
Abstract
In France, patients’ right to take part in decisions regarding their health has been recognized by law since 2002. This legal recognition was the outcome of a long-standing call to allow all individuals to be “actors in their own health” and to co-develop their care pathway with the professionals involved. In practice, care pathways simultaneously intertwine both standardization and personalization dynamics, which involve different forms of professional-patient interaction. This article analyses the links between the organizational variables of care pathways, and the ways in which patients are involved in the management of their own pathway. To date, these links have received little attention in the management science and health literatures. We draw on material from a case study carried out in 2 French territories, combining the analysis of patient pathways with interviews conducted with professionals and carers. Building on this analysis, we propose a typology of patient profiles which distinguishes between their different forms of involvement in the development of their care pathway, based on its organizational characteristics.
Introduction
As of 4 March 2002 and the enactment of the Kouchner Law, France has officially recognized the individual and collective rights of patients, and particularly their role in the management of their health—something that was long overlooked. 1 “This legal recognition was motivated by patients’ desire for more autonomy and a greater say in decisions regarding their health – in line with the concept of empowerment 2 – and by the shift toward more balanced relationships with the medical profession”?. 3
The desire to rethink the patient’s role has gone hand in hand with growing awareness of the fact that the needs to take into account exceed the strictly curative management of the illness: they include other needs—prevention, therapeutic education, as well as social and medico-social needs—, stemming from the impact of the illness(es) and the associated dependence on the daily lives of patients. 4 The evolution of the very concept of “pathway” over the last 10 years reflects this situation: the concept of a (coordinated) “care pathway,” overseen by the primary care physician, has gradually been supplemented with the notions of “health pathway” and “life trajectory.” 5
Yet even with this broader scope, the concept of pathway appears ambivalent. On the one hand, a pathway-based approach implies considering each person’s situation as singular, due to the interactions between the illness and patients’ personal characteristics (age, gender, resources, life trajectory, etc.). It also involves taking into account a patient’s subjective perception, their “lived experience” of their situation,5,6 with a view to co-developing their pathway. On the other hand, the emphasis on organizing pathways better has led to the development of a protocolization of care, influenced by Evidence Based Medicine (EBM) approaches, following a standardization-of-care logic.7,8 Although the role of the patient appears to be more limited in this case, they nevertheless retain the ability to choose between the therapies proposed and/or to influence the way in which these therapies are performed.
In practice, the variable mix of standardization and personalization of care, depending on the situation, leads to different forms of engagement with the patient. 9 This article studies this hybrid practice, embedded in a complex and interactive process of pathway co-development. Although the singularity of each situation renders the quest for a standard model futile and unsuitable, we believe that studying this process closely can yield interesting results. This will enable us to identify the links between the organizational variables of a pathway, and the scope and nature of the patient’s role.
To shed light on this question, we draw on a theoretical framework at the interface between the management science and health literatures, on 2 themes that we wish to articulate: the analysis of health pathways,10-12 and the analysis of the ways in which patients are involved in building their care pathway.9,13-15
We document our approach by presenting a case study carried out in the Ile-de-France region (Paris and surrounding areas), which involved a qualitative analysis of the relationships between patients and professionals, based on interviews, participation in work meetings on the organization of care pathways, and the analysis of patients’ care pathways managed by a support framework or institution (CLIC [Local information and coordination center (Centre Local d’Information et de Coordination)], MAIA [Method of action for the integration of support and care services in the field of autonomy (Méthode d’Action pour l’Intégration des services d’aides et de soins dans le champ de l’Autonomie)], health network) or an EHPAD (Medicalized elderly care homes [établissement d’hébergement pour personnes âgées dépendantes]).
Our findings detail the way in which patients, carers and professionals cooperate around key activities in the organization of pathways that inextricably involve both health and social care: the determination of needs and their management, and the coordination of the effective provision of care and assistance.
Our study concludes with a typology of patient profiles, which reflects their role in the development of their pathway.
Part 1: Theoretical Framework
The theoretical framework underpinning our study is based on management analyses of health pathways and of the modes of patient participation.
