
Abstract
Aim:
This article aims to document 10 service trajectories of young adults (YA) and their parents, informed by healthcare professionals (HP), before and during a first episode of psychosis (FEP).
Design:
Based on a crisis model perspective of the Life Course Theory (Elder; Elder and Shanahan) developed by Carpentier and White, and adapted to the current context to track community and specialized services trajectories. Thematic analysis was used to code responses to open-ended questions around the need for help and accessing services by young adults affected by a psychotic disorder, and their parents.
Setting:
In collaboration with FEP clinics, setting of choice by YA and their parents.
Participants:
5 YA, 12 parents, and 6 HP.
Results:
10 individual service trajectories grouped into 3 distinct types of trajectories (optimal, typical, and complex) based on grouping 5 similar characteristics, highlighting service access complexity and early intervention in FEP.
Conclusion:
This study is the first of its kind to examine the experiences of those who seek needs-based community and specialized services leading up to and during a FEP. Findings provide key insights related to early intervention in FEP and recommendations on improving access to such services in Quebec.
Keywords
Introduction
First episode of psychosis (FEP) has been the focus of research for nearly 2 decades.1,2 Best practice treatment guidelines in Quebec recommend early intervention,3,4 proven to limit the deterioration of the affected person’s social functioning5,6 and reduce family burden.7,8 Best practices also recommend involving families early in the process,2,3 as such interventions have a positive effect on the affected person, including reductions on the relapse rate. 7 This model of early intervention has been evaluated by well-established early intervention programs in Australia, the United Kingdom, and Canada as an essential component of the intervention aimed at maximizing family functioning and reducing the risk of long-term difficulties. 9 Yet the trajectories of needs-based community and specialized services used before and during a FEP rarely have been studied.
The importance of community and specialized services in the context of FEP
The FEP context often requires different interventions to address specific needs, yet it is not always necessary to use specialized services such as counseling or family therapy. Specialized services offered by FEP programs deal with the emergence of the disorder, whereas community-based services offer support to families and their YA affected by FEP. The Family Care Pyramid 10 often operates as a framework for caregiver-assistance programs, guiding the delivery of services to meet caregiver needs. Morin and St-Onge 11 highlight the value of offering various services to families who support their YA with a FEP. Access to community and specialized services, as well as managing transitions between these 2 types of service are important considerations in caring for and supporting YA affected by FEP, and their families.
This study aims to document service trajectories used by YA and their parents before and during a FEP, and is structured around the following objectives: (1) to better understand how the request for help was initiated; (2) to identify the services (community-based and specialized) used by YA and their parents; (3) document barriers encountered during the service trajectory; and (4) document, from the perspectives of young adults, parents, and healthcare professionals, the impact of service use on reducing distress and responding to families’ need for support.
Methods
The crisis model analytical framework developed by Carpentier and White 12 in the field of family studies and caregiver care trajectories is based on Life Course theory,13,14 which was developed to understand links between social trajectories, individual development, and sociohistorical contexts in human development. 15 According to Carpentier and White, 12 the Life Course perspective is appropriate for studying caregiver care trajectories, as engagement in caregiving can extend over a long period of time. Crisis model trajectories are made up of transitions occurring in unpredictable and chaotic contexts or events. This type of trajectory analysis allows not only for the modeling of the individual’s subjective experience, making it possible to explore the service trajectory entry, but also the delays before diagnoses, and the waiting time before accessing resources. 12
Events and transitions over time affect the condition of the YA and their parents faced with the uncertainty and ambiguity that characterize a FEP. As they initiate help-seeking services, YAs and their families create trajectories in accessing services. This study adapts the crisis model perspective to the current context of accessing community and specialized services trajectories before and during a FEP in order to track the complex paths taken by YAs and their parents, as well as highlighting the duration and level of help-seeking depending on when and what services are received. Analysis of individual services trajectories of YAs and their parents, identifies points of convergence and divergence, in addition to focusing on the singularity of these pathways regarding the demand for help. For instance, events, defined as punctual facts that can be recorded at a specific time and that concerns an individual, in a particular time and space 15 correspond to YAs and their parents accessing community and specialized services. Transitions refer to short periods of instability in the trajectory between 2 more stable periods 15 wherein role changes experienced by YAs and their parents can occur in their respective trajectories. For example, transitions such as the emergence of the FEP, a psychotic crisis, entry into a new service or a change of services can lead to role changes.
