
Abstract
The COVID-19 pandemic has challenged the capacity of health systems in various countries. This study was designed to evaluate the response rates of hospitals in the prevention and control of COVID-19 in Hamadan province, Iran. In this cross-sectional study, all 20 hospitals in Hamadan province were monitored in February 2020. The instrument used in this study was the WHO checklist, entitled “Infection prevention and control health-care facility response for COVID-19.” In each hospital, the hospital infection control officials completed the checklists under the supervision of the hospital managers and were then provided to the project manager. Data analyzed by SPSS 22 software. There were 3482 hospital beds (the average beds of each hospital was 174) in the studied hospitals. Of 15 055 patients admitted to all hospitals, 2196 (14.6%) individuals were COVID-19 patients. The total average score obtained from the checklist was 62.25. Among 7 domains studied, the lowest scores belonged to 2 domains of “infrastructure and equipment” and “patient screening and triage.” The scores of domains “IPC programs” and “visitors” were significantly higher in hospitals with ICU beds than other hospitals (P-value = .03 in both domains). A comparison between university-teaching hospitals with other hospitals and those in Hamadan city with other cities revealed no significant differences in any of the domains. The mean response rate (62.25) of hospitals in terms of COVID-19 in Hamadan province indicates their relative readiness to prevent and control the COVID19 pandemic. The shortage of infrastructure and equipment and screening and triage problems of patients were the main challenges of hospitals in managing the COVID-19 pandemic in Hamadan province, Iran.
Background
At the end of 2019, the outbreak of the COVID-19 pandemic posed a significant threat to the health system in many countries worldwide. From the outset of this pandemic, countries with inefficient health systems were at high risk for the disease.1-4 During its short period, the incidence of COVID-19 revealed many shortcomings and inadequacies in health care services worldwide. 5 In the field of hospital care, the disease leads to hospital stay and hospitalization in the intensive care unit (ICU) in 15% and 5% of cases, respectively. Hence, it was initially clear that hospitals could not admit this number of patients in most countries of the world. To deal with this shortcoming, patient admission policies have been changed in many countries that focus on the non-admission of elective patients to evacuate hospital beds for COVID-19 patients. Moreover, the establishment of field hospitals, using private hospitals against COVID-19, and using the maximum capacity of the health system workforce are the other strategies that have been considered to deal with this emerging virus in different countries. 6 The increase in the health system capacity in dealing with COVID-19 can be scrutinized from 2 aspects. The first includes infrastructure facilities such as increasing manpower, equipment, and facilities, and the second includes the proper response of the health system, the use of updated guidelines and instructions, and using effective technologies to deal with this pandemic. 7 The World Health Organization has underlined the need for accurate information in the management of this disease in different countries. 4 The urgent need for obtaining data in this pandemic highlights the importance of data security, patient satisfaction, and ethical codes required in research under normal circumstances. Therefore, these factors are recommended to be regarded as bureaucratic barriers that postpone access to data in the current conditions. 8 Unfortunately, many countries around the world have challenges in access to up-to-date and accurate data on the capacity and facilities to fight this epidemic. In this respect, according to the WHO, only a few countries provide accurate and up-to-date information on their health system capacity about this disease. To respond to this need, the WHO has published a monitoring tool entitled “response rate for the prevention and control of COVID-19 pandemic.” This tool can improve the facilities and conditions of various health departments against COVID-19. The WHO recommends the use of this tool to monitor the care of COVID-19 in various medical centers, particularly hospitals. 5 Given the importance of using such a valid and practical tool in monitoring the management of COVID-19, this study was designed to evaluate the response rate of hospitals in the prevention and control of the COVID-19 pandemic in Hamadan province, in order to be able to provide an estimate of the general situation of Iranian hospitals in this regard.
