
Abstract
Heart Failure (HF) has been identified as an important public health problem, with high morbidity and mortality, despite advances in current therapy. New strategies are demanded to reduce the number of hospitalizations and deaths. Telemedicine approaches could improve the management of patients with cardiovascular conditions. Sixty patients with heart failure with reduced ejection fraction (HFrEF) were randomized to this pilot study. Weekly electronic messages were sent for 1 year. The use of telemedicine was effective instrument for the evolutionary follow-up of patients with HFrEF during the COVID-19 pandemic, but did not demonstrate an impact on the reduction of cardiovascular outcomes or hospitalization for HF. REBEC - Brazilian Registry of Clinical Trials identifier RBR-5q6x56k. Monitoring heart disease patients via WhatsApp during the COVID-19 pandemic. Available from http://www.ensaiosclinicos.gov.br/rg/RBR-5q6x56k/
Introduction
Heart failure (HF) is a severe syndrome that are originated from structural and (or) functional cardiac abnormalities leading to an impaired ventricular filling and ejection capacity. 1 It has been identified as an important public health problem and considered as a new epidemic, with high morbidity and mortality, despite advances in current therapy.1,2
HF contributes annually to all-cause mortality rates of 17% and to hospitalization rates of 44%. 3 The economic and public health impact is much more significant when considered that almost 50% of all hospitalized patients with this diagnosis are readmitted within 90 days after hospital discharge. 4 Readmission is one of the main risk factors for death. 3
Approximately 40% of hospitalizations for decompensated HF are preventable. 1 Patient poor therapeutic adherence and also the difficulties in medical assistance access in public health system are important reasons that affect primarily disadvantaged social and economically groups. 3
New strategies and approaches are needed to try to reduce the number of hospitalizations and death in patients with HF. One of these strategies is the telemedicine and telecare, a modality that showed significant growth during the COVID-19 pandemic. 5
Telemedicine is defined as the use of technologies to provide health support. Telemonitoring (TMO) is one its particularly useful subtypes.5-7 It can be invasive (eg, implantable devices) or non-invasive—such as telephone calls, emails, video calls, and text messages via cell phone.5,8
Although clinical trials of non-invasive TMO have conflicting results,9-12 meta-analyses involving observational and randomized studies have shown positive results in the prognosis of patients with HF, including reduced hospitalizations, mortality and improved quality of life.5,6,8,13
During the COVID-19 pandemic, many barriers to telemedicine have disappeared. 14 Virtual visits and telemonitoring strategies have become routine. 14 The scientific research on safety and effectiveness of virtual visits to replace in-person visits is accumulating.5,14 Instant messaging applications are a widely used tool used telemonitoring scenario.9,15 WhatsApp® is a mobile app for exchanging text messages and communicating in audio or video, available for smartphones from different operating platforms.16,17 This tool seems to be a promising possibility because intuitive and has low cost. Besides, it can provide individualized patients monitoring in real time, avoiding hospitalizations, and reducing public health costs. 16
There is a lack of data in the medical literature on the use of the WhatsApp® application as a follow-up strategy for HFpEF patients. We present our experience, using a follow-up strategy in a context of real practice based on text messages via the WhatsApp® application. The main goal of this study was to evaluate if an educational strategy would reduce clinical decompensation episodes and hospitalizations in HFrEF patients during the COVID-19 pandemic.
Methods
Study design
This is a pilot study, longitudinal, prospective, randomized, carried out in an outpatient clinic of General Hospital Roberto Santos, located in Salvador, Bahia, Brazil and registered in the Brazilian Registry of Clinical Trials (ReBEC): RBR-5q6x56k. The study followed the guideline of the Declaration of Helsinki. The Research Ethics Committee from the Roberto Santos General Hospital reviewed and approved the study (Number: CAAE: 30701720.0.0000.5028). A verbal informed consent was obtained from each patient before randomization.