Three qualitative research tools comprising descriptive and explorative components are used to document specialized and community services trajectories of the participants, and their subjective viewpoints regarding the meaning they give to their experience. This approach makes it possible to access the complexity of phenomena from the participants’ own experiences, within a given social context, 16 in addition to revealing the commonality among participant experiences.
Study Sample and Recruitment
Young adults (YA), their parents, and Healthcare professionals (HP) were recruited in collaboration with clinical programs specializing in the treatment of a first episode of psychosis (FEP clinics), as well as community organizations affiliated with Réseau Avant de Craquer (RADC) network. Eligible YAs were 18 years of age or older who previously or currently received services in a FEP program, were able to consent to participate in the study, and were stable. Parents had to play a significant role in supporting their child and had used FEP program services themselves.
Recruitment proceeded as follows: (1) HPs were informed of the research study and were asked to identify YAs and their parents who met the research criteria. A factsheet describing the study was distributed to all potential participants; (2) interested participants could authorize HPs to transmit their contact information to the research team; (3) the research team then contacted those who agreed to participate in the research, verified their eligibility, and explained what their participation would be. An interview appointment was set at a time and place of the participants’ choosing; and (4) once the YAs and parents were interviewed, the research team asked them for consent to have the HP on their case participate in the research study to provide further information about their case. HPs were contacted if participants gave consent.
Data Collection Tools
Twenty-three interviews were conducted over a 6 month period. The sample presentation appears in the Results section. All participants provided written, free and informed consent to participate in the research. Data collection was conducted using 3 different tools: (1) Service Timetable, (2) Retrospective Interview Technic (RIT), and (3) Semi-structured Interview.
Service timetable
This study used an adapted form of the services calendar tool developed by Freedman et al, 17 and employed in several qualitative studies of care trajectories.15,18-20 The service timetable provides a tabular compilation of community-based and specialized services used by YAs and their parents before and during the FEP. The table is comprised of a column indicating a time marker (year and month, or period) followed by columns listing types of services received.
Two versions of the timetable were created, one for the YA and one for the parent. The YA timetable depicts all services received only by the YA, whereas the parent timetable indicates all services received by the family. In addition, the parent timetable distinguishes services received either from the FEP clinic, or other community organizations. A guide accompanying the service timetable includes a list of services potentially used by the participant. The participant indicates which services were used and, if so, identifies who benefited from the service, who initiated the request for assistance and for what reason. The Service Timetable used for the parent is presented in Appendix A and includes the interviewer’s guide.
Retrospective interview technique
The Retrospective Interview technic (RIT) is a tool used to assess participants’ perception of the evolution of their interpersonal relationships as a function of events that are significant to them. 21 It is mainly used in research around trajectories, 22 turning points,23-25 and events. 26
In this study the RIT was adapted to analyze the evolution of the level of need for support of YAs and their parents as a function of the services used. An RIT chart was created in order to plot the data from the semi-structured interview (hereafter described) with the participant. The graph’s horizontal axis indicates the period of time over which participants indicated they accessed needs-based services, and the vertical axis indicates the participant’s assessment of level of need for support rated on a scale from 0 to 10, with 0 representing no need for support and 10 representing the greatest need for support.
Next, the interviewer plots the main services the participant received over the period of time indicated on the horizontal axis, based on the information from the Service Timetable. Then, for each element placed on the horizontal axis, the participant qualifies his level of need for support at that time between 0 and 10 on the vertical axis. Once the participant has specified a level for each element of the horizontal axis, points are connected to draw a curve. The participant can then elaborate on what he or she thinks led to the situation. Appendix B presents the RIT chart for the parents and the interview guide.
