
Abstract
There is a great demand for quality early intervention services for autistic children and their families. Caregiver-mediated interventions are critical components of evidence-based early intervention. However, their implementation in publicly funded systems is often done with poor fidelity. Qualitative evidence suggests that family characteristics impact clinicians’ use of caregiver-mediated intervention coaching strategies. We estimated associations between family characteristics and clinicians’ use of a caregiver-mediated intervention in a publicly funded early intervention system, leveraging data from a pilot randomized trial. Data were collected from 12 clinicians and 34 families. We used multiple linear regression models to estimate associations. The association between household income and clinicians’ overall coaching fidelity demonstrated a quadratic trend (b = −10.4, standard error = 4.1, p < 0.05) with low fidelity for low- and high-income families relative to middle-income families. Use of in vivo feedback, one component of coaching, was similarly associated with income (b = −0.5, standard error = 0.2, p < 0.05). Clinicians’ coaching fidelity was lower among families in exclusively English-speaking homes than for families who speak other languages (b = 18.4, standard error = 8.8, p < 0.05). Results suggest that associations between family characteristics and clinician behavior may be more nuanced than previously understood.
Lay abstract
There is a high demand for quality early intervention services for autistic children and their families. A key part of effective early intervention is teaching caregivers how to support their child’s development through caregiver-mediated interventions. However, in publicly funded programs, these strategies are often not followed correctly. Some studies suggest that family characteristics may influence how well clinicians apply these coaching methods. In this study, we explored the connection between family factors, like household income and language spoken at home, and the way clinicians coached families. We found that clinicians used coaching strategies less consistently with both lower- and higher-income families compared to middle-income ones. In addition, families that spoke only English at home received less consistent coaching than those who spoke other languages. These findings highlight the complex relationship between family background and how early intervention services are delivered, suggesting a need for further research.
Keywords
Early intervention (EI) services are critical to enhance autistic children’s outcomes (Fuller & Kaiser, 2020; Reichow & Wolery, 2009; Zwaigenbaum et al., 2015). Federal policy mandates that EI help caregivers support their child’s development (Individuals With Disabilities Education Act (IDEA), 2004). Caregiver-mediated interventions (CMIs) involve clinicians coaching caregivers to use strategies that foster children’s development. CMI improves children’s social skills and communication, and reduces disruptive behavior (Cheng et al., 2023; Hume et al., 2021).
In community-based studies of CMI, outcomes tend to be worse than in university-based studies (Brookman-Frazee et al., 2012; Green et al., 2022), at least in part because community clinicians are less likely to coach caregivers (Aranbarri et al., 2021; Pellecchia et al., 2022). When clinicians coach caregivers in the community, it is often with lower fidelity than observed in university-based studies (Pellecchia et al., 2022). Clinicians vary in their intentions to implement specific coaching components (Lawson et al., 2022; Pellecchia et al., 2024), with some used more than others (Pellecchia et al., 2023b).
Racially minoritized and socioeconomically disadvantaged autistic children have less access to and receive lower-quality behavioral healthcare than their White (Begeer et al., 2009; Liu et al., 2023; Magaña et al., 2012, 2013) and socioeconomically advantaged peers (Carr et al., 2016; Fountain et al., 2012). This may be in part due to clinicians’ perceptions, as well as the experienced barriers related to family characteristics and living conditions, that hinder CMI coaching (Straiton et al., 2021; Tomczuk et al., 2022).
The present observational study leverages data from a community-based trial of a CMI (Project ImPACT). We examined whether family characteristics were associated with clinicians’ use of caregiver coaching.
Methods
This study comprised a secondary analysis of data collected from a pilot randomized trial of Project ImPACT, a caregiver-mediated Naturalistic Developmental Behavioral Intervention (NDBI; Ingersoll & Dvortcsak, 2019). The parent study was approved by the City of Philadelphia’s Institutional Review Board (IRB) and involved the collaboration of EI agency partners. The trial design and results are published elsewhere (Pellecchia et al., 2023a). De-identified data have been submitted to ClinicalTrials.gov (ID: NCT04729127) and will be available following quality control review by the National Library of Medicine.
