
Abstract
Diabetes treatment cost represents an ever-growing problem. The adoption of new drugs in therapy, although they can guarantee an improvement in patient’s quality of life, can meet obstacles when it involves an increase in costs. We decided to compare the costs and benefits of the new saxagliptin and dapagliflozin combination versus traditional therapies. Bodyweight loss and the sharp reduction in hypoglycemic episodes were the 2 main clinical outcomes that emerged from registered studies of saxagliptin and dapagliflozin compared with the sulfonylureas. These results, combined with the good cardiovascular risk profile, led to develop a cost-utility analysis. We aimed to show the economic value of this new association therapy. We carried out a cost-utility analysis from the Italian National Healthcare System (NHS) perspective, focused on direct costs related to the treatment and management of main diabetes complications. Utility scores adopted have been measured based on the patient’s perception of weight changes. In light of the better durability profile of saxagliptin/dapagliflozin compared with gliclazide, we also considered a simulation scenario to assess the impact on costs of switching to basal insulin, starting from gliclazide and the fixed combination, respectively, and based on the related probabilities to switch. To assess the robustness of the results, a 1-way sensitivity analysis was performed by changing the main parameters by ±20%. Furthermore, the sensitivity of the results was tested considering the addition of a percent discount, because the purchase costs of drugs are usually subject to hidden discounts. We calculated the total direct annual cost per patient of saxagliptin/dapagliflozin versus gliclazide and insulin glargine for patients with type 2 diabetes mellitus not achieving glycemic control on metformin plus saxagliptin alone, dapagliflozin alone, or gliclazide at a lower dosage. Total treatment costs have been obtained adding the direct cost of the drug, needles, glycemic self-monitoring, hypoglycemic events, cardiovascular complications, and effect on consumption of other drugs. The total direct cost of saxagliptin/dapagliflozin fixed dose combination was €414.62 higher than gliclazide (€1.067.72 vs €653.10), and greater than basal insulin, with a difference of €166.99 (€1067.72 vs €900.72). Despite the higher annual direct total cost, the additional cost per quality-adjusted life year (QALY) gained, compared with gliclazide, has been €11 517, and €4639, when compared with insulin glargine in the base-case scenario, and the robustness of the results has been shown in the sensitivity analysis. The results of our cost-utility analysis, expressed as incremental cost-effectiveness ratios, were fully compliant with the threshold adopted for Italy. Then, saxagliptin/dapagliflozin can be considered a cost-effective oral hypoglycemic agent. The positive effect of this drug on the quality of life, induced by the bodyweight loss, has allowed this outcome, despite the higher annual cost per patient, mainly determined by the drug purchase cost.
Introduction and Objective
Diabetes represents a relevant public health problem worldwide due to its growing prevalence and socioeconomic burden. In Italy, over 3.2 million people are diabetic, that is, 5.3% of the total population. 1 In total, 72.9% of people with diabetes are treated with oral hypoglycemic agents (OHAs), and sulfonylureas are adopted in 20.3% of these patients. 2 Moreover, 18.8% of patients with diabetes in our country have HbA1c levels higher than 64 mmol/mol. 2 Patients with suboptimal metabolic control risk developing chronic and acute microvascular and macrovascular complications, as well as severe hypoglycemia that affects patients’ survival, quality of life, and costs. The correlation between diabetes and complications means that patients with diabetes not only have shorter life expectancy than the general population3-5 but also experience worse health-related quality of life (HRQoL). 6 Moreover, patients with diabetes-related complications have lower HRQoL than diabetes patients without complications.7-9 In addition to diabetes comorbidities, also impact of side effects of some antidiabetic agents, such as weight gain, should be considered. It has been shown that weight gain increases the risk of complications and significantly decreases HRQoL, treatment satisfaction, and treatment adherence.10-12
Tight glycemic control reduces the development of diabetic complications and long-term costs related to the disease.13-15 On the contrary, tight glycemic control is often neglected to avoid treatment-related hypoglycemia. 16 An economic evaluation of diabetic complications and antidiabetic therapies side effects is important for a chronic and high-cost disease such as diabetes. Moreover, the inclusion in health economic models of complications and drug side effects impact on HRQoL has become increasingly relevant over time, because subjective health status is an important aspect of the cost-effectiveness of treatments. From a health economics perspective, a preference-based measure of HRQoL is required to estimate health-state utility values and calculate quality-adjusted life years (QALYs). 9
Newer therapeutic agents for type 2 diabetes mellitus (T2DM) have improved benefit-risk profiles. Among the advantages it is worth noting the reduction of body weight, 17 and fixed-dose combinations of drugs with different mechanisms, now available, allow to add benefits of different drugs simplifying administration. Since 2006 diabetologists can take advantage of dipeptidyl peptidase-4 inhibitors (DPP-4i) as a valid therapeutic option to treat diabetes and reduce hypoglycemic risk as well. Saxagliptin is a highly potent and selective DPP-4i, which enhances glucose-mediated insulin secretion, reduces glucagon secretion, and lowers both fasting and postprandial blood glucose levels. 18 In clinical studies, saxagliptin monotherapy has been shown to reduce HbA1c by 0.4% to 1.1%, mainly depending on baseline HbA1c values.19,20 In 2015, sodium-glucose cotransporter-2 inhibitors (SGLT2i) joined the basket of OHAs. Dapagliflozin is a highly potent, selective, and reversible SGLT2i. It inhibits the reabsorption of up to 50% of filtered glucose, thereby inducing glycosuria of about 70 g/day and reducing fasting and postprandial glucose levels independently of insulin levels and without hypoglycemic risk for the patient. 18 Dapagliflozin has been shown to reduce HbA1c by 0.66% to 1.12%, mainly depending on baseline HbA1c values and duration of treatment.21,22 A single-pill combination of saxagliptin 5 mg and dapagliflozin 10 mg (Qtern®) has been approved for type 2 diabetes management in the United States and Europe. Saxagliptin/dapagliflozin shows a mean adjusted HbA1c reduction after 24 weeks of 1.47%, significantly higher than saxagliptin (0.88%) or dapagliflozin (1.20%) alone, and comparable to the efficacy of gliclazide at maximum dose (1.47% vs 1.78%), but with reduced hypoglycemic risk (severe hypoglycemia: none vs 0.06%) and a mean weight loss of 2 kg.23-26 Diabetes treatment costs represent an ever-growing problem. 27 The adoption of new drugs in therapy, although they can allow an improvement in patient’s quality of life, can meet obstacles when it involves an increase in costs. Hence, it is necessary to carry out cost analysis to compare costs and benefits of new drugs versus traditional therapies. Bodyweight loss and the strong reduction in hypoglycemic episodes (virtually none for Dapagliflozin) were the 2 main clinical outcomes that emerged from the registration studies of saxagliptin and dapagliflozin compared with the sulfonylureas. We decided to adopt these results combined with data about the good cardiovascular risk profile, to develop a cost-utility analysis, a type of cost-effectiveness study, to show the economic value of this single-pill combination therapy. Cost-effectiveness analysis describes the cost per unit health outcome obtained with an experimental intervention versus usual care. 28 It provides a measure of the value for the money spent and may be used to guide resource allocation. In the cost-utility analysis, health outcomes are measured by QALYs, a metric that adjusts the length of life for quality of life. Quality of life is assessed with health utility scores, measures that reflect the general population’s preference for specific health states. Health utility scores fall on a continuum between 1.0 and 0, where 1.0 represents perfect health and 0 represents death. QALYs are calculated as the sum of the product of the number of years of life and the quality of life in each of those years. The goal of an experimental intervention is to maximize the number of QALYs gained for the money spent relative to usual care. The cost-effectiveness analysis was developed considering the economic implications of CVD-Real studies I and II outcomes, focusing on the impact of weight changes on HRQoL.
