisciplinary processes, for example, as a follow-up of an earlier interdisciplinary evaluation, for example, to confirm or reject a suspected disorder can be accepted. Level 1 is locally organised, easily accessible (nearby and accessible without referral), offers less resource-intensive diagnostic activities and coordinates the entire trajectory (eg, by means of case management). 12
Diagnostic evaluations of complex, comorbid disorders or differential diagnosis between similar and complex disorders, requires teams of highly specialised professionals in specific domains. On level 2, more specialised, less frequently needed more resource-intensive diagnostic activities are organised on a larger (subregional) area particularly for these groups.
On a third level, a regional dedicated expertise centre for diagnostic trajectories is organised. The mission of this centre is to optimise the quality of the diagnostic trajectories and activities within and across organisations and networks, to support the sharing of expertise and knowledge, to monitor diagnostic activities and networks in order to support policy and network management.
We also stress the fact that collaboration and network implementation are not mere a ‘technical’ design question but will require an understanding of institutional logics37,38 and personal factors as authority, legitimacy, expertise, relational network, reputation. Governance will be necessary.13,39 A culture and attitude of shared responsibilities in diagnostic trajectories will be needed including clarity in roles, mutual understanding, trust, sharing knowledge and expertise, access to tailored information, and efficient care trajectories along different organisations.40,41
To meet population needs and a patient centred approach, a programmatic regional distribution of diagnostic activities for all ages and pathology groups, is needed.
We are aware that the model is a mere theoretical reflection: Implementation research concerning the model grounded in a realist evaluation perspective, 42 addressing effects on accessibility, cost effectiveness and the impact of policy regulation and processes of (inter)organisational collaboration will be needed.
Methodological limitations
This contribution has some methodological limitations. APP and private providers are not represented in this study, while they could have given additional insights on barriers and facilitators in paediatric psychiatric services on the one hand and on the other hand the non-subsidised diagnostic evaluations by private practices. Neither did this research include the experiences of children/parents or authorities. The visions and experiences of parents and children along care trajectory 43 would shed additional light on their needs. Collecting data on the public authorities’ opinion on current organisation of the field and accessibility, will improve the understanding of the ‘macro’ perspective.44,45
There is a possible selection bias in the focus groups as participants were selected by the organisations and focus groups were in some cases for practical reasons organised as a follow-up of other meetings, affecting the participants. This could affect the representation of ideas on collaboration as for example, clinicians could have another focus or perspectives compared to managers of staff members.
Conclusion
Children with a developmental disorder need accessible and timely diagnostic evaluations along their care trajectory to get the most optimal care and support. The field of subsidised multidisciplinary settings offering diagnostic evaluations in Flanders, Belgium, currently lacks well-thought interorganisational and intersectoral collaboration. An integrated, collaborative stepped care organisational network model, considering the diagnostic needs along diagnostic trajectories of the children has been suggested as an output of this study. To optimise the organisational model, further research on governance, institutional logics, culture and attitude of the diagnostic field, is needed. To maximise a successful implementation of the model, piloting and permanent monitoring and evaluation of evolving processes, dynamics, results and impact on diagnostic trajectories, is recommended.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was commissioned by the Flemish Authorities, to provide knowledge supporting a reorganisation of the diagnostic field.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Eva Cloet is the main author, Anna Jansen reviewed the article, Mark Leys contributed to the design of the work, the interpretation of data and reviewed the article.
Ethical Approval Statement
Ethical approval was not required for this study.
Participant Consent Statement
Informed consent to the research and to publication of the results was given by the participants at the beginning of the focus groups and have been audiotaped.