
Abstract
Objectives
To develop a model to support health systems in clarifying how they might target action to reduce health inequalities, and to use it to understand current policy on health inequalities in England.
Methods
We used the wider literature on the definitions of health inequalities to draw together a schematic model which attempts to link together the different conceptualisations of health inequalities present in the literature with potential sites of action that could be taken by local health systems. We then undertook a document analysis of the policy documents and programmes underlying the recent reorganisation of the NHS in England.
Results
The need to tackle health inequalities is cited as one of the main rationales underlying the changes. However, there is a lack of clarity within the documents around: the type of inequality being addressed; the identification of the group(s) suffering from inequalities; and the ways in which the assumed ameliorative mechanisms will work in practice. The documents place considerable emphasis on the assumption that closer partnership working will address inequalities, although the mechanisms by which this will be achieved are not specified and previous research demonstrates how difficult this can be.
Conclusions
The aspiration to tackle health inequalities through newly constituted Integrated Care Systems and Boards is welcome. However, it is well known that the contribution that health care services can make to addressing inequalities is relatively limited. Greater clarity is required of policy and local strategy if efforts are to be appropriately targeted.
Introduction
Inequalities in health status and outcomes are not new, but the Covid 19 pandemic provided stark evidence of their impact and importance. 1 In the UK, governments have sought to reduce health inequalities for decades. For example, Health Action Zones targeted resources and support at areas identified as suffering poor health. 2 Judgements as to their value were mixed, 3 and the subsequent Marmot report advocated a shift away from such targeting to what was called ‘proportionate universalism’ – ‘actions must be universal, but with a scale and intensity that is proportionate to the level of disadvantage.’ 4 The Health and Social Care Act of 2012 gave newly created Clinical Commissioning Groups (CCGs) a statutory responsibility to address health inequalities. Research found that whilst this duty was taken seriously by CCGs, little was achieved, in part because of a lack of shared understanding of what was meant by ‘health inequalities’. 5 The 2022 Health and Care Act established Integrated Care Systems (ICSs) and gave each Integrated Care Board (ICB, the statutory body) a similar duty.
If ICBs are to fulfil this duty, it is important that we interrogate what it is that they are being expected to do. The contribution that health services can make to reducing health inequalities is relatively limited compared to the potential impact of concerted, national-level action to reduce income inequalities and tackle the social determinants of health,6,7 with research suggesting that the most cost effective approaches would focus upon programmes to tackle unemployment, income inequalities and early childhood interventions, alongside traditional public health approaches such as improving physical environments and using regulation and price to tackle risky behaviours. Clearly, most of these actions are not within the gift of ICBs.