According to the Italian National Healthcare System (NHS) perspective, we have considered only direct costs in our analysis. Specifically, we have used direct costs related to the treatment and management of the main complications of diabetes. Utility scores adopted for our cost-utility analysis have been measured based on the patient’s perception of weight changes. In line with the NHS perspective, we have not considered indirect costs in our analysis. However, as the burden of indirect costs is significant in chronic diseases such as diabetes, we have carried out a simulation scenario to assume the hypothetical effect of adding indirect costs on the results of our analysis. We have reported this effect in the discussion section.
Saxagliptin/dapagliflozin purchase cost has been recently published. 29 It is more expensive than other standard treatments but, due to its efficacy and safety, it may provide an improvement in the management of the disease, allowing a valid therapeutic option to control patients with diabetes avoiding the use of drugs that have been used for a long time in therapy, but that are associated with greater complications and costs. Our study has been developed precisely to evaluate this potential economic benefit for the Italian NHS based on clinical benefits and to assess the additional benefit deriving from the patient’s quality-of-life improvement.
Clinical Background
A Swedish study demonstrated that cardiovascular events increased risk in patients treated with sulfonylureas plus metformin versus the ones treated with DPP-4i plus metformin, showing an adjusted hazard ratio (HR) (95% confidence interval [95% CI]) of 1.17 (1.01-1.37). 30 This evidence provided important support for our analysis. However, the main contribution was provided by EMPA-REG study, 31 a double-blind randomized study versus placebo developed on 7020 patients with type II diabetes with high cardiovascular (CV) risk. This study analyzed long-term effects on cardiovascular morbidity and mortality of empagliflozin (an SGLT2i) in add-on to standard antidiabetic therapy. EMPA-REG study demonstrated for the first time the possibility to modify comorbidity and mortality of patients with diabetes employing an oral antidiabetic agent. In fact, empagliflozin treatment reduced the composite endpoint of the study, a composite of 3 MACE (major adverse cardiovascular events), by 14% (P = .0382) versus the control group. CV mortality cumulative incidence was reduced by 38% (P < .0001), hospitalizations for heart failure (HHF) were reduced by 35% (P = .0017), and mortality for all causes by 32% (P = .0001). 31 Moreover, empagliflozin reduced the nephropathy risk by 39% and also reduced body weight and blood pressure. 31 Empagliflozin treatment was mainly associated with metformin (74%), sulfonylureas (42%), and insulin (48%). The mean duration of treatment was 2.6 years, and the entire observation period was 3.1 years. This milestone study left 2 open questions: if it was a molecule-dependent or a class effect, and if the effects shown were also detectable in an unselected diabetic population. The recent publication of the CVD-REAL 32 study gave cogent answers to these questions. In this real-life study, data were collected via medical claims, primary care and hospital records, and national registries from the United States, Norway, Denmark, Sweden, Germany, and the United Kingdom. Propensity score for SGLT2i initiation was used to match the 2 treatment groups of 154 528 patients each, starting from a pool of 1 392 254 new users of SGLT2i or other glucose-lowering drugs (oGLD) fulfilling the eligibility criteria. In the SGLT2i class, canagliflozin, dapagliflozin, and empagliflozin accounted for 53%, 42%, and 5% of the total exposure time, respectively. There were 961 HHF cases during 190 164 person-years follow-up (incidence rate: 0.51/100 person-years), and use of SGLT2i versus oGLD was associated with lower rates of HHF (HR: 0.61; 95% CI = 0.51-0.73; P < .001) and death (HR: 0.49; 95% CI = 0.41-0.57; P < .001), with no significant heterogeneity by country. 32 So, this large real-life multinational study suggests that the empagliflozin benefits, shown in EMPA-REG randomized trial, may be applicable to a broad population of patients with type 2 diabetes not selected for CV risk. Moreover, the lack of heterogeneity in results, despite the different geographic use of the SGLT2i, suggests also a class effect. Following CVD-REAL, CVD-REAL 2 study, 33 analyzed an even broader sample of patients, (235 064 in each group after propensity-matching) from Australia, Canada, Israel, South Korea, Japan, and Singapore, treated with different SGLT2i (dapagliflozin, empagliflozin, ipragliflozin, canagliflozin, and tofogliflozin). This study confirmed the results shown in EMPA-REG and CVD-REAL studies, demonstrating similar hazard ratios: HHF (HR: 0.64, 95% CI = 0.50-0.82; P = .001), death or HHF (HR: 0.60, 95% CI = 0.47-0.76; P < .001), and myocardial infarction (MI) (HR: 0.81, 95% CI = 0.74-0.88; P < .001). Moreover, it showed a positive effect on the stroke incidence (HR: 0.68, 95% CI = 0.55-0.84; P < .001), which was an aspect not demonstrated in the above reported previous studies. In summary, with saxagliptin/dapagliflozin single-pill combination, we can achieve the same HbA1c level than with a maximum dose of gliclazide and insulin glargine basalization, but with lower CV and mortality risk, lower hypoglycemic risk, lower need of blood glucose self-monitoring tests, lower need of HHF, and, last but not least, with a reduction of weight and general improvement in the quality of life. In our study, we have tried to exploit the multiple benefits of this fixed-dose combination therapy from a pharmacoeconomic point of view, highlighting the impact on costs for the Italian NHS, but also considering the impact on the patient’s quality of life.