Semi-structured interview
The semi-structured interview aims to understand the perspective and behavior of individuals in particular situations by exploring their subjective experience. 27 The interviewer asks broad questions that allow the participant to express his or her point of view while respecting the boundaries of the research objective. 27 This type of interview usually accompanies service timetables and the RIT.15,19,20,24-26 It makes it possible to understand the context in which events take place and the place they occupy for participants in their trajectories. 15
Semi-structured interview conducted with YAS, their parents, and HPs in this study. Topics explored included the process of initiating the request for help, providing details on the community and specialized services used by YA and their parents, identifying some of the obstacles encountered and the impact of using services on reducing families’ need for support. YAs and parents were interviewed separately for 90 minutes, at a time and in a place of their choosing. On average, 30 minute interviews with HPs were conducted by telephone and included a few additional questions on the professional’s practice.
Data Analysis
Data in this study were analyzed using thematic analysis consisting of identifying, analyzing and interpreting the themes that emerged. Coding was the main process used to develop themes by identifying items of analytical interest in the data and labeling them with code. 28 Individual interviews were recorded and transcribed for content analysis using QSR NVivo 9 software. Data were analyzed using thematic content analysis consisting of coding, categorization, linking, integration, modeling, and theorization.16,27 The first stage consisted of an intra-subject analysis or vertical analysis of individual trajectories and the second phase, an inter-subject analysis or transversal analysis of trajectories, aimed at highlighting the elements of convergence and divergence in the participants’ discourse with regard to the different themes addressed. Based on the theoretical approach chosen, the analysis carried made it possible to identify the main events and transitions, and to identify the trajectories of services before and during a FEP. This ordering aligns with the notion of order important for understanding the impact of events and transitions on trajectories. 12 The effects of a transition will not be the same depending on when it appears in the trajectory and the events that preceded or followed it. 1
Ethical Considerations
This multi-centric study was first approved by the ethics committee of one of the 3 Quebec sites where the study took place (MP-CISSSBSL-2018-05) with the ethics certificate subsequently recognized by ethics committees of other 2 sites (CIUSSS-CN, MEO-27-2019-1510 and CIUSSS MCQ, 612-PEP). In addition the ethics committee of the Université du Québec à Rimouski also approved the research project (CER-101-746).
Results
Participant socio-demographic characteristics
A total of 23 participants included 12 parents, 5 Young Adults (YA) who experienced a FEP and 6 Healthcare Professionals (HP). Ten individual trajectories made up of 2 triads and 2 dyads comprised of a parent and/or YA and/or HP who shared their experience about their service trajectory. The majority of parents (n = 12) identified as female (n = 10), ranging in age from 44 to 69 years old. Two men joined their spouses to participate in the interviews for a total of 12 parents, however only 10 individual trajectories are counted. All parents completed post-secondary education and most were employed (n = 7). Three male YA and 2 female YA between 20 and 28 years old, participated in the study. Most YA were unemployed or looking for work (n = 4). One YA combined full-time studies with part-time employment. Of the HP who participated in the study (n = 6), 5 were from FEP clinics. Two HP responded twice to the interviews as 2 families who were not in their clinical charge were involved in this study. HP were between 34 and 63 years old, mostly female with a university education in social work (n = 5). Their experience in family intervention varied between 8 and 27 years, with HP practicing in FEP intervention settings between 4 and 20 years.
Participant service trajectories
Ten (10) service trajectories of triads/dyads were grouped into 3 trajectory categories: Optimal, Typical, and Complex, based on 5 characteristics identified in the trajectory analysis: (1) use of child psychiatry services during childhood and/or adolescence, (2) age of onset at the first signs of the FEP, (3) request(s) for help leading to entry into the service trajectory, (4) the community and specialized services used by the YA and their parents, and (5) the duration of the service trajectory during the FEP (Table 1). The HPs’ perspectives concerning each of the service trajectories corroborated the categorization of care trajectories and provided a complementary view of the service pathways of these families.
Characteristics of the 3 Service Trajectories before and during a FEP.

Optimal Service Trajectory (N = 3)
The Optimal Service Trajectory (OST) consisted of 3 triads of YAs, parents, and HPs, totaling 9 semi-structured interviews. The OST illustrates the evolution of the need for support as a function of the services used (Figure 1). The majority of families in the OST previously used youth and/or adolescent services. For this group, the estimated duration of non-treated psychosis was between 1 month and a year, with the average age of onset of a FEP of 23.7 years. YAs and/or their parents sought help either by consulting a family doctor, or a specialized educator at a community clinic or community organization, or at the hospital emergency department. Follow-up referrals to a FEP clinic were made for YAs and parents, in addition to ongoing use of other community-based resources by both of these participants. The OST duration varied between 2 and 5 years.