Health pathways: Between standardization and personalization
Management analyses approach health pathways as the outcome of a production process involving the classic stages of design, production, assembly, and distribution.10-12,16 The first stage consists in defining the diagnosis and the care strategy, while the next 3 relate to its implementation. Production refers to the performance of the basic operations necessary for the treatment of the patient; assembly relates to the way in which they are sequenced; and distribution consists in ensuring the delivery of care and assistance to the patient. Each of these stages can involve a variable mix of standardization and personalization along a continuum in which one of these dynamics is prevalent.
Standardization stems from the Evidence Based Medicine (EBM) movement. 17 Striving to be as comprehensive as possible, EBM systematically analyses the most relevant recent bibliographical data on a given subject 18 to reduce diagnosis and treatment variations deemed “inappropriate.” 19 Personalization, on the other hand, is rooted in the very nature of care, informed by the infinite variety of expressions of patient needs. It has recently been bolstered by 2 developments: on a medical level, the emergence of so-called “personalized” medicine, as a result of advances in medical technology (imaging, molecular biology, genomics, etc.), which allows for providing “tailored” care; and on a societal level, patients’ desire for care that better respects their wishes. 17 These 2 developments have led to patients being given a greater say in the choice of therapeutic strategies—a trend that has been associated with the term “empowerment.” 15 Empowerment, identified by the World Health Organization as a way of giving people control over their own health, can be summed up by the call to “be an actor in one’s own health” or by the saying “No decision about me without me.” 3 It can materialize in numerous ways, ranging from the choice between several standard protocols, to the development of a personalized care pathway.
If standardization and personalization inextricably coexist within the health system and most often within each pathway, 20 how can we capture this variable combination in a synthetic way, and what can we deduce from this about the role of the patient?
Lamothe’s 13 analysis of in-hospital care pathways identifies 4 types, by order of complexity: pure standardization; segmented standardization; segmented personalization; and integrated personalization. Pure standardization refers to the least complex pathways, in which the therapies used correspond to a single specialized treatment required for a given pathology. At the other end of the complexity spectrum are the pathways of patients—in geriatrics for instance—whose overall treatment is comprised of several specialized treatments, which fit within the “integrated personalization” category. In segmented standardization, one specialized treatment is applied to serve a core function, and ancillary specialized treatments are added to this main treatment. In the second intermediate case—segmented personalization—, several specialized treatments, more than one of which can perform a core function, are applied and each of them is combined with one or more ancillary standardizable specialized treatments. Based on this typology, and after analyzing it, in Section 1.2 we present the (variable) level of involvement of patients in their care.
This approach departs from other analyses, in which patient involvement is linked to factors that are independent of the patient’s background. 14 For example, in the model provided by Carman et al, 21 the level of patient involvement depends on personal aptitudes (eg, education), the culture of the host organization, and societal norms. Depending on the orientation of these different criteria, patient engagement can be situated along a continuum, ranging from information to partnership and including 2 intermediate stages: consultation and collaboration.15,21 While the idea of fluctuation in a patient’s capacity to be an actor in their own care seems interesting, this model does not account for the articulation between the patient’s involvement and the type of care pathway they follow. Yet this appears to be one of the explanatory variables determining what they can decide or co-develop with professionals.
The spectrum of forms of patient participation: Contributions and limits of the analysis of in-hospital pathways
This articulation, between the patient’s involvement and the type of care pathway they follow, is captured by the work of Lamothe, 13 which posits that the patient’s participation is informed by the way in which their needs are identified and managed.
In pure standardization pathways, the patient’s needs are defined in a generic way based on their pathology, and care is protocolized. The patient’s participation is very limited due to the standardized nature of the treatment and the focus on a pathology and an organ. In segmented standardization pathways, the patient interacts with the different specialists, and the implementation of treatments ancillary to the main care requires their active participation. However, for the implementation of the main treatment—often a surgical operation—, the patient’s role remains passive (except upstream, in the decision to opt for the operation or not). In situations of “segmented personalization,” the patients suffer from a pathology that determines which department they are to be hospitalized in, but the other pathologies they have may influence the choice of treatment, unlike in segmented standardization pathways. The identification of the patient’s particular needs is a longer, multidisciplinary step involving interaction with the patient and between the professionals themselves. Moreover, depending on how the patient responds to the treatment, adjustments may be necessary, requiring their active participation. Finally, in integrated personalization pathways, the multi-dimensional nature of the issues at stake and the unpredictable evolution of the patient’s situation, due to their overall fragility, further compound the complexity of the care provided. The patients and their carers are very much involved by the professionals and, as with the previous type of pathway, their active participation in the various treatments is considered essential to their success.