Materials and Methods
The study design adopted was a cost-utility analysis. We have applied this type of economic evaluation to the above reported clinical outcomes. The analysis was conducted from the Italian NHS point of view to evaluate the potential economic benefits deriving from the saxagliptin/dapagliflozin combination use. We have compared the costs of the new combination treatment versus gliclazide, both in add-on with metformin. We have developed our cost-utility model in Microsoft Excel® and we have considered also costs of the less expensive among basal insulin analogs, Abasaglar,® titrated to 20 IU, corresponding to the average dosage used for the treatment of patients with type II diabetes.34,35 We decided to evaluate also the cost of basalization with insulin analogs because the better durability profile of saxagliptin compared with gliclazide, and of saxagliptin/dapagliflozin as well (because the durability of dapagliflozin depends only on renal function), might delay the need of insulinization. 36 Therefore, we considered a simulation scenario that assesses the impact on the cost of the switching to basal insulin therapy, starting from gliclazide and saxagliptin/dapagliflozin combination, respectively. In this scenario, we have adopted the different probabilities to switch to insulin for the 2 therapeutic alternatives, considering a 4-year period. Costs of gliclazide were related to a 120 mg dose, corresponding mainly to the hypoglycemic effect of saxagliptin/dapagliflozin.23,24
Our model aims to estimate the direct cost associated with the treatments compared in this analysis and to find out the real gap in costs between saxagliptin/dapagliflozin combination and the apparently much cheaper gliclazide and insulin glargine, while evaluating potential economic benefits related to the single-pill combination and the impact of improvement in the quality of life. To assess the impact of changes in T2DM patient’s body weight on HRQoL, we used utility data from the literature, 37 and we have calculated utility values for weight changes related to saxagliptin/dapagliflozin, gliclazide, and insulin glargine. Finally, we have compared the difference between costs and utilities related to weight changes to assess the overall benefit for the patient taking saxagliptin/dapagliflozin. In this analysis, we have considered as direct costs all the resources consumed to provide health care services, as well as those used to counteract the possible adverse effects of the therapies used. Direct costs represent the public health decision-makers’ point of view. By comparing the total direct costs to the utility values, we have been able to quantify the benefits also on the quality of life. This was done based on body weight reduction, a fixed-dose combination therapy positive effect highlighted in clinical trials. The cost-utility analysis results were expressed as incremental cost-effectiveness ratio (ICER). It was calculated as the difference in the cost of the alternative therapies, divided by the difference in the QALYs. This Costs/QALYs ratio was then compared with a threshold (willingness to pay). Willingness to pay differs from country to country. Although no officially established value is available for Italy, it is worth noting that recent guidelines by the Italian Health Economics Association (AIES) recommend that a threshold of €25 000–40 000 be adopted. 38
To assess the robustness of the results, a 1-way sensitivity analysis has been performed by changing the main parameters by ±20%. Furthermore, as the purchase costs of drugs are usually subject to hidden discounts, except for generic products, the costs of which are included in a transparency list, the sensitivity of the results has been tested considering the addition of a percent discount. Specifically, to reproduce an economic evaluation as close as possible to the real direct cost paid by hospitals, we have tested the effects of increasing discount rates applied to ex-factory price (40%, 45%, and 50%).
Model description
Our model, developed in Microsoft Excel®, compared the costs of the above-mentioned therapeutic options, including costs of therapy management and side effects, both negative and positive, while the costs which do not vary within the different scenarios, such as costs of metformin and outpatients’ costs, were not included in the calculation.
To evaluate total direct costs, we have considered the following cost items:
The cost of the drug (including needles if injectable);
The cost of glycemic self-monitoring;
Direct costs related to hypoglycemic events;
Direct costs related to cardiovascular diabetic complications:
MACE (stroke and nonfatal MI)
HHF
Costs and gains related to the consumption or spare of other drugs (antifungals for urogenital infections and antihypertensive drugs).
We have calculated the total direct annual cost per patient of saxagliptin/dapagliflozin versus gliclazide and insulin glargine for patients with T2DM not achieving glycemic control on metformin plus saxagliptin alone, or dapagliflozin alone, or gliclazide at a lower dosage. Total treatment costs have been obtained adding the direct cost of the drug, needles, glycemic self-monitoring, hypoglycemic events, cardiovascular complications, and effect on consumption of other drugs.
The model, based on a 1-year time mark, was developed referring to Italian NHS and data were inputted by reference to the scientific literature, using Italian evaluation of costs whenever possible, and adopting internationally acknowledged data when it was not possible otherwise. We considered only direct costs according to the NHS perspective. The efficacy data considered for the analysis were glycemic self-monitoring frequencies, hypoglycemic event rates, cardiovascular complication rates, and the incidence of urogenital infections and hypertension in patients with diabetes, useful to assess the consumption of other drugs. Based on utilities data from the literature, 37 we calculated utilities values for weight changes related to saxagliptin/dapagliflozin, gliclazide, and insulin glargine. Finally, we obtained ICER for these treatment options.
Model input data
Cost of drugs
To determine purchasing cost of drugs, for each product we considered the price that can more appropriately reflect real spending on the NHS (ASL). Specifically, the price based on the reimbursement band provided and the possible adherence to the payback were considered.
