
Abstract
Background:
Data on abortion procedures costs are scarce in low- and middle-income countries. In Mexico, the only known study was conducted more than a decade ago, with data from years before the abortion legislation. This study estimated the costs, from the health system’s perspective, of surgical and medical abortion methods commonly used by women who undergo first-trimester abortion in Mexico.
Methods:
Data were collected on staff time, salaries, medications, consumables, equipment, imaging, and lab studies, at 5 public general hospitals. A bottom-up micro-costing approach was used.
Results:
Surgical abortion costs were US$201 for manual vacuum aspiration and US$298 for sharp curettage. The cost of medical abortion with misoprostol was US$85. The use of cervical ripening increases the costs by up to 18%. Staff comprised up to 72% of total costs in surgical abortions. Hospitalization was the area where most of the spending occurred, due to the staff and post-surgical surveillance required.
Conclusions:
Our estimates reflect the costs of “real-life” implementation and highlight the impact on costs of the overuse of resources not routinely recommended by clinical guidelines, such as cervical ripening for surgical abortion. This information will help decision-makers to generate policies that contribute to more efficient use of resources.
Background
Reducing global maternal mortality is a target of the United Nations’ Sustainable Development Goals (SDGs). 1 Despite efforts to achieve universal access to safe and effective health care, the world is not on track to achieve this objective. 2 Maternal mortality is still a global public health issue, affecting primarily low and lower-middle-income countries (LMICs), 3 where approximately 94% of all maternal deaths occur. 2 Of the total maternal deaths reported globally, 8% are related to abortion. 4 In Mexico, according to data from the National Institute of Statistics and Geography (INEGI), similar figures are reported. 5
With the aim of promoting safe abortion care, the World Health Organization (WHO) has established recommendations on best practices based on evidence. Currently, the methods recommended by the WHO for first-trimester abortion are vacuum aspiration, as the surgical method of choice; and medical abortion, either with misoprostol only or in combination with mifepristone. 6
Electric or manual vacuum aspiration is recommended for pregnancies up to 12 to 14 weeks gestation. Vacuum aspiration consists of dilating the cervix, inserting a plastic or metal cannula into the uterus through the cervix, connecting the cannula to a vacuum source, and aspirating the uterine content. The vacuum source can be electric or manual. This method lasts from 3 to 10 minutes depending on the uterine size and the amount of ovular remains. It is an effective and safe technique; its effectiveness ranges between 95% and 100% and the complication rate is estimated to be less than 1% . 7 General anesthesia is not routinely recommended. Generally, only analgesics and local anesthetics are administered, so the woman can leave the clinic after a short period of observation, usually not more than 1 hour. 7 In surgical abortion, current guidelines suggest the use of misoprostol or mifepristone before the vacuum aspiration as a method of cervical ripening. 6 Although cervical ripening is recommended after 13 weeks gestation to reduce the duration of the procedure and the risk of incomplete abortion, its use is not routinely recommended during the first trimester. 8
Medical abortion comprises the use of mifepristone in combination with misoprostol or misoprostol alone. These drugs stimulate uterine contractions and cause the uterine contents to be expelled. The combined use of mifepristone and misoprostol has been considered the standard of care, but recent evidence has shown equal effectiveness with misoprostol alone as with the combined regimen, with complete abortion rates of 94% and higher. 9 Misoprostol alone to induce abortion is an option where mifepristone is not available. As well as in vacuum aspiration, complications with medical abortion are reported in less than 1% of patients. The cost of a medical abortion varies according to the regimen used, but it is generally considered a low-cost method. 7
Sharp curettage is a surgical method that consists of dilating the cervix and using a metal curette to scrape the walls of the uterus. In this procedure, it is common for the woman to undergo general anesthesia or sedation. Compared to vacuum aspiration, sharp curettage is a less safe procedure with twice the chance of minor and serious complications.6,7 Sharp curettage for surgical abortion is considered obsolete by both the WHO and the International Federation of Gynecology and Obstetrics (FIGO).6,10 Therefore, it is well documented that manual vacuum aspiration is as effective as sharp curettage, but with a lower rate of complications, shorter hospital stay, no need for general anesthesia, less post-surgical pain, and lower costs.11,12
However, despite these recommendations, the use of sharp curettage as the method of choice for first-trimester abortion remains high in several low and lower-middle-income countries.13,14 In Mexico, the routine use of sharp curettage in public and private hospitals has been extensively documented.15,16 In a recent study conducted in 41 Mexican public hospitals in 2019, it was reported that 41% of women with first-trimester abortions were treated with sharp curettage. Among the relevant factors identified that contribute to the routine use of this method were the availability of supplies, including budgeting and procurement, and the confidence and training of personnel in other methods. 17
The emergence of new technologies forces health systems to implement policies that promote the use of safe procedures at the lowest cost. For this reason, it is important for healthcare providers and decision-makers to evaluate efficient ways to allocate resources. Having robust cost estimates available will provide valuable insights for future efforts to assess the cost-effectiveness of these abortion methods with the aim of increasing the availability and accessibility of safe abortion care. This is particularly relevant in contexts where resources are limited, as in many LMICs, where preventing inefficiencies becomes essential to provide quality health care services.
