
Abstract
Background:
Many people in developing countries are struggling with chronic diseases yet traditional health services remain under-utilized in the quest for universal health care. Thousands patronize these outlets for care yet little is known about provider’s competence and how these competencies inform palliative care decisions and practices. The study documented traditional health practitioners (THPs) competencies and practices for traditional palliative cancer care service delivery in Kenya.
Methods:
This study utilized mixed-methods design and was undertaken in major towns across Kenya. A total of 201 Traditional health practitioners were purposely sampled, and interviewed. Five in-depth interviews and 6 focus group discussions were conducted. Quantitative data were analyzed using SPSSv22 while thematic and discourse analysis was carried out for qualitative data.
Results:
Majority (92.7%) of the THPs provided general traditional health services. Nearly half of the respondents (47.7%, n = 92) stated that they had received their knowledge and abilities through divine gifting, 71 (36.8%) lineage, 61 (31.6%) apprenticeship, and 39 (20.2%) formal study. Palliative care was determined by patient state and followed consultation with caregivers for 165 (85.5%) of respondents. For 160 respondents (83%), management practices involved a mix of patient examination, conventional medical tests, herbal medicine administration, follow-up or referral. Positive feedback consisted of symptom reduction and function recovery.
Conclusion:
Core competencies identified include: knowledge acquisition and specialization, assessment, diagnosis and disclosure, decision making, treatment, follow-up, and referral. Traditional palliative care providers share common health-related beliefs, practices and abilities that influence how they approach and make decisions regarding the health management of their patients, despite marked ethnic diversity. The shared pathways offer a chance to develop a cogent traditional palliative care service delivery model and health policy framework to promote its integration within the health workforce. The leading unmet requirements are knowledge of intellectual property rights, disclosure frameworks, and ethical regulation principles.
Introduction
In palliative and end-of-life care worldwide, cultural and conceptual differences, 1 cultural traits, values and rules, 2 provider capacities, competencies and their herbal formulations 3 are increasingly recognized as useful in shaping complementary management and response for cancer.2,3 Therefore, cultural differences in the way providers and consumers understand and handle disease and death nuances are of central importance in ensuring the effectiveness of any health care delivery. 2 The implications of cultural differences are particularly poignant during the palliative and dying trajectory. 2 There is scant literature on palliative care services from an indigenous perspective. 1 A critical component is understanding how provider competencies translate into practice and service 4 particularly for patients in need of palliative care 6 of indigenous nature. The World Health Organization (WHO) defines palliative care as a medical specialty that addresses physical, psychological, social, legal, and spiritual domains of care through an interdisciplinary team of professional and lay health care providers. 5 Palliative care is provided to a person who is living with a long-term chronic condition or life-threatening illness with the aim of improving their quality of life, irrespective of age. 6 World Palliative Care Alliance (WPCA) recommends that all institutions accept and use this definition and aim to guide creation of national health care policies and palliative care implementation strategies. 5 The universal call to alleviate suffering and enhance quality of life inspires the various kinds of care provided within the palliative care systems, including care provided at home, in a hospital, in a hospice, in residential healthcare facilities, and through non-conventional practitioner outlets. 5 The extent, scope, and tools used to deliver care however, vary by area, continent, and level of care and are provided by multiple providers with ill-defined competence. 7
Worldwide, palliative care is in high demand4-7 with approximately 56.8 million people in need of palliative care services; 78% of whom live in low and middle-income countries.5,6 This is attributed to the aging global population particularly in Europe 10 and rising cancer rates in both established and developing nations.5-8 In developing nations, particularly in Africa, it is primarily driven by a high burden of communicable and non-communicable illnesses. 8 The WHO states that over 10 million people in Africa are in need of palliative care (PC) annually.8,9 In Kenya, close to 1 million people are in dire need of palliative care every year. 6 Patients with cancer (28.2%), HIV (22.2%), cerebrovascular diseases (14.1%), dementia (12.2%), and lung diseases (5.1%) make up the bulk of these cases requiring palliative care. 6
There are palliative care services available in about 136 of the 234 nations across the globe.9,10 However, the level of integration varies greatly and resources vary by nation.2,5,7 Most of these countries with limited access to palliative care services are in Africa, 8 Kenya included. 6 Of 800 000 Kenyans in need of palliative care every year, only about 14 552 (2%) access these services. 6 The remaining 98% are in limbo waiting for palliative care appointments in the few and limited facilities. Thousands live and die with severe pain and other debilitating symptoms. 6 Nonetheless, a number of patients are flocking to lay health care providers (Traditional health Practitioners) to seek relief from physical and emotional symptoms.11,12 The concept of Traditional Health Practitioners (THP) is grounded on Traditional Medicine (TM) which refers to the knowledge, skills and practices based on theories, beliefs and experiences indigenous to different cultures, and used in the maintenance of health, prevention, diagnosis, improvement or treatment of physical or mental illness. 13 THPs resonate well with many inhabitants in Kenya and are recognized as a source of primary healthcare.14,15 Even though they have access to and can afford modern medicine, many Kenyans still believe in the efficacy of traditional medicine. 14