In understanding how ICBs might meet their statutory obligations, national policy and guidance are relevant because they set the parameters within which action may be taken and determine the potential monitoring regime. We examine the policy documents under which ICBs were established to explore what the policy targets are and what mechanisms are expected to be activated to address those targets.
To make sense of these documents we developed a simplified model to classify potential targets for health service action (Figure 1), teasing out the multiple definitions of health inequalities used and showing relevant linkages. Our contribution is twofold. Firstly, for ICBs and policy makers in England we provide some clarity in a confused topic area,
8
highlighting potentially problematic implicit assumptions in current policy and drawing attention to areas in which health service action may have an impact. More widely, we believe that our simplified model may be of value to other health systems seeking to address health inequalities, allowing structured conversations about who can do what, and which types of outcomes might change. Our model is not intended as a contribution to the literature on the wider social determinants of health and the ‘fundamental causes’ underlying them
9
; rather it is an attempt to support the rapid appreciation by health system leaders of how and where they can and should act. Model linking potential causes and definitions of inequalities amenable to NHS action, highlighting sites at which inequalities may become visible or measurable.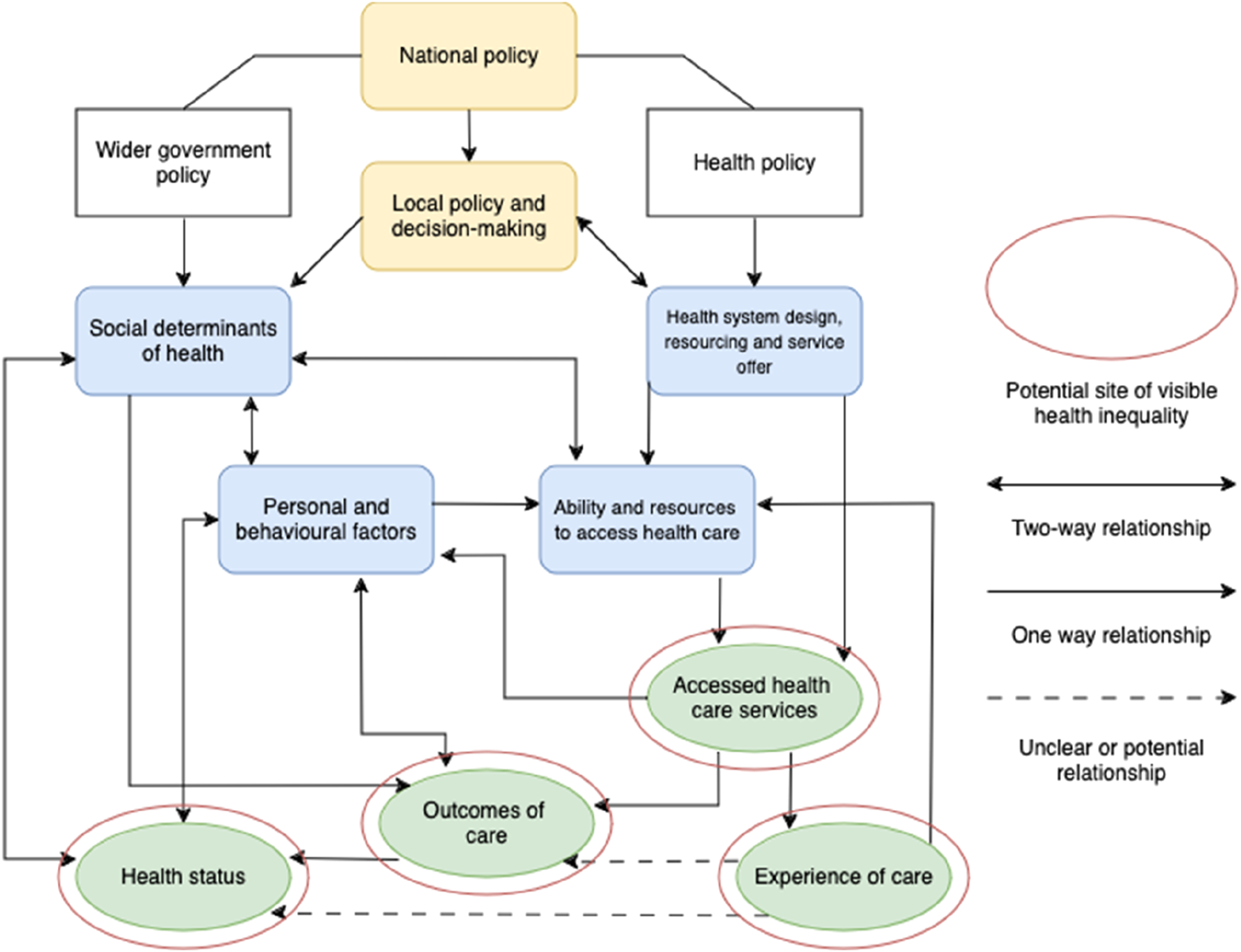
Addressing health inequalities in England: current structures and policy
The Health and Care Act 2022 introduced a new health system in England. Around 200 CCGs (responsible for commissioning health care services for a given population) were replaced by 42 Integrated Care Systems (ICSs).10,11 It was argued that modern health care requires a more integrated approach, with emphasis placed upon the need for health care commissioners and providers to work collaboratively together and with other sectors including social care providers, Local Authorities and the voluntary sector. ICSs have both an Integrated Care Board (ICB), which has statutory responsibility for arranging the provision of health services for their population, and an Integrated Care Partnership (ICP), which is a wider body bringing NHS providers and commissioners together with Local Authorities and other organisations serving the population. ICB and ICP membership is locally determined, but the ICB is the statutory body and must include representatives of local commissioners and all providers. The ICP sets the overall local strategy, working across sector boundaries. The ICB must commission services to meet the strategic needs identified and importantly for this paper, were given a statutory duty to address health inequalities.
Inequalities –definitions and perspectives
The term ‘health inequalities’ can be defined in a variety of different ways.
McCartney et al
8
review a wide range of literature and suggest the following definition: Health inequalities are the systematic, avoidable and unfair differences in health outcomes that can be observed between populations, between social groups within the same population or as a gradient across a population ranked by social position.
