
Abstract
Considerable research has focused on hospitalizations for ambulatory care–sensitive conditions (ACSHs), but little of that research has focused on the role played by chronic disease in ACSHs involving children or youth (C/Y). This research investigates, for C/Y, the effects of chronic disease on the likelihood of an ACSH. The database included 699 473 hospital discharges for individuals under 18 in Texas between 2011 and 2015. Effects of chronic disease, individual, and contextual factors on the likelihood of a discharge involving an ACSH were estimated using logistic regression. Contrary to the results for adults, the presence of chronic diseases or a complex chronic disease among children or youth was protective, reducing the likelihood of an ACSH for a nonchronic condition. Results indicate that heightened ambulatory care received by C/Y with chronic diseases is largely protective. Two of more chronic conditions or at least one complex chronic condition significantly reduced the likelihood of an ACSH.
Introduction
Hospitalization remains one of the costliest items in the United States’ health care shopping basket. In 2015, inpatient services accounted for 38% (US$1 trillion) of total personal health care expenses in the United States. 1 That same year, the estimated average costs per inpatient stay in hospital for those under 18 years of age was US$21 272. 2 Unlike expenses for ambulatory care, which are incurred by roughly three-quarters of the population, inpatients expenses are incurred by a much smaller proportion of the population (eg, 6.6% in 2014). 3
Hospitalizations for certain cases of trauma and a wide range of other conditions are clearly recognized as unavoidable hospital admissions. However, another class of hospitalizations, hospitalizations for ambulatory care–sensitive conditions (ACSHs), has become the object of increasing scrutiny by both health care providers and those paying for health services. Hospitalizations for ambulatory care–sensitive conditions (ACSHs) are commonly considered hospitalizations that appropriate ambulatory care might have prevented.4,5
Considerable research on ACSHs has focused on adults or older persons. Estimates for the period from 2003 to 2007, based on national hospital discharge data for those 18 to 64 years of age, indicate that 12.7% of all hospital discharges for this group involved ambulatory care—sensitive conditions. 6 For Medicare recipients, estimates for 2013 indicate that county rates of ACSHs per 1000 beneficiaries ranged from 21.9 to 280.9, with the mean county rate being 71.6 ACSHs per 1000 benificiaries. 7
This previous research on adults has demonstrated that the likelihood of ACSHs is related to access to services,7,8 rurality,7,9 and sociodemographic characteristic such as age, race, ethnicity, and economic status.9,10 Gao et al 11 confirmed the significant effects of most of the factors mentioned above in this special population, as well as the impact of prior health care utilization and previous care costs. Saver et al 12 concluded from their analyses that comorbidities, the bulk of which were chronic conditions, were the most important factor increasing the likelihood of an ACSH among older adults.
Those researchers investigating pediatric-specific ACSHs have often produced results similar to those found in investigations focusing on adults and older persons. Access to health insurance affects the rate of ACSHs for children and youth. Continuity of care or well-child care visits seem to reduce the likelihood of ACSHs.13-15 Children or youth in lower income groups, children of color, younger children, income inequality, and children and youth in more rural areas have been found to be at higher risk of an ACSH.16-20
As indicated above, researchers investigating the role of chronic conditions in ACSHs for older persons have found that chronic conditions play an important role in increasing the likelihood of an ACSH among members of that population. 12 Some ACSHs among children and youth involve chronic conditions, such as diabetes or asthma, 13 but the effect of other chronic conditions on hospitalizations for nonchronic conditions, such as bacterial pneumonia, has received relatively little attention in the investigation of ACSHs for children and youth.
This research supplements the current research on ACSHs involving C/Y with its focus on clarifying the impact of chronic conditions and complex chronic conditions on the likelihood of an ACSH for nonchronic diseases.
Methods
Data
The Texas Department of State Health Services maintains the Texas Inpatient Public Use Data File, which contains public use data files on hospital discharges. From those data, pooled cross-sectional data on hospital discharges from October 2011 to September 2015 involving patients under the age of 18 years were extracted. 21 During this time, hospitals in Texas reported 2 223 066 discharges from 576 hospitals. Like early research on this issue, discharges that had a primary diagnosis of a mental health issue were excluded. Discharges were also excluded if they involved normal births—newborn admissions or those births with both a length of stay of less than 5 days and a discharge home with no services. 22
Asthma and diabetes are chronic conditions found among the list of ambulatory care sensitive conditions for C/Y. A discharge for one of these conditions would automatically have a likelihood of being considered an ACSH equal to 100%. This reality would unduly inflate the effect of chronic conditions on ACSHs. To avoid this problem, we deleted all discharges for children or youth involving asthma or diabetes. The resulting database included a total of 699 473 discharges of children or youth under the age of 18 years. Seventeen percent (118 805) of these discharges had a nonchronic ambulatory care–sensitive conditions (ACSC) as a primary diagnosis.