Despite the acceptance that traditional medicine contributes significantly to palliative care, and that models of holistic medicine contribute effectively to quality of life,1,11,15 the outcomes of these visits, modes of operation and treatment patterns in Kenya remain largely unknown. Similarly, little is known about provider knowledge and capacity, skills and clinical practice, or how these competencies inform palliative treatment decisions and practice. This study was therefore undertaken in view of the enormous need for universal, holistic and appropriate palliative care services for well-being of all people, and for support of research and development of affordable medicine for non-communicable diseases. The objective was to document THPs competencies for traditional palliative cancer care service delivery to guide future developments that explore the potential role of Kenya’s indigenous treatment regimen in the palliative management of cancer. The study was hinged on the bow tie model of 21st century palliative care. The model emphasizes that people affected by diseases such as cancer have varied needs over the course of their journey and thus require services from multiple providers at various times,16,17 including supportive care which is not exclusively provided by one discipline or agency. 18 Hence there is need for investigations to clarify their appropriateness including profiling the providers.
Material and Methods
Design
This was a sequential mixed-methods design. The quantitative study preceded the qualitative approaches. The qualitative approach provided context to the quantitative findings as rationalized by Bryman, 19 and Schoonenboom and Johnson. 20 Qualitative data was collected using focus group discussion (FGD) and in-depth interviews (IDI).
Setting
The study setting was informed by the operation zone and location of THPs service points (stand-alone clinics or THPs residence). Many THPs operate satellite clinics with diary and consultation scheduled days in each of the satellite clinics in key towns.12,21 Therefore, the sampling was based in 12 major towns namely: Mombasa, Nairobi, Kisumu, Nakuru, Kericho, Nyeri, Thika, Machakos, Kakamega, Kisii, Eldoret, and Meru where key THPs operate, in addition to rural areas for highly renowned practitioners.
Sampling and sampling procedure
This was a provider survey in which census was undertaken with the main traditional provider responsible for diagnosis, prescription of treatments and management. The target populations were THPs who reported to treat patients with cancer and were registered as THPs with the Ministry of culture, Kenya. The Ministry of Culture provides annual registration to THPs who submit the duly filled application form, provide 2 recommendations from government authorities, provide herbal medicine samples for testing at authorized research organizations and pay a prescribed fee. 22 A sampling frame was developed from the list of registered THPs obtained from the Ministry of culture, supported by referrals and snowballing. The sampling frame was purposely chosen to broaden the base of the data and ensure that all registered and acclaimed THPs were included and participated in the study. All registered THPs were mapped and screened in respect to reported management of cancer patients. The 2000 THPs identified from the sampling frame were contacted and invited to participate in the study. A screener survey was administered to allow identification of THPs who met inclusion criteria of: registration with ministry, more than 1 year of practice, history of managing cancer patients, and willingness to participate. Those THPs that did not meet these criteria were debriefed and discharged.
Research instruments
The Research tools were developed from reviewed literature. The themes in the questionnaire and qualitative guides included respondent demographics, practice characteristics, treatment protocols, management competence and general patient care practices. Additional questions included provider knowledge, beliefs and practices; priority natural products used and sources. The questionnaire was subjected to content and construct validity by a multidisciplinary team through Delphi technique. The questions were cross-checked for consistency with study objectives and conceptual framework. The study adopted an equivalence approach for reliability. Four invited raters reviewed and validated the questionnaire. The feedback was reviewed and compared in panel discussion. A pre-test crowned the adjustment and reliability of the instruments. Trustworthiness and rigor were obtained through the crystallization workshop, and immersion and back-check as advanced by Ghafouri and Ofoghi. 23 The research findings were presented to select THPs for validation in a 3-day workshop. The prolonged engagement with THPs provided an immersion session in which members from similar cultural contexts back-checked, criticized and reviewed participants’ contributions for consensus. The qualitative guides were deduced from emerging results from the quantitative survey and enriched with available literature.