RIT graph for the Optimal Service Trajectory (OST) for Triad 02.
Some YAs attempted to obtain help themselves with their parents’ support. One YA’s parents followed up with a specialized educator at the community clinic following suicidal remarks.
Lucky we had [specialized educator of the CLSC], we were extremely well served, lucky he was there, because he pointed us everywhere. (P02)
HPs in the OST reported that YAs and their parents actively participated in the intervention process (eg, participation in parent support groups, parents attending intervention plans, YAs attending medical appointments, participation in workshops, etc.) and collaborated with care and treatment plans. HPs observed a high level of involvement by parents supporting their YAs.
It doesn’t compromise their involvement [in reference to geographical distance families travelled to the PEP clinic], they were more involved than families who live 2 blocks from here (. . .) Parents were more involved than average. I would put them in my top 10 families I’ve seen in the last 10 years. . . (HP02)
The OST in the RIT graph plateaus between the time of the first consultation and the follow-up referral at the FEP clinic, indicating support needs remained high between the diagnosis of the FEP by the family doctor and the follow-up service at the FEP clinic. However once the YA was followed by the FEP clinic, need for support markedly decreased and the outcomes in the OST were optimal. This service trajectory is similar to that of the other 2 triads in this group.
Typical Service Trajectory (N = 3)
The Typical Service Trajectory (TST) consists of 3 dyads of parents and HPs, totaling 6 interviews. No YAs participated in the TST interviews. According to HPs, the TST is “typical” as it corresponds to trajectories usually encountered in FEP program practices. The HPs also use the term “standard” to describe this type of trajectory, referring to the systematic way that follow-up to a FEP clinic and family involvement commences. The TST is punctuated by YAs refusing services, however parents usually remain involved throughout the trajectory.
The TST indicates that no child and/or adolescent services were used prior to the onset of the FEP, yet parents reported that their YAs experienced functional difficulties over time, varying between 1 year and 10 years before the emergence of a FEP (prodromal stage). According to Malla et al, 6 the prodromal stage precedes the psychosis, thus if risk factors associated with the development of a FEP, such as a state of depression, irritability, social withdrawal, and anxiety, are detected during this stage, a FEP could be prevented. Parents had more difficulty in accurately determining the age of onset of the FEP situated approximately between 19 and 26 years of age. Following the emergence of the FEP, the initial request for help varied depending on the situation or event (eg. police intervention through a crisis agency, consultation in psychology and with the family doctor, or emergency room consultation with hospitalization). Reports of psychiatric hospitalizations varied between 48 hours and 4 months prior to follow up referral to a FEP clinic. Parents’ first contact with community organizations occurred either during the YA’s hospitalization, or at follow-up with the FEP clinic. The TST duration varied between 3 and 5 years.
One parent stated that she had to connect healthcare professionals with services so that information could flow between them: “(. . .) it is the common thread because there is no one who cares” (P03).
The RIT graph line of the TST for Dyad 07 (Figure 2) shows that the parent’s support needs decrease gradually and then markedly following attendance of the YA at the PEP clinic. A similar finding is identified for the other 2 dyads in the TST.

RIT graph of the Typical Service Trajectory (TST) for Dyad 07.
Complex Services Trajectory (N = 4)
The Complex Services Trajectory (CST) consists of 1 triad, 2 dyads (composed of a parent-HP dyad and a YA-parent dyad), and a lone parent, totaling 8 interviews. The CST is characterized by a more complex course compared to the OST and the TST due to comorbidity, a lack of commitment to treatment on the part of YAs and difficulty in making an accurate medical diagnosis.