Lamothe’s work thus sheds light on the link between a patient’s participation and the type of pathway in which they find themselves. Nevertheless, this analysis remains binary (active or passive patient) and does not detail the patient “profiles” behind these generic terms, particularly the actual substance of the role they play. It is also likely that this role is more extensive in the context of a health pathway than in an in-hospital pathway, in which an existing team takes charge of the patient.
The modalities of coordination between professionals described by Lamothe are moreover the same as those proposed by Mintzberg 22 for a professional bureaucracy: it relates to the standardization of qualifications, supplemented by ancillary methods, in particular mutual adjustment for personalized pathways. While this framing is suitable for an organization such as a hospital, where professional paradigm is dominant, 23 how fitting is it for the coordination in inter-organizational health pathways? The change of scale and the multiplicity of professionals involved, with diverse intervention rationales, mean that coordination has to be envisaged and organized following a different approach, while seeking effects similar to those induced by the mechanisms described by Mintzberg: the definition of responsibilities, the introduction of predictability in behavior, and the development of a shared understanding of situations.24,25 Depending on the case, the need for coordination can be met by the patient, possibly with the help of the health professionals involved, and/or by a dedicated coordinator in complex situations. The role of the latter is to provide a comprehensive and concerted response to a patient’s multiple and interrelated problems, which professionals all too often address in a fragmented and partial way. This is either because they apply a disciplinary or sectoral approach, 5 or, in certain complex situations, because the number of interactions is so high that it exceeds the resources that the health organizations involved can commit to providing. 11 Dedicated coordination can thus help to mitigate 2 risks associated with ordinary coordination in complex situations: the risk of choosing default solutions or lacking knowledge of existing systems (eg, resorting to emergency services, resulting in hospitalizations that could perhaps have been avoided); and the risk of burnout among carers, who are mobilized beyond their physical or cognitive capacity. 26
In the following sections of this article, we articulate these different analyses of the issues and modes of support surrounding health pathways, in order to characterize the role played by patients in the management of their care pathway.
Part 2: Methodology
Our methodology is based on a case study 27 which we present, before describing our data collection and analysis methods.
A case study of 2 territories
The practices of health professionals and patients were explored following the case study method which, as Yin 27 explains, allows for “understand[ing] complex social phenomena” by highlighting the “holistic and meaningful characteristics of real-life events.” The way in which the actors in the field perceive the role of the patient in the development of their care pathway and attempt to operationalize it in their practice is indeed a complex social phenomenon, given the multiple approaches and the difficulties encountered in implementing this operationalization. Our analysis is comprehensive, in the sense that we seek to “objectify the factors that explain the action and interaction” 28 between patients and professionals, by comparing the accounts shared by the actors with our own analysis.
We carried out our study in 2 areas of the Ile-de-France region: the 13th and 14th arrondissements of Paris, and the southern part of the Seine-et-Marne département. It focused on the implementation of the “e-parcours” program—a national program to disseminate digital coordination tools among health professionals—and on the analysis of the management of complex care pathways by CLICs, MAIAs, health networks, and an EHPAD.
The characteristics of our 2 territories differ significantly. The first is urban, densely populated (25 380 inhabitants per km²), and its population is aging. One of the major challenges it faces appears to be the organization of complex pathways for dependent and polypathological elderly patients requiring highly personalized care and repeated, long-term treatment. The south of Seine-et-Marne département, on the other hand, is very rural and has the lowest population density in the region (166 inhabitants per km2). The death rate from cancer and cardio-respiratory diseases is above average, and it has a higher prevalence of diabetes and mental health problems than the rest of the region. These unfavorable indicators underscore the challenges surrounding the coordinated and multi-professional organization of care, taking into account these multiple impacts (health, functional, social) of these conditions on the daily life of a patient (Source: Observatoire Régional de Santé d’Ile-de-France. Indicateurs Territorialisés de Santé).
