
Abstract
While the burden of neurological and mental disorders has been drastically increased in Vietnam, the current mental healthcare services do not meet the public demand. In order to determine perceived barriers to the use of mental health services, we conducted a cross-sectional study on 376 elderly people from a rural district in Hanoi, Vietnam. We found that depression may be an important indicator of the need for formal and informal community and home care mental health services. Barriers to mental healthcare access were categorized into 7 groups namely stigma, emotional concerns, participation restrictions, service satisfaction, time constraints, geographic and financial conditions, and availability of services. The most significant barriers are the limited availability of and accessibility to health professionals and services in rural areas. Our study highlights the urgent efforts that need to be made in order to enhance availability of mental healthcare services in rural areas of Vietnam.
Background
As a result of longer life expectancy and decreasing fertility rates, the world population is rapidly ageing. 1 Studies indicate that at least 20% of seniors will suffer from a mental or neurological disorder and these disorders which account for 17.4% of their Years Lived with Disability (YLD). 2 The most common mental and neurological disorders among this age group is depression, accounting for approximately 7% of the world’s elderly population. 2 When undiagnosed and untreated, it can lead to physical, social and functional impairment, thereby contributing to lowering quality of life and in more severe cases, to suicide. 3 Although the demand for disease screening and management has continuously increased, available health care services remain very limited.4–7 Many countries share the gaps between high demand and supply of mental health services. 8 Furthermore, the proportion of mental health care utilization remains, accounting for only 30% of all cases.5,9 A study by Mohr et al 10 revealed that more than half of elder adults perceived at least 1 barrier to the access and utilization of psychological services. The situation is even worse in the rural where relevant services and transportations are substantially limited. 5
Vietnam is one of the fastest ageing countries in the world and will become an ageing nation by 2035. 11 While multiple mental health burdens are documented among the Vietnamese elderly, depression accounts for the highest percent (approximately 17%). 11 Although mental illness accounts for a significant proportion of the disease burden of the elderly, there is not any specific policy document related to mental health care services. 11 The burden of providing healthcare for neurological and mental diseases continues to increase as a consequence. There are 2 types of elderly health care services for the elderly in Vietnam 12 : (1) geriatric hospitals managed by the Ministry of Health; (2) social protection centres and private health care centres for the elderly managed by the Ministry of Labor, War Invalids and Social Affairs. 12 However, the current health care system does not meet the demand for mental healthcare, and there is a significant lack of large-sale screening and managing for mental health disorders. 13 At the grassroots levels, there is no standardized screening guidelines for early detection of depression. 11 Understanding barriers to mental health services would enable policy makers and service providers to develop pragmatic strategies. To date, there was limited available data on perceived barriers to mental health services among this population, particularly for individuals in rural environs of Vietnam. Thus, our study aimed to determine the perceived barriers and some factors associated with not seeking and using mental health services among older people in a rural area of Vietnam. The results from this study will enrich the current understanding of barriers to utilization of mental health services in rural elderly populations and inform the development of pragmatic solutions to promote healthcare access and quality in the future.
Methods
Study settings and design
A cross-sectional study was conducted in Chuong My District – a rural district located in the west of Hanoi, the capital city of Vietnam.
Study participants
Participants included those aged from 60 years old and above who lived in Chuong My district in the last 12 months and were able to understand and answer the provided questions.
Sample size and sampling technique
The study sample was calculated using the one-proportion sample size formula. The calculated sample size was 380 people. Participants were selected using non-probability, self-nominated sampling.
A 2-stage sampling technique was employed: (1) randomly select 2 communes from a list of 33 communes divided by economic status (high and low income); (2) 190 elderly adults were randomly chosen from each of the 2 selected communes. The randomly selected individuals were then invited to participate in a face-to-face interview. The response rate was 98.9%, with a total of 376 elderly people agreed to participate in the study with the response rate as 98.9%.
Study variables
Dependent variable
Barriers to access to psychological services was measured using the Perceived Barriers to Psychological Treatment (PBPT) scale 10 which contains 27 items. Each item is to ‘rate the degree to which different kinds of problems might get in the way of seeing a counsellor or a therapist’. Response choices comprised the following: 5 (impossible), 4 (extremely difficult), 3 (moderately difficult), 2 (slightly difficult), or 1 (not difficult at all). A cut-off score of 3 or higher in each item is identified as higher risk in perceived barriers to psychological treatment.