Study population and randomization
Eligibility requirements included an age of at least 18 years, chronic HF with reduced ejection fraction (EF ⩽ 40%) regardless of etiology, functional class I-IV (New York Heart Association—NYHA), optimized drug therapy, cellular device with access to the Whatsapp® application. Exclusion criteria: cardiogenic shock, cardiac surgery in the previous 8 weeks, heart transplant waiting list, chronic renal failure on dialysis, uncontrolled high blood pressure, inability to understand or interact with text messages due to illiteracy, cognitive impairment or social problems, severe depression, and uncontrolled arrhythmia.
Verbal informed consent was obtained and patients were randomized in a 1:1 ratio to the intervention group (IG) who received weekly messages via the WhatsApp®. The control group (CG) had usual follow-up. Randomization were made using a table of random numbers. Patients began to be recruited in June 2020.
Follow up
After randomization, patients or their caregivers allocated to the IG received an educational message weekly through the WhatsApp® application sent by a central. Educational messages contained information on signs and symptoms of HF decompensation, daily activities, medication use, lifestyle, fluid intake, and vaccination. The messages were short with the aim of encouraging patients to take actions such as take medication, weighing loss, or seek medical attention. Patients were informed not to respond the messages, but they were allowed to interact with the central and be directed for guidance via telephone or in person with the assistant cardiologist if necessary. Telephone calls with structured interviews were made monthly by medical students to both groups. Questionnaires such as the Minnesota Living with Heart Failure Questionnaire (MLHFQ—validated version in Portuguese) to assess quality of life and Framingham Criteria to assess possible HF decompensation were applied during phone calls. If signs of clinical worsening or cardiac decompensation were identified, the participants were advised by telephone by a cardiologist. If there was no clinical improvement, the participant was instructed to go to the emergency department. The control group received the standard treatment approach for HF patients, involving medical outpatient visits in which they received instructions regarding pharmacological and non-pharmacological therapeutic strategies.
Study outcomes
The primary outcome was a composite of total hospitalizations (first and recurrent) for heart failure and cardiac decompensations in patients with HFrEF undergoing noninvasive telemonitoring via electronic messages.
Secondary outcomes were worsening NYHA functional class; worsening of quality of life using the MLHFQ, ICU admission, and death from any cause in a time-to-first-event analysis.
Statistical analysis
Categorical variables were expressed as frequency and percentage and analyzed using the χ2 test. Continuous variables were tested by the Kolmogorov-Smirnov test for normality. Thus, continuous variables in normal distribution were expressed as mean ± SD; non-normal distribution was expressed as median and interquartile range. For comparison of variables, Student’s t test, Mann-Whitney, ANOVA or Kruskal-Wallis test were used, as appropriate. Paired comparisons at different time points were performed using the Wilcoxon test. A P value <.05 was considered statistically significant. SPSS 27.0 (SPSS Inc., Chicago, IL, USA) was used to perform the statistical analysis.
Results
From June 1, 2020 through to December 31, 2020, we recruited 76 patients with HFrEF previously followed up at the HF outpatient clinic of the Roberto Santos General Hospital, as detailed in Figure 1. Sixty patients were randomized assigned, in a 1:1 ratio, to the Telemonitoring group or Control group. Follow up was discontinued by 6 patients in the telemonitoring group and 2 in the usual follow-up group, thus 52 patients were enrolled for the study. The clinical and sociodemographic data of the population are presented in Table 1. No significant differences were noted between the groups. The mean age was approximately 55 years and the male gender had a higher prevalence (55.8%).

Enrollment, randomization, and follow-up (CONSORT 2010 flow diagram).
Baseline characteristics of the patients.

No significant differences were noted between the groups. Plus–minus values are means ± SD. Values displayed as n (%) unless otherwise noted.
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CIED, cardiac implantable electronic devices; SD, standard deviation; TIA, transient ischemic attack; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association.
The study population was composed of several etiologies of HF. Six patients (14.5%) were due to Chagas’ disease, 14 (26.9%) had an ischemic myocardiopathy and 20 (38.5%) were due to: valve disease, systemic arterial hypertension and other causes. The mean left ventricular ejection fraction measured by echocardiography was 30.52% ± 8.8%, with no statistical difference between the groups (P = .44), highlighting the patient’s heart failure severity.
Arterial Hypertension and Diabetes Mellitus were quite prevalent, affecting 65.4% and 32.7% of patients, respectively. Almost half of the patients (42.3%) had already suffered at least 1 previous infarction and 30% a transitory ischemic attack or a stroke.