Data collection and analysis
The collection of the material
Our data collection took place from October 2018 to March 2021, and consisted of interviews, participation in e-parcours project meetings, and the study of patient pathways.
Forty interviews were conducted during this period (The breakdown by territory and type of health professional is shown in the Appendix). The actors we met within the framework of the e-parcours project fit within 4 main categories: ambulatory care, health institutions, medico-social institutions (EHPAD, SSIAD [Home nursing service (Service de Soins Infirmiers A Domicile]) and support frameworks (network, MAIA, and CLIC or PAT [Territorial Autonomy Centre (Pôle Autonomie Territorial)]). The interviews, which were semi-structured, focused on the way in which these actors analyze the overarching issues surrounding care pathways in their territory. MAIA case managers, network actors and CLIC/PAT coordinators, as well as their managers—network and CLIC/PAT directors, MAIA managers—were also interviewed to identify the challenges associated with individual patient care.
Retracing the pathways of 19 patients, mainly dependent elderly people living at home, enabled us to analyze “real-life” professional/patient connections. We used the “traces” of the interactions and actions of the various stakeholders, including patients and their relatives, stored in the information systems of an EHPAD and several DACs (« Dispositif d’appui à la coordination » « Coordination Support Facility »): multidimensional analysis and orientation forms (Formulaires d’Analyse Multi-dimensionnelle et d’Orientation), reports on assessments carried out at patients’ homes, minutes and summaries of meetings, personalized care plans, emails about the situation exchanged between the various partners, etc. This study was authorized by the Commission Nationale Informatique et Libertés (CNIL, national commission for information technology) in January 2020.
Analysis of the material
The purpose of our analysis was threefold. First, it sought to grasp the way in which professionals involve the patient in the development of the different stages of their care pathway. What forms of cooperation do they mobilize? What difficulties do the professionals and the patients encounter and how do they potentially overcome them? Second, it seemed relevant to identify key actors in this process, whose intervention facilitates patient-professional collaboration, or practices that have the same effect. Finally, our study aimed to establish a typology of the modalities and forms of co-development of care pathways between patients and professionals, in order to refine the categories (active/passive) defined by Lamothe. 13
Based on the material gathered from the interview and meeting transcripts, we analyzed the different forms of cooperation that professionals establish with patients, along with the scope and substance of this cooperation, as they perceive it. We compared the professionals’ approach with that of 2 carers, who shed light on the respective roles of the professionals and the patients’ relatives, as well as their own. Retracing the timeline of patients’ pathways, following an approach similar to that of process studies, 29 highlighted the impact of the time factor on the development of cooperation (particularly the patient’s willingness to be helped). It revealed the substance of the interactions that make up such cooperation, as well as its evolving nature, punctuated by progress and sometimes setbacks.
Part 3: Results
In this section we draw on 2 examples of complex pathways (Mrs A., and Mr and Mrs B.) to illustrate the way in which patients and professionals co-develop the content and coordination of the care provided.
Patients’ interactions with carers and professionals in complex pathways: Presentation of 2 examples
The study of the pathway of Mrs A., a resident of the 13th arrondissement of Paris until 2018, began in June 2016, when she lost her husband. She was 70 years old and lived alone in her home. She suffered from parietal meningioma and primary progressive aphasia, which causes early cognitive problems. She complained mainly of memory impairment and wanted cognitive stimulation. Her daughter also wanted this for her mother and was likewise concerned about her social isolation. She wanted her mother to join the day-care center at the EHPAD near her home, and for her to receive assistance. Mrs A., who was initially reluctant, agreed to attend the day-care center and she integrated well. Weekly home help was also set up.
In March 2017, Mrs A. underwent emergency surgery to remove her meningioma. From late March to early August 2017, she was provided with temporary accommodation at the EHPAD for her convalescence. Quite quickly, Mrs A. no longer wished to stay at the EHPAD, but the professionals considered it too dangerous for her to return home, as she had limited awareness due to her health issues. A “managed” return home was eventually organized from 7 August 2017 to 7 August 2018: Mrs A. attended the day-care center every day and took her meals at the EHPAD in the evenings and on weekends. The home help was increased, with visits from the life assistants twice a day to take her to the EHPAD and back to her home, and Mrs A. was placed under guardianship.