Independent variables
Demographic characteristics included (1) gender (male, female), (2) age group (60-70 years old, over 70 years old), (3) religious (yes, no), (4) education level (under-high school, high school and over high school), (5) employment status (unemployed, employed), (6) family member (living with spouse, living with offspring, living apart with partner and living alone), (7) economic status (poor family and not-poor family), (8) visit doctor in the last 12 months (yes, no).
Demand for mental health services was determined by asking the following question: ‘Have you had a need for mental health services in the past 12 months?’ (‘yes’ coded ‘1’ and ‘no’ coded ‘0’)
Depression status was evaluated using the Patient Health Questionnaire (PHQ-9) scale. 14 The Vietnamese version of PHQ-9, which has high validity and reliability, was used to screen for depressive symptoms. 15 A cut-off score of 10 or higher was used as this is the score at which referral for counselling or psychotherapy is recommended for depression status.
Perceived social supports were evaluated by using the Multidimensional Scale of Perceived Social Support (MSPSS). 16 The 7-point scale contains 12 items referring to social supports from different sources including family, friends and a significant other. The Vietnamese version of this scale was validated suggesting its potential as a useful tool to measure social supports in Vietnamese samples. 17 In this study, we compared the frequency of each item and the mean score between 3 groups: family support, friend support and significant other support.
Data collection
A community-based sampling survey was conducted during 2 months from July to August 2019. The questionnaire was designed using Kobo Toolbox tool- a web-based platform for data collection. We collected data via face-to-face interviews using a tablet. The data waives waivers were automatically transferred to Kobo Toolbox’s website at the end of each day. Then, the final data was exported to Excel for data cleaning.
Data analysis and statistical methods
Data analysis was performed using STATA version 14.0 (Stata Corp. LP, College Station, TX, USA). Descriptive statistical methods were used to summarize data on socio-demographic characteristics of participants. With regards to categorical variables, data were summarized using frequencies (n) and percentages (%) for categorical variables. We used exploratory factor analysis (EFA) to assess the construct validity of the PBPT questionnaire because the tool has not been tested in any previous studies in Vietnam. The Wilcoxon-Mann-Whitney test was used to determine the association between the social supports and the perceived barriers to psychological treatment of participants. A p-value of less than 0.05 was considered statistically significant. Multivariable logistic regression was applied to identify factors associated with the barriers to psychological treatment among respondents. The regression model was combined with stepwise forward selection strategies, using the P-value of log likelihood of less than 0.1 to build the final reduced model.
Ethical considerations
Ethical approval for our study was obtained from the Institutional Review Board of the Hanoi University of Public Health (HUPH) in Vietnam under Decision No. 406/2019/YTCC-HD3. All study participants were introduced to the study and asked to give their written informed consents. Participants’ involvement was voluntary and they could withdraw from the survey at any time. Participants’ information was taken confidentially and only used for the purpose of this study.
Results
Table 1 describes the general characteristics of respondents. A total of 376 elderly people were enrolled in this study with the average age of 71.7 years old (SD = 7.9). The majority were 70 years old or above (52.7%). There was no significant difference between the age groups in the demand for mental health services regarding their age. The majority of participants were female (66.5%) and non-religious (77.9%). They also had significantly higher demand for mental health services (P < 0.01). Nearly 86% of participants obtained less than high school education, 50.3% still worked, 93.1% lived with family members and 93.4% belonged to the not-poor household economic status (93.4%). Notably, more than one-fourth of participants were at risk for depression and 88.8% of respondents reported they had visited a clinic at least once in the last 12 months (for health check, diagnosis, or treatment).
Socio-economic characteristics of the participants.