Data collection procedure
Trained research assistants obtained informed consent from 201 purposively sampled THPs prior to interviewing them. Most THPs have several satellite clinics in different towns, and either visit each clinic at scheduled times or hire personnel to manage. For example, “Mambo” operates a major facility in Nakuru but visits her Kisii and Nyamira clinics every Thursday and Friday respectively. Therefore, the selected THPs were visited and interviewed on a day and time convenient to them during the survey period of September to November 2019. For quality purposes, a member of the research team reviewed the questionnaires and checked for completeness, accuracy and consistency at the end of each day, with corrective measures taken as needed. Qualitative data was collected via focus group discussion (FGD) and in-depth interviews (IDIs) in order to blend and enrich quantitative propositions, contextualize practice, and gain a deeper understanding into a variety of issues around skills, best practice, patient handling process, medication and treatment regimen prescription. Six FGDs were held with THPS selected using cluster sampling whereby the THPs were clustered per region, ethnicity and operation area. Journey mapping IDIs were conducted with 5 THPs with best practices to provide emic perspective, allowing co-creation. The criteria for best practices included operation of structured outlets, use of reference materials, patient records, documented operating procedures, cooperation, and the willingness to participate in the research.
Ethical approval
The Institutional Research and Ethics Review Committee of Kenyatta National Hospital- Nairobi University approved the study -Ethics and Research Committee/A/319. Research permit NACOSTI/P/18/41197/24208 was granted by the Kenya National Commission for Science, Technology and Innovation (NACOSTI). The association of THPs outlets gave permission to access the facilities and interview them or another primary provider. Before data collection, participants were assured of anonymity and confidentiality of information and informed that their participation in the study was voluntary. All consenting persons were asked to sign prior informed consent forms as per ethical approval requirements. The study was guided by 3 regulations. First the study relied on Article 31.1 and Article 24 1 of the United Nations Declaration on the Rights of Peoples and intellectual property law in regards to intellectual property rights. 24 Also, by the laws of Kenya, No. 33 of 2016 on protection of traditional knowledge and cultural expressions act 25 and last but most important human subject research ethics. No direct benefits were provided to consenting respondents in exchange for the information but they were reimbursed for highway transport during the qualitative study. The data collection team were trained on research etiquette, purpose and procedures of the study and consenting processes.
Data analysis
Quantitative data was entered into Statistical Package for Social Science (SPSS) version 22. Descriptive analysis was undertaken to generate trends and proportions in the data with bias to THP profile, competence, knowledge, skills, outlet dynamics and management practice. The core research team participated in the qualitative interview and analysis. The qualitative content analysis manually utilized the 7 steps of qualitative content technique 26 though some steps were undertaken simultaneously. The thematic content and discourse analysis techniques were used to detect important words, text, nuances, patterns and themes in the data. The data was aggregated into categories and subcategories, coded, to allow identification of themes. Excerpts and direct quotes from the data were used to support the qualitative themes and quantitative figures.
Results
Respondent’s demographic characteristics
From a total of 201 quantitative interviews conducted, 8 were incomplete or inconsistent, and were excluded from analysis. The findings are therefore from 193 respondents. Forty-two THPs participated in the FGDs and 5 in the IDIs. Respondents represented a variety of ethnicities, including 3 non-Kenyans with more males 145 (75%) than females. Majority of respondents were over the age of 40 years (92%) with more than half 107 (55%) being in the age range of 50 to 69 years. Respondents were mostly married 176 (91%) and professed Christian faith 172 (89%). A total of 131 (67.9%) respondents were farmers. Ninety-four (48.7%) respondents reported to have provided indigenous health services for over 21 years. Only 24 (12.4%) respondents had no formal education, with the rest having attended primary, secondary, and tertiary levels of education (Table 1).
Respondent’s demographic characteristics.

Knowledge acquisition and specialization
The respondents in this study acquired their skills and techniques through various pathways as presented in Table 2. Close to half (47.7%) of those surveyed indicated that their practice was a result of a divine gift bestowed on them. In contrast, 71 (36.8%) respondents had the knowledge passed down to them from previous generations of family, while 61 (31.6%) and 39 (20.2%) respondents acquired the skills through apprenticeship and formal training respectively. Seventy-one percent (137) reported participating in short courses like workshops, seminars, and conferences in order to improve their skills and techniques. Furthermore, 115 (59.6%) reported acquiring reference materials for use and guidance. The reference materials included books, personal notes from training courses, and the internet, used either individually or in combination, and with books having the greatest frequency of use (73%). In order to maintain continuity and sustainability, 143 (74.1%) respondents had mentored and trained young people. The majority of respondents were general THPs who managed a wide range of health conditions, but 14 (7.3%) were known for their expertise in certain cancer conditions. Five (2.6%) and 2 (1%) respondents respectively were famous for prostate and colon cancer management while others were renowned for blood, brain and mouth, throat, breast, skin, stomach and wound cancers at 0.5% respectively.