Several studies on the costs of abortion methods have been carried out in different countries. In general, surgical methods are reported to be more expensive than medical abortion methods.15,18-20 Of the surgical methods, the most expensive is sharp curettage.15,18,21,22 Different approaches have been used to estimate the unit costs of abortion procedures; while some used methodologies based on micro-costing, others used diagnosis-related groups or fees charged set by facilities.18,19,21,23 The problem of using hospital charges is that they are usually standardized amounts and, in some cases, it is not possible to disaggregate by type of category, which can underestimate the cost of certain inputs, such as the staff costs.
In Mexico, there is scant information about the costs of abortion procedures. The only known study was conducted more than a decade ago in Mexico City, with data from years prior to the passage of the abortion legislation. An ingredients-based micro-costing method was used, based on the WHO’s clinical practice guidelines, and it did not include information about medical abortion with combined medications.15,24
Therefore, the objective of this study was to obtain estimates of the costs of surgical uterine evacuation methods (manual vacuum aspiration and sharp curettage), and medical abortion in 2 regimens (either with misoprostol only or combined with mifepristone), used on women who undergo abortion before 13 weeks gestation at 5 public hospitals in Mexico, using a micro-costing approach from the health system’s perspective.
Methods
Study setting
In Mexico, abortion services in the public sector are only provided in second-level general hospitals (except in Mexico City, where medical abortion is also provided in first-level clinics). Therefore, our study was conducted at 5 public general hospitals, located in 5 different Mexican states. These units were teaching hospitals, that provide basic health care services such as general surgery, internal medicine, pediatrics, and obstetrics and gynecology. Three of them are located in states’ capitals; the remaining 2 are located in municipal capitals. The management and funding of these hospitals depend directly on the Mexican Ministry of Health. In the period in which the study was carried out, abortion had not been decriminalized in any state where the hospitals are located, so abortion services were only provided under certain causes (eg, rape, congenital malformations, serious damage to health, etc.), and there was no elective abortion. These hospitals have a collaboration agreement with Ipas Mexico and were selected for convenience, as long as they performed the abortion procedures of interest.
Ethical clearance
The Allendale Investigational Review Board approved the study. Informed consent was obtained by telephone, before the interviews (Approval number: cam costco.072320)
Information mapping and patient flow description
The first step was to carefully define all the inputs, activities, and patient flow within the health care units. With this aim, we conducted a mapping of information across hospital areas, through interviews with members of staff at the sites. This detailed description allowed us to develop a costing framework (Supplemental File 1), which served as a starting point to create Excel-based tools to collect information across healthcare units.