Methods
This descriptive-analytic cross-sectional study was performed in all 20 hospitals of Hamadan province in February 2020. For this purpose, we used the checklist of the WHO entitled “infection prevention and control health-care facility response for COVID-19” as a monitoring tool. The checklist evaluates and monitors hospitals in 7 domains: IPC (Infection Prevention & Control) program, IPC guidelines and standard operating procedures, IPC training and monitoring, screening, triage, early recognition and testing of COVID-19, built environment, infrastructure and supplies, visitors and maintaining IPC interventions. The World Health Organization checklist states that a calculated score should be reported for each of the 7 domains as well as overall. 5 In each hospital, the hospital infection control officials completed the checklists and provided them to the project manager. To assess face validity, we sent the Persian checklist along with the original text to all scientific focal points and other project collaborators (5 people). Then, we asked them to express their comments on the compatibility of the Persian translation with the English text. The final version of the Persian checklist was prepared by summing the comments. The reliability of the checklist was evaluated by the inter-rater reliability method in 2 teaching hospitals in the province. To do this, we evaluated the results of the 2 separate checklists, which were completed simultaneously and independently in the same hospital, using the project focal point and the infection control official of the 2 hospitals. The reliability of the checklists was evaluated based on the coefficient of concordance between the 2 people. In this study, a calculated kappa = 0.804 between the 2 researchers indicated a high value and good reliability of the checklist.9-11 The research checklist had 25 questions, each scored based on a 3-point Likert scale, include +3, +2, and +1, which indicate complete fulfillment, partial fulfillment, and non-fulfillment of the objectives of the question, respectively. Accordingly, the minimum and maximum points obtained from the checklists were 25 and 75 points, respectively. Data were extracted from the checklists and analyzed using the SPSS 22 software based on the descriptive and analytical objectives of the project. For comparisons between 2 groups, independent sample t-test (for normally distributed data) or Mann-Whitney U tests (for non-normally distributed data) were used respectively. This research was registered in the ethics committee of the Research and Technology Vice-chancellor of Hamadan University of Medical Sciences (the ethics ID: IR.UMSHA.REC.1399.805). Hospital information was published in groups without mentioning the names of hospitals.
Results
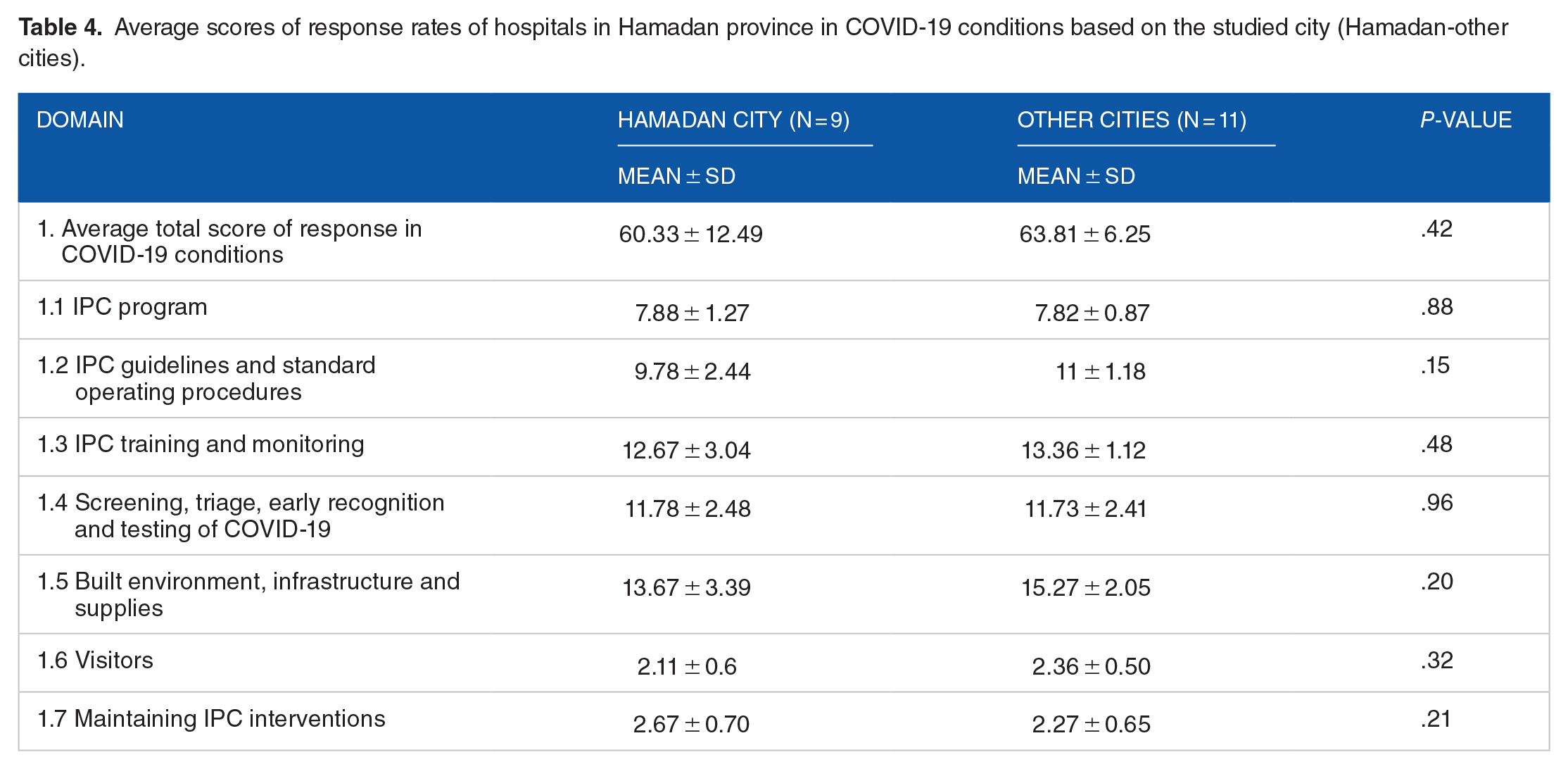