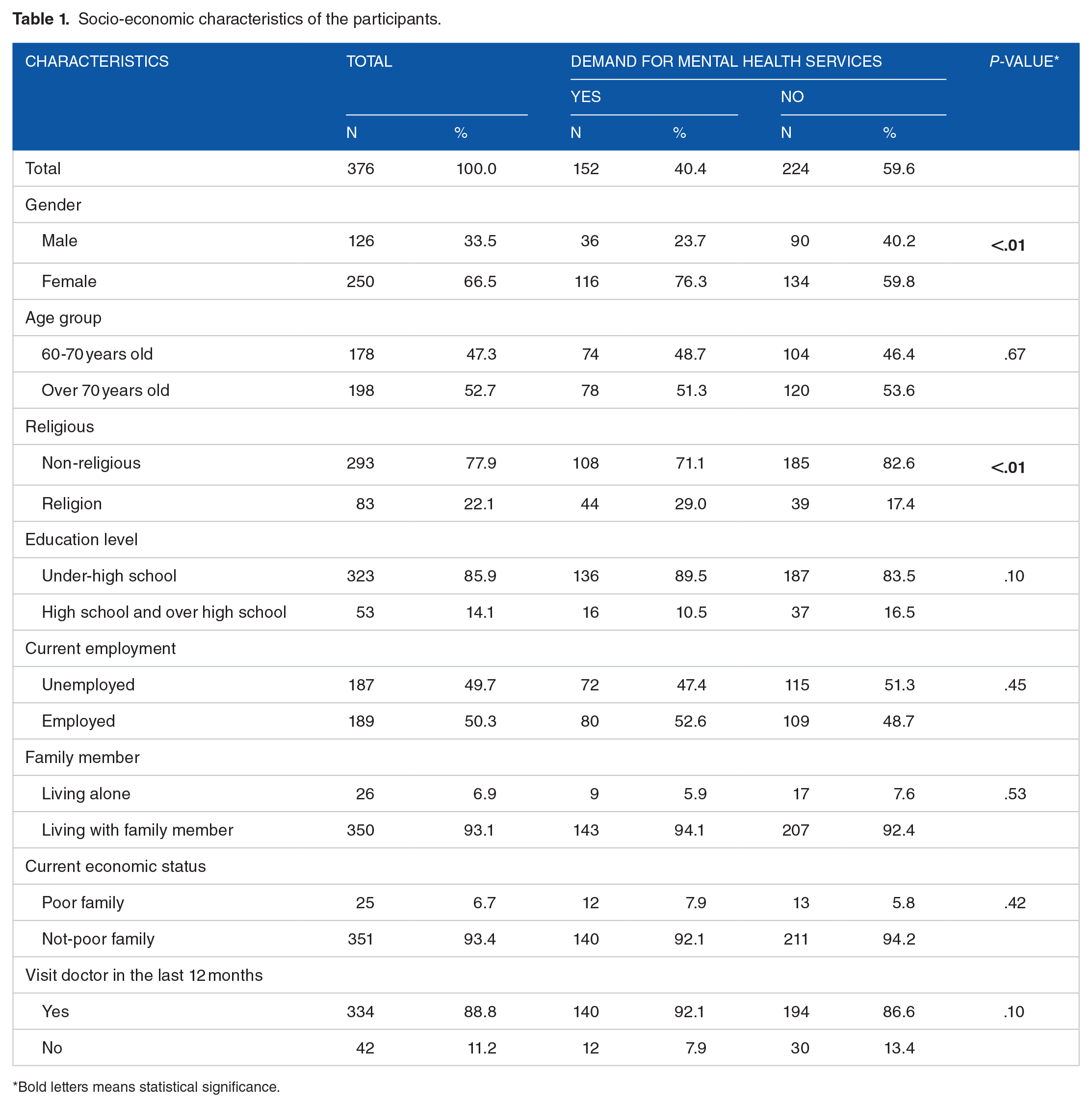
Bold letters means statistical significance.
Table 2 presents the construct validity of the PPBT questionnaire. Seven dimensions pertaining to the difficulties to accessing psychological treatment services were defined from a factor analysis. The 7 dimensions are as follows: stigma, emotional concerns, participation restrictions, service satisfaction, time constraints, geographic and financial conditions, and availability of services. The Cronbach’s alpha values for each of the dimensions were 0.84, 0.82, 0.90, 0.77, 0.77, 0.63 and 0.75, respectively. Among those, the participations restrictions (3.34 ± 1.14), the availability of treatment services (2.72 ± 1.23) and the geographic & financial accessibility (2.67 ± 0.99) were found as the major problems that hinder elderly people seeking psychological services.
