
Abstract
Diabetic foot ulcers (DFU) are a prevalent and severe disease with vascular and/or neurological complications, and if not diagnosed and treated promptly, it may rapidly deteriorate. Despite amputation or nonamputation treatment, there is still a high rate of re-ulceration. Previous studies have shown that the recurrence rate varies from 43% to 59% after 2 years. Currently, there is still a high rate of lower extremity amputation intervention, particularly above-the-ankle amputation, at Cho Ray Hospital in Vietnam, reaching 50%. The effectiveness of this intervention in the long term based on re-ulceration has not been evaluated in Vietnamese diabetic patients (DPs). This study aims to describe the long-term outcomes of amputation intervention in Type 2 DPs after 24 months and identify factors related to DFU recurrence in order to improve DFU management in low-middle-income countries like Vietnam. From January to June 2022, archived clinical and direct visit or phone follow-up data were collected and analyzed from diabetic foot ulcer patients with low extremity amputation who were treated at Cho Ray hospital from 2018 to 2020. The high re-ulceration rate in the 24th month was 29.8% (17/57), and the factor related to this outcome was “late diagnosis and care” (32.4 days vs 26.9 days with P = .03). Other potential factors (higher rates but no significant statistical difference with P > .05) included failure of HbA1c control greater than 9% (82.5% vs 67.5%), the severity of foot ulcers with TEXAS 3B (82% vs 60%), the number of years having diabetes (8.7 years vs 6.7 years), loss of monofilament sensation (82.5% vs 70.6%), and a history of diabetic foot ulcer (17.6% vs 10%). The re-ulceration after 24 months might depend on various clinical factors. Therefore, early diagnosis and care for diabetic foot ulcers could help reduce amputation rates and the risk of re-ulceration.
Introduction
Diabetic foot ulcer (DFU) is a prevalent disease among Type 2 diabetic patients (T2DPs) often associated with vascular and neurological complications. 1 The prevalence of foot ulcers among T2DPs is about 6.3% for all countries. The highest prevalence is in Belgium at 16.6%, and in Asia, it is 5.5%. 2 The lowest prevalence of foot ulcers in Australia is 1.5%. Limb amputation may be necessary as a last choice to prevent infection and mortality. The decision to amputate varies globally such as 26%, 3 29.7%, 4 and 51% 5 depending on risk factors such as infection, lower extremity artery disease, and ulcer severity. Despite aggressive treatment measures, the recurrent rate of DFU remain high at 40% after 1 year, 6 60% after 3 years, 6 and 65% after 5 years, 6 affecting the quality of life, and exerting a financial burden to patients.
The common reasons for diabetic foot re-ulceration are due to: (1) Poor glycemic control; (2) Peripheral neuropathy; (3) Peripheral arterial disease; (4) Poor foot care; and (5) Comorbidities. Prevention of re-ulceration involves proper foot care, regular monitoring of blood sugar levels, and management of comorbidities. Multidisciplinary care teams can help to identify and address the underlying causes of re-ulceration and provide appropriate interventions to prevent recurrence. 7 The reported factors in previous studies that contribute to late diagnosis of diabetic foot ulceration may include lack of awareness among patients and healthcare providers, inadequate screening and monitoring, and poor access to healthcare services.8,9
In Vietnam, healthcare providers prioritize limb preservation in treating DFU by using appropriate antibiotic selection, glycemic control, and proper ulcer care and removal, but amputation may still be necessary in some cases. However, the rate of amputation indication at Cho Ray Hospital was previously high (up to 50%), even when following international treatment guidelines.10-12 Although short-term outcomes of amputation intervention have been studied, long-term outcome assessments still need to be improved. This study aims to describe the long-term outcomes of amputation intervention in Vietnamese T2DPs after 24 months and identify factors related to DFU recurrence to improve DFU management in low-middle-income countries like Vietnam.