We also identify the patient flow within the sites. In the hospitals where the study was carried out, the first contact of a woman presenting with a first-trimester abortion, spontaneous or induced, is made in the emergency room on an unscheduled basis. Initial evaluation, clinical history, and physical examination are performed along with laboratory studies and obstetric ultrasound. Once the diagnosis is confirmed, the decision about which method to choose is made between the woman and the health care personnel. This choice depends on women’s and physicians’ preferences and the availability of resources. For example, if no vacuum aspirator is available at the time, sharp curettage is offered. Women eligible for surgical abortion are sent to the delivery or operating room to perform manual vacuum aspiration or sharp curettage, respectively. Although it is not recommended as a routine procedure, the use of cervical ripening with misoprostol or mifepristone prior to surgical abortion was reported in the sites studied. As a general rule, after the procedure, women are sent to hospital surveillance and subsequently discharged, regardless of the surgical method performed. Postoperative surveillance time tends to be longer in women who underwent sharp curettage compared to manual vacuum aspiration. After discharge for surgical abortion, women may need outpatient follow-up only in particular situations. On the other hand, women eligible for medical abortion had their initial assessment in the emergency room, where they receive the medical treatment; then they are discharged and subsequently referred to the outpatient clinic for follow-up.
Data collection
Data collection was conducted during an 8-week period, from August to September 2020.
The tool collected data on the site’s general information, staff costs, staff time allocation, quantities, brands, and prices of supplies and consumables per type of abortion method.
To collect data, we selected respondents with the support of clinical coordinators at each hospital. We scheduled telephone interviews with at least 5 staff members for each of the following cadres: Ob/gyn specialists and residents, anesthesiologists, undergraduate medical interns, and nurses. After giving informed consent by telephone, interviewees were asked about the time dedication they spent on women who undergo first-trimester abortion procedures, their work hours, and wages received. Information on salary amounts was checked against official administrative records. If the salary reported in the interview was lower than the salary found in records, we used the latter for the analysis due to the tendency to underestimate the salary in direct interviews. Regarding data on quantities of supplies, consumables, and medications, interviewees were instructed to answer questions regarding their usual resource use and work habits during the work months prior to the COVID-19 pandemic, in view that the hospital’s dynamic may have shifted due to the health emergency.
Information about prices, brands, and dosages of medications and other supplies was obtained from procurement lists at site pharmacies and warehouses. Data not available in these records were obtained from the Ministry of Health’s consolidated procurement platform. We obtained the prices of imaging and lab studies from the price lists at each hospital.
Cost estimation
We used a micro-costing approach, from a health system perspective, having as a time horizon one-woman episode of healthcare for first-trimester abortion, either spontaneous or induced. Our estimates represent the economic cost in the real world, since they are based on the costing framework we developed and not on clinical practice guidelines. 25
Staff, medications, surgical equipment, instruments, and laboratory and imaging costs were included. Table 1 shows all the supplies we included in the study.
List of medications, supplies, and equipment included in the costing study.

Abbreviations: PT, prothrombin time; PTT, partial thromboplastin time.
To obtain staff costs, we first calculate an estimated hourly wage for each cadre, using the information obtained on monthly wages and working hours. Since we asked about the time the staff spends caring for women with first-trimester abortion, per type of method, and per hospital area, we were able to estimate the cost of each cadre for a specific abortion procedure. We multiply the hourly wage by the time spent on each procedure and, then, we add the costs of the different cadres involved in the provision of care for women undergoing each abortion method.
For medications, supplies, and consumables, we multiplied the price of each one by the amount used. Based on the shelf life reported by providers, the cost of equipment and surgical instruments was annualized to 5 years with a discount rate of 3%. We took into account equipment reuse for each procedure and computed a proportional cost, which was included in the total. We assumed that surgical instruments are used only for abortion procedures and are not shared with other departments at the site. Under surgical instrument costs, we included sterilization costs, according to what was reported in the literature. 26 As in other similar costing studies, neither overhead costs (electricity, water, gas, internet, etc.) nor salaries of administrative staff and paramedical support were included due to the logistical challenge of estimating those costs within the context of general hospitals serving patients in various specialties.13,27 Furthermore, given that one of the objectives of the analysis was to compare costs between alternatives, we assumed that overhead costs are identical for the 3 procedures of interest and do not add variability.
To estimate the cost of each procedure, we summed the cost of the resources and supplies involved in each abortion method. Based on what was reported by the hospitals, we were able to estimate the variation in cost according to the different quantities and brands of supplies, as well as the different combinations of staff cadres reported in each abortion method. For example, it was reported that manual vacuum aspiration could be performed either with local or regional anesthesia, as well as with different types of antibiotics, analgesics, or other medications and could involve different staff members (eg, Ob/Gyn specialist, resident, and nurse, or only an Ob/Gyn and nurse). For a more detailed description of this variation on cadres, see “Supplemental File 2, Table 1.”