The Area Health Resource Files (AHRF) dataset provides information regarding health care professions, health facilities, population characteristics, economic activity, health professions training, hospital utilization, hospital expenditures, and socioeconomic and environmental characteristics at the county, state, and national level from various sources. 23 In this research, AHRF county–level data were used to obtain information regarding average median income and the average number of pediatricians per 1000 children and youth for each Texas county included in the analysis.
All data used in this research are available in widely distributed public use databases. All aspects of this project were approved by the Institutional Review Board at Texas A&M University.
Measurement
Dependent variables
The dependent variable in the logistic regression model was a binary indicator indicating the presence or absence of any nonchronic ACSH in our database of almost 700 000 discharges for C/Y.
This dependent variable reflected the presence of any of 16 previously validated ACSHs for C/Y. 24 These included bacterial pneumonia, cellulitis, dental problems, ear/nose/or throat problems, failure to thrive, gastrointestinal issues or dehydration, iron deficiency, kidney infection or urinary tract infection (UTI), nutritional issues other than malnutrition, pelvic inflammation, skin problems, tuberculosis, and conditions for which vaccines were available but not used. A diagnosis of malnutrition is considered an ACSH, but no discharges involving malnutrition appeared in the database. Hospitalizations for diabetes or asthma were not included in the dependent variable.
Major independent variables
The presence of a chronic condition was indicated if any of the diagnoses listed in the discharge record indicated the presence of a chronic condition. Chronic conditions were identified using the Chronic Condition Indicator database developed from the Healthcare Cost and Utilization Project (HCUP). The database indicates whether a chronic condition exists in any of the 18 categories related to major body systems (eg, respiratory, circulatory or genitourinary, etc) or related to specific conditions (eg, infections or parasitic diseases). 24 As noted above, discharges involving 2 chronic conditions, asthma or diabetes, were excluded from the data and the analysis because they also represented discharges for an ambulatory care–sensitive condition.
Complex chronic conditions were identified using Feudtner and his colleagues’ list identifying pediatric complex chronic conditions. This complex chronic condition list is more specific than the Healthcare Cost and Utilization Project (HCUP) chronic condition list. For example, the HCUP list might indicate a chronic respiratory problem. The list of complex chronic respiratory problems includes diagnoses such cystic fibrosis, a malformation in the respiratory system, the presence of a transplant, or other more challenging respiratory conditions. 25
Covariates
Information included in the hospital discharge record used directly as covariates included patient sex, race/ethnicity, age, year of discharge, type of hospital (public, private, government), and source of payment.
The Rural Urban Classification Codes, version 2103, were used to construct binary variables indicating that the hospital operated in a large metropolitan area (1 000 000 or greater, a metropolitan area of moderate size (250 000-999 999) or some more rural setting (less than 250 000). 26 Two county-level variables that may also have affected access to ambulatory care were used in this effort; these were the median income in the county and the number of pediatricians per 1000 children in the county receiving Medicaid services. Binary variables representing the 11 Texas Public Health Regions were also included as covariates to adjust for any regional differences in health service resources. A variable indicating the calendar quarter (1-16) was also included in the model to ascertain if any changes in the likelihood of an ACSH occurred over time.
Analysis strategy
All analyses were performed using STATA, Version 14. 27 Descriptive data for all variables were analyzed. The variables include in these analyses had differing numbers of missing cases, but none had missing data that exceeded 5%.
The multivariate models involved logistic regression for estimating the likelihood of discharge for a nonchronic ACSH among all appropriate hospital discharges for C/Y. The measures of goodness of fit for the logistic model were the pseudo-R2 and the area under the receiver operating curve (ROC).