Setting
The parent study was conducted in publicly funded EI agencies during the COVID-19 pandemic. Project ImPACT sessions occurred via video conferencing for all families.
Project ImPACT
Project ImPACT is an evidence-based caregiver-mediated NDBI designed to teach caregivers strategies to help their child develop social communication skills during daily routines and activities (Ingersoll & Dvortcsak, 2019; Ingersoll & Wainer, 2013). The clinician training protocol is published elsewhere (Pellecchia et al., 2023a).
Participants
Participants included community EI clinicians and caregivers and children from the clinicians’ caseloads. Upon enrollment, children were less than 36 months of age and were either at high likelihood of or diagnosed with autism. Project ImPACT was delivered in English. All caregivers spoke English, and some families also spoke other languages fluently at home.
Measures and procedures
Clinician and family dyad characteristics measures
Participants completed demographic questionnaires. Age, education, racial/ethnic identity, household annual income, and language were provided categorically. Household size was reported as a continuous variable.
Outcome measures
Trained raters evaluated clinicians’ use of coaching strategies during sessions using two measures: Project ImPACT Coaching Fidelity Checklist (ImPACT Coaching Fidelity; Ingersoll & Dvortcsak, 2019) and the Parent Empowerment and Coaching in Early Intervention Caregiver Coaching Fidelity Tool (PEACE Fidelity; Pellecchia et al., 2020).
ImPACT Coaching Fidelity evaluates clinician adherence to Project ImPACT coaching procedures (Ingersoll & Dvortcsak, 2019). A total of 18 items are scored as 0.0 (not observed), 0.5 (partially observed but not to fidelity), or 1.0 (sufficient quality); items may also be scored as not applicable. We created weighted fidelity scores by multiplying scores for each item by a weight based on the intervention developer’s recommendations about the item’s relevance to high-quality coaching with Project ImPACT (e.g. providing positive coaching comments has a weight of 3, while setting an agenda has a weight of 1; for more details see Supplemental Table S1). ImPACT Coaching Fidelity overall score was the sum of the weighted fidelity scores, divided by total possible points, and multiplied by 100. The total maximum possible score depends on the specific items scored as applicable for a given session.
PEACE Fidelity is an intervention-agnostic measure of quality and use of caregiver coaching strategies in CMI (Pellecchia et al., 2023b; Supplemental Appendix S1). The PEACE Fidelity includes five subcomponents: collaboration, practicing in daily routines, demonstration, practice with feedback, and reflection with problem-solving. Its 25 items are scored across subcomponents on a 5-point scale, ranging from 1 (never observed) to 5 (almost always observed). The mean of all items scored is the PEACE Fidelity overall fidelity score (Pellecchia et al., 2020).
Video recording procedures
Fidelity for both measures was scored by trained research staff. Twenty percent of videos was double-coded. Mean inter-rater agreement was 87% for PEACE Fidelity and 94% for ImPACT Coaching Fidelity. Video recordings were collected after 8–12 weeks of Project ImPACT implementation.
Data analysis
Analyses were conducted using R version 4.1.2 (R Core Team, 2021). We examined family characteristics using descriptive statistics. Families’ reported racial and ethnic identities were categorized into one of two groups: “racially/ethnically minoritized families” or “White, non-Hispanic families.” Household language was aggregated into two groups: “exclusively English-speaking household” or “other languages household,” meaning a non-English language was spoken in the home.
We calculated descriptive statistics for both fidelity measures. Correlations between mean total scores and subcomponents of fidelity measures were computed as a basic assessment of construct convergence between the two measures (Campbell & Fiske, 1959; Strauss & Smith, 2009). Correlations between family characteristics and total scores were computed (e.g. Pearson r for continuous variables, point-biserial correlation rPbis for continuous-dichotomous variables; Shmueli, 2010). Multiple linear regressions models were computed for each measure’s overall fidelity score as functions of each family characteristic variable with covariates controlling for total hours in session and parent study group assignment (i.e. families were randomized into Project ImPACT for 1 or 4 h per week; see Pellecchia et al., 2023a). Given the exploratory nature of this study, correlations and multiple linear regression models were computed to assess preliminary associations (Shmueli, 2010).