On 4 and 7 August 2018, Mrs A. was admitted to the emergency services of a facility within the territory, due to worsening cognitive problems, and eventually had to be placed in an EHPAD near her daughter’s home.
The course of Mr and Mrs B.’s pathway reflects other ways of navigating the challenges surrounding the organization of complex pathways.
Mrs B., aged 89 at the start of her care, lived with her husband, who was her carer, at her home in the 13th arrondissement of Paris. They had no children. In June 2018, Mr B. was admitted to the emergency ward at the Pitié Salpêtrière Hospital. The CLIC coordinator was alerted by the hospital of Mrs B.’s isolation and went to her home. This visit was facilitated by neighbors, who introduced the coordinator to Mrs B. She initially refused support, but as her husband’s hospitalization was prolonged, she eventually agreed to receive home help. Mrs B.’s neighbors regularly helped out by managing issues with keys (making copies), liaising with the CLIC about the evolution of Mr B.’s health, and accompanying the coordinator on her visits. The home help was set up, here again with the neighbors support in orienting the carers and notifying the building manager about their visits. In August, Mr B. returned home as part of the “hospital at home” program (HAD, hospitalisation à domicile). The CLIC coordinator made an APA (Personalized autonomy allowance) application for Mrs B., and a few months later an assistance plan was drawn up. The neighbors confirmed to the CLIC that the assistance provided was going well and seemed sufficient for the time being.
Analysis of the dynamics at play in these 2 pathways
The challenges of determining choices of care: Adapting to the dynamics of a situation and reaching compromises
Mrs A.’s case illustrates the capacity of the care and assistance system to adapt to the particularity of individual situations and to offer personalized services with different levels of intervention, taking into account the patient’s express wishes and the dynamics of their situation. Mrs A.’s care, which initially followed a conventional route, evolved toward a “tailored” and more original pathway from August 2017 to August 2018, made possible by a joint effort by the EHPAD and the SAAD (home help service, Service d’aide à domicile) to adapt to her situation. The former set up a personalized service to secure Mrs A.’s return home and avoid admitting her into the EHPAD, which she did not want, while the latter changed the times of the carers’ visits in the mornings and evenings. In the interview with us, her daughter emphasized how much her mother appreciated the freedom that the EHPAD granted her, allowing her to attend the day-care center as she wished, without setting fixed times, and to switch freely between the day-care center and the EHPAD for her activities. She experienced this freedom as a manifestation of the active role she was able to maintain in her life choices. This example illustrates a process of co-development of care, giving Mrs A. a central role—though oriented by professionals—in determining the modalities of her care (up to the decision to place her in an institution).
The strategy for managing Mrs B.’s needs involved traditional methods, but their acceptance had to be negotiated: through her initial refusal, Mrs B. showed her desire to remain “in control” of her care pathway, but ultimately had to accept a compromise necessary for her to remain at home in the absence of her husband.
The dynamics of managing pathways: The delegation of the coordination function
While coordination is generally managed by the patient (or their carer), in simple pathways, in complex pathways 2 situations may arise. First, coordination may be entrusted to one or even several people, some of whom are professional coordinators and others “lay” coordinators, often people close to the patient, as shown with the example of Mr and Mrs B.′s neighbors.
These neighbors played a highly valuable role as informal coordinators. They introduced the CLIC coordinator and regularly updated her on the couple’s situation. Likewise, they facilitated the intervention of the home helpers, and provided a form of oversight of the assistance plan’s evolution and its alignment with the needs at hand. Finally, they acted as mediators between all the actors involved and Mr and Mrs B., facilitating interactions.
In the second type situation, which can sometimes arise, coordination is still delegated, but the provision of care is the responsibility of a single actor, as in the case of Mrs A. mentioned above, in which the EHPAD was responsible for coordinating with the SAAD.