With this variation in inputs, cadres, and prices, we computed a minimum and maximum cost for each abortion method, as a sensitivity analysis. The use of cervical ripening significantly increased the cost of each procedure compared to using none, so each abortion method was subcategorized based on the type of ripening medication (misoprostol, mifepristone, or none) to highlight this increase. We report the unit cost with a variation range (minimum and maximum) for the different abortion methods analyzed. All costs were converted to USD 2020.
Finally, we disaggregated the unit costs according to the hospital area where the expense occurs (emergency room, operating room, hospitalization and outpatient consultation), since we obtained information about the areas where the supplies were used and the time spent by the staff at every moment of the healthcare process.
Results
Total costs and their composition
We identified 3 main categories of abortion methods regularly performed in hospitals: manual vacuum aspiration, sharp curettage, and medical abortion. The first 2 were subcategorized according to the cervical ripening method used (misoprostol, mifepristone, or neither). Medical abortion was subcategorized into abortion either with misoprostol only or combined with mifepristone.
Table 2 shows the unit cost estimates. These estimates include the cost of all the personnel and supplies involved in the management of a patient with a first-trimester abortion, from her arrival at the emergency room to the completion of her medical care, either by hospital discharge or outpatient follow-up. The costs of the surgical methods were USD$201 and USD$298 for manual vacuum aspiration and sharp curettage, respectively. The cost of medical abortion using misoprostol only was USD$85, while combined with mifepristone was USD$122. Sharp curettage cost, even without cervical ripening, was usually higher compared to manual vacuum aspiration and medical abortion. It is important to note that the use of cervical ripening with misoprostol or mifepristone increased the unit cost of manual vacuum aspiration by 9% and 18%, respectively, and sharp curettage by 6% and 13%, respectively, compared to not using ripening. We also disaggregate the costs of the procedures according to the type of anesthesia used. For a detailed description of these cost estimations, see “Supplemental File 2, Table 2.”
Total costs estimated per procedure, in 2020 US dollars.

Abbreviations: MA, medical abortion; MVA, manual vacuum aspiration; SC, sharp curettage.
Figure 1 shows cost composition by input category. For manual vacuum aspiration and sharp curettage, the staff costs accounted for the largest percentage of the total (between 57% and 72%). The second most expensive category for manual vacuum aspiration and sharp curettage was imaging and lab studies. For medical abortion with misoprostol only, the most expensive category was imaging and lab studies, while for medical abortion using misoprostol combined with mifepristone, the most expensive inputs were medications. While clinical practice guidelines on abortion management are against the routine use of ultrasound, and it has been shown that its use does not have an impact on the efficacy and safety of abortion,28,29 we found in our study that more than 80% of the physicians interviewed used ultrasound routinely.

Breakdown of total procedure costs by input categories, USD 2020.
Figure 2 shows the staff costs breakdown. As the distribution is similar regardless of the cervical ripening method, we present only one column per procedure. For manual vacuum aspiration and sharp curettage, the costliest staff category was nursing. For medical abortion, Ob/gyn category represented the highest percentage of the total. After nursing and Ob/gyn, the costliest category was medical residents.