For generic products public list prices were adopted, while for the other drugs costs were deducted from ex-factory prices (with −5% to 5% mandatory rebates if not subject to payback or with −5% if it is applicable). 39 We calculated the annual direct cost per patient of each drug using the dosages reported in Table 1. Data adapted to calculate the costs of pharmacological treatment alone, including the costs related to needles for insulin therapy, are shown in Table 1. Needle use cost has been derived based on the frequency of administration according to the summary of product characteristics and needle unit cost. The cost of a needle differs in our country from region to region. We considered needle unit price adopted in Liguria Region, 40 chosen as a benchmark. To calculate the total number of needles per day, we assumed it equals the number of daily administrations.
Pharmacological treatment costs: drug cost.

Abbreviations: API, active pharmaceutical ingredient; IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination; tab, tablet; UI, units of insulin.
Glycemic self-monitoring: frequency and unit costs
We assumed that cost per blood glucose test includes strip unit cost and lancet unit cost. To evaluate the costs of glycemic self-monitoring, we considered the number of glycemic control per week. We have assumed that one sample per week should be usually available for all patients with low hypoglycemic risk so that no additional strip and lancet were considered with the addition of saxagliptin/dapagliflozin to metformin. For the same reason, one strip and one lancet per week were also discounted from costs of blood sampling for gliclazide and insulin as well. Table 2 shows then the additional measurements to the standard weekly hypothesized and unit cost of strip and lancet. For the recommended frequency of checks concerning therapy, we referred to national scientific societies (AMD-SID) guidelines, 41 reporting a mean value extrapolated from these indications. In Italy, cost of stripes differs from region to region, with an average price per unit of about €0.55. In our model, we adopted the last price suggested by CONSIP (Italian public procurement office), which amounts to €0.35. In our model, we also considered the cost of blood sampling, amounting to €0.0145 per lancet in accordance with acquisition cost in Liguria Region, chosen as a benchmark. 40 We must also consider that, even if prices resulting in the latest public tenders are getting lower and lower, distribution costs remain unchanged so determining incompressibility of real costs, 42 not considering that new technologies in glycemic monitoring (ie, continuous monitoring portable devices) are spreading and this will probably bring up average costs again, at least for insulin-treated patients.
Glycemic self-monitoring: frequency and unit costs.
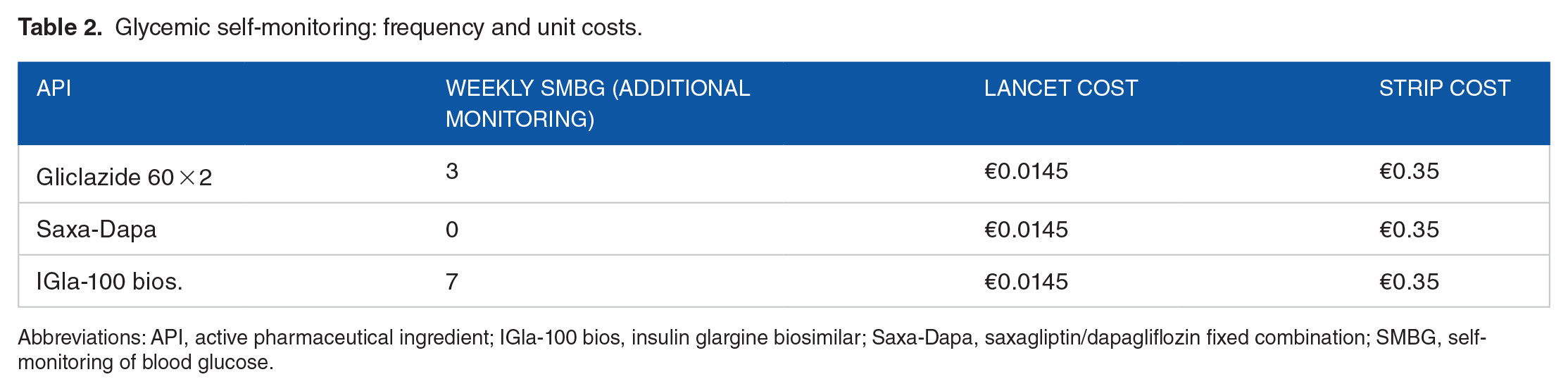
Abbreviations: API, active pharmaceutical ingredient; IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination; SMBG, self-monitoring of blood glucose.
Hypoglycemic events: rates and costs
A severe hypoglycemic event is defined as an episode with symptoms of low blood glucose levels during which the patient requires assistance from another person, mainly through hospitalization; when the patient can solve the problem by himself or herself, the event is defined as moderate. 43 To estimate the costs of hypoglycemia, we referred to the incidence of hypoglycemic events reported in international literature for patients with type 2 diabetes.43,44 We considered only severe and moderate hypoglycemia, not including mild ones, because of their negligible economic impact. We inputted direct mean costs of severe hypoglycemic events, valued at €1911, referring to an Italian study, 45 whereas for moderate ones we adopted a large Swedish study which reported data about it, already cited above. 43 For each treatment, we considered direct costs per patient/year combining the mean cost per event with the incidence of events related to each drug (Table 3). According to available literature, dapagliflozin severe hypoglycemia incidence is close to zero, whereas the highest values are reported for insulin treatment (0.1180) and gliclazide (0.0116). Data on rates and costs of hypoglycemic events are reported in Table 3.
Hypoglycemic events: rates and costs.

Abbreviations: API, active pharmaceutical ingredient; IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination.