Primary and secondary outcomes are summarized in Table 2. There was no difference in the combined primary outcome (P = .36). Most patients in both groups were in functional class II (NYHA) at baseline, but progressed to functional class III at the end of follow-up. However, there was no statistically significant difference when compared heart failure functional class at admission and at the end of follow-up (P = .73).
Primary and secondary outcomes in intervention and control population.
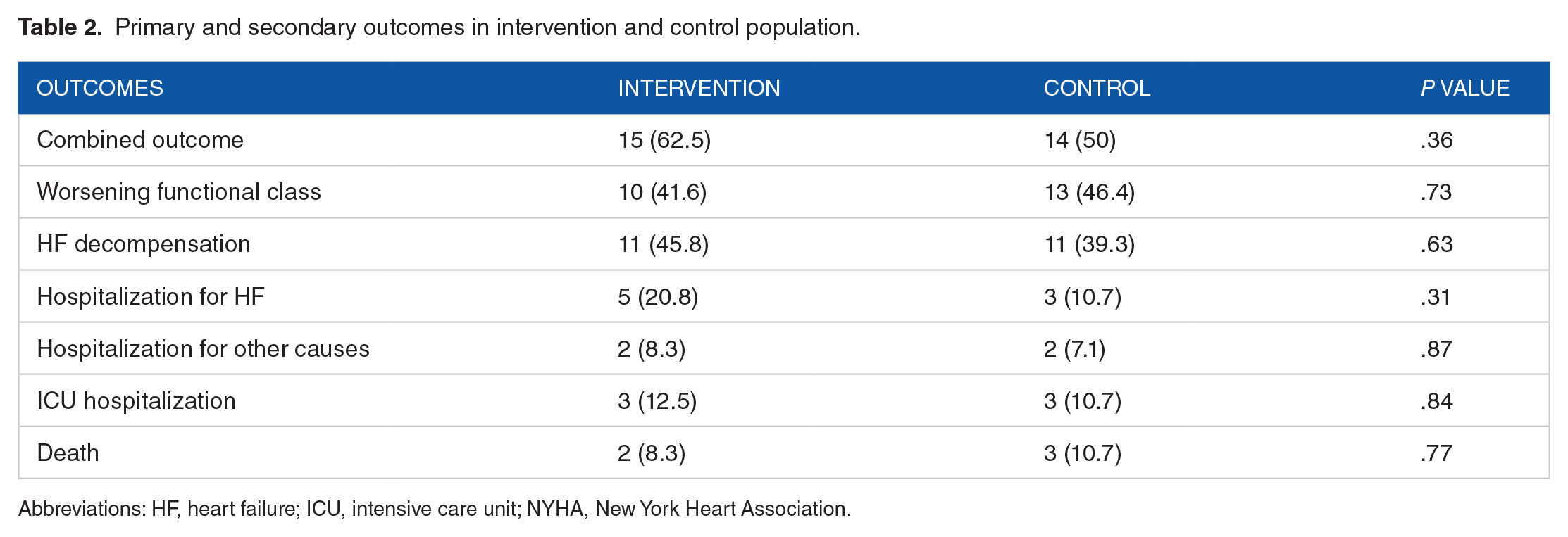
Abbreviations: HF, heart failure; ICU, intensive care unit; NYHA, New York Heart Association.
Approximately 45% of the patients in the intervention group had at least 1 episode of HF decompensation and 39% in the control group (P = .32). Five patients in the intervention group required hospitalization due to cardiac decompensation, 3 patients were admitted to the intensive care unit and 2 died during the follow up of the study. In the control group, 3 patients need hospitalization, all of them were admitted in the ICU and 3 died during the follow up. There was no difference between the number of ICU admission and deaths in the control and intervention groups (P = .55).
Baseline and one year NYHA functional class and the Minnesota Living with Heart Failure Questionnaire (MLHFQ) are detailed in Table 3. The MLHFQ score was 38.8 ± 16.45 in the intervention group and 34.57 ± 18.22 in the control group (P = .39) at baseline and 35.54 ± 13.02 in the intervention group and 37.86 ± 19.48 in the control group (P = .62) after 12 months. The change from baseline in the MLHFQ global score was not statistically different between the telemonitoring group and usual care group (P = .22).