Material and Methods
Study site and study population
Cho Ray Hospital, situated in Ho Chi Minh City, Vietnam, is a tertiary healthcare facility that patients that caters to the needs of T2DPs referred from lower-level provincial or hospitals, including those with severe diabetic foot infections.
The observation study included 57 Type 2 T2DPs with DFU who met the hospitalization criteria as per Infectious Diseases Society of America (IDSA) 11 from 2018 to 2020. All the participants underwent low extremity amputation and were followed up for 2 years, with complete 24-month follow-up data available for analysis.
Re-ulceration definition as the primary end-point
This study’s definition of ulcer recurrence was the development of a new ulcer in a T2DP at any point during the 24-month follow-up period subsequent to the healing of the original ulcer.
Clinical data pertaining to wound healing time, mobility, foot care, and ulcer recurrence were collected every 3 months through telephonic or direct visits.
The T2DP cohort was classified into 2 groups based on intervention efficacy, namely Group A, which comprised patients who experienced at least 1 re-ulceration, and Group B, which included patients who did not experience any re-ulceration. The end-point for classification was based on the occurrence of the first re-ulceration or not event during the follow-up period.
Data analysis
Data from archived clinical records, direct visits, and phone followed-ups were collected for analysis. Statistical analysis was performed using STATA version 15. Continuous variables obtained from the clinical characteristics were expressed as the mean ± standard deviation and were compared using the student t-test. The chi-squared test or Fisher’s exact test depending on the number of events for evaluated variables, was used for comparisons made between categorical variables.
Ethical approval
The research complied with the requirements and regulations for biomedical research review of the Ethical Council of the University of Medicine and Pharmacy of Ho Chi Minh City. The study was approved by the Ethics Committee in Biomedical Research at the University of Medicine and Pharmacy of Ho Chi Minh City under Decision No.22/IRB-VN01002/IORG008603/FWA0023448. And the study was also approved by the Cho Ray Hospital’s Board of Directors to carry out the project.