We conducted analyses between family characteristics and PEACE Fidelity subcomponents. We estimated multiple linear regression models for each PEACE Fidelity subcomponent. We conducted PEACE Fidelity subcomponent analyses for family characteristics with statistically significant associations with overall scores. A subcomponent analysis for the ImPACT Coaching Fidelity was not appropriate because of parent study group assignment (Pellecchia et al., 2023a; Supplemental Appendix S2, Table S2).
Results
Clinician and family dyad characteristics
Table 1 presents clinician and family descriptive information.
Clinician and family characteristics.

Race/ethnicity reporting is non-exclusive, meaning summation of percentages maybe greater than 100%. Am.Indian/Alaska Nat. = American Indian or Alaska Native; Asian/NHPI = Asian or Native Hawaiian and Pacific Islander.
Certification Other includes Behavior Specialist, Applied Behavior Analysis.
Other Languages include Arabic, Cambodian, Haitian Creole, Laos, Russian, Spanish.
Clinicians
Twelve clinicians participated. Most had a graduate degree (n = 10, 83.3%) and were between ages 36 and 40 (n = 4, 33.3%). Five clinicians were Black (41.7%) and seven were White (58.3%).
Family dyad
We enrolled 34 family dyads, an average of two families (range = 2–4) from each clinicians’ caseload. Children were less than 36 months of age (mean age 23.8 months; SD = 3.4); most children were male (n = 22, 64.7%). Participating caregivers were predominately mothers (n = 29, 85.29%). Most families were Black (n = 18, 52.9%). Eight families (23.5%) reported speaking languages other than English in their homes. Most families reported an annual household income under $20K (n = 18, 52.9%).
Outcome measures
On average, coaching fidelity was low (ImPACT Coaching Fidelity score M = 56.9%, SD = 22.0; PEACE Fidelity overall score M = 2.6, SD = 0.6; Supplemental Table S3). Correlations between overall scores and fidelity subcomponents were generally moderate to high (Supplemental Table S4). ImPACT Coaching Fidelity and PEACE Fidelity overall scores were moderately correlated (r = 0.64, p < 0.01). ImPACT Coaching Fidelity overall score was moderately correlated with PEACE Fidelity in-vivo feedback and reflection & problem-solving (r = 0.56, p < 0.01). See Supplemental Table S4.