In this study, 20 hospitals were surveyed in Hamadan province. There were 3482 hospital beds in the 20 hospitals (174 beds on average with minimum and maximum of 32 and 540 beds, respectively) in the studied hospitals. Generally, 15 055 patients were admitted to all studied hospitals during the study period (1 month), 2196 (14.6%) of which were COVID-19 patients. Having 15 055 patients admitted at the study period, the average number of patients admitted to the hospitals per 100 hospital beds was 432.36 patients per month during the study period. Also, the average number of admitted COVID-19 patients was 63.06 per 100 hospital beds. On average, 58.99 beds (minimum of 0 and maximum of 180 beds) were allocated to COVID-19 patients. At the time of the study (February 2020), the average number of hospital beds (174 beds) and the average number of COVID-19 beds (59 beds) shows that only 34% of hospital beds were allocated to COVID-19 patients in Hamadan province. ICU beds were found in 15 (75%) of the studied hospitals with 13.6 ICU beds on average (minimum of 3 and maximum of 53 beds) in the studied hospitals, all (100%) allocated their beds to COVID-19 patients at the time of the study. Of the total hospitalized patients, 516 subjects died during the study month (a mortality rate of 3.42%). Besides, 284 out of 2196 hospitalized COVID-19 patients died within this month. The fatality and overall mortality rates of COVID-19 were 12.93% and 1.88%, respectively. The average total score of the response rate of hospitals for the prevention and control of COVID-19 disease was 62.25 (minimum 35 and maximum 72 points). Table 1 lists the average scores in the 7 domains. Hospital response conditions were examined separately for university-teaching hospitals (5 hospitals) and other hospitals in the province. In most items, university hospitals gained a better average score than other hospitals, but the differences were not statistically significant (Table 2). In this study, ICU beds were available in 15 hospitals and were absent in 5 hospitals of the province. Table 3 compares these 2 categories of hospitals in terms of response rates in COVID19 conditions. According to the table, the average scores of hospitals with ICU beds were higher than those without ICU beds in almost all domains except screening and triage. However, this difference was only significant in the domains of “IPC program” and “visitors” (P = .03) and after correcting the P value by the Bonferroni correction test, these 2 domains were not significant either. Finally, the response scores of hospitals in Hamadan province in COVID-19 conditions were examined separately in the province’s cities and for both domains of “hospitals in Hamadan city” and “hospitals in other cities.” In most of the domains, hospitals in cities of the province gained higher scores than those in Hamadan city (Table 4).
Average scores of response rates of hospitals in Hamadan province in COVID-19 conditions based on 7 studied items and 25 different areas.

Average scores of response rates of hospitals in Hamadan province in COVID-19 conditions based on the type of hospital (university-teaching with other hospitals).

Average scores of response rates of hospitals in Hamadan province in COVID-19 conditions by the presence or absence of ICU beds in the studied hospitals.

Significant level is considered as P < .007 according to Bonferroni correction test.
Average scores of response rates of hospitals in Hamadan province in COVID-19 conditions based on the studied city (Hamadan-other cities).