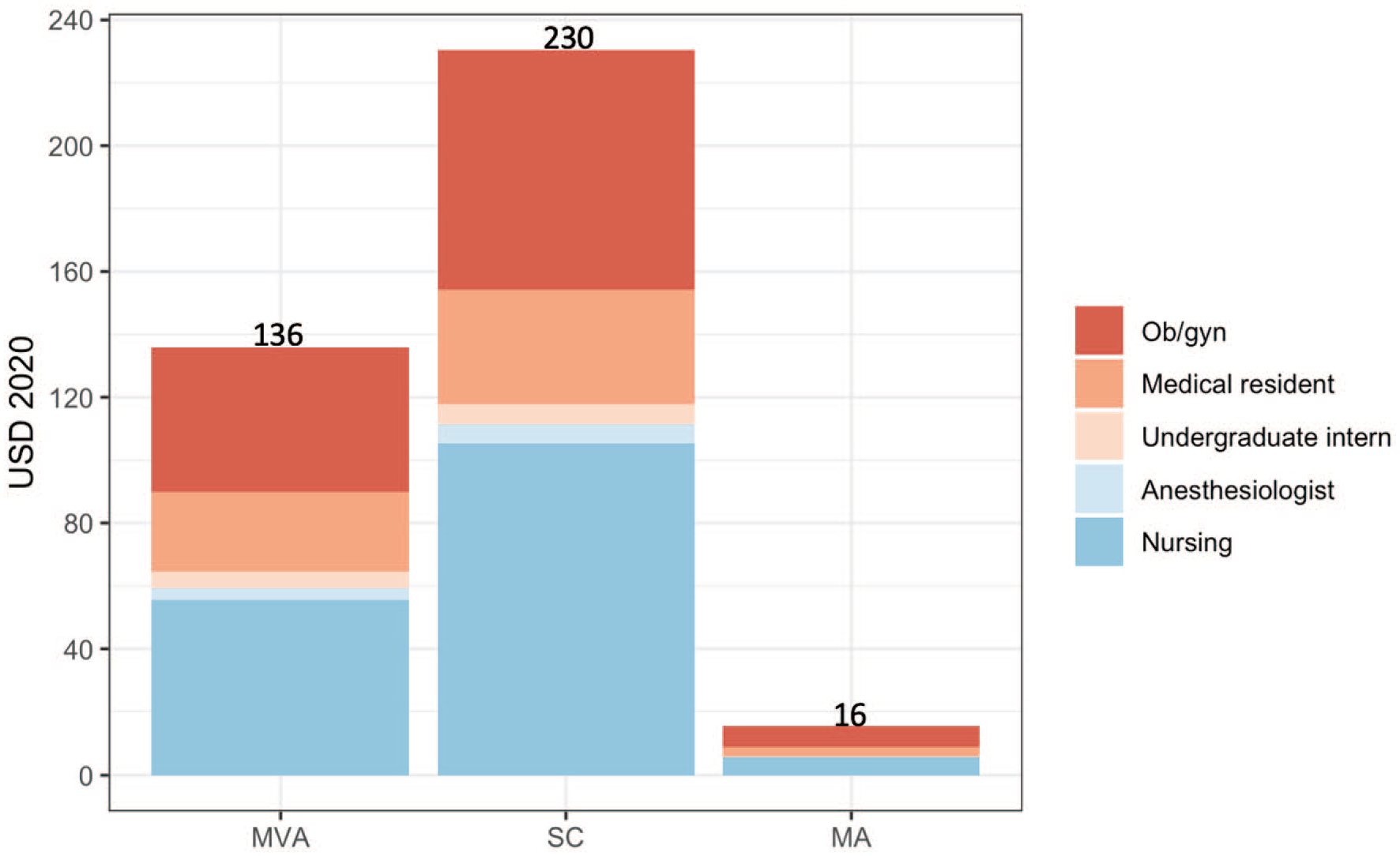
Breakdown of staff costs per procedure by type of staff category.
Details on staff time allocation are shown in “Supplemental File 2, Figure 1.” Medical residents and undergraduate interns were the cadres who allocated the greatest number of weekly hours of work (around 25%) to treating women undergoing a first-trimester abortion, of which 10% to 14% was spent on treating women who undergo manual vacuum aspiration. Overall, staff reported that they spend most of their time treating patients who undergo manual vacuum aspiration. The anesthesiologist was the category that spends the least amount of time on abortion procedures.
Patient flow and costs per hospital area
With the intrahospital patient flow description, we made a decomposition of the costs of each abortion method according to the hospital area where the supplies are spent.
Figure 3 shows the breakdown of total costs by hospital area. The highest proportion of manual vacuum aspiration and sharp curettage spending occurs in hospitalization; due to the staff time spent on post-procedure surveillance, as well as the supplies costs and hospital stay. For both procedures, the second most expensive area was the emergency room and the third was the operating room. In medical abortion with combined medication, approximately 60% of the total cost is spent in the emergency room, mainly due to the cost of misoprostol and mifepristone that are initially provided in that area. In both cases of medical abortion, the cost of the outpatient visit includes the follow-up studies that are requested on a routine basis.