Factor loading and reliability of measurements of perceived barriers to psychological treatment items.

Table 3 describes the frequency of receiving social support from family, friends, and a significant other as well as the association between social support and the demand for mental health services. The participants received the most supports from their family (5.5 ± 1.2 mean score). In which, with over 80% of them expressing that they could share their problems with their families and thought that their family was willing to support them. With regards to support from friends, there were about over one-third of participants felt comfortable when talking about their problems, joy and sorrows with their friends. In terms of support from a significant other, only nearly 60% of respondents said that they could share their joys and sorrows with their significant other.
The association between perceived social support and demand for mental health services.

Bold letters means statistical significance.
Notably, the frequency demand for mental health services among respondents who have support from family, friends and a significant other was slightly lower than the demand among their counterpart. The demand for mental health services was lower among those who had support from their family to make decisions (P = 0.03). This trend was similar to the elderly who could count on their friends when things went wrong, felt comfort when sharing joys and sorrows with their friends or a significant other (P < 0.05).
Table 4 describes the frequencies of perceived barriers to psychological treatment and factors associated with PBPT among participants. In general, the respondents with greater levels depression reported at least 1 barrier to psychological treatment more frequently than their counterparts. Statistically significant differences were seen between those with greater levels of depression and those with lower levels or no depression across all 7 groups of barriers except for time constraints.
Some factors associated to perceived barriers to psychological treatment among participants.

P < .01. **P < .05. *P < .1.
Perceived barriers to psychological treatment including stigma, emotional concerns, participation restrictions, service satisfaction and geographic and financial conditions decreased significantly by 0.55, 0.4, 0.42, 0.47 and 0.37 times respectively among elderly people having demand for mental health services.
Depression was a strong predictor of 5 out of 7 in the perceived barriers to psychological treatment among participants. Respondents with depression have a significantly higher likelihood of facing barriers related to meet emotional concerns (OR = 2.93, 95%CI = 1.74-4.86), participation restrictions (OR = 2.67, 95%CI = 1.59-4.49), geographic and financial accessibility (OR = 2.43, 95%CI = 1.42-4.17), availability of services (OR = 1.58, 95%CI = 0.94-2.66) and a lower likelihood of having service satisfaction stigma (OR = 0.59, 95%CI = 0.35-0.97).
In terms of receiving supports, elderly people who have participation restrictions received family supports are significantly higher 2.82 times than their counterpart while they received significant other supports are significantly less than those who did not have physical health problems. In addition, receiving support from a significant other was associated with the time constraints barrier (OR = 1.55, 95%CI = 0.94-2.57).
Discussion
Barriers to access mental health services
We found 7 barriers to accessing psychological treatment services: (1) stigma, (2) emotional concerns, (3) participation restrictions, (4) service satisfaction, (5) time constraints, (6) geographic and financial conditions and (7) availability of services. These results correlate with previous systematic reviews18,19 showing that the most common barriers to accessing psychological treatment services included concerns related to stigma, shame and rejection, participant restriction, lack of knowledge and treatment-related doubts, fear of negative social consequences, and limited resources, time, and expenses. 19 Inconsistently, a study by Mohr et al 10 which utilized a similar questionnaire revealed 8 barriers including stigma, lack of motivation, emotional concerns, negative evaluations of therapy, misfit of therapy to needs, time constraints, participation restriction and availability of services. These discrepancies might be attributed to geographic differences; while this current study was conducted in a geographically disadvantaged location, the Mohr et al 10 study was carried out in a wealthier locations, namelyChicago, United States. 10
Stigma and emotional concerns
Our findings are consistent with a previous study indicating that self-stigmatization of mental illness and fear of judgement from families, friends and others prevent people from seeking the mental health services. In addition, our study found that emotional concerns included 5 items that reported about upsetting feelings in counselling and motivation to seek help. This finding is also consistent with conclusions from the previous reviews within the rural population.5,10 To date, stigma and feelings of embarrassment associated with seeking help for mental health are widespread in Asia. This can potentially lead to delayed presentation in mental healthcare. In Vietnam, the definition of mental illness refers to those with severe psychiatric abnormalities or madness that could not only afflict those suffering from mental health illnesses but others as well. 20 As a result, instead of seeking mental health services, some may deny or hide the existence of their disease. To solve this problem, it is crucial to change the public’s perspectives through massive education campaigns.21,22 The correct understanding of the meaning of mental health will help reduce its social stigmatizations and prejudices associated with it, thereby encouraging those suffering from mental health illnesses to seek relevant medical care in Vietnam.