Skills acquisition and refresher training.

Diagnosis and disclosure
Over a third of the respondents (35%) indicated that their patients arrived with prior knowledge of their condition, but for the majority of patients, diagnosis is necessary, and THPs rely on various methods to diagnose patients. In this study, the diagnostic approaches ranged from review of patient’s clinical records (62.7%), provider’s experience (39.4%), patient’s verbatim history (35.8%) and medical diagnostic tests (23.3%). Disclosure appears to be a stumbling block for THPs. Only 10 (5%) respondents reported to disclose the diagnosis directly to patients, while 13 (6.7%) opted to manage the patient’s condition and break the news after improvement (Table 3).
Results dissemination approaches.

The discussants in FGDs reported that they consciously withheld the information of cancer conditions in order to avoid difficult questions from the patients or family members. Secondly, respondents withheld information to avoid uncertainties and facilitate smooth interaction and treatment process. One 58-year-old male discussant in a FGD narrated that “since most patients come to us when they are severely ill, withholding information reduces tension among the patients and between patient and family members and THPs.” He cited an example where upon sharing information, patients withdrew while others asked tough and unanswerable questions including: “why me? How much longer shall I live? Can I afford treatment? Will the THPs regimen work or cure this condition? Who will take care of my Children? Who cursed me?” Another female discussant reported that managing psychological effects of disclosing disease conditions to patients was a major challenge in THP practice. In her own words “In Kenya, Cancer is considered a deadly and debilitating disease. Patients lose hope and motivation to live. Hence, it is necessary to treat and provide palliative services without divulging the condition.”
Patient care practices
The study established that providers employed a few approaches in managing cancer. A third of the respondents (34.2%) routinely examined, provided herbal medication and provided follow-up. Another 54 (28%) respondents also examined their clients and provided herbal medication but without follow-up. A few respondents (3%) combined conventional and indigenous methods by ordering medical tests prior to physical examination, herbal prescription or referral (Table 4). For a variety of reasons, the majority of THPs (85.5%) involved caregivers in decisions regarding the patient’s care but 28 (14.5%) did not, due to confidentiality. The involvement was primarily for advice and instruction on the patient’s care 79.4% (medication adherence, moral and financial support) as shown in Table 5. Other drivers included giving dietary advice to patients (16.4%) and obtaining their medical background and history (4.2%).
Treatment procedures.

Consultation decision-making and caregiver involvement.

When requested to describe cancer palliative patient care practices, discussants agreed the process is subject to the patient state of presentation and no procedure fits all. However, for walking and talking patients, they take the patient’s personal information, medical history, undertake physical examination, then prescribe a treatment regimen. One FGD discussant explained “It is important to make caregivers understand the instruction of preparing the (treatment) regimen, the need to provide a good social environment and the values of eating healthy.” Another added “every patient in Kenya receives advice from family, neighbors and friends about disease management, treatment, drug adherence, cost and surgery. For this reason, it is important to rope in the family members to reduce negative influence from external people but more importantly, to reduce denial or none acceptance of having a cancer condition, and treatment”