This definition highlights the unfairness inherent in inequalities (some differences between populations are not unfair) and the fact that they must be potentially avoidable. However, its breadth means that it is not necessarily helpful to those required to undertake immediate practical steps to mitigate inequalities. For example, relevant ‘health outcomes’ may include: health status; life expectancy; healthy life expectancy; likelihood of developing particular illnesses; access to care; experience of care; or outcomes of care (for example see:12–14). These different important and relevant outcomes and associated varying measurement approaches will identify different populations as suffering disadvantage; all are clearly valid, and there will be overlaps, but action will look different depending upon the definition and disadvantaged group chosen.
In terms of the underlying causes of inequalities, the role of social factors in determining health outcomes is universally accepted. 15 Fundamental cause theory 9 posits that persistence of the gradient in outcomes across socioeconomic groups over time and in a wide variety of places indicates underlying mechanisms acting to maintain it. Unequal access to flexible resources drives inequalities, and therefore ameliorative action must address the fundamental underlying societal conditions driving this. From this perspective, those providing health services have a more limited role to play, as the theory suggests that whatever changes are made to service provision, those with access to flexible resources will benefit most. However, the theory also identifies mechanisms such as stigma and racism as driving unequal access to appropriate services, suggesting some mechanisms by which health services may contribute. Marmot and Allen 6 consider this potential role, highlighting a range of estimates of the proportion of inequalities amenable to health care service action from 15% to 45%, and identifying the configuration of the health system and extent of universal coverage as driving factors in the variation seen. In the UK, a free NHS provides for universal access, but research nevertheless identifies significant problems in accessing services for some members of society. 16
Finally, tackling identified inequalities requires a comparison group. In identifying such groups, area-based measures of deprivation are often used, such as the Index of Multiple Deprivation. 17 However, research has demonstrated that such measures miss significant numbers of people suffering from deprivation, 18 especially if the geography chosen is too large or too heterogenous. Moreover, many deprivation measures include health in their calculation, raising potential issues of endogeneity bias, although research suggests this may not be a significant problem. 19
Against this background, supporting ICBs to develop concrete programmes of work to fulfil their statutory duty around health inequalities looks daunting. With limited resources and an NHS working at full capacity, the time and effort to devise such programmes may be in short supply, and it could be argued that a more cost-effective approach would be to focus upon larger scale societal change. 7 However, as ICBs now have a statutory duty in this area, we would argue that the implicit and explicit assumptions around the role of the NHS in tackling inequalities embedded in policy design and guidance should be interrogated. What the NHS can do is, in part, conditioned by how it is organised and managed, and it is therefore worthwhile to explore how those responsible for the NHS reorganisation envisaged the duty to tackle health inequalities being enacted and supported by the changes made under the Health and Care Act 2022. This paper therefore analyses the foundational policy documents and associated guidance issued as ICBs were set up to explore what it was assumed ICBs might do to meet their statutory duty, and offers a model which tries to make sense of different potential approaches which may be of value to policy makers and health system actors required to develop programmes of work in this area.
We begin with a short description of our proposed model followed by an explanation of how we approached our policy analysis. We then set out the range of potential targets and associated mechanisms identified in the documents. Our discussion considers the implications of our findings.
A model for understanding potential targets for health system action in tackling health inequalities
Our initial reading of the relevant policy documents generated multiple concepts, potential mechanisms and policy aspirations. To make sense of these we developed a heuristic model (Figure 1) identifying the potential targets of action by ICBs to reduce health inequalities. The model builds upon definitions of inequalities in the literature, focusing on those where health care services might be expected to have a role, and includes areas addressed in policy documents. It is not intended as a more general model of inequalities, nor to rival models such as that of Diderichsen et al 20 in identifying populations with differing vulnerabilities or susceptibilities to disease. Rather it is intended for use alongside such models to support systems and policy makers in identifying and classifying which causes and consequences of inequalities particular policies might address. We recognise that our inclusion of the complex web of social determinants of health in a single box without further analysis may seem reductive. However, for our purposes, the social determinants of health are factors largely outwith the ability of health care services to effect change, and they are therefore not the focus of the model.
Methods
Policy sources analysed for this study.