In both cases (dedicated coordination and integrated care), the patient’s role in the implementation of their care appears to be limited, which is consistent with the observation that at face value, the levers to be mobilized—the time and knowledge of those involved—to ensure effective coordination exceed his or her capacities. The patient can nevertheless influence the way in which the professionals coordinate with one another and with him or her, either by reporting possible failures in coordination, or by requesting different arrangements that more adequately take into account his or her needs and constraints, or else by directly organizing certain aspects of the care.
Thus, in the various activities studied, the patient appears as one of several actors of their own pathway, most often negotiating their choices, in ways and with results that can vary. This points to the existence of several patient profiles, which we present and discuss below.
Part 4: Typology of Patient Profiles and Discussion
In the Table 1, we present different patient profiles, based on the characteristics of the patient’s pathway. This typology is informed by broader reflection than the conclusions drawn from the empirical material presented in the previous section, as it draws not only on the 19 patient pathways (including those of Mrs A. and Mr and Mrs B.) which we studied in detail, but also on our interviews and the meetings that we attended, which extended our reflection to less complex pathways.
Characterization of a patient’s profile according to their pathway. a

Reading aid: the patient profile includes both the patient themselves and their carer.
Our study points to 4 different patient profiles (ideal types): pilot patient, advised partner, assisted partner, and piloted patient. In Table 1, we associate these profiles with examples of health issues characterizing pathways of increasing complexity [We have already used these pathway examples in previous studies, to distinguish between cases based on a fee-for-service approach and those following a pathway approach, and to characterize the issues involved in defining the modes of care and coordination of pathways according to the situation 30 ). We distinguish between acute one-off episodes (eg, a fracture, a flu), which are conceived of and treated without situating them within a broader timeline, and situations that fit a pathway logic, as they are considered to unfold over time. We provide 3 archetypal examples illustrating the latter: a chronic illness with a simple pathway and no associated complications, which therefore lends itself to fairly standardized care; a complex situation involving both health and social issues, the treatment of which is not determined from the outset (complex evolution of a chronic illness, loss of autonomy at home); and finally, a very complex situation involving multiple, severe, interrelated and highly evolving issues (an elderly person living at home with a significant loss of physical and mental autonomy or in an EHPAD). We describe the role of the patient in the 2 levels, mentioned above, of determining the care strategy and implementing it.
In the simplest cases (acute episode), we consider that the patient is the pilot of their pathway, insofar as they are free to choose to consult one or more professional (or not) to discuss the different existing care options, and to choose one or more of these options, which they implement autonomously (by choosing the professionals, scheduling appointments, etc.). Although the room to maneuver may be limited as the care is often standardized, the patient remains free to opt for this care or not and to organize the practical aspects. The “pilot patient” can thus be considered as a conductor who mobilizes and articulates the different resources (care and services) of the health system.
In the case of a chronic illness with a simple trajectory, the discussion on the care strategy, which unfolds over the long term, is enriched by the patient’s feedback on the evolution of the illness, the effects of the treatment, and possible alternatives. The patient/health professional relationship thus becomes a partnership, with the professionals’ role consisting in analyzing this feedback, advising the patient on possible adjustments to the care, and helping them to implement these adjustments. The situation nevertheless remains sufficiently “simple” for the patient to self-manage and steer their own care.
In more complex cases, where the situation calls for collective reflection by the patient and the professionals to identify and prioritize needs, determine a care strategy, implement it, and adapt it whenever necessary, managing the pathway requires the intervention of a dedicated coordinator. The coordinator will help the patient to express their needs and choose a course of action, and then to implement it. In such cases, the patient goes from being an autonomous partner to being an assisted partner retaining the ability to choose, and the pathway is co-managed with a complex-pathway coordinator.
In cases where the patient is highly dependent, particularly on a cognitive level, the management of the care pathway is delegated entirely to a dedicated coordinator, who becomes the primary point of contact for health professionals. The patient is consulted on a regular basis, but is accompanied (or “steered”), either at home or in an institution, within the framework of their life project.