Results
There were 94 Type 2 T2DPs whose toes were amputated. The different amputation levels included 73.3 % toe, 8.5% foot sole, 16.0% instep, and 2.1% thigh at 2.1%. Only 57 T2DPs with complete 24-month followed-up data were divided into 2 groups: Group A (Re-ulceration, n = 17, 29.8%) and Group B (Non-re-ulceration, n = 40, 70.2%).
We identified some crucial factors associated with the failure of amputation intervention after 24 months by comparing the 2 groups’ clinical. Data in detail are described in Table 1.
Related factors to the amputation efficacy between 2 groups after 24 months.
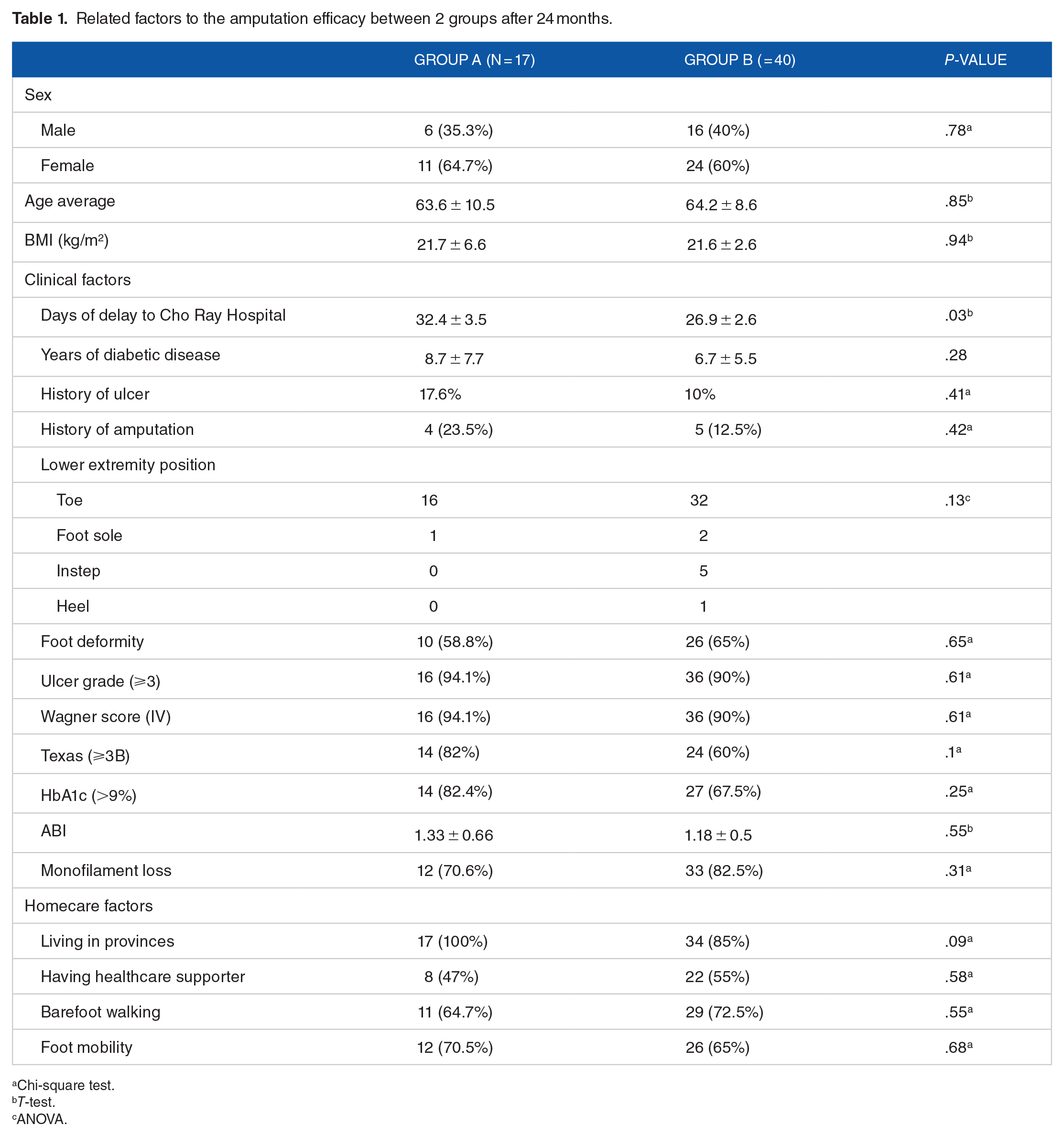
Chi-square test.
T-test.
ANOVA.
(a) Late medical foot ulcer diagnosis and care
All patients in group A (100%) live in provinces around Ho Chi Minh City, far from Cho Ray Hospital, ranging from 30 km (Binh Duong Province) to over 150 km (Can Tho City). It was found that the delay time from the onset of early ulcer symptoms to hospitalizing at Cho Ray hospital was significant longer for Group A than for Group B (32.4 days vs 26.9 days), with P-value of .03.
(b) Other potential factors with a higher rate of re-ulceration, but not statistical difference.
Severe ulcer at the time of amputation
The tissue damage of the ulcer at the time of amputation was found to be more severe in Group A than in Group B with depth grade 3 and Wagner 4 (94.1% vs 90%). The study also revealed a higher incidence of infection with TEXAS 3B in Group A compared to Group B (82% vs 60%).
Having a history of ulcers, amputation, and a longer time of diabetes with failure in HbA1c control
Group A had a longer duration of diabetes than group B (8.7 years vs 6.7 years), a higher failure rate of HbA1c control (HbA1c > 9%) as 82.4% versus 67.5%, a higher rate of loss of monofilament sensation (82.5% vs 70.6%), and 2 times higher of having history of foot ulcers and amputation.