For the model, clustered robust standard errors were calculated. This approach protects against any bias in the standard errors created by the clustering of discharges in hospitals. The approach also considers that multiple discharges may be associated with only one child or youth. Multiple discharges for a single person are likely to be from the same hospital, contributing to the intracluster correlation for which the clustered robust standard errors adjust. 28
Only parameters with an alpha of 0.01 or lower are considered statistically significant. This alpha level was chosen to adjust for the increased likelihood of Type II error that occurs when a model including a large number of parameters are estimated. The most traditional approach to the multiple-comparison issue is a Bonferroni adjustment, but the Bonferroni is an extraordinarily conservative approach to the problem. 29 Thus, this effort does not use the Bonferroni adjustment, but it does address the issue of multiple comparisons by using an alpha of 0.01 rather than 0.05.
Results
Table 1 provides descriptive statistics for hospital discharges involving children or youth that occurred over a 4-year period and conformed to the requirements noted earlier. The age group with the highest percent (24.3%) of discharges was newborns; the age group with the lowest percent of discharges was 10 to 14 years (12%). The discharges were almost evenly split among women and men.
Descriptive statistics for hospital discharges among C/Y in Texas, 2011-2015 (N = 699 473).

Discharges do not include discharges after normal births or discharges where a mental health problem was the principal diagnosis. Discharges involving diabetes or asthma are also not included in the table.
Abbreviations: ACSH, hospitalization for an ambulatory care–sensitive condition.
Hispanic children or youth constituted the largest percent of discharges (45.2%), with non-Hispanic Whites responsible for just over one-third of discharges. Blacks accounted for almost 11.8% of discharges. Over half of the discharges (54.3%) involved Medicaid recipients, occurred in large urban areas (55.2%), or involved not-for-profit hospitals (58.7%).
Roughly half of discharges involved C/Y with no chronic conditions; one-fifth had one chronic condition; the remainder had 2 or more, with just more than 11% presenting with 4 or more chronic conditions. Slightly less than one-fifth (18%) of discharges involved C/Y with at least one complex chronic condition. Just more than 9% (9.2%) had 2 or more complex chronic conditions. Almost 17% (16.9%) involved C/Y with a nonchronic ambulatory care–sensitive condition as a principal diagnosis.
The average median income in the counties included in this research (US$50 558) was roughly US$3000 higher than the average median county income in the United States. The counties average almost 2 pediatricians (1.97) for every 1000 C/Y receiving Medicaid services.
The results of the logistic regression provide estimates of the effect of each of the indicators in Table 2 on the likelihood of a nonchronic ACSH. Many of the parameter estimates in the model were not statistically significant (P > .01). These included payment source, time, and those county characteristics that might serve as impediments to access. These parameters are omitted from Table 2.
Logistic regression predicting ACSH discharge for a nonchronic condition among C/Y in Texas, 2011-2015 (N = 656 085).
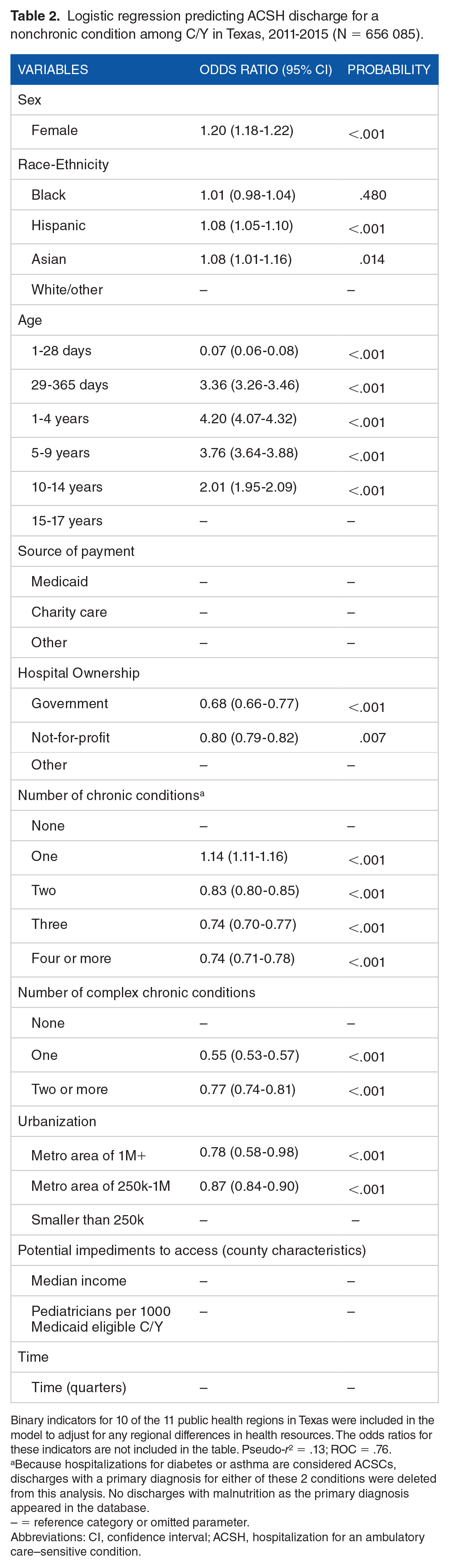
Binary indicators for 10 of the 11 public health regions in Texas were included in the model to adjust for any regional differences in health resources. The odds ratios for these indicators are not included in the table. Pseudo-r2 = .13; ROC = .76.