MACE (nonfatal MI and stroke): event rates and costs
A major incidence of cardiovascular events (unstable angina, MI, or stroke) has been detected in patients treated with sulfonylureas versus DPP-4i (HR: 1.23; P = .01), after propensity-matching by age, sex, fragility, prior CVD, use of statins, low-dose aspirin, and antihypertensives. 30 In addition to this evidence, the above-described CVD-REAL 2 study reported a significant reduction of MI (HR: 0.81; P < .001) as well as of stroke (HR: 0.68; P < .001), in patients treated with SGLT2i. 33 We have therefore included in our economic model the direct costs of MI and stroke described in an Italian study derived from Osservatorio ARNO population. 46 We started from MI and stroke incidence among patients with diabetes and we applied the 8.4% incremental correction coefficient defined for patients with diabetes versus general population in the Italian study. 46
HHF: event rates and costs
Heart failure is highly prevalent in patients with diabetes, occurring in more than 20% of over 65-year patients so that HHF amounts to about 0.51/100 person-years.32,47 As shown above, SGLT2i reduce HHF rate (HR: 0.64, 95% CI = 0.50-0.82; P = .001), 33 and hence a reduction in health spending related to HHF, that in our country amounts to €11 000 per person/year considering only direct costs. 48
Table 4 shows the risk of stroke, acute nonfatal MI, and hospitalization for heart failure occurrence for gliclazide, saxagliptin/dapagliflozin combination, and insulin glargine, respectively. Specifically, the hazard ratio is reported for each drug, highlighting the different impacts of treatments on events over a year, compared to the frequencies of occurrence in the reference population (0.59% for stroke, 0.97% for acute myocardial infarction [AMI], and 0.51% for HHF). Moreover, direct costs per event are reported in Table 4.
Cardiovascular diabetes complications: event rates and costs.

Abbreviations: AMI, acute myocardial infarction; API, active pharmaceutical ingredient; HHF, heart failure hospitalizations; HR, hazard ratio; HR, P value: HR = 1.23, P = .010; HR = 0.68 (0.55-0.84), P = .001; HR = 0.81 (0.74-0.88), P < .001; HR = 0.64, P < .001; References: 30, 33; IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination.
Consumption of other drugs: hypertension/urogenital infections incidence and cost of treatment
Dapagliflozin, like the other SGLT2i, reduces also systolic blood pressure in patients with type 2 diabetes, including those receiving concomitant antihypertensive medication. This reduction amounts to an average of −3.1 mm Hg and statistically significant results (P = .001). 49 To economically quantify this benefit, we applied the mean cost of a generic antihypertensive medication (ie, doxazosin/amlodipine), which amounts to about €0.228 per day, to the hypertension prevalence in Italian diabetic population (58.6%), as reported in our AMD (National Diabetologist Association) annals. 39 The use of saxagliptin/dapagliflozin, therefore, allows saving €48.8 per patient on annual antihypertensive therapy cost. On the contrary, we included the treatment cost of urogenital infections, an adverse event also reported for another SGLT2i, empagliflozin (incidence of 3.2%), 31 and extendable to dapagliflozin, though this turned out to be irrelevant (considering clotrimazole use, we have calculated €0.23 per patient/year).
Simulation scenario: analysis on durability and switch to insulin rates
Several observational studies showed different maintenance rates between DPP-4i and sulfonylureas as second-line treatment in add-on to metformin, so that dual therapy with metformin and DPP-4i can be maintained for longer than metformin and sulfonylurea.30,50 Conversely, a proportion of patients needed a treatment intensification mainly represented by starting an insulin-based regimen (coefficient of failure vs sulfonylureas varying from IR: 0.24 vs 0.38 at 12 months to 0.44 vs 0.59 at 36 months). 50 Dapagliflozin also showed greater durability than sulfonylureas in a 4-year efficacy study (coefficient of failure vs glipizide at week 208: 0.19 vs 0.61; P = .0001), 51 and saxagliptin/dapagliflozin confirms this trend. Then, we developed a simulation scenario in which we assumed that all patients, who no longer maintain metabolic control with previous treatment with metformin plus a maximum dose of gliclazide or plus saxagliptin/dapagliflozin, switched to an insulin-based regimen (the switch to GLP1 receptor agonist resulting equal in costs, if not more expensive). To provide a comprehensive overview of costs related to switch to insulin based on different durability of drugs, after switching we applied the cost estimated in our model for basal insulin therapy (Glargine 100 biosimilar) instead of the cost of previous treatments. In our simulation, based on literature data, 51 we have considered a coefficient of failure at 208 weeks of 0.19 for saxagliptin/dapagliflozin and of 0.61 for gliclazide. Finally, based on the difference in rates of failure between sulfonylureas and saxagliptin/sapagliflozin, 51 we calculated the final cost related to the switch, respectively, starting from gliclazide and saxagliptin/dapagliflozin. Simulation scenario results have been calculated considering a 4-year period, obtaining both results for each year and cumulative for 4 years.
Utilities
Above we have reported data need to develop a cost analysis regarding different antidiabetic therapies; however, our study aims to extend the view also including the evaluation of the new therapies’ benefits on the patients’ quality of life. In particular, we considered the effects of body weight changes. It is known that some classes of antidiabetic drugs involve an increase in the patient’s weight. Sulphonylureas and basal insulin are certainly among them while, on the other hand, treatment with dapagliflozin has been associated with a significant reduction in weight.17,52 Moreover, the relevant impact of body weight on patients’ perceptions of quality of life is now recognized. Based on these assumptions, we carried out a literature analysis aimed at identifying the weight variations associated with gliclazide, basal insulin glargine, and saxagliptin/dapagliflozin, considering a 1-year time period. This research showed an average weight increase of 1.5 kg for the treatment with both gliclazide and insulin glargine53,54 compared to a weight reduction of 2.1 kg with the fixed combination saxagliptin/dapagliflozin treatment. 25 So, we applied these differences in weight to utility measures calculated in a Swedish study, 37 which shows for loss and gain of 2 kg weight utility values of 0.92 and 0.88, respectively. By combining weight variations (delta of 4 kg reported in Ridderstråle’s study) 37 and utility values, we calculated the utility value related to 1 kg variation, such as to be easily associated with the specific weight changes highlighted in the literature for a year of treatment with drugs in our analysis, obtaining denominators for the cost-utility analysis.
Sensitivity analysis
To assess the robustness of our analysis, a 1-way sensitivity analysis has been carried out varying by ±20% of the main input parameters in the model base case, namely, cost data and efficacy data (complications and side effects rates and utility values). Regarding drug purchase costs, furthermore, as reported above, we have tested the effects of increasing discount rates applied to ex-factory price (40%, 45%, 50% discount) for non-generic drugs, to reproduce, as close as possible, the direct cost paid by hospitals.