Higher mobility
T2DPs in Group A had a higher mobility rate after their first amputation than T2DPs in Group B (70.5% vs 65%).
Discussion
This study is the first in Vietnam to evaluate long-term outcomes, including ulcer recurrence and amputation rate in 57 cases over 24 months following their initial amputation and good diabetic care. The rate of ulcer recurrence remained high by 29.8% after 24 months (Group A, n = 17).
Hospitalization is necessary for the proper and intensive intervention of diabetic foot ulcers. However, in Vietnam, T2DPs often face late diagnoses and delayed medical intervention for their condition. The high lower-limb amputation rate in our study (46.5% of which mainly toe amputation 73.4%) was mainly related to the degree of infection (severe infection accounted for 41.6%) and the degree of tissue damage (Wagner).4,5 Thus, the level limb extremity rate is mainly related to late detection and proper care of ulcers. Our study observed a significant difference in the duration of time taken to hospitalize patients with early ulcer symptoms between group A and group B, where group A exhibited a delay time of 32.4 days as compared to group B's delay of 26.9 days with a P-value of .03. This result is consistent to previous studies on short-term outcomes in Vietnam with 29.9 days (in 1998) and more than 28 days (in 2003). T2DPs with foot ulcers accessed a podiatrist had a median time of 15 days in the UK, 13 and 4 weeks in Sweden. 14
The most prevalent reasons for amputation are late self-diagnosis, delayed hospitalization for primary care, and referral with severe infection and excessive foot tissue damage. Late referrals are a common issue worldwide; for instance, in Europe, the duration of DFU was unknown, or the referral was delayed for more than 3 weeks in 55% to 66% of cases. 15 On average, 48% of T2DPs were referred with unknown duration or after more than 1 month from the onset of DFU. 15 Late admission is frequently observed due to a variety of factors, such as the majority of T2DPs living in distant provinces, financial constraints, and peripheral nerve complications (accounting for approximately two-thirds of T2DPs in our study), which can lead to decreased or loss of sensation, making foot ulcers challenging to detect. T2DPs admitted late and receiving treatment at provincial hospitals may still be at risk of poor treatment outcomes due to primary care practitioners not adhering to best practice foot care recommendations. 16 T2DPs initially sought care from a variety of different venues—primary care doctors, podiatrists, specialists, emergency rooms, and urgent care clinics—as determined by how serious their DFU and insurance status and access issues. 17 Strategies to improve early detection and treatment of diabetic foot ulceration include patient education, regular foot exams, and multidisciplinary care teams.7,8 Furthermore, it is important for T2DPs to be vigilant about foot care and to seek medical attention promptly if they notice any signs of foot injury or infection. Healthcare providers should also be proactive in screening and monitoring patients for diabetic foot ulceration and providing timely intervention when necessary. Patients in the re-ulceration group had a higher degree of foot ulcers with more severe infection with TEXAS 3B (82% vs 60%) at the time of intervention. It might cause re-ulceration (29.8%) after 24 months, but other studies reported higher rates. In the combined study by Armstrong 2017, 3 the rate of ulcer recurrence after 1 year was about 40%, and after 3 years it was 60%. The rate of recurrence after 2 years was varied by studies, such as Chanteleau 59% 18 and Dargis 48%. 19 We found that those studies investigated the overall recurrence rate for both amputation and non-amputation patients, which may account for the higher rates observed.