Time constraints
The EFA showed that the time constraints factor, which consists consisted of 3 items related to household responsibility, could limit access to the mental healthcare. This finding is consistent with those of various other studies.18,19 This may be partially attributed to the long-standing practice of co-parenting in Vietnamese culture. 21 It is particularly the case in the rural areas where old people, instead of enjoying their retirement, spend their whole day taking care of their grandchildren. It is necessary to increase the support from family members for the elderly people such as supporting with going to regular check-ups for prevention and early detection of abnormal symptoms. Also, in order to timely detect signs of mental health disorders in a timely manner, grassroots healthcare settings, like commune health centres, should act as an initial gatekeeper to assist with routine mental health screening and quickly refer patients to appropriate facilities. To do this, there is a need for the development of a standardized, community-based screening tool for mental health disorders which could be used as a part of the routine care in grassroots healthcare settings in Vietnam.
Availability of services
In accordance with a large body of literature on the topic,4,5,22 our study suggests that limited services is a barrier for seeking official mental support. Mental health problems are highly prevalent among the elderly in rural areas. However, there is a paucity of available mental health professionals and services and people may find it difficult to find a source close by at the local grassroot level. This emphasizes the importance of enhancing the human resources for mental health services in rural areas, and improving the accessibility to these services for the elderly.
Participation restrictions
There are only a limited number of studies which identify participation restrictions, which consists of 3 items related to physical health illness or disability in Activities of Daily Living (ADLs), a barrier to accessing psychological services. 23 However, findings from our study indicate that in rural settings, where there is a paucity of available transportation for disabled people, people with limited ability to carry out ADLs tend to face difficulties in going out and seeking help.
Service satisfaction
The EFA analysis showed that the service satisfaction factor, which consists of 4 items related to bad experiences or distrust with counsellors, is a barrier to accessing psychological services. This finding is consistent with findings from previous studies, 22 which reported that trust in the counsellors led to greater help-seeking intentions. Concern about negative experiences with therapy may also relate to stigma, where a fear of a breach in confidentiality stems from the fear of stigma and embarrassment that friends or families can find out that an individual had sought help. 24
Geographic and financial conditions
Consistent with findings from other studies on the topic, our study suggests that limited transportation, not having health insurance and financial disadvantages would prevent the elderly from seeking needed mental health services.25,26 In fact, the cost of treatment and lack of financial resources often prevent the elderly from accessing to mental health services, even when insurance or financial assistance is available. Conducting health literacy interventions on positive coping strategies should be given more attention. Through these, the elderly will learn how to better cope with their mental health issues.
Elderly in rural Vietnam identified a variety of barriers to access mental health care. One of the most recognized barriers is the limited availability of and accessibility to health professionals and services in rural areas. Along with other barriers, such especially geographic and financial accessibility, for elderly people in rural areas, participation restrictions are also a critical barrier to accessing psychological services. To the best of our knowledge, this is the first study to systematically explore barriers to accessing psychological services the older population face in Vietnam. Given the fact that PBPT is widely used in Vietnam, future researches should focus on the feasibility of using this tool for different populations.