Results
This economic evaluation has allowed obtaining the total annual direct cost of the treatments in the analysis. Total annual direct costs and individual cost items making up the total cost for each therapy are shown in Table 5.
Total annual cost of treatments.

Abbreviations: AMI, acute myocardial infarction; API, active pharmaceutical ingredient; HHF, heart failure hospitalizations; IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination; SMBG, self-monitoring blood glucose.
The total direct cost of saxagliptin/dapagliflozin fixed-dose combination was €414.62 higher than gliclazide (€1.067.72 vs €653.10), and greater than basal insulin, with a difference of €166.99 (€1067.72 vs €900.72). However, breaking down final cost in the individual items, we note that the high total cost of fixed combination is mainly determined by purchase cost, which is more than 6 times higher than that of gliclazide, long-time drug in use, now available in generic form, and more than 4 times higher than insulin glargine biosimilar. Against the item related to drug acquisition cost, all others have shown a positive effect on costs, in contrast to gliclazide and basal insulin. Indeed, saxagliptin/dapagliflozin has involved lower self-monitoring blood glucose costs, lower costs related to hypoglycemia (gain of €72.37 and € 230.85 when compared with gliclazide and insulin glargine, respectively), a significant reduction in costs related to cardiovascular complications (gain of €118.39 and €68.92 when compared with gliclazide and insulin glargine, respectively), as well as saving in other drugs costs (€48.57) (Table 5). Simulation scenario, assessing the effect on the direct costs of switching to basal insulin from gliclazide or saxagliptin/dapagliflozin, highlighted a reduction of the total cost gap by about €231.84 in the fourth year, based on better durability profile of the fixed combination therapy (switching to basal insulin 19% vs 61% at 4 years). 51 The direct annual costs obtained for treatment have been used in the cost-utility analysis. Based on utility values for 2 kg weight gain or 2 kg weight loss, 37 the utility for 1 kg variation was calculated to equal 0.010. Multiplying this value by the weight variation associated with 1 year of treatment with gliclazide, insulin glargine, or saxagliptin/dapagliflozin, and the utilities resulted in 0.021 for the fixed combination and −0.015 for gliclazide and insulin glargine.
The difference between total costs of saxagliptin/dapagliflozin and gliclazide and insulin glargine, respectively, has been divided by the difference between the utilities, obtaining positive ICER both in the base-case scenario and in the simulation scenario in both drug comparisons. In the base-case scenario, the additional cost per QALY gained, compared with gliclazide, has been €11 517, and €4639 when compared with insulin glargine (Table 6). In the simulation scenario, the results have been even more positive, due to the better durability profile of saxagliptin/dapagliflozin compared with gliclazide, reporting an ICER at 4 years of €6440 and €3757 when compared with gliclazide and insulin glargine, respectively.
Cost-utility analysis results: base case scenario.

Abbreviations: API, active pharmaceutical ingredient; ICER, incremental cost-effectiveness ratio; IGla-100 bios, insulin glargine biosimilar; QALYs, quality-adjusted life years; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination.
These results do not consider extra-discount on drug prices, usually negotiated with local health care units.
The ICERs obtained resulted in fully compliant with the threshold adopted for Italy. Then, saxagliptin/dapagliflozin can be considered a cost-effective OHA. The positive effect of this drug on the quality of life, induced by the bodyweight loss, has allowed this outcome, despite the higher annual cost per patient, mainly determined by the drug purchase cost.
Sensitivity analysis
The sensitivity analysis has shown the robustness of the results. Indeed, the variation of cost and effectiveness data (±20%) have not resulted in significant deviations from the results, always keeping ICERs well within the acceptable threshold, never exceeding €25 000 (Figure 1). Furthermore, we have evaluated the effect of major durability of saxagliptin/dapagliflozin compared with gliclazide over 4 years, resulting in a lower rate of switching to basal insulin, avoiding related cost implications. Moreover, we carried out a sensitivity analysis that assumed feasible scenarios with 3 increasing discounts (40%, 45%, and 50%) applied to ex-factory price for non-generic drugs, to assess the cost-utility of saxagliptin/dapagliflozin adopting a discounted price closer to the real one. Sensitivity analysis findings are shown in Table 7 and Figure 1.

Findings of sensitivity analysis: cost per QALY gained. QALY indicates quality-adjusted life year.
Summary of cost-utility analysis results and sensitivity analysis.