ImPACT coaching fidelity and family characteristics
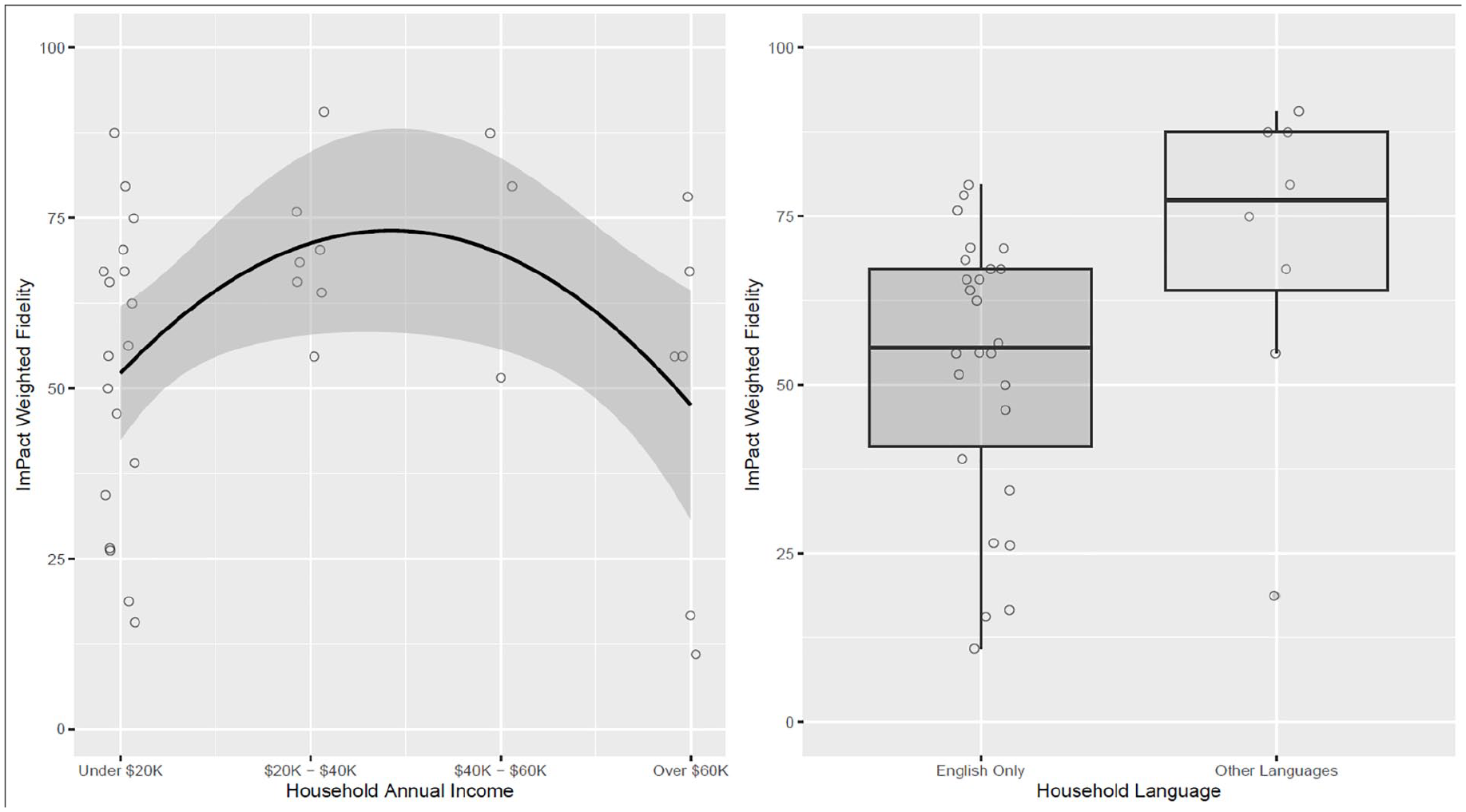
Correlations between ImPACT Coaching Fidelity score and family education, minoritized racial/ethnic status, household income, and household size were small and not statistically significant. The correlation between ImPACT Coaching Fidelity score and household language was low and statistically significant (rPbis = 0.34, p = 0.05). Visual inspection demonstrated a curvilinear relationship between ImPACT Coaching Fidelity score and household income.
Multivariate models did not demonstrate significant associations between clinicians’ adherence to Project ImPACT coaching and caregiver education, family racial/ethnic identity, or household size (Table 2). Household income and language were significantly associated with ImPACT Coaching Fidelity overall score (Table 2; Figure 1(a) and (b)). A multiple linear regression was estimated with household income as a quadratic term to better fit this relationship between household income and coaching fidelity. The association between household income and ImPACT Coaching Fidelity overall score was statistically significant, b = −10.4, standard error (SE) = 4.1, p < 0.05. The quadratic term for household income accounted for an additional 18% of the variance in coaching fidelity. Coaching fidelity was lower and more variable for households with income at or below $20K and above $60K compared to families with household incomes between $20K and $40K and between $40K and $60K. The association between household language and ImPACT Coaching Fidelity score was statistically significant, b = 18.5, SE = 8.8, p < 0.05; clinicians’ Project ImPACT coaching adherence was lower when coaching caregivers in households where English was the only language spoken.
ImPACT coaching fidelity overall score × family characteristics.
Fidelity overall scores × family characteristics multivariate linear regression results.