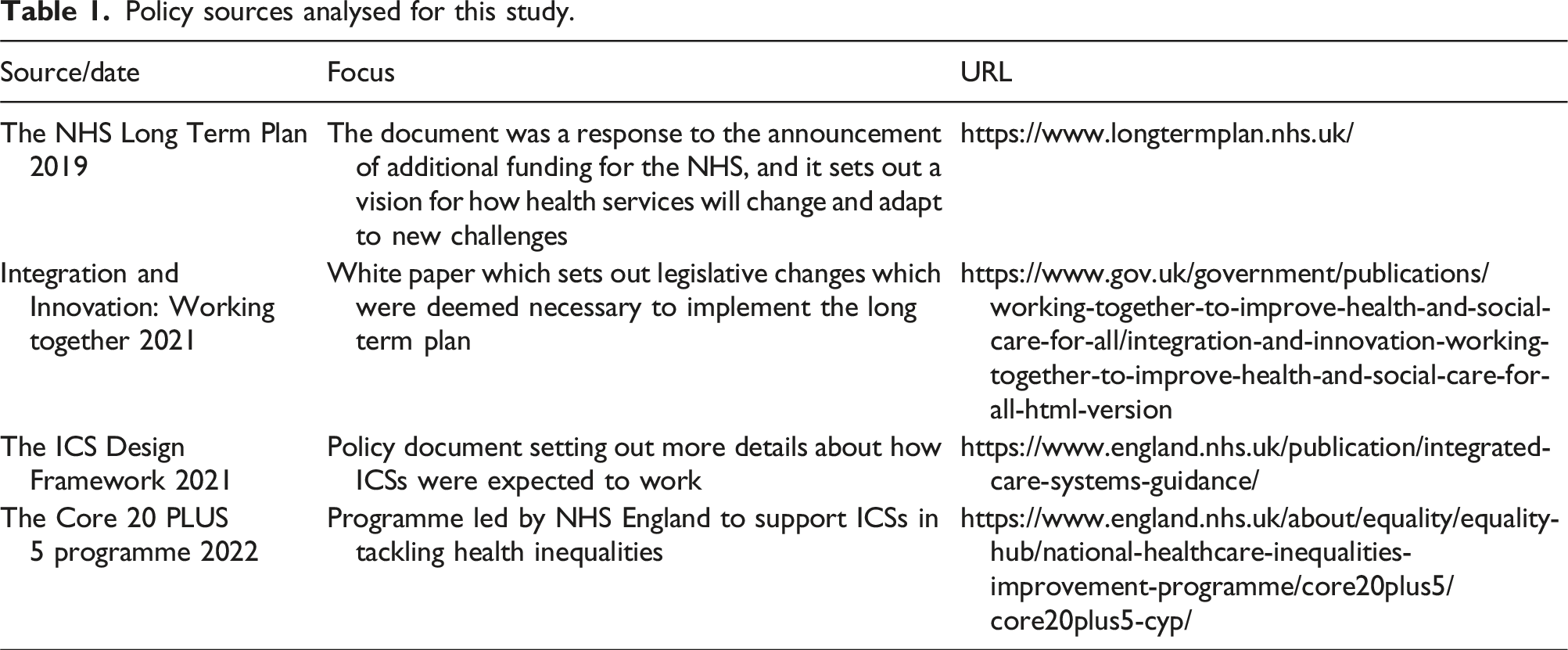
We followed a programme theory approach to analysis. 21 This involves interrogating policy document content to tease out the explicit and implicit assumptions around the mechanisms by which policy changes will drive the desired outcomes. We focused upon how the structural and process changes creating ICBs were assumed or intended to tackle health inequalities. This exercise may be a little unfair to policy makers, as the changes embodied in the Act are far reaching and designed to do many things alongside tackling health inequalities. Nevertheless, given the statutory focus on health inequalities (not all responsibilities were given a statutory footing), and the fact that the documents highlight health inequalities as a driver of the changes, we argue that this is a legitimate and relevant analytical exercise.
Initial reading, independently, of each document by two of the research team was followed by the extraction of all references to tackling health inequalities. Each of these was then considered against our schematic representation of the different concepts associated with ‘health inequalities’. We first identified the conceptualisation of health inequalities that the policy was intending to address, although this was often not explicitly articulated. We then sought to identify the ‘programme theories’ 21 which underpin the claims about how the new system will address inequalities. These represent the implicit logics within the policy, including the underlying assumptions as to how the policy prescription (the establishment and design of ICBs) will meet the required policy goals (reducing health inequalities). Two team members undertook this process independently, and discussed and adjusted potential programme theories until a consensus was reached for each document. For example, the initial guidance on the establishment of ICBs 10 states: ‘The purpose of provider collaboratives is to better enable their members to work together to continuously improve quality, efficiency and outcomes, including proactively addressing unwarranted variation and inequalities in access and experience across different providers.’ (p. 31) This statement was assessed as addressing inequalities in access and experience, and to embody an implicit logic that collaboration between NHS organisations would support action to target services at those currently not receiving care and improve patient experiences. As this example shows, for many such statements, the assumed mechanisms lack specific detail. The two team members were from different backgrounds, with one a clinician with many years’ experience as a GP, and the other a health services researcher with previous experience of researching health inequalities. These different perspectives ensured richness in the analysis, and collaborative discussion of each identified programme theory ensured that this was captured in the final description of each one.