Treatment protocols
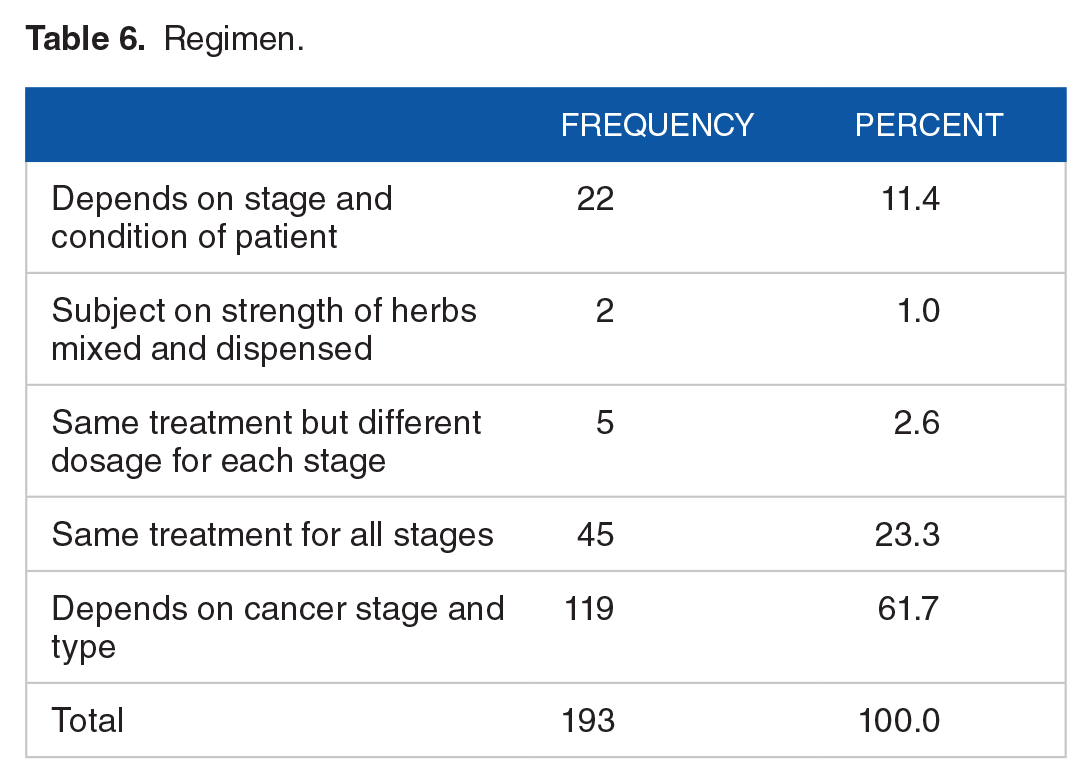
The patient’s cancer stage and type are the 2 factors that determined the herbal regimen to be prescribed for 119 (61.7%) of respondents. As many as 45 (23.3%) respondents prescribed the same regimen irrespective of cancer stage while other respondents considered the condition of the patient, stage of cancer, or strength of herbal medicines [Table 6]. Discussants in FGD affirmed that cancer condition is informed by the stage and patients-maintained status. One female FGD discussant said “the stage and condition of the patient is key in dosage dispensation. For severely ill or elderly patients, a cautious approach is necessary. Introduction of nutrition supplements followed by immune enhancing herbs is essential. Otherwise, you will miss the desired effect.”
Regimen.
Referral process
The study found that referral of patients is practiced by 134 (69.4%) of the respondents. Among respondents that did refer their patients, 41% referred only to other THPs if condition did not improve. For 35.1%, referral to hospital was part of the provider’s assessment and follow-up process while 23.9% referred patients to both THPs and conventional medical practitioners for complicated cases. During the IDI, one male service provider was asked about his mode of referral and the respondent recounted how a patient referral to a medical doctor made a fundamental difference in his practice. He said “a one patient referral to a hospital in Nairobi for diagnosis jump started key partnerships leading to establishment of a laboratory and employment of clinical officers in my facility to monitor vital signs.” Another respondent from the IDIs explained, “we coexist and partner with our colleagues in this field, and medical doctors in several ways. We exchange notes, herbs and patients with our peers and at times refer complicated cases for medication, diagnosis and debriefing. I for example concede diagnosis and breaking of diagnosis news to medical centres in Nairobi to allow proper counseling and debriefing.”
Progress review
The THPs review treatment progress and outcome through various physical, psychological and laboratory indicators. The most applied approach is a combination of physical examination and patient’s feedback at 36.1%. The physical indicators range from weight gain, ability to stand and ambulate independently, to improved speech, eating, swallowing, sleep, urination and reduced vomiting and swelling.
Similar results of improved signs and symptoms were reported qualitatively. During an IDI, a 65-year-old service provider was asked about her way of assessing progress and improvement, and she adduced: “apart from restored hope and positive feelings, I have witnessed my clients walk, eat, swallow and talk after using the (treatment) regimen.” Patient feedback on physical improvement and feelings were also independently used to gauge progress by 21.2% of respondents, while 8.8% considered a healthier appearance as well as reported recovery of ability and function. Other approaches were: documented change in vital signs, reported change in pain intensity, reduced inflammation and bleeding (8.3%), and post management lab assessment at a hospital (7.8%) (Table 7).
Reviewing of treatment outcomes approaches.