LL and UL indicate the lower and upper limits of a confidence interval, respectively.
p < 0.05; **p < 0.01.
PEACE Fidelity and family characteristics
PEACE Fidelity overall score
Correlations between PEACE Fidelity score and family characteristics were not statistically significant. PEACE Fidelity score was not associated with any family characteristics (Table 3).
PEACE Fidelity subcomponents × family characteristics multivariate linear regression results.

LL and UL indicate the lower and upper limits of a confidence interval, respectively.
p < 0.10; *p < 0.05; **p < 0.01.
PEACE Fidelity subcomponent scores
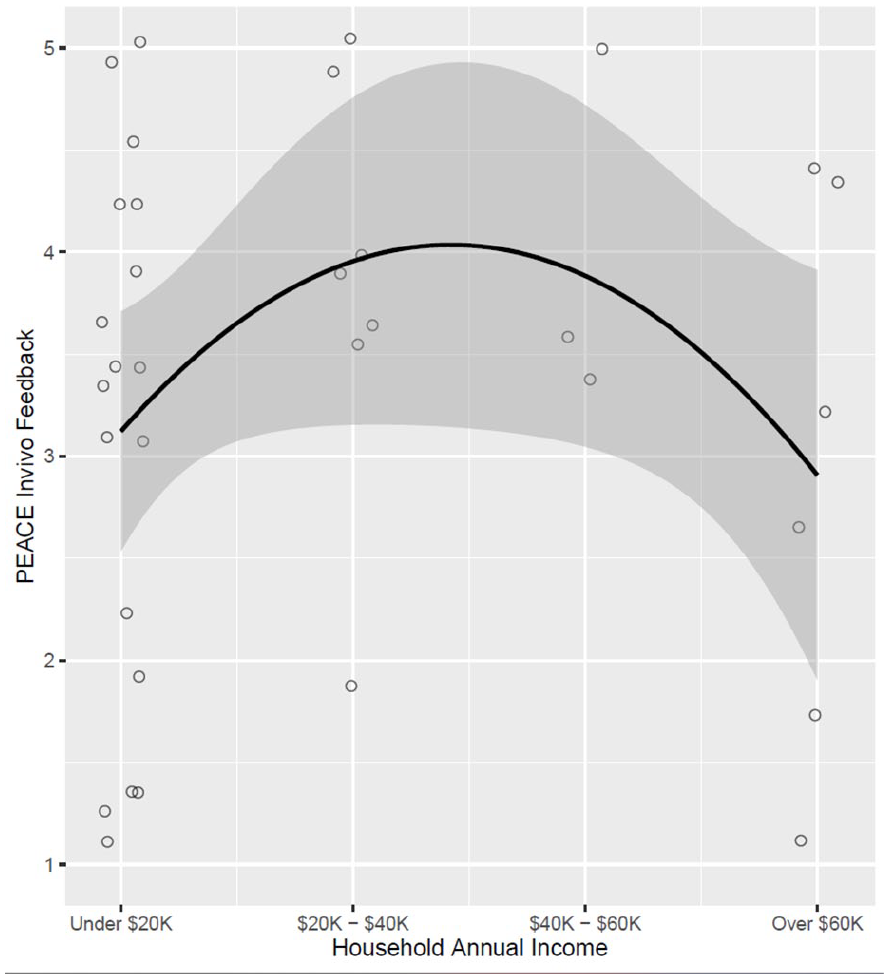
Subcomponent-specific models were run per each PEACE Fidelity subcomponent with household income and language (Table 3). The association between families’ household income and clinicians’ PEACE Fidelity in-vivo feedback was statistically significant, b = −0.5, SE = 0.2, p < 0.05, and demonstrated a curvilinear relationship (Figure 2). Neither household income nor language was associated with any other PEACE Fidelity subcomponents.
PEACE Fidelity in vivo feedback × household annual income.
For transparency and robustness check, significant results were computed without covariates (Supplemental Table S5; Simmons et al., 2011). Household income remained significantly associated with ImPACT Coaching Fidelity overall score, b = −10.3, SE = 4.1, p < 0.05. Other results were no longer statistically significant (p < 0.07).