Results
In each of the documents analysed, ‘tackling health inequalities’ appears as one of the core purposes of the changes. For example, the NHS Long Term Plan contains 39 references to reducing inequalities, with every chapter containing references to how proposals will achieve this aim. The White Paper, Integration and Innovation suggests that the legislative changes proposed are necessary because: ‘we need the right legislative framework to support the recovery [from Covid 19] by improving outcomes, reducing health inequalities and making best use of limited resources’ 22 , p. 12. Similarly, the ICS Design Framework positions reducing inequalities as the second of four priorities for ICSs, and argues: Integrated Care Systems (ICSs) will play a critical role in aligning action between partners to achieve their shared purpose: to improve outcomes and tackle inequalities, to enhance productivity and make best use of resources and to strengthen local communities 10 (p. 2.). Thus, each document suggests that health inequalities form part of the fundamental justification for the changes being made. It is therefore important to clarify exactly how this is expected to be achieved.
NHS Long Term Plan (2019)
The NHS Long Term Plan 23 set the agenda for the NHS for the next decade and focused upon the need for greater collaboration. The Plan finished with a set of legislative proposals which were eventually developed into the Health and Care Act 2022. The Plan focuses upon the triple aim of: ‘promote better health for everyone, better care for all patients and sustainability for the NHS system and for the wider NHS’. The Plan references ‘inequalities’ and the need to reduce them without necessarily defining the term. It is implied that inequalities in health status are the main target, but also references access to services and outcomes. This latter is again undefined. The Plan thus implies multiple definitions of inequalities.
In terms of inequalities in health status, the Plan focuses upon prevention of specific diseases, suggesting a more preventative model of healthcare would reduce inequalities. Box 1 sets out how the Plan envisages this working in practice.
Problem conceptualisation 1: People in deprived areas have higher incidences of a variety of degenerative diseases, leading to inequalities in health status
Logic (how the problem is understood): • People in deprived areas are more likely to suffer from ischaemic heart disease, chronic obstructive pulmonary disease, liver disease, diabetes etc. • Prevention of these diseases will reduce inequalities Mechanism: • Key programmes of work to be rolled out: • Smoking cessation • Weight management • Alcohol and drug treatment • Hypertension screening and management • Diabetes programme
This approach to reducing inequalities requires that the programmes of work listed are specifically targeted to those particular population groups most in need. How this might be achieved in practice is not addressed.
The Plan also addresses inequalities in access to services.
Problem conceptualisation 2: There are inequalities in access to health care services
Logic: • People in deprived areas do not access services at the same rate as people in more affluent areas. Mechanism: • Target funding at areas of maximum need by adjusting funding formulae to account for need, specifically focussing on inequalities in access and outcomes.
The Plan sets out an aspiration that the allocation of core funding should include greater weighting for health inequalities and unmet need, although these are not defined, and no details are provided as to which dimensions of need should be included. The dimensions included in the formula will shape which areas receive additional funding, and the size of the geographies over which need is measured will affect which areas are prioritised.
In terms of which group is being compared with others, the Long Term Plan singles out ‘inclusion groups’, which includes: people who experience homelessness, people with drug and alcohol dependence, vulnerable migrants and refugees.
Problem conceptualisation 3: Specific groups in society are disadvantaged compared with others
Logic: • Inclusion groups collectively suffer inequalities compared with the general population • These often include various minorities, such as people experiencing homelessness and those with learning disabilities. Mechanism: • Services should be designed specifically for and targeted at inclusion groups
This approach requires a clear rationale as to which groups should be targeted in any particular area. As highlighted by MacMahon 24 individuals can play a significant role in raising the profile of particular groups, and such targeting must be defensible. The Long Term Plan does not explicitly state how system changes will facilitate this.