Factors associated with the perceived barriers to psychological treatment
Our study found that those with perceived higher levels of depression were less likely to seek mental health services. This finding is consistent with observations from other studies.5,10,26 In our study, depression was a strong predictor of significantly increasing perceived barriers in most of the domains, with the exception of time constraints. About two-third of depressed older people (PHQ ⩾ 10) reported at least 1 barrier in participation restrictions, geographic and financial conditions and availability of services domains. These domains are considered as major barriers to service utilization and engagement.4,5,27–29 Moreover, elderly people either might not perceive their problem as a mental illness or might not know that they could be treated if they seek assistance through mental health services. It is also more difficult to screen and care for rural elders because of the shortage of professionals trained to identify and treat mental illnesses, as well as the stigma associated with mental health problems. 4 On the other hand, providing mental health services in rural areas or where transport is difficult, and resources are concentrated in a single central, typically urban area, is a common practical problem in many developing countries, 8 and Vietnam is no exception. While people in the urban benefit directly from health facilities for the elderly, more than 70% of Vietnamese elderly live in rural areas, where limited financial resources are available, 30 and thus have difficulties with accessing health services. 31 Since elderly people with depression are especially vulnerable to barriers of mental health services, we propose that the interventions should target these seniors. Depression may be an important indicator of the need for formal and informal community and home care of mental health services.
Low perceived need is also considered as the major barrier to seeking and complying with treatment for individuals with common mental disorders worldwide. 32 The relations between greater demand for mental health services and increased barriers to psychological treatment have been examined in previous studies.26,33,34 In our study, perceived barriers to psychological treatment including stigma, emotional concerns, participation restrictions, service satisfaction and geographic and financial accessibility, decreased significantly among elderly people having a demand for mental health services. However, disorder specific needs were not assessed in our study as we grouped all those who had a demand for mental health services in the last 12 months together. Notwithstanding this limitation, our results might well reflect the fact that lack of perceived need for healthcare is an even more important barrier. Therefore, identification of the demand of elderly people for mental health services is necessary to provide them with the care and services they need and improve the quality of life for Vietnamese elders in living in rural communes.
In terms of receiving supports, increased interactions with family, friends or a significant other contributes to maintaining good psychological health for elderly people. Our results confirmed that as the barriers of the elderly for mental health services is increasing, supports from family members of the elderly is also on the rise. In our study, those with participation restrictions received more support from families but less support from significant others than the counterparts. This finding was not surprising, because seniors with few or no functional limitations may not even be aware of state long-term care contexts. 35 Thus, the protective effects of support from family, friends or a significant other have not been significantly associated with most of barriers to mental health treatment. Perhaps, regardless of their current mental health status, the elderly usually have a sense of informal support availability. Only when specific needs arise do elderly people seek specific services and identify perceived barriers they may encounter. Most elderly people living in rural areas rely on their spouses, family members or informal support networks to assist them with their financial, household and other needs. Understanding the features of family and other social supports of elderly people is critical to understanding disparities that might occur in their long- term care needs. 36 Therefore, the future researches should shed light on the link between social supports and perceived barriers so that we can strengthen specific social supports to reduce barriers to mental health services for seniors.
Limitations
Several study limitations should be noted. First, the study participants were randomly selected from the list of households provided by local authorities in the rural district of Hanoi, Vietnam. Thus, to validate the generalizability of the results for the elderly in rural Vietnam, the study should have involved more participants from different regions and districts. Secondly, in terms of the measures, the PBPT scale was initially designed for use in Western countries and was not tested in Vietnam. Thus, further studies need to be performed to determine its validity and reliability.
Conclusion
In conclusion, elderly adults in rural Vietnam identified endorsed a variety of barriers to accessing mental healthcare. The availability of services and geographic and financial accessibility are the most common t barriers to accessing mental healthcare services. To better meet the mental health needs of elderly people living in rural area of Vietnam, it is crucial that mental health services are available, readily accessible and address the rising need for mental illness to improve their quality of life of the rural elderly population as well as reduce mental health service disparities.
Footnotes
Acknowledgements
The authors sincerely thank the Chuong My District Health Center and the elderly people for their enthusiastic participation in this study. We would also like to thank the interviewers who contributed to the data collection process.
Author Contributions
Conceptualization: N.HNV; methodology: N.HNV and N.TKH; formal analysis: N.TL and N.TKH; writing—original draft preparation, N.HNV and N.TKH; writing—review and editing: N.TL, M.TH, P.QT, D.MD, V.TTM and T.TH. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Hanoi University of Public Health, Vietnam.