Breakdown of total costs by hospital area involved in each type of procedure.
Discussion
The present analysis constitutes an updated description of the costs of the abortion methods used most often to treat women undergoing first-trimester abortion in public hospitals in Mexico. Currently, the only information available on the costs of abortion interventions in Mexico comes from a study with information from 2005, before the legalization of abortion, 15 for which it was necessary to make an update based on the current context and the new technologies.
Our micro-costing approach allows us to identified costs by input category and, in a novel way, the costs by hospital area involved. It describes in detail health staff costs through their time allocation, as well as the costs of staff in training (medical residents and undergraduate interns), who play a critical role in Mexico public hospitals. We calculated cost ranges based on the possible combinations of inputs reported by the hospitals, which reflects the cost of “real-life” implementation and not the cost based only on clinical practice guidelines. This is relevant for decision-making in the hospital management setting, as it helps identify relevant inputs and their impact on costs, thus contributing to the most efficient use of resources.
As has been reported in the literature, our findings showed that the most expensive procedure is sharp curettage.11,12,15 This is mainly due to the fact that sharp curettage requires longer post-surgical surveillance in the hospital with the corresponding expense in supplies and staff time. Therefore, in addition to being contraindicated according to clinical guidelines, cost considerations do not recommend the use of sharp curettage either, so this procedure should not be used in practice. Conversely, the unit cost of medical abortion is lower in comparison to surgical methods due to lower staff costs, as no hospitalization is required.
As in a previous study, we found that the staff cost category is the one that contributes the most to the cost of manual vacuum aspiration and sharp curettage. 15 Conversely, the staff cost for medical abortion is lower in comparison to the other methods, as no post-surgical surveillance is required.
The cost of surgical abortion (manual vacuum aspiration or sharp curettage) increases significantly with the use of cervical ripening, with either misoprostol or mifepristone. It has been reported in previous studies that mifepristone has greater or equal efficacy than misoprostol but at a higher cost.30,31 However, despite the fact that the choice of one or the other drug is based on availability, cost, convenience, and preference; the use of cervical ripening is not routinely recommended in the first trimester. 8 Therefore, the routine use of drugs for cervical ripening implies an additional cost that can be avoided, not only because of the medication costs but also because mifepristone also increases the length of hospital stay, having to be administered 24 hours before the abortion. 32 The same case occurs with the cost of imaging studies, which we find highly requested by doctors in our study, despite the fact that international consensus does not recommend their routine use.28,29 This highlights the importance of promoting good clinical practices and cost-saving recommendations in order to avoid unnecessary costs.
Several policy implications emerge from our findings. The first is in relation to current international recommendations, which establish that health services should switch from sharp curettage to manual vacuum aspiration or medical abortion and, if possible, prohibit the practice of sharp curettage. For instance, in Mexico, many hospitals practice sharp curettage as the first choice of treatment for first-trimester abortion, 17 despite the global guidance and trends by WHO and FIGO against it.7,10 Although both procedures have similar success rates,33,34 the evidence has shown a higher rate of complications pain, and discomfort for women treated with sharp curettage and also, higher costs, as has been corroborated in this study.15,16,35 Therefore, health personnel should be trained to offer women safety and less expensive alternatives such as medical abortion and manual vacuum aspiration.
Other cost-saving recommendations have to do with task shifting from Ob/gyn to general practitioners or from Ob/gyn to nurses. As we found in this study, in Mexican public hospitals nurses are a constant part of the staff of every procedure, no matter which provider cadre actually performs it. This is particularly important because the WHO guidelines for health workers’ roles in providing safe abortion establish as a recommendation that both, manual vacuum aspiration and medical abortion procedures in the first trimester of pregnancy, can be carried out only by nurses, midwives, or non-specialist doctors.33,36 Abortion services provided by nurses and midwives have been documented to be just as effective, of higher quality, and with less over-medicalization and unnecessary practices compared to those provided by physicians. 37 According to WHO guidelines, self-management abortion is as effective as assessment by a trained health worker and results in more satisfaction with the process. 38 Therefore, one cost-saving alternative is to make nurses eligible as providers and get rid of the unnecessary and substantial costs of all rest staff involved, and promote the use of alternatives such as self-management abortion since they provide higher quality and satisfaction, with the same effectiveness but with less use of resources. Future analyzes must focus on obtaining estimates of the costs of these other alternatives, as well as obtaining data on the quality of care and satisfaction.