White Paper Integration and Innovation: working together to improve health and social care for all (2021)
The White Paper ‘Integration and Innovation’ set out the legislative proposals which became the Health and Care Act 2022. The document emphasises the importance of a partnership approach in tackling health inequalities, highlighting the role of ICBs in working together with local organisations. The type of inequalities being targeted is not defined; rather, the document suggests that the development of ICBs will create the conditions within which the wider determinants of health inequalities will be addressed.
Problem conceptualisation 1: Social determinants of
health are the root causes of health inequalities
Logic: • Health inequalities are driven by the social determinants of health and deprivation Mechanism: • Creating ICBs and ICPs will support better integration between health services and local authorities • The resulting partnership working will enable activity to tackle the social determinants of health and therefore reduce inequalities
No detailed explanation of how this will be achieved is provided, beyond an aspiration that working more closely together will allow action to tackle the social determinants of health.
ICS Design Dramework (2021)
The ICS Design Framework provided advice and guidance about how Integrated Care Systems would operate. The document emphasises the statutory role of ICBs in addressing health inequalities. There are five main conceptualisations of problems related to health inequalities in the document, some reflecting the ideas introduced in earlier policy documents, whilst others use a different lens.
Problem conceptualisation 1: People in deprived areas are not receiving the care that they need
Logic: • The people who need it most are not getting the care that they need Mechanism: • Adjust funding for need • Develop strong partnerships which will facilitate transfer of resources
This suggests that health inequalities are about inequalities in access to care. This approach requires clarity as to how need is being quantified and measured, as different measures will identify different populations. The extent to which resources can be transferred will depend upon local relationships and trust as well as formal mechanisms to move funding between organisations and/or sectors.
The ICS Framework introduces the concept of ‘place’ (most commonly historical CCG footprints) and place-based partnerships. These are described as local NHS organisations working with other partners to co-ordinate planning to address the wider determinants of health. The Design Framework emphasises the importance of this in tackling health inequalities:
Problem conceptualisation 2: Inequalities are driven by the wider determinants of health
Logic: • Multiple forms of deprivation drive inequalities in health outcomes Mechanism: • Strong place-level partnerships will enable action to tackle the wider determinants of health. • These local partnerships will be able to feed intelligence up to the ICS to support them to tackle inequalities.
This approach focuses upon the social determinants of inequalities rather than defining a particular type of inequality. It is argued that tackling the causes of deprivation will reduce all types of inequalities, and the documents suggests that ICBs have a role to play in this. However, the mechanism by which place-level partnerships will be able to act remains unspecified, and previous approaches to partnership working to reduce inequalities have shown that this can be difficult. 25 Beyond partnerships, the Framework emphasises the importance of local data about health needs to underpin action, with a focus on local areas providing relevant data to their ICB.
The Framework also introduces the idea of Provider Collaboratives. These are collaborations between large scale providers to improve care. Provider Collaboratives are also said to have a role in reducing inequalities. In this case, the focus is upon inequalities in access to and experience of services.
Problem conceptualisation 3: Access to services is unequal
Logic: • Health inequalities are driven by unequal access to services Mechanism: • Provider Collaboratives will be able to work together and thereby tackle unwarranted variations in access • Provider Collaboratives will improve patient experience, and this will tackle variations in patient experience • The collection of good data across Provider Collaboratives will allow them to target disadvantaged population groups • Provider Collaboratives will be able to work together and use the feedback they get from patients to level up patient experience
This suggested mechanism raises a number of questions. Firstly, it is not clear if an overall increase in access is envisaged (and therefore increase in hospital activity) or whether the intention is to reduce access for some groups. Secondly, it is not clear how this duty will interact with individual Trusts’ financial obligations.
The Framework also discusses the role of Primary Care Networks (PCNs) as a vehicle for reducing inequalities. The type of inequalities to be addressed is not defined, although the focus on service responsiveness suggests that the target may be access to services. Two mechanisms are mentioned: the ability of PCNs to feed their knowledge of local populations to the ICB; and direct incentivisation.
Problem conceptualisation 4: A lack of intelligence about local need makes tackling health inequalities more challenging.
Logic: • Inequalities arise because services are not responsive to the needs of particular populations Mechanism: • Primary Care Networks will be able to feed intelligence up to ICSs about local population health need
This approach assumes that PCNs are aware of the need in their area, and it assumes that ICBs will have mechanisms in place to gather such intelligence.