Most parents in the CST consulted with a family doctor or used child psychiatry services due to functional difficulties experienced by the YA before the emergence of a FEP. The CST trajectory for child/adolescent services ranged between 2 and 6 years. In addition, the estimated duration of untreated psychosis (DUP) covered a period of between 1 and 2 years. One mother described the DUP as a time when she felt left alone to fend for herself:
But at that time, I think I was the only one who could intervene and help him; I was alone to figure it out. [. . .] It was hard, yes, yes, it was on my shoulders, it took a lot of energy, because I worked, I am all alone, and I couldn’t afford to lose my job. I felt helpless [. . .] with my son in this. He could have ended up taking his own life. . . (P04)
THE CST indicates that the first clear signs of a FEP occurred between the ages of 18 and 22. In this trajectory, it is more difficult to identify the initial request for help as YAs were already in the care of a family doctor or psychiatrist before the onset of a FEP. Often, the initial request for help occurred amidst repeated emergency department consultations, as well as interventions by community crisis agencies in this scenario. YAs entered FEP clinics either following hospitalization or pursuant to a referral by a psychiatrist who provided outpatient follow-up. YAs also benefited from many public and community services in addition to FEP clinic services.
Parents demonstrated a strong commitment to their YAs. However, the complexity of cases proved to be a more difficult trajectory for families. For instance, 2 HPs on the CST reported that YAs had difficulty accessing services and were on a waiting list before accessing the FEP clinic. Also, 2 of the YAs were resistant to treatment plans and did not have any HPs on their file at the time of the interview.
The CST duration varied between 2 and 8 years and was punctuated by hospitalizations or emergency room visits, the number of which is impossible to quantify by the participants as they were so numerous. The RIT graph line representing the mother’s need for support decreases following case management by the FEP clinic. However in this trajectory the YA’s need for support persists and increases during follow up at the FEP clinic. In another trajectory on the CST, a mother’s need for support increased during follow-up at the FEP clinic (Figure 3).
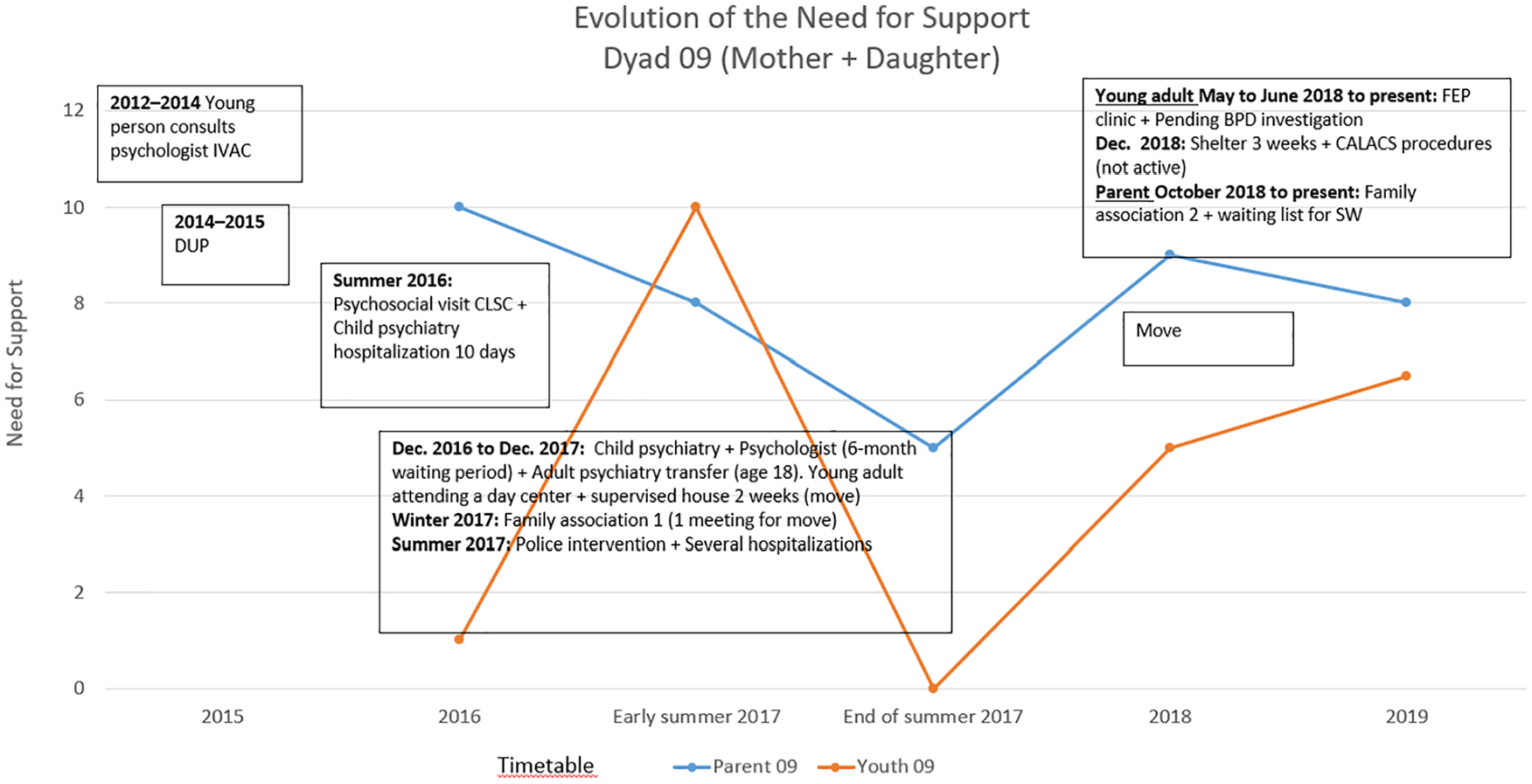
RIT graph of the Complex Services Trajectory (CST) for Dyad 09.