These profiles are ideal types that can rarely be observed “in their pure form” in practice. A patient may present different facets, varying over time and depending on the person with whom they are speaking. As the patient moves through the various stages of the pathway and as their life evolves, they may switch from one profile to another. Thus, Mrs A. went from being a partner patient of the professionals at the beginning of her illness, to being a piloted patient following the aggravation of her illness, the deterioration of her cognitive faculties, and the associated loss of autonomy (which is also translated into her being placed under guardianship).
The shift from advised partner to assisted partner is indicative of a person’s situation deteriorating. It is important to identify this deterioration in order to prevent a possible breakdown in the care pathway, which often leads to the intervention of a dedicated coordinator. In one of the territories that we investigated, primary care professionals systematically offer people aged 75 and over a multidimensional assessment of their situation (health and social), in order to set up assistance, if necessary and with their consent, to ensure that they can continue to live at home. This type of initiative certainly warrants the support of public authorities (which is the case in this example). In addition to their beneficial effects for patients, who see their autonomy and ability to manage their care pathway increase, such initiatives allow dedicated coordinators to focus on the most complex situations, which are often time-consuming and require significant support and coordination. Guided by this philosophy, the French state has decided to introduce preventive consultations at 3 key ages in life, including one at the age of 60, with a view to detecting the shift from one patient profile to another as early as possible.
Conclusion
Our article summarizes and expands the existing literature on the ways in which patients participate in their care, with a typology of patient profiles that articulates the degree of complexity of the care pathways, the types of care practised, and the nature of the patients’ involvement. We show that being an actor in one’s own care pathway is not just a matter of individual will (the patient’s desire to be involved, and the professionals’ willingness to give them a place); it depends on the organizational characteristics of the pathway itself, which largely determine the “realm of needs and the realm of possibilities” for both the patient and the professionals concerned. The pilot patient, the advised partner, the assisted partner and the piloted patient are thus profiles of forms of pathway organization, as much as they are the manifestations of personal positions. Fostering the development of patient participation therefore involves identifying the issues at stake for each type of pathway, with a view to then defining participation methods tailored to these issues.