Problem conceptualisation 5: Inequalities exist in delivery of primary care services
Logic: • Primary care services, like all services, have not been responsive enough to need • If local inequalities are tackled this will scale up to ensure inequalities are tackled throughout the ICS population Mechanism: • Directly incentivise action to tackle local inequalities through the Primary Care Network contract
The direct incentivisation of PCN activity does not define the type of inequality to be addressed; rather, PCNs are required to identify target groups and programmes of work. Recent research has found that, whilst PCNs understood the importance of this issue, they found undertaking the work quite daunting, and schemes of work developed under the policy tended to be small scale and short lived. 26
In summary, the guidance for establishing ICBs frames health inequalities as an important issue, and sets out multiple ways in which the new NHS structures will facilitate action. However, health inequalities are often poorly defined, and the mechanisms by which health inequalities are to be addressed remain imprecise and open to a number of challenges. Overall, the document places heavy emphasis on the importance of partnership working as a mechanism to reduce inequalities, although evidence that this is feasible is lacking and is reliant upon trust and robust mechanisms for working together.
Core20PLUS5-an approach to reducing health inequalities (2021)
The Core20PLUS5 is an approach to tackling health inequalities developed and introduced by NHS England’s Health Inequalities Improvement Team. The Core20PLUS5 website suggests that this is an approach to prioritising action to tackle ‘healthcare inequalities’. This is usually taken to mean inequalities which can be addressed via changes in health care services. However, the section of the website which defines the term ‘healthcare inequalities’ actually refers to health inequalities more widely, including the social determinants of health. Within pages referring to potential action, reference is made to inequalities in access, experience of services and outcomes, but outcomes in this case are not specifically defined, and could mean health status outcomes or treatment outcomes.
The programme is intended to be used by ICBs to identify the groups to be targeted in pursuit of reducing healthcare inequalities. It does this by identifying three specific groups: the Core 20; ‘plus’ groups; and five clinically defined groups.
The Core 20 focuses upon deprivation, with ICBs required to identify their 20% most deprived population using the Index of Multiple Deprivation. This index measures poverty across key components such as income, housing and education. ICBs are encouraged to identify this population and devise programmes to reduce inequalities, but the type of inequalities to be targeted are not defined. As discussed earlier, the size of geographical area used to define this population will be important: if too large an area is chosen, those living in pockets of deprivation in more affluent areas will be missed, whilst too small an area makes it difficult to design appropriate service change programmes.
The PLUS aspect of the model encourages ICBs to identify specific local population groups experiencing poorer than average access to, experience of, and outcomes from healthcare. This includes inclusion health groups such as people experiencing homelessness, people with learning difficulties or gypsy and traveller populations. The inequalities being addressed are those associated with the provision of healthcare, and the approach envisages targeting additional services at groups historically receiving poorer access to care. These inclusion groups may overlap with the Core20 population, but may cover different geographical areas and different spatial scales.
The ‘5’ refers to five clinical areas of focus for ICBs, including: maternity, severe mental illness, chronic respiratory disease, early cancer diagnosis and hypertension case finding. This focus on particular clinical areas is somewhat at odds with the other elements of the framework, as it removes from ICBs the opportunity to identify local specific service inequalities. As with the NHS Long Term Plan, the underlying assumption is that targeting programmes of work towards these clinical priorities will reduce inequalities, although the mechanisms by which this is expected to happen are not clearly explained.
Overall, the Core20PLUS5 approach is focused upon identification of target groups; it does not attempt to clearly define the type of inequalities to be targeted, with slippage between mention of healthcare inequalities and a more general definition of inequalities.
Summary
Policy documents setting out the design and roles of ICBs include a variety of claims as to how the new system will be well-placed to tackle health inequalities. However, there is some lack of clarity within the documents, particularly around: the exact type of inequality being addressed; the identification of the group(s) singled out as suffering from inequalities; and the ways in which the assumed mechanisms will work in practice. Moreover, within the documents terms are used imprecisely and interchangeably, and there is a profusion of potential policy objectives, targets and assumed mechanisms. The documents also do not explicitly consider the extent to which different approaches to tackling health inequalities may be in tension with one another. For example, a focus on the social determinants of health will look quite different from an approach which prioritises improving access to NHS services. With limited resources, systems will need to prioritise their actions. Finally, the profusion of targets and potential approaches does not provide a firm basis upon which progress could be measured and tracked.