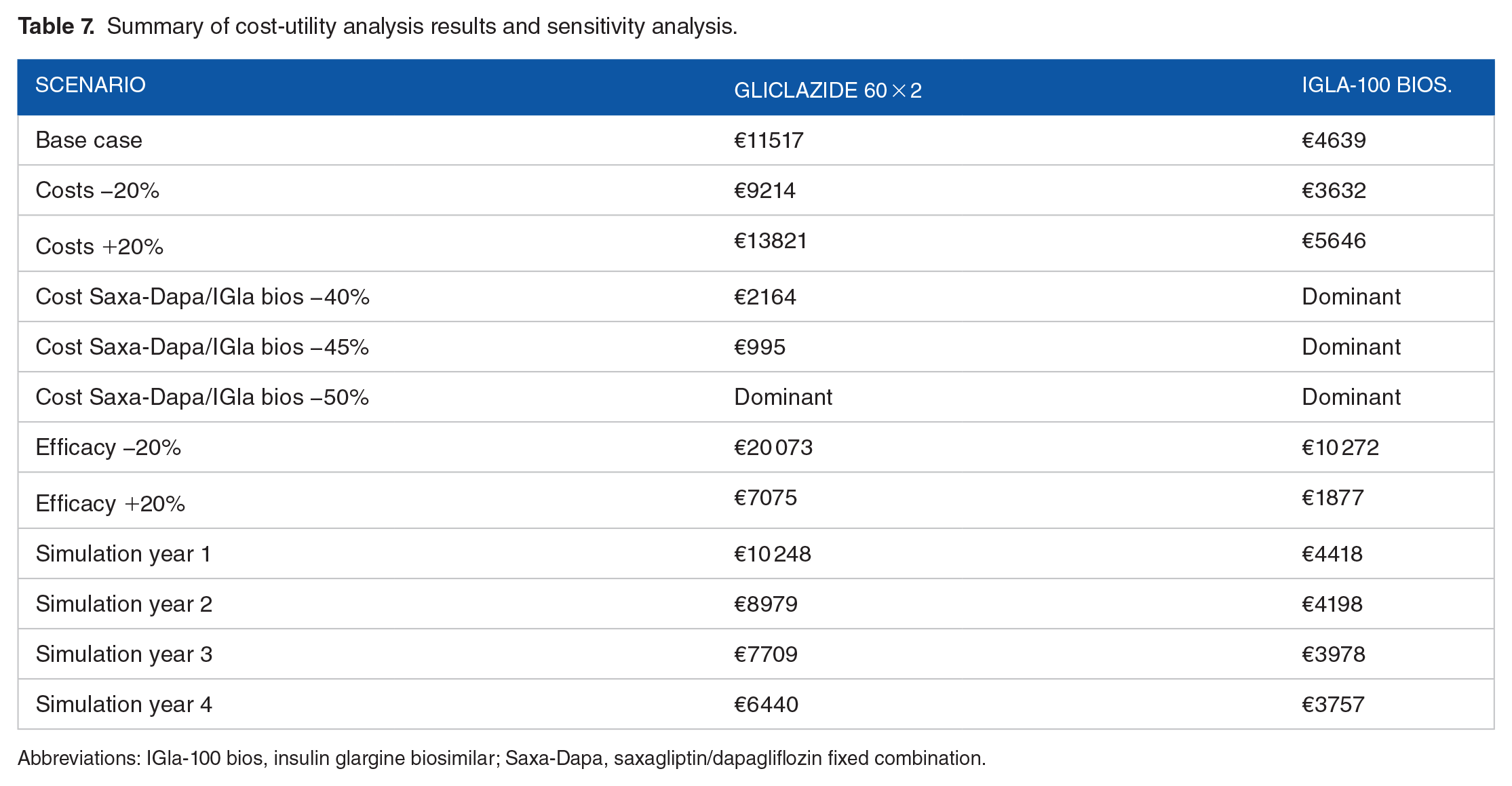
Abbreviations: IGla-100 bios, insulin glargine biosimilar; Saxa-Dapa, saxagliptin/dapagliflozin fixed combination.
In all the scenarios, the cost-utility of saxagliptin-dapagliflozin combination has been demonstrated. Particularly, in comparison with gliclazide, ICER has reported positive results in the simulation scenario over 4 years due to the better durability of saxagliptin/dapagliflozin combination. Focusing on the scenarios with discounts applied to the ex-factory price of saxagliptin/dapagliflozin and insulin glargine, ICERs have shown the combination can be considered a dominant option compared with insulin glargine and characterized by an excellent cost-utility profile when compared with gliclazide.
Discussion and Conclusions
Our study aimed to evaluate the economic implications of positive effects on cardiovascular outcomes and weight loss of the fixed-dose combination saxagliptin 5 mg/dapagliflozin 10 mg versus gliclazide and basalization with insulin glargine on the basis of clinical evidence, such as CVD-Real I and II studies. Today, there is evidence regarding the cardiovascular effects and impact on the bodyweight of newer glucose-lowering agents and the importance of them for the management of metabolic control and cardiovascular risk in patients with T2DM and, on the other hand, complication related to the sulfonylureas class. 55 We developed a cost-utility analysis to assess the value of the newer fixed combination therapeutic option, providing, through ICER, information on the additional resources that have to be used to achieve the additional benefit. In our analysis, saxagliptin/dapagliflozin fixed combination was found to be cost-effective when compared with gliclazide and insulin glargine biosimilar. Indeed, although the difference between total direct costs of the compared treatments is disadvantageous for the fixed-dose combination, lower costs associated with complications and the favorable difference in terms of utility have allowed obtaining a positive ICER value, well below the accepted willingness to pay threshold, set in Italy at €40 000. 38 This economic evaluation has been focused on direct costs, adopting the perspective of the Italian NHS. The utility has been evaluated on the basis of the effects of the compared treatments on the bodyweight variations and their consequences on patients’ quality of life. Despite all cost items, except for the drug purchase, are in favor of the combination, mainly due to the significant benefits on the cardiovascular risk profile and to the lower incidence of hypoglycemic events, the total direct cost is negatively influenced by the cost of the drug. However, the real value of the combination emerges by extending the perspective and incorporating into the cost analysis the benefits of the treatment on the patient’s quality of life, allowing to define this treatment cost-effective. Indeed, the base-case scenario has reported for the combination an ICER of €11 517 and €4639 when compared with gliclazide and insulin glargine, respectively. The cost-effectiveness of saxagliptin/dapagliflozin has also been highlighted in the simulation analysis that has offered interesting insights, considering the possibility to reduce the switching to insulin over 4 years based on better durability showed in literature. 51 Adoption of saxagliptin/dapagliflozin instead of gliclazide allowed to generate cost reduction that, at 4 years, thins out the gap. It is important to note that we have calculated drug costs based on ex-factory prices for non-generic drugs, although it is not the real drug cost paid by health facilities in Italy because a confidential discounted price is usually negotiated between manufacturers and Italian NHS. Thus, since at the basis of the gap between total direct costs, there is precisely the high purchase cost of the combination, to evaluate the uncertainty around the real direct cost paid by hospitals, we tested the effects of increasing discount rates applied to ex-factory price (40%, 45%, and 50%). The application of these discounts to saxagliptin/dapagliflozin and insulin glargine biosimilar ex-factory costs has resulted in an extremely positive ICER compared with gliclazide, while it has made the combination dominant in comparison with insulin glargine.
Moreover, the findings of our cost-utility analysis were robust when tested in sensitivity analyses.