Discussion
Effective management of the COVID-19 pandemic in hospitals has a key role in disease control in the current situation of its widespread outbreak. This issue is so important that the WHO has designed a checklist and used various tools to encourage hospitals to self-evaluate the interventions made to prevent and control the COVID-19 pandemic. The tool used in this research was the World Health Organization checklist. This checklist has been used in other studies as well 12 or it has been cited in other studies.13-15
In the present study, 20 hospitals in Hamadan province of Iran were examined to evaluate the response in COVID-19 conditions. The average total response score of the hospitals in the province was 62.25 points (minimum of 35 and maximum of 72), about 13 points less than the maximum achievable (75 points), suggesting the relative readiness of hospitals in the prevention and control of the COVID-19 pandemic in the province. Considering 7 different domains, the hospital infrastructure and equipment domain gained the lowest score (an average of 14.55 out of 18 points) compared to the other domains, suggesting the inadequacy of hospitals in this regard for managing the COVID-19 outbreak. The screening, triage, and early detection (an average of 11.55 out of 15 points) gained the second lowest score, indicating of the weak screening and triage programs of the studied hospitals.
The lack of readiness of hospitals against COVID-19 has been addressed in many studies. For instance, Zeenny et al reported the readiness of hospitals to deal with COVID-19 in only half of the hospitals in Lebanon. Meanwhile, shortages of medicines and supplies, rising prices, and delays in receiving masks and disinfectants were among the reasons for the lack of readiness of hospitals against COVID-19. 16 In a review study by Al Thobaity et al in hospitals of 5 countries (ie, China, USA, Iran, Australia, and Spain), the authors concluded the lack of a disaster plan to deal with the epidemic in most hospitals. Lack of nursing staff, personal care facilities and equipment, and shortage of hospital beds account for major problems in caring for COVID-19 patients in most countries of the world. 17 In line with the studies by Zeenny and Al Thobaity, our study recorded an average score of 14.55 (out of 18 points) for infrastructure and the required equipment for the hospital. These results suggest the absence of items such as hand hygiene or providing other means of infection prevention and control, including the distribution of masks among clients.16,17 Contrary to the study of Al Thobaity, Noh et al articulated the experience of South Korea as one of the countries that have limited the COVID-19 epidemic by adopting appropriate strategies to combat the COVID-19 pandemic in the context of a model called Swiss cheese model.
From the beginning of the epidemic, wearing masks were made mandatory for hospital staff and visitors in this country. Moreover, the gate screening policy became obligatory in the triage of all hospitals and hospital gates, and the RT-PCR screening test was extensively provided to hospitals. In addition to all these activities, telemedicine was launched for COVID-19 consultation to reduce the burden of face-to-face visits in areas of disease outbreaks. Researchers believe that the introduction of this layered model led to the successful control of the epidemic in South Korea. 18 In the present study, contrasting the study of Al Thobaity, the domains of screening and triage of patients in hospitals of Hamadan province was one of the poor domains in the management of the COVID-19 crisis. According to the above points, the shortage of personal protective equipment (PPE) and medicine, which is in the infrastructure and equipment domain, was one of the problems of hospitals in managing the COVID-19 outbreak in the Hamadan province. In a recent study on the “shortage of essential drugs in the COVID-19 epidemic” by Farrell et al, researchers acknowledged that the problem of providing the required COVID-19 drugs, in particular those used to induce anesthesia and intubation, and antibiotics used in critically ill patients, are the major problem in hospitals in most parts of the world. In addition to deficiencies in the provision of PPE and other essential equipment such as ventilators, the abovementioned shortages have further complicated the treatment process of COVID-19 patients. 19
The shortage of PPE and the resulting problems for hospital staff have also been highlighted in a systematic review conducted by Fernandez et al, 20 in which the shortage of PPE in hospitals and uncertainty about the success of these devices in preventing infection were some factors exacerbating nurses’ anxiety. Unlike most existing articles on the COVID-19 pandemic focusing on the lack of facilities and diagnostic tools for the disease, Pezeshki et al conducted a systematic review on the overuse of medical facilities and equipment during the COVID-19 epidemic in Iran. Reviewing 41 articles (18 on treatment and 23 on diagnosis), they concluded that almost all articles highlighted the overuse of medical devices and tools in managing this crisis. Among these studies, overuse of antibiotics (31%-97%), MRI (33%-88%), and CT scan (19%-50%) were the most common types of overuse.