Because hospitalizations for diabetes or asthma are considered ACSCs, discharges with a primary diagnosis for either of these 2 conditions were deleted from this analysis. No discharges with malnutrition as the primary diagnosis appeared in the database.
– = reference category or omitted parameter.
Abbreviations: CI, confidence interval; ACSH, hospitalization for an ambulatory care–sensitive condition.
As those results indicate, women were 20% (1.20; 1.18-1.23) more likely than men to experience an ACSH. Differences among different races or ethnic groups were evident in the slightly elevated likelihood (1.07; 1.02-1.12) of ACSH involving Hispanics. The results for age were relatively complex. Compared to discharges involving C/Y 15 to 17 years of ages, all other age groups had significantly higher likelihoods of an ACSH.
The results presented in Table 2 indicate that multiple chronic conditions had a protective effect for C/Y. Although the discharge of a C/Y with one chronic condition increased the likelihood (1.13; 1.04-1.22) of an ACSH, the presence of more than one chronic condition reduced the likelihood of an ACSH for a non-chornic condition by between 20% and 30%. The presence of any complex chronic condition among C/Y was uniformly protective against an ACSH for a non-chronic condition.
Discussion
In older persons, the presence of chronic conditions or comorbidities clearly increases their likelihood of a hospitalization for an ambulatory care–sensitive condition.11,12 In contrast, the analyses presented here indicate that for children or youth hospitalized for an ambulatory care–sensitive condition, the presence of chronic conditions or complex chronic condition is largely protective against nonchronic ACSHs.
The obvious conclusion one reaches is that those C/Y with chronic conditions in these data receive more ambulatory care, which reduces their likelihood of an ACSH. Unfortunately, hospital discharge data contain no information on the nature of ambulatory care received by members of this population prior to their hospitalization. However, earlier research on C/Y in Texas with chronic illnesses who received services through Medicaid’s Early and Periodic Screening and Diagnosis (EPSDT) program support this conclusion. In 2009, those C/Y in the EPSDT program in Texas had roughly twice as many physician visits for evaluation and management as did C/Y who received services through Medicaid but had no chronic illness. 30
Those results are consistent with an explanation indicating that the increased ambulatory care provided to those with chronic illnesses helps them avoid unnecessary hospitalizations for other conditions. The results for the presence of one chronic condition seem to indicate, that in these data, the ambulatory care needed to reduce the likelihood of an ACSH may not occur until a child or youth suffers from more than one chronic condition or any complex chronic condition.
The limitations of this research are relatively clear. These data pertain only to the care provided in a single state, during a limited time period. Also, hospital discharge data do not contain information about the health services a patient received prior to the hospitalization, provide a detailed record of the patient’s condition at admission, or the specific hospital services received during the hospitalization. In addition, discharges involving asthma or diabetes were excluded from our analyses because such discharges are automatically considered hospitalizations for an ambulatory care sensitive condition, and the focus here was on ACSH for nonchronic conditions. Further analyses of this issue with alternative databases should better clarify the dynamics underling these results.
Conclusions
Despite its limitations, this research clearly implies that the role of chronic disease in children or youth, as it relates to ACSHs, differs dramatically from the role of chronic disease in adults and older persons. Multiple chronic illnesses for children or youth or the presence of a complex chronic condition seem to reduce the likelihood of an ACSH, most likely as a result of more intense primary care services for children or youth faced with multiple chronic diseases or any complex chronic condition . . . .
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CDP and RO provided original research question. HCK and CT were responsible for data development and analysis. ON and CDP wrote first draft. All authors reviewed and commented on each element of the paper as it was produced.