A further interesting aspect is the intrinsic benefits associated with the use of fixed drug combinations, especially in a chronic disease such as diabetes. Polypharmacy is a common problem among patients with diabetes and the use of fixed-dose combinations is a rational approach to achieve and maintain glycemic control. Fixed-dose combinations are also useful to improve the adherence and compliance compared with multiple administrations. 56 There are now several antidiabetic fixed combination therapies, and others are in development or study, designed with the aim of improving the control of disease by providing benefits of more active ingredients in a single administration. There are many combinations of metformin with other oral glucose-lowering drugs (eg, empagliflozin, dapagliflozin, saxagliptin, sitagliptin, vildagliptin, rosiglitazone), and recently, fixed combinations with basal insulin have been made available, such as iglargine/lixisenatide, idegludec/liraglutide, as well as drug combinations of active ingredients belonging to the categories GLP-1 receptor agonists, SGLT2i, or DPP-4i. In a context of limited economic resources for NHS, the higher acquisition cost of newer therapies has made health technology assessment (HTA) necessary to confirm the additional value of these therapies. To our knowledge, this is the first cost-utility analysis of saxagliptin/dapagliflozin fixed-dose combination versus gliclazide and insulin glargine in inadequately controlled on metformin monotherapy in patients with T2DM, aimed at defining the economic implications of this combination positive effects on cardiovascular risk and body weight, developed from the perspective of the Italian NHS. Although no other economic analyses have been found comparing these therapeutic options, results shown in our study are comparable with those of other economic evaluations conducted on different antidiabetic drugs fixed combinations.57-62 In various studies in the literature, it is shown that the high cost of the newer drugs is offset by the benefits obtainable on the reduction of complications, especially cardiovascular events and hypoglycemia. Our cost-utility allows us to go beyond the pure analysis of costs and provides a global assessment of the therapy’s value, highlighting the potential economic benefits for the NHS, due to the enhancement of multiple clinical outcomes in patients with diabetes and improvement of the quality of life. In particular, we have chosen to consider the impact of therapies on cardiovascular risk and weight changes based on the most recent literature.
Regardless of the limitations of our analysis, it is correct to specify that data input relating to Italy were not available, and reliable international sources have been considered. So, because of the lack of suitable Italian data on the effect of changes in body weight on HRQoL of patients with T2DM, the utilities for the health states “2 kg gain” and “2 kg loss” adopted in the model were derived from Riddestrale’s Swedish study. 37 The analysis essentially has considered the effects of hypoglycemic and cardiovascular complications, while it has not included the other types of comorbidities typically associated with diabetes and potential adherence benefits related to single-pill combination use has not been considered.
In an economic evaluation, it is difficult to accurately measure the study variables, and each medication therapy may bring different treatment costs when applied among different populations or medical institutions; nevertheless, the robustness of our analysis suggests the generalizability of the results.
Further investigation for Italy is useful to have a better understanding of the long-term effects of the combination treatment and its impact on patient’s quality of life.
Our analysis has been carried out including only direct cost, to reflect the perspective of the Italian NHS; however, in economic evaluations, it is important to consider also indirect costs that are included when the social perspective is adopted. Indirect costs are instead related to work-related absenteeism, reduced productivity both at work and home, reduced labor force participation from chronic disability, and relevant aspects for chronic diseases such as diabetes. The addition of indirect costs to our analysis would make the benefit of saxagliptin/dapagliflozin combination even more evident. Indeed, this has shown clear positive outcomes on the reduction of hypoglycemic events and cardiovascular complications, which are characterized by a relevant impact on indirect costs. Based on these considerations, we have developed an approximate calculation of the indirect costs associated with hypoglycemic events (moderate and severe) and cardiovascular adverse events (stroke, IMA, HHF). Indirect costs related to hypoglycemic events have been provided from a Swedish study mentioned earlier, 43 while cardiovascular adverse events’ indirect costs have been evaluated calculating a 62/38 ratio between direct and indirect costs, the latter expressed as both loss of productivity and informal care, as reported by an analysis of costs of cardiovascular diseases in Europe. 63 Adding the direct costs reported above to the indirect ones, we have obtained total costs, useful to express the social perspective, and we, therefore, have applied these total costs in the cost-utility analysis. The results of this additional analysis have shown ICER extremely positive for saxagliptin-dapagliflozin combination. Specifically, ICER has been €8955 when compared with gliclazide, while the combination has resulted dominant when compared with insulin glargine. In the face of continuously increasing health care costs, it is very crucial to determine which strategy provides better value and it is necessary for further research focusing on the long-term impact of fixed-dose combinations as well as the economic outcomes.
Although drug costs are increasing, due to the progressive adoption of newer therapies, the greatest component of the economic burden of T2DM remains the treatment of diabetic complications, which can be reduced with effective management of the disease. In this perspective, the adoption of saxagliptin/dapagliflozin fixed combination, taking advantage of complementary mechanisms of action, providing better control of the therapy, a cardioprotective effect, and a positive impact on weight loss, is an important therapeutic option, also in light of the demonstrated cost-effectiveness when compared with the other treatments.
The fixed combination saxagliptin/dapagliflozin was shown to be a cost-effective treatment option from the Italian health care system perspective as add-on therapy to metformin in patients with inadequately controlled T2DM. Study findings have the potential to provide stakeholders valuable evidence to support the adoption of this cost-effective third-line therapy compared with gliclazide or basal insulin after the addition of DPP-4i or SGLT2i due to metformin monotherapy failure.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: his analysis was funded by AstraZeneca, Italy.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.T. has received consultancy and/or speaking fees and research grants from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Johnson & Johnson, MSD Italy, Novo Nordisk, Sanofi, and Takeda, over the last 3 years. G.L.C. received research and educational grants from Abbott, Amgen, DOC Generici, Eisai, LeoPharma, Menarini, Merck Sharp and Dohme, Novo Nordisk, Sanofi, and Takeda. The other authors report no conflicts of interest.
Author Contributions
ET and LCB made substantial contributions to the clinical data analysis and contributed to the definition of the model framework and its revision. GMB supervised the project and helped in writing the manuscript. SDM developed the economic model. CM supported the model development and wrote the manuscript with input from all authors. MCV supported the writing and the editorial process. GLC supervised, coordinated and validated the work.