Baseline and one year NYHA functional class and the Minnesota living with heart failure questionnaire (MLHFQ).

Abbreviations: SD, standard deviation; MLHFQ, minnesota living with heart failure questionnaire; NYHA, New York Heart Association.
Values expressed as mean ± SD.
Discussion
The use of electronic messaging and telemedicine resources for remote monitoring of patients during the pandemic was an important medical care instrument. In the present study, we conducted a randomized pilot study with the objective to evaluate the impact of a non-invasive telemonitoring strategy through electronic messages (using WhatsApp®) on the number of hospitalizations and decompensations in patients with HFrEF. To date, this study is the first to exclusively use a text messaging application, WhatsApp®, for outpatients with HFrEF.
We found that there was no statistical difference between the intervention and control groups in any outcome assessed; numerically, in both groups, there was a worsening of the functional class from II to III at the end of the follow-up, suggesting that telemonitoring can be a useful tool in monitoring the functional class and can also be used to detect possible emergencies and facilitate their management.
Previous studies with invasive approaches such as wireless implantable hemodynamic monitoring of pulmonary artery pressure used to guide treatment optimization significantly reduced the risk of hospital admissions due to heart failure and therefore already was integrated into the 2016 ESC guideline. 11 However, there is disagreement about the effectiveness of non-invasive methods in reducing hospitalizations and deaths of patients with HF, and this type of monitoring is not yet part of any guideline or consensus.9-12,18-20
In this scenario, simpler and lower-cost monitoring, such as send a message via WhatsApp® application, may be a plausible alternative for a larger number of patients, since 99% of world population with smartphones use the application as a tool to send and receive messages. 17 Furthermore, SMS-based strategies for monitoring patients with chronic diseases such as diabetes mellitus and human immunodeficiency virus infections have been shown to be effective. 15 The uniqueness of our study lies in its strategy of weekly electronic messaging using the WhatsApp® app in a public health care-assisted HFrEF population in a middle-income developing country.
An American study evaluated a Short Message Service (SMS) intervention in hospitalized patients with decompensated heart failure. 9 Self-care and education messages about diet, symptom recognition and syndrome management were sent like our study. The intervention was associated with significant improvements in self-care and maintenance of clinical compensation. 9 However, Chen et al found different results using a similar approach. At a short-term follow-up (30 days), there was no difference in clinical outcomes between the groups studied. 15 These interventions also modified self-care behavior, such as medication adherence and fluid restriction.
The Minnesota Living with Heart Failure Questionnaire (MLHFQ) is an important measurement instrument for assessing the quality of life of heart failure patients. 21 Scores range from 0 to 105, with higher scores indicating more significant impairment in health-related quality of life. We found a numerically improvement in the quality-of-life assessment based on the MLHFQ in the intervention group at 365 days, however no statistical significance when compared to the control group (P = .27). Chen et al found similar results. 15
Regarding mortality, our study showed no statistical difference between the intervention and control groups, as well as large previous studies.15,21,22 In Tele-HF, the largest study on telemedicine and heart failure, with 1653 patients, telemonitoring did not reduce readmission for any reason, death from any cause, and hospitalization for heart failure within 180 days when compared to the control group. 21
In TIM-HF, patients performed a daily self-assessment with ECG, blood pressure, scale and oximeter, and the data were transferred to the telemedicine center, which provided medical support. No significant reductions were observed between groups for primary or secondary outcomes such as death from any cause, cardiovascular death, and hospitalization for HF. 22
The BEAT-HF study used a more intensive telemonitoring strategy compared to our study, such as the use of ECG, blood pressure device, weight balance and oximeter. Even with the addition of information and data, remote telemedical management compared with usual care was not associated with a reduction in all-cause mortality and did not reduce 180-day all-cause readmission after hospitalization for HF. 12
On the other hand, the practice of telemedicine by non-medical professionals has shown different results.22,23 The follow-up of patients based on telephone support and/or home visits by nurses and health workers is also an available option, especially in developing countries, such as Brazil, where social, cultural and economic restrictions can limit the effectiveness of HF treatment outside the hospital environment. 22
The practice of telemedicine by non-medical professionals based on telephone support and/or home visits is also an available option, especially in low/middle income countries, such as Brazil, where social, cultural and economic restrictions can limit the effectiveness of treatment.23,24 The HELEN-II followed patients with HF after hospital discharge from the public health system. 23 The study intervention performed by the nursing team resulted in a relative reduction of 27% in the combined clinical outcome of hospital admissions, care in the emergency or death sector. The TEN-HMS study, also carried out by nurses, showed that the strategy increased survival and decreased hospitalization during 240 days of follow-up. 24 Differently from what was found, our data suggest that in a population well-informed on care by the team, the use of Telemedicine-type resources did not add positively to statistical differences in hard outcomes such as death and hospitalization and intensive care unit.