Discussion
Respondents’ demographics and characteristics
This could be the first description of the THPs competence and management practices for palliative care services in Kenya. While THP is a self-designated title, recognition and registration by the government requires the candidate to meet pre-defined requirements. The profiles were marked with pronounced ethnic diversity but with similarities in services and regimen, competence, practice and perceptions. The diversity resonates with Kenya’s multi-ethnic endowment and suggests that indigenous systems are built on solid principles grounded on ethnic ethos and pluralism.27,28 The mean age of the respondent was 58 years suggesting that Kenya’s cultural heritage is mostly maintained by the older generation. Additionally, most of the senior respondents were men which is similar to THPs characteristics in Liberia but unlike in other parts of the world like Indonesia and Mali where traditional practitioners are mostly women. 29 The gender inequity in the study may be attributed to variation in socio-cultural governance in Kenyan communities and tribes, which dictate and regulate social and gender roles and customs. 30 Farming was the primary source of livelihoods for the providers, suggesting that the THP service would be a secondary role and service to the community. The respondents therefore, could be a good cohort to be optimized in the promotion, propagation and conservation of useful but endangered medicinal plants. Unlike previous studies in Mali and one Kenyan community31,32 where THPs were mostly uneducated, close to half of the survey respondents reported a secondary or higher level of education. Three of the IDI respondents hold doctoral degrees, signifying that such providers may be encouraged and facilitated to play a significant role in research, and in achievement of universal health care including promotive, preventive, and rehabilitative modalities.
Skills acquisition and specialization
The indigenous health system predates the introduction of formal education and conventional healthcare in Kenya and THPs were integral to the health and well-being of every ethnic community. Survey responses indicated that traditional apprenticeship, divine intervention (supernatural gifting) and formal training were the primary channels of knowledge and skill acquisition, and technique mastery. Knowledge of palliation of cancer was also acquired and shared between senior practitioners and exchanged consultatively through in person visits, personal notes and demonstration. This is comparable to skills acquisition methods in Mali where Nordeng et al, found learning from a master and hereditary knowledge to be major pathways in traditional medicine. 29 In line with the constructivist theory of learning, acquired skills were honed through continuous education in formal workshops, seminars and conferences and via technology platforms like internet and WhatsApp networking.
Respondents who identified as specialists had consistently and effectively managed symptoms associated with particular cancers. The diffusion of formal sets of practice and new technologies into the informal pathways enriches the opportunities for apprenticeship to enhance skill bases, upgrade and expand existing systems and protocols. The willingness to enhance knowledge implied by high participation in short courses and 3 highly educated respondents with PhDs suggests that optimizing the use of technological platforms, and Technical and Vocational Education Training (TVET) colleges may improve the traditional provider skills, working conditions, customer-client relationship, innovations and job creation. Among the handful of self-declared specialists, the area of specialization seems to be based on human anatomy and physiology. Evidence suggests that colon and prostate cancer are connected and patients who have had prostate cancer in the past may be more likely to have colorectal cancer.33,34 According to Kim et al, males diagnosed with colorectal cancer have a higher risk for prostate cancer 34 while people with prostate cancer had a higher risk of having advanced abnormal growths in the colon. 33
Diagnosis and disclosure
Patients present to THP outlets with varying states and needs. Assessment is thus an important first step to guide the interaction of the patient with the THP. Medical diagnostic tests and clinical reports were the most applied methods of diagnosis. Many of the THPs’ patients agreed that medical diagnosis remains the primary mode of diagnosis, but a few apparently relied on self-diagnosis. 12 The results suggest that THPs and their patients are knowledgeable and cognizant of medical diagnosis as an appropriate health seeking behavior. However, experience and patient’s verbatim history remain significant for a few providers. In order to disclose diagnosis information, the 4 methods of direct messaging with counseling, direct messaging without counseling, indirect communication through caregivers, and non-disclosure until after recovery were used. The results support previous data which indicate that health workers apply various approaches of information management, and disclosure of diagnostic results is challenging to health workers.35-38 The underlying reason for non-disclosure is to avoid compromising the patient’s recovery process, a phenomenon that was noted in empirical studies reviewed by Ewuoso et al. 35 Although this is worrisome, the finding that THPs do utilize different methods of disclosure and are cognizant of the effects of implicit and explicit communication to the patients provides a foundation for developing a good information disclosure framework and regulation. With some patients being in the dark about their diagnosis and others not being counseled, investment in effective counseling and patient-THP communication strategies is vital to moderate the patients and providers behavior before and after diagnosis in the informal health sector. Evidence for establishing ethical standards and approaches to dealing with information management may be provided by research analyzing the ethical and information management challenges in the traditional health realm.