Discussion
It is clearly to be welcomed that ICBs have been given a statutory duty to tackle health inequalities, and the foundational policy documents that we reviewed emphasised the rhetorical importance placed upon this duty. However, our exploration of these documents has shown that there remains a significant lack of clarity over what this means or how it might be achieved. The strength of our analysis lies in our detailed engagement with the relevant policy documents, and the fact that two researchers independently assessed each one, working collaboratively to reach a consensus around the identified logics and presumed mechanisms. Our study only addresses the role of health services in tackling inequalities. A wider analysis which also included public health policy documents would be interesting, but for this paper we have focused only upon the role of the NHS and specifically the statutory role of newly created ICBs.
Historically, research has shown that institutional issues associated with the policy making process have acted to limit the extent to which research evidence around health inequalities has been able to influence the policy agenda, with lack of institutional memory highlighted as a key issue. 27 The emphasis that we found within recent policy documents on the potential for partnership working to act as an important mechanism to reduce inequalities suggests that this has not changed; previous reviews of the impact of partnership working in inequalities have demonstrated the limited evidence supporting this claim. 28 Moreover, in the face of financial austerity and constrained Local Authority funding it seems unlikely that the complexities of partnership working will be easily resolved. Overall, the lack of clarity around the other mechanisms by which ICBs are intended to act suggests that the operationalisation of the ICB duty will require further consideration if it is to be successful.
Against this background it would be easy to fall into a policy nihilism, abandoning the attempt to tackle inequalities because it seems too hard. However, we would argue that this would be a mistake. Whilst it is true that the role of health care services in reducing inequalities is limited when compared with the potential gains from wider redistributive policies, 6 it is not true that nothing can be done. Our analysis suggests a number of potential opportunities. Firstly, we would argue for policy realism, moving beyond optimistic claims and strategic ambiguity 29 and focusing upon the limited field within which health care services can act. Realistic expectations of what is possible are more likely to be fulfilled, and less likely to generate policy fatigue. 30 Secondly, we suggest that our simplified model of the different types of inequalities amenable to NHS action can provide a heuristic tool to support both policy makers and ICBs in targeting action.
ICBs could use the tool to help them to identify the type of inequality that they wish to target. All types of inequality are of course important, but relevant action will differ for different types of inequality. Systems should then consider what comparison they are going to make and therefore which population they are going to target. The Core20PLUS5 framework supports this, but we believe that it remains too broad. We would suggest choosing a single group initially, with regular re-assessment and widening of approaches over time. It is particularly important at this stage to be explicit about the geographical area over which comparisons are to be made – the size of area chosen will depend upon the type of action being considered. The final step in this process would be to use our schematic to consider what particular drivers of their chosen inequality they can and should target. Thus, for example, should they decide to tackle access to care for people experiencing homelessness, consideration will need to be given to the availability of services, their accessibility and their flexibility in dealing with populations whose lives may be unpredictable. Similarly, should they decide to tackle inequalities in outcomes achieved after surgery, consideration of personal behaviours before surgery (so-called ‘prehabilitation’) should be considered, alongside decisions about prioritisation for treatment and support provided during recovery.
Policy makers, meanwhile, could use our model to help develop a more specific and realistic set of mechanisms by which it is expected ICBs will address inequalities. This needs to be teamed with an appropriate monitoring regime, which realistically identifies changes that might be expected as a result of action by ICBs.
Health inequalities are a significant problem, and the scale of the problem can potentially inhibit action. Our model not only provides a framework within which ICBs can plan their actions, it also makes plain the fact that action which focuses upon the role of health care services will necessarily be piecemeal and incremental in nature. This may feel uncomfortable to those aware of the significant challenges experienced by many in the population, but we would argue that systematic and incremental attention to identified problems is preferable to the paralysis which often occurs if too much is attempted at once. The most profound impact on health inequalities of all kinds would occur if the underlying social determinants of health were tackled via national policy attention to welfare, housing, education and employment. The policy aspiration is that better partnership working within the wider ICS will enable and support action in these areas, although as we have seen this has proved difficult in the past. 28 This is represented in our model by the opportunity for local health care systems to influence local policy and decision making; the extent to which this is truly possible will become clear over time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article draws upon the findings from independent research commissioned by the Department of Health and Social Care and carried out by the Policy Research Unit in Health and Social Care Systems and Commissioning (PRUComm). PRUComm is funded by the National Institute for Health Research (NIHR) Policy Research Programme (Ref: PR-PRU-1217-20801). The views expressed are those of the authors and not necessarily those of the Policy Research Programme, NIHR or the Department of Health and Social Care.