These initial findings call for further research. Our study mainly focused on complex pathways, most often of elderly patients with moderate to severe loss of autonomy. It would be useful to complement this analysis with an in-depth study of other pathways, to enhance the validity of the results (particularly in terms of the identification of types of participation) or to establish the scope of their validity. Additional interviews with patients and carers would also allow us to better grasp the nature and content of their interactions with the professionals involved, which in our study we approached solely through the prism of the information recorded in the patients’ files and our interviews with professionals and carers. Finally, the dynamics of the co-development of a care pathway could certainly be investigated in greater depth with long-term studies of care pathways, showing the transformations in the patient-professional relationship over time. Much remains to be explored in order to further our understanding of the different facets of the patient’s role and all the learning we can derive from them, both academically and empirically.
Footnotes
Appendix
Interviews carried out on the territory of the south of the Seine-et-Marne département.
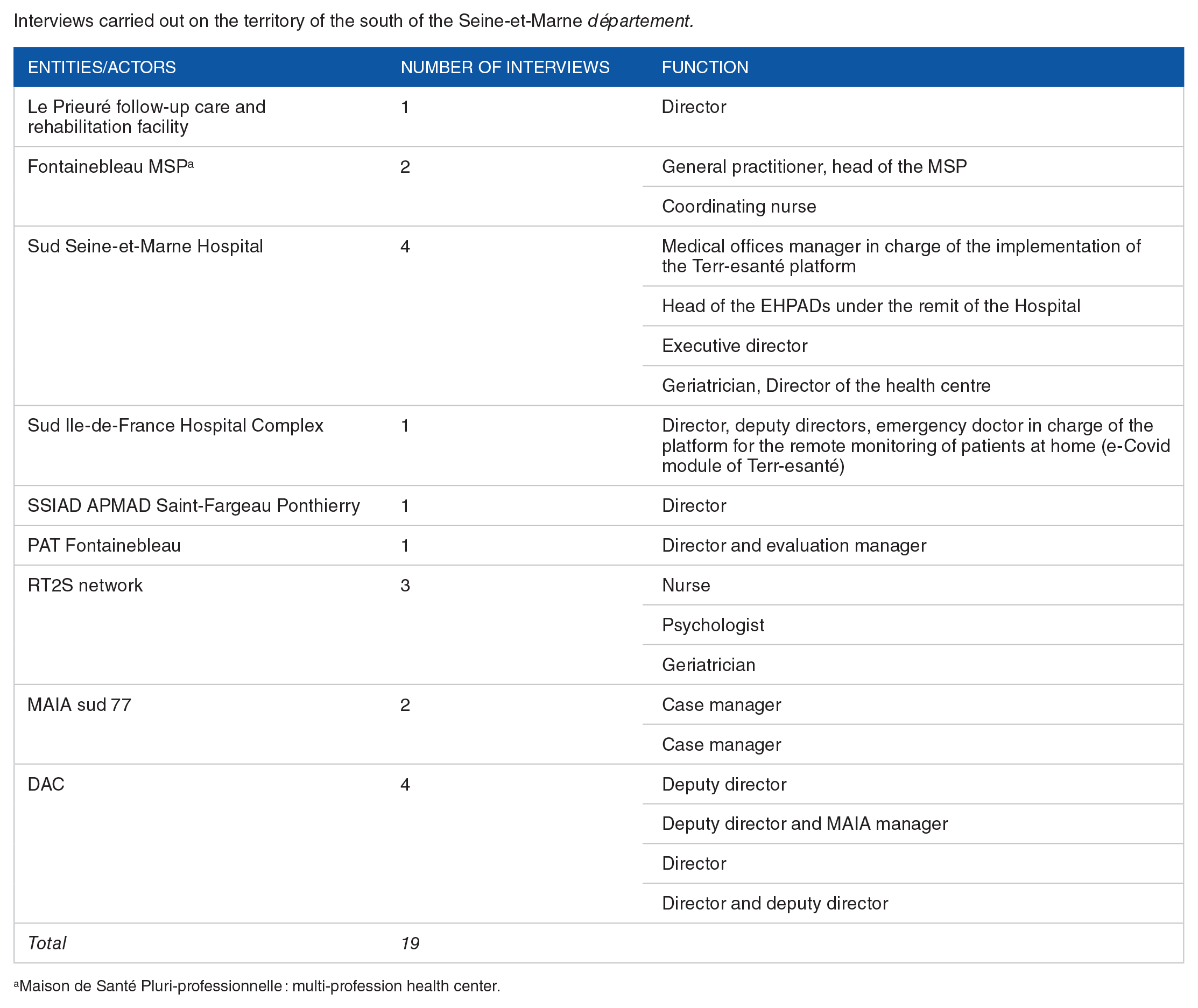
| Entities/actors | Number of interviews | Function |
|---|---|---|
| Le Prieuré follow-up care and rehabilitation facility | 1 | Director |
| Fontainebleau MSP a | 2 | General practitioner, head of the MSP |
| Coordinating nurse | ||
| Sud Seine-et-Marne Hospital | 4 | Medical offices manager in charge of the implementation of the Terr-esanté platform |
| Head of the EHPADs under the remit of the Hospital | ||
| Executive director | ||
| Geriatrician, Director of the health centre | ||
| Sud Ile-de-France Hospital Complex | 1 | Director, deputy directors, emergency doctor in charge of the platform for the remote monitoring of patients at home (e-Covid module of Terr-esanté) |
| SSIAD APMAD Saint-Fargeau Ponthierry | 1 | Director |
| PAT Fontainebleau | 1 | Director and evaluation manager |
| RT2S network | 3 | Nurse |
| Psychologist | ||
| Geriatrician | ||
| MAIA sud 77 | 2 | Case manager |
| Case manager | ||
| DAC | 4 | Deputy director |
| Deputy director and MAIA manager | ||
| Director | ||
| Director and deputy director | ||
| Total | 19 |
Maison de Santé Pluri-professionnelle : multi-profession health center.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Ile-de-France’s Health Regional Agency for the research presented in this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to and approved the final manuscrit. IA led the conceptualization, analysis and writing of the manuscrit. JCS and FK contributed to the data analysis, the shaping of the typology of patient profiles and its discussion. All authors revised the final draft of the manuscrit.