Discussion
Access to services during a first episode of psychosis
The FEP Program framework advocates for accessibility to FEP programs and is consistent with early intervention cases of FEP.29,30 In Ontario, family physicians play a primary and active role in the service pathway for youth with psychosis. 30 In this study, all 3 service trajectories indicate a variety of medical interventions undertaken from the first signs of the disorder. For example, all YAs consulted their family doctor and/or presented at the emergency room (with or without psychiatric hospitalization).
OST participants were able to more accurately name the timing of the onset of the FEP whereas participants in the TST and CST found it more difficult to identify prodromal symptoms or accurately state when the onset of the FEP occurred. Identifying the initial request for help and who makes it (the YA and/or the parent) was not always clear cut. Thus the uncertainty and ambiguity that characterize the emergence of a FEP over a longer period of time are reflected in the greater complexity of the TST and CST of YAs and their parents in these particular contexts.5,31,32 Yet the fact that many services were identified in all the trajectories testifies to the concrete and often repeated actions taken by YAs and their parents to obtain help.
In line with Carpentier and White’s 12 crisis model analytical framework of transitions occurring in unpredictable and chaotic contexts, the present analysis of service trajectories made it possible to elicit the subjective experience of the individual in order to ascertain, among others, the entry into the service trajectory, as well as delays before diagnoses, periods of inaction, and waiting for access to resources. Moreover, this analytical process made it possible to take into account the complexity of the paths of YAs and their parents, who did not follow pre-established pathways with well-defined stages. For instance, YAs and their parents sometimes made multiple requests for help, and received services from, various public and community services, often well before they were accepted into care by a FEP clinic.
Frontline services appear to be the preferred entry point for YAs and their families. Considering that early treatment of FEP ensures a better chance of recovery, this service pathway needs to be expedited. To do this, frontline workers (including school and employment settings) need to be able to recognize the signs of FEP and quickly refer youth/YAs and their families to FEP programs. 30
Early intervention and reducing the duration of untreated psychosis (DUP)
The approximate duration of the lead-up to starting a FEP program and the duration of untreated psychosis (DUP) is 1 year or less in the OST, and between 8 months and 2 years in the TST. However, the DUP in the CST can extend up to between 1 year and 2 years. Although the DUP is relatively shorter for some participants, the delay before entry in the FEP program is nevertheless remarkable. For CST participants, the effect of repeated consultations with various HPs, in addition to the YA’s deteriorating condition impacting different spheres of their life, makes it tortuous for these persons to obtain services and ultimately delays treatment initiation. 29
In our sample, the divergence between the estimated DUP and the duration of the service trajectory during an identified FEP is proportional. As indicated in the OST, a shorter DUP results in a shorter service trajectory duration during a FEP, compared to the CST where the estimated DUP results in a longer service trajectory during a FEP. Thus, the organization and efficiency of services influences the duration of the YAs’ service trajectory and ultimately, their recovery.