Discussion
We found associations between household income and language with clinicians’ coaching fidelity. Families at the lowest and highest ends of the income range received less Project ImPACT coaching manual adherence than middle-income families, suggesting a more nuanced relationship than previously appreciated. A significant curvilinear relationship was similarly observed with PEACE Fidelity in vivo feedback and income. These results align with qualitative studies where clinicians report that challenges such as housing instability, food insecurity, and lack of play materials or other essential resources create barriers to coaching lower-income families (Straiton et al., 2021; Tomczuk et al., 2022). Low coaching fidelity among higher-income families may reflect clinicians perceiving reduced authority or a preference among these caregivers for clinician-directed sessions focused on their child, rather than caregiver-focused coaching.
ImPACT Coaching Fidelity overall scores were higher for families that spoke languages other than English. These results may stem from language differences between clinicians and caregivers that reduce casual conversation, allowing more time for coaching. While prior research highlights barriers such as challenges engaging caregivers and discomfort providing feedback to culturally and linguistically diverse (CLD) families (Stewart & Applequist, 2019), our findings present mixed results. This suggests a need for more expansive and mechanistic studies to better understand these associations.
ImPACT Coaching Fidelity and PEACE Fidelity overall scores and subcomponent scores were moderately and positively correlated (Supplemental Table S4), yet fidelity scores were differentially associated with family characteristics. In vivo feedback had both the highest mean score and the greatest variability (M = 3.32, SD = 1.26) among PEACE Fidelity subcomponents (Supplemental Table S4). It may be that the subcomponent-level PEACE Fidelity in vivo feedback presents with greater signal relative to other subcomponents (e.g. daily routines; M = 1.58, SD = 0.48). Differences in coaching fidelity at the subcomponent level are consistent with differences in intention to use different coaching components (Pellecchia et al., 2024).
This study is an exploratory analysis with a small sample size. Therefore, results should be interpreted with caution. Family characteristic variables were not selected a priori, limiting, for example, income ranges. Yet, household income association with coaching fidelity demonstrated consistency across ImPACT Coaching Fidelity score and PEACE Fidelity in vivo feedback.
Conclusion
We provide preliminary evidence that family characteristics and clinicians’ coaching fidelity are associated. This study responds to calls for more inclusive autism research by engaging and enrolling diverse, marginalized families, with the goal of advancing health equity (Machalicek et al., 2022; Maye et al., 2022; Straiton et al., 2024). Future research should collect more comprehensive family characteristic data. This study sets the stage for research to ameliorate and improve associations between family characteristics, circumstances, and clinicians’ caregiver coaching.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251317780 – Supplemental material for Short report: Associations of family characteristics and clinicians’ use of caregiver coaching in early intervention
Supplemental material, sj-docx-1-aut-10.1177_13623613251317780 for Short report: Associations of family characteristics and clinicians’ use of caregiver coaching in early intervention by Alyssa M Hernandez, Diondra Straiton, David S Mandell, Brooke Ingersoll, Samantha Crabbe, Sarah Rieth and Melanie Pellecchia in Autism
Footnotes
Acknowledgements
The authors thank the City of Philadelphia’s Early Intervention system leaders, clinicians, and the families they support for their participation, cooperation, and collaboration.
Author contributions
Data availability statement
The data supporting this article will be made available by corresponding author upon request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.S. is a Project ImPACT trainer and receives funding for training providers in Project ImPACT. B.I. is a co-developer of Project ImPACT. She receives royalties from Guilford Press for the sale of the curriculum and fees for training others in the program. She donates profits from this work to support research and continued development of Project ImPACT.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided through a research grant from the Eagles Autism Foundation. The first author is a scholar of the Health Policy Research Scholars program, a national leadership program supported by the Robert Wood Johnson Foundation.
Informed consent
The research study conducted received approval from the City of Philadelphia’s Institutional Review Board. The research team obtained informed consent from clinician and caregiver participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.