Previous studies reported risk factors associated with re-ulceration including s poor glycemic control,20 peripheral neuropathy, lower extremity artery disease, late foot ulcer diagnosis, non-adherence to appropriate footwear, and improper foot care.16,17 In our study, the re-ulceration group had a long time of having diabetes as well as high failure rate in controlling HbA1c, so there could be more chronic complications (higher rate of monofilament loss of sensation and vascular stenosis) than in the non-re-ulcerative group. However, the duration of diabetes in foot ulcer patients in our study was shorter than in European and American studies. Patients with foot ulcers had an average duration of diabetes of 17.5 years, 21 15 years, 22 and 14.7 years. 23 The duration of diabetes for 10 years is an independent risk factor for leg ulcers and amputation. 24 The shorter duration of diabetes with leg ulcers may be due to the late detection of diabetes, poor glycemic control, socioeconomic status, poor health care system, and poor awareness of foot protection. We also examined other relevant factors, such as age, sex, and BMI, between the 2 groups and did not observe any significant differences based on the equality values (refer to Table 1).
The history of foot ulcers and amputation is an important risk factor for ulcer recurrence. Following a foot ulcer or amputation, the anatomical structure and weight distribution in the sole become increasing altered, leading to further deformity, eventually ulceration. In addition, T2DPs with a prior history of ulcers and amputations often already have all the risk factors for foot ulcers to continue to cause new ulcers. In our study, the failure group (Group A) had a history of foot ulcers and amputation nearly 2 times higher than the success group. Other studies also showed that ulcer recurrence patients had history of foot ulcers and amputation, such as 39.5% (foot ulcers), 21 34.0% (amputation), 21 37.2% (foot ulcers), 22 and 16.5% (amputation). 22
After undergoing amputation, elderly T2DPs (with an average age of 64 years) are advised to decrease their activity level, and mostly remain at home, utilizing wheelchairs or stay in bed. A sedentary lifestyle minimizes pressure on the stump, and the opposite leg, thereby reducing damage to the foot, and the likelihood of ulcer recurrence. The participants in our study has poor glycemic control (HbA1c = 11%), a high rate of peripheral neuropathy (about two-thirds of T2DPs), low awareness of foot care, (about two-thirds go barefoot), lack of orthopedic shoes (which increases the risks of ulcer recurrence, deformity, and posterior amputation). The ulcer recurrence rate was lower than other studies mainly due to the degree of mobility. The degree of exercise greatly affects the recurrence of ulcers, when wearing orthopedic footwear will reduce the rate of ulcer recurrence by 50%. 25 In our study, the patients with more exercise, and more mobility had more risk of ulcer recurrence (Group A 70.5% vs Group B 65%). In order to enhance mobility and decrease the recurrence rate of ulcers after amputation, Vietnam requires specialized rehabilitation centers to assess post-amplification foot pressure and provide appropriate orthopedic shoes for T2DPs. Currently, these centers are scarce and T2DPs have limited access them.
Our study was subject to 2 principal constraints, namely: (1) The collection of data from DP records using an observational approach, as opposed to designed or intervention studies with predetermined sample size and enrollment, and adherence to all research protocols throughout the duration of the study; (2) The acquisition of a significant number of T2DPs with complete data after 24 months was nearly unattainable for observational studies, resulting in a limited number of T2DPs for detecting statistical differences.
Conclusion
Our study demonstrated a high incidence of amputation due to delayed ulcer detection, inadequate care, severe infection, tissue damage, and toe necrosis. Additionally, the 2-year followed-up re-ulceration rate in our study was 29.8% and the risk of re-ulceration after 24 months might depend on many clinical factors. Early diagnosis and treatment of diabetic foot ulcers may help in reducing the amputation rate and the risk of re-ulceration in Type 2 diabetic patients.
Footnotes
Acknowledgements
We would like to thank to Cho Ray Hospital and University of Medicine and Pharmacy of Ho Chi Minh City for supporting us to conduct this research.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Huynh Tan Dat: Conceptualization (equal); Methodology (equal); Data curation (lead); Investigation (equal); Validation (lead); Writing-original draft (equal).
Tran Chi Thanh: Conceptualization (equal); Methodology (supporting); Data analysis (lead); Writing-review & editing (equal);
Pham Le An: Methodology (equal); Writing-review & editing (equal)
Nguyen Thy Khue: Methodology (lead); Writing-review & editing (lead)