Finally, researchers have suggested that the COVID-19 epidemic is an opportunity for health policymakers at the national level to reconsider and explain their policies in controlling and preventing unnecessary services. 21 As mentioned, the screening and triage domain was also among the weak cases in managing COVID-19 patients in hospitals of Hamadan province. In contrast to this finding, Gupta et al shared successful experiences with the COVID-19 pandemic in their hospitals. The most important reasons were responsive and effective leadership with rapid response, an infection surveillance system with screening and testing at the hospital gate and the emergency department, widespread use of PPE, strict observance of social distancing, redistribution of hospital beds to increase the capacity of hospitalization beds for COVID-19 patients, strict observance of criteria for testing, and examining suspicious people. 22 In this study, the COVID-19 surveillance was in the subset of guidelines and procedures, which obtained a score of 10.45 (out of 12). This score indicates the relatively good activity of the hospitals of this province in this field. Contrary to our observations, a study on “epidemiological surveillance to control COVID-19: types, challenges, and application” in Saudi Arabia showed a poor epidemiological surveillance system in developing countries. The most important reasons for such poor performance were the shortage of facilities and adequate training. The report also points to 2 other hospital problems in the COVID-19 epidemiological reports, including the absence of timely reporting and incomplete reports of disease cases. 23 The establishment of isolated sites and isolation of patients with COVID-19 is also an effective measure in the disease prevention and spread, which was addressed as an essential item in the infrastructure and equipment section.
Our study obtained a relatively low average score of hospitals in this item in the province. Considering the situation of Iran as one of the countries with the highest daily statistics of infection and death due to COVID-19, Sharifi et al investigated the effects of different scenarios of social distancing and isolation conditions of patients on disease control in the country. Their study included different scenarios in which 0% to 40% of patients were involved. They concluded that epidemic conditions and death rates in the country would be controlled within the next few months only under the isolation scenario of 40% of patients. Furthermore, other scenarios emphasize a continuously increasing trend of patients and mortality. 24
In the continuation of the study, the examined hospitals were compared 2 by 2 in different groups including with and without ICU ward, teaching and non-teaching hospitals, and center and non-center of the province hospitals. Despite higher scores obtained in many domains in teaching hospitals than non-teaching hospitals, there were significant differences in none of the domains. Comparing hospitals with and without ICU beds revealed a preliminary significant difference only in 2 domains (infection control and prevention programs and hospital visitors) and after correcting the P value by the Bonferroni correction test, these 2 domains were not significant either. The impact of ICUs on managing the COVID-19 epidemic has been noted in Uppal et al 25 study in New York as well.
In general, hospitals with ICUs and ICU departments are more sensitive to infection control, and focal points or IPC professionals play a more active role in these hospitals. Several studies also point to the role of the ICU in better infection control. Also, infection control guidelines are implemented better in ICU departments, for example, in Alhazzani et al’s 26 study in Saudi Arabia, the importance of using evidence-based recommendations in the management of Covid-19 in ICU departments is mentioned.
Regarding hospital visitors, it should be mentioned that ICU departments are more sensitive to the screening of patients for Covid-19 at the entrance of the department and have better protocols to limit the direct visits of patients in the ICU departments or have virtual visits instead of face-to-face visits.27,28 Jamaati et al proposed a model for managing the COVID-19 crisis at Masih Daneshvari Hospital in Tehran as one of the major centers for the admission and treatment of COVID-19 patients. This model considers items such as increasing staff awareness about COVID19, changing the use of different parts of the hospital, including changing the ICU of tuberculosis patients to the ICU of COVID-19 patients, canceling all elective surgeries in the hospital, increasing patients’ triage units from 1 to 3 cases, and allocating maximum possible beds to COVID-19 patients. Along with these measures, the use of complete PPE (including masks, double-layer gloves, goggles, eye shields, and surgical gowns) was made mandatory for all personnel. According to the researchers, the model was helpful in the better management of COVID-19 disease in the hospital and better crisis management. 29
Limitations of the study: “This study had some limitations including the relatively small sample size, limited to the only one tool for its measurements (WHO checklist) and focus on the one province of Iran (Hamadan) instead of all over the country. The limitations were mainly due to time constraints, and implementation of the research in defined geographic areas.”
Conclusion
In this study, an average response rate of 62.25 for hospitals in COVID-19 conditions in Hamadan province indicates the relative readiness of hospitals in the prevention and control of the COVID-19 pandemic in the province. Overall, the shortage of infrastructure and equipment and screening and triage problems were the significant challenges of hospitals in managing the COVID-19 outbreak in Hamadan province.
Footnotes
Acknowledgements
The authors would like to appreciate the Vice Chancellor of Research and Technology of Hamadan University of Medical Sciences for their support.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors confirm their responsibility in the study design, data collection, analysis and interpretation of results and all authors contributed to approving the final manuscript.