Patient care practices
Participatory decision making emerged in the study as a proactive care strategy involving the patient, provider and caregiver triad. The participatory approach assists in mining patient medical history, medication adherence, nutrition, referral, social, and financial support. The finding intimates that this joint engagement and partnership in decision making holds the key to service delivery. The results resonate with Yamamoto et al, who found that collective decision making facilitates the trust-building process between patients, family members and service providers, alleviates fears around palliative care services, and removes doubts about the adherence to the regimen prescribed.1,39 The authors reiterated that a living and flexible model is required to assist with service delivery. We concur with their proposition and suggest the addition of patient and provider attributes such as diagnosis and regimen preference, and people-centered care to augment quality traditional palliative care services.
Treatment protocols
Typically, a practitioner used one generic remedy in palliative cancer management, however specific formulation was safeguarded. Nonetheless, to adjust the dosage, efficacy and manage side effects of the standard of care, the number, proportion and combination of medicinal components was manipulated. The adjustment was pegged on cancer type, stage and patient’s condition. This is corroborated by Cheboi et al, finding that patients opined that THPs prescribe different doses based on patient condition, available herbs, formulation and regimen shelf-life. 12 The practitioners advanced for a singular treatment approach devoid of combination of traditional with conventional regimen. This is to avoid over-medicating the patient and to facilitate documentation of the effect of a specific regimen. Nevertheless, THPs recommended diet and lifestyle changes, counseling, massage therapies and spiritual nourishment to achieve body equilibrium, reduce stress and cope with the physical and mental disease burden. This phenomenon is well documented and elaborated.40,41 Rentala et al, wrote that, integrating a complementary therapy with body–mind–spirit intervention decrease depressive symptoms, improves general health and emotional management. 40 Chan et al, further explained that the body-mind-spirit model (BMS) is a comprehensive strategy that incorporates the basic and universal components of wellbeing with the aim of addressing a person’s physical, mental, and spiritual requirements. 41 It can then be deduced that patients and providers in the informal sector are aware of the importance of interconnectedness of the complementary and spiritual care; healthy eating, environmental and behavioral transformation hence may be valuable channels that promote health seeking behavior and a healthy lifestyle. Strategies and information sharing activities promoting stress reduction and reassuring physical and mental health such as massage and healthy eating are timely in the informal health sector.
The finding also suggests that THPs are aware of phytomedicine, pharmacology, and pharmacognosy concepts, and, just as was reported by Yin et al, and El Orfi et al, these herbal extracts and mixtures encompass a vast and useful repertoire of chemical entities manipulated to confer a complex, holistic and balanced medicinal activity.3,43 Additionally, the treatment modalities in traditional medicine are grounded on regimen contents not just targeting cancer sites but providing holistic health, healing, and life longevity. Our finding echoes the statement that traditional medicine is a holistic and complex treatment system containing several treatment modalities that are utilized to promote healing and wellness. 43 It is sufficed to report that 26 respondents shared their secret ingredients and natural product sources, majorly plants. The shared formulations and sources were documented in a yet to be published document. Nkosi and Sibiya similarly reported the willingness of THPs to provide evidence of their practices, in order to demonstrate their role and practices in cancer treatment.44,45 From their evidence a medicinal plant palliative display garden was established in National Museums of Kenya, Nairobi to provide a reliable source of authentic medicinal plant materials for reference, conservation, research and awareness. Additionally, priority plant species were subjected to phytochemical, anti-proliferative and cytotoxicity analysis with human prostate cancer and the preliminary result suggest growth inhibitory activity. This preliminary data provides potential leads for advanced research on the priority plants and mixtures used in traditional palliative cancer care.
Referral process
Intra and inter professional referral is well pronounced in the field of traditional cancer palliative care. Intra referral is between THPs and is premised on hierarchical model characterized by vertical, horizontal and back patient movement. The Intra referral model is informed by the THPs prowess, respect and niche. A pathway can be optimized to standardize and improve care practices within disciplines and between generalist and specialist practice, according to the intra consultancy, which shows the traditional providers’ desire to participate in conversation. The finding agrees with Smith et al, who writes that informal consultations have additional potential for standardizing and better integrating the delivery of care between and across dissimilar clinical disciplines, such as chiropractic and medicine, in a multidisciplinary environment. 46 The reason for inter referral in traditional health care is similar to that in conventional care. 47 Intra professional referral reported in this study is an explicit marker for good professional relationship and pathway for jumpstarting integration process as well improvement of coordination and continuity of care for patients shared between these provider types.