Linking community and institutional services
The initial demand for assistance and accessibility to services is closely linked to the connection between community and specialized services. In this study YAs and their parents used services from both the health and social services network (HSSN) and community, private, or other services (eg. police and legal services) throughout their service trajectories. All YAs received public services, including follow-up with a family doctor, outpatient psychiatric clinical services, and/or with a psychosocial worker at the community clinic. The majority of YAs also received local community services and other supports in the community (eg. professional reintegration organizations) and/or temporary housing organizations (eg. crisis center). Police services also intervened at one time or another in the trajectories of YAs, especially in the CST. Although all community and specialized services were used during the DUP and prior to entering a FEP clinic, the majority of YA referrals to FEP clinics occurred following hospitalization (n = 7), followed by referral from a community clinic (n = 2) or by an outpatient psychiatrist (n = 1).
All families benefited from the support of community organizations, some before the YA entered the FEP clinic, while others were supported after entry into the FEP clinic. While community and specialized services exist, communication between services is tenuous. Analysis of interviews with HPs revealed they are aware of service resources, however communication between institutions is practically non-existent, thus complicating efficient and timely access to services and the networking between them.
In order to meet the support needs of YAs and their families, and ensure continuity and complementarity in the various mental health services that ultimately offer greater assurance for recovery, HSSN institutions must facilitate territorial consultation mechanisms with community organizations and inter-sectorial services. 3 Action 7.7.1 of the 2022-2026 Inter-ministerial Mental Health Action Plan is useful in the context where referrals to FEP clinics could be made much earlier in service trajectories, ensuring a network of more effective services.
Study Limitations
Two selection biases concerning the recruitment of participants are present in this study. First, HPs from FEP clinics and community organizations were encouraged to present the proposed study to YAs and their parents in order to invite them to participate in the research. We determined that HPs targeted YAs and their parents who would demonstrate good collaboration at the research interview. Next, the requirement that the parent had to have received services from a FEP clinic and an RADC network organization, led to recruiting parents already well involved and invested in the trajectory of services of their YA. This limitation hindered our access to families who were less involved in the service trajectory of their YA. Other limitations included the effect of time, and changes in the organization of services since the interviews were conducted. Also, some norms around referrals to FEP programs have evolved in the field since the study was conducted, as well as the increase in number of FEP clinics in Quebec.
The fact remains that the 3 trajectories, and the experiences of participants in this study, are representative of the stories documented in the field and that these types of trajectories shed new light on understanding the service paths in a FEP.
Conclusion
By documenting the service trajectories taken by YAs and their parents before and during a FEP, this study reveals that YAs and their parents make several requests for help and support in various public, private, and community agencies and institutions. Also highlighted in this study is that the duration of a DUP is proportional to the duration of the FEP. Thus, the earlier YAs and their parents can access and receive appropriate services prior to a FEP, the shorter the duration will be of the FEP.
Better screening by all HPs in both the public health and social services network, and community sectors, means easier access to FEP programs. For example, if YAs and their parents could apply directly to a FEP clinic for evaluation, then a true network of services between the public and community networks would ensure early intervention in a FEP. Also, the addition in FEP teams of family peer support workers33,34 who use their experiential and service navigation knowledge to support families in similar situations, could open another door to improve service trajectories for YAs and their families. Peer support workers help navigate mental health and social services systems by making trajectories more fluid, rapid, and humane. Family peer support workers may facilitate linkages between community and institutional services, promoting better access to those services.
Footnotes
Appendix A Service Guide and Timetable (Parent)
Appendix B Retrospective Interview (RIT) and Guide (Parent Version)
Acknowledgements
The authors would like to thank Anne-Sophie Bergeron and Angelina Lacroix, research professionals, as well as Émilie Peredo-Tessier, research assistant at the Université du Québec à Rimouski (UQAR) for their involvement in the various stages of the study. They would also like to thank Mary Anne Levasseur for her contribution to the revision of the manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research study was funded by the Fonds de recherche du Québec–Société et culture (FRQSC), through its Établissement de nouveaux professeurs chercheurs program (2017-2021). The first author would like to thank the granting agency for this valuable financial support.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The authors confirm contribution to the paper as follows: conception and design: MHM; date collection: MP; analysis and interpretation of results: MHM & MP; draft manuscript preparation: MHM & MP. All authors reviewed the results and approves the final version of the manuscript.