Another important aspect is the impact that the inappropriate use of inputs has on the total cost. As we mentioned previously, the cost-saving recommendations apply to inputs: the use of unnecessary cervical ripening medications, ultrasounds, and blood tests should be restricted and, if possible, prohibited in cases where the evidence has shown not to be necessary.
Due to the high costs of hospitalization and post-surgical care, another recommendation has to do with promoting the routine performance of manual vacuum aspiration out of the operating room and hospitalization to routinely outpatient procedures. The cost estimate by hospital area can also yield valuable information that may contribute to the appropriate distribution of commodities and resources within hospital units. For instance, care and treatment in an emergency room and hospitalization areas for manual vacuum aspiration versus medical abortion can be performed in a consultation room on an outpatient basis.
Our study is not exempt from limitations. First, one important limitation is the lack of precision in estimating the staff’s time allocation due to the potential recall bias, as it was not possible to implement an approach other than phone interviews (such as direct observation), due to hospital dynamics resulting from the COVID-19 pandemic. Another limitation is, as we described above, that we did not estimate overhead costs due to the challenge of doing this in hospital units that treat patients in multiple specialties; however, we assume that overhead costs are similar for the different abortion methods assessed.
We also do not include costs from the perspective of the patients, such as transportation, lodging, food, etc., since the objective was not to describe the cost from a social perspective. However, despite these limitations, the results can be useful for decision-makers and health system institutions, for planning and budgeting, as well as for developing cost-effectiveness analyzes of the new technologies used in first-trimester abortion in countries with contexts similar to that of Mexico.
Finally, our study focused on public hospitals of the Ministry of Health and did not include other institutions such as the private sector. However, as mentioned before, abortion procedures in Mexico are performed mainly in second-level public hospitals, such as those included in our study. Our cost estimates and the cost composition analysis will be useful for policymakers to consider investing in options that are safer and more effective, but at the same time less expensive for the public health system.
Supplemental Material
sj-docx-1-his-10.1177_11786329221126347 – Supplemental material for Cost Analysis of Surgical and Medical Uterine Evacuation Methods for First-Trimester Abortion Used in Public Hospitals in Mexico
Supplemental material, sj-docx-1-his-10.1177_11786329221126347 for Cost Analysis of Surgical and Medical Uterine Evacuation Methods for First-Trimester Abortion Used in Public Hospitals in Mexico by Jorge Eduardo Sanchez-Morales, Jose Luis Rodriguez-Contreras, Leslie Ruiz-Lara, Beatriz Ochoa-Torres, Mara Zaragoza and Karen Padilla-Zuniga in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329221126347 – Supplemental material for Cost Analysis of Surgical and Medical Uterine Evacuation Methods for First-Trimester Abortion Used in Public Hospitals in Mexico
Supplemental material, sj-docx-2-his-10.1177_11786329221126347 for Cost Analysis of Surgical and Medical Uterine Evacuation Methods for First-Trimester Abortion Used in Public Hospitals in Mexico by Jorge Eduardo Sanchez-Morales, Jose Luis Rodriguez-Contreras, Leslie Ruiz-Lara, Beatriz Ochoa-Torres, Mara Zaragoza and Karen Padilla-Zuniga in Health Services Insights
Footnotes
Acknowledgements
The authors would like to thank Maribel Lopez and Catalina Munoz for their assistance with conducting interviews.
Author Contributions
All authors contributed to the conceptualization of this research.LRL, BOT, MZ, and KPZ contributed to the project administration and coordinated data collection.
JESM, JLRC, LRL and BOT helped with the methodology.
JESM and JLRC contributed to the analysis.
JESM and JLRC prepared the original draft.
All authors reviewed, edited, and approved of the final version.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.