Progress review
At follow-up, practitioners evaluated patient progress based on physical examination and feedback received from the patient or caregiver. The physical indicators used by THPs genuinely mirror measures of activities of daily living in conventional medicine. Performance of personal care activities such as selfdressing, walking, doing laundry, preparing meals and bathing are considered to be necessary for independent living. Independence is a crucial element in palliative care since the objective is to improve the patient’s quality of life. Patients who reported restored hope and positivity to their provider embody the importance of feeling heard and understood especially in palliative cancer care where effective counseling and communication skills are required. Providers are also reported to rely on clinical results such as vital signs and lab tests, hence displaying a basic understanding of physiology of the human body. This was similar to the practice observed by healers in Botswana. 48 The authors noted that scheduled follow-up visits and phone calls were used to assess adherence and address side effects. These practitioners could further improve their ability to assess patient progress by either adopting the conventional performance scores such as Karnofsky or ECOG scales, or innovating similar standardized scales better suited for this unique setting.
Limitation of the study
This study is not without limitations. This was a mixed methods study, and among the limitations of our study was the unstipulated length of time of being on the traditional medicine treatment relative to healing perception. Thus, the associated results must be interpreted with caution.
Conclusion
Key THP competencies essential for traditional palliative care include knowledge acquisition and specialization, assessment, diagnosis and disclosure, decision making, treatment, follow-up, and referral. Traditional health practitioners hold similar health-related beliefs, practice models and abilities that influence how they view, handle, and make decisions about their patients’ health. Traditional palliative cancer care management protocols are characterized by varied approaches for diagnosis and disclosure, prescription of herbal treatment, review and follow up. The traditional palliative cancer care value chain may be improved by empowering providers with knowledge of ethical standards of health practice, intellectual property rights and information management skills for classification of protocols and treatment regimens. The formulation of official training as well as government-standardized knowledge and practice will aid development of a service delivery model and health policy whilst augmenting indigenous representation and integration within the health workforce. Detailed documentation of procedures and practices as well as rigorous research to support pharmacopeia claims will increase acceptance of services especially in the context of evidence-based practice. Providers are service and context driven and may play a significant role in documenting the prevalence of other chronic conditions such as diabetes and blood pressure when trained. The authors additionally, call for empowerment of THPs on the fundamentals of intellectual property rights and training on disclosure frameworks, and ethical regulation principles.
Supplemental Material
sj-docx-1-his-10.1177_11786329231211780 – Supplemental material for Providers’ Competencies and Management Practices for Traditional Palliative Cancer Care Service Delivery in Kenya
Supplemental material, sj-docx-1-his-10.1177_11786329231211780 for Providers’ Competencies and Management Practices for Traditional Palliative Cancer Care Service Delivery in Kenya by Solomon K Cheboi, Wanjiru S Ng’ang’a, Philamon Nyamanga and Stanley Kibet in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329231211780 – Supplemental material for Providers’ Competencies and Management Practices for Traditional Palliative Cancer Care Service Delivery in Kenya
Supplemental material, sj-docx-2-his-10.1177_11786329231211780 for Providers’ Competencies and Management Practices for Traditional Palliative Cancer Care Service Delivery in Kenya by Solomon K Cheboi, Wanjiru S Ng’ang’a, Philamon Nyamanga and Stanley Kibet in Health Services Insights
Footnotes
Acknowledgements
The authors are grateful to the traditional practitioners for participating in the study. Sincere gratitude goes to the executives of their organizations and the Ministry of culture- Kenya for linking the study team with the organizations and their members. We also appreciate NACOSTI Kenya for permitting the study and National Museums of Kenya (NMK) management for their infrastructural support.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful to National Research Fund (NRF), Kenya for funding the research.
Declaration of Conflicting Interest:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The authors have contributed significantly for this manuscript. Solomon Kemoi Cheboi (SKC) conceptualized the idea, sourced for funds, implemented the methodology, processed the write up, and analyzed the data while Wanjiru Scolastica (Ng’ang’a, (WSN), Philemon Nyamanga, (PN) and Stanley Kibet (SK), contributed equally in the project write up, design implementation, data collection, supervision and provided technical and critical revision and review of the reports
Data Availability
The data that support the findings of this study are available from the corresponding author.
Disclaimer
The views and opinions expressed in this article are those of the respondents and authors and do not reflect the official policy or position of any affiliated agency of the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.