The lack of conclusive efficacy results can be explained by differences in the actual content and intensity of each intervention and the heterogeneous nature of the patient populations included in different studies.
To date, studies with specialized multidisciplinary heart failure management programs have tested multifaceted approaches (multidisciplinary input, home/clinic visits, telephone support; SMS).24, 25 As a result, it has been difficult to identify the incremental benefits of the components of each intervention.24, 25 Multiple care options will emerge, combining conventional care and telemonitoring, according to patients’ needs and preferences, as well as health service resources. The main objective is to organize an economic and universal, but personalized, methodology for the provision of care. 14 An important fact to be highlighted is that telemonitoring results in greater patient satisfaction, improved self-care and adherence to treatment.
The present study, in agreement with previously published data, did not demonstrate the benefit of the remote monitoring strategy in reducing hospitalizations and episodes of cardiac decompensation. However, communication through the WhatsApp® application favored the early detection of worsening of the functional class, generating therapeutic adjustments and early medical consultations, possibly avoiding episodes of cardiac decompensation, in addition to facilitating the clinical follow-up of patients with heart failure.
As limitations, this is a single-center study with a small sample size. Please note that this is a pilot project. Although only one hospital participated in this trial, the population heterogeneity is representative enough that the results have reasonable external validation. Another questionable point is the time period between messages being sent. Weekly may have been a long time, having no effect on the analyzed outcomes. In the future, daily messages, preferably at the same time, may be a more appropriate choice. The study did not assess cost-effectiveness or ethical issues of telemonitoring.
Adherence may have been a critical factor. It is a key point in any telemedicine program, because poor adherence can compromise the benefits of such monitoring. Ten percent of patients randomized to the intervention began to complain about messages and phone calls. Some patients may have misunderstood the questions or answered without proper attention. Future research should focus on identifying optimal strategies, duration of follow-up, patient profile, and cost-effectiveness. An individual simple monitoring will not change the disease progression, unless there is an action. More efforts should be made to foster the inclusion of vulnerable patients and improve global telemedicine access.
Conclusion
In outpatients with HFrEF, sent eletronic messages via WhatsApp® application did not reduce the number of hospitalizations and cardiac decompensations. At the end of the follow-up, it was observed that there was no improvement in quality of life, but telemedicine favored the early detection of worsening of the functional class.
Supplemental Material
sj-docx-1-his-10.1177_11786329231154692 – Supplemental material for Use of Electronic Messages in the Follow-Up of Patients With Heart Failure: Randomized Pilot Study
Supplemental material, sj-docx-1-his-10.1177_11786329231154692 for Use of Electronic Messages in the Follow-Up of Patients With Heart Failure: Randomized Pilot Study by Igor Santos Schonhofen, André Maurício Souza Fernandes, Roque Aras Júnior, Taís Sousa Macêdo, Bruno Bonfim Da Silveira, Guilherme de Andrade Costa, Marina Domingues Feitosa and André Rodrigues Durães in Health Services Insights
Footnotes
Acknowledgements
We thank General Hospital Roberto Santos for their assistance during the pilot study.
Correction (October 2023):
This article has been updated with minor grammatical or style corrections since its original publication.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
IS and AD undertook the study design, data analysis, and drafted the manuscript. All authors contributed to interpretation of results, review and editing of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.