
Abstract
Pain management in the United States reflects attitudes to those in pain. Increased numbers of disabled veterans in the 1940s to 1960s led to an increased focus on pain and its treatment. The view of the person in pain has moved back and forth between a physiological construct to an individual with pain where perception may be related to social, emotional, and cultural factors. Conceptually, pain has both a medical basis and a political context, moving between, for example, objective evidence of disability due to pain and subjective concerns of malingering. In the 20th century, pain management became predominately pharmacologic. Perceptions of undertreatment led to increased use of opioids, at first for those with cancer-related pain and then later for noncancer pain without the multidimensional care that was intended. The increased use was related to exaggerated claims in the medical literature and by the pharmaceutical industry, of a lack of addiction in the setting of noncancer pain for these medications—a claim that was subsequently found to be false and deliberatively deceptive; an epidemic of opioid prescribing began in the 1990s. An alarming rise in deaths due to opioids has led to several efforts to decrease use, both in patients with noncancer conditions and in those with cancer and survivors of cancer.
Keywords
Between 1999 and 2016, more than 630 000 persons in the United States died from drug overdoses—most of these drug-related deaths were due to opioids prescribed for pain. 1 From 1999 to 2010, overdose deaths due to opioid pain relievers increased continuously, a time known as the first wave of the opioid epidemic. After this wave, the second and the third waves of opioid overdose deaths due to heroin and illicitly manufactured fentanyl (IMF), respectively, affected the United States significantly.1-6 There was an increase in deaths from 52 404 in 2015 to 72 000 deaths (provisional) by 2017.7-9 A recent suggested revision to the classification of prescription opioid-related deaths removes synthetic opioids (such as fentanyl) from this category to better characterize those deaths as, increasingly, from illicit opioids. This reclassification has important implications for strategies to address the problem as we discuss under possible solutions. 10 This article reviews the evolution of the understanding of pain and the impact of pain (initially with disability of WW II veterans as the proxy for the subjective symptom of pain) on the political, legal, and regulatory systems in the United States as a template for the increase in use of opioids in the past 2 decades. Finally, we discuss current solutions to the opioid epidemic—guidelines, policies, monitoring and other approaches. Space does not permit an expansion of the sociological background—the article by Dasgupta 5 explores these causes of the rise in abuse of both illicit and prescription opioids.
Modern theories of pain began with Descartes in the mid-1600s with his theory of pain specificity. A painful stimulus on the surface of the body was transmitted by a nerve through the spinal cord to a site in the brain where pain was perceived.11-15 This theory had several implications—pain was a physiologic concept that was seemingly straightforward, but left out were the emotional, cultural, or social modification of the message, and only one site in the brain processed pain input. Most importantly, the body and the mind were separate in this conceptualization. The understanding of pain evolved over the next 3 centuries—metaphysical explanations and the influence of the church waned; suffering and psychological components were further downplayed; however, by the 1900s, the notion of suffering and the psychological component again was acknowledged. Finally, the concept of modulation of the pain message assumed more importance with the 1968 publication of the Gate Control Theory of Pain. 13 The further evolution of this theory has helped reinsert components of suffering—psychological, spiritual, and cultural that were discounted over the past 4 centuries. This theory was advanced in part due to the political and cultural ethos that was extant and evolving pari passu with the understanding of the mechanism of pain from a simple transmission along a defined pathway to modulation of the message by areas of the brain that respond to related factors such as culturally learned stoicism. 15
The therapies for pain began to evolve in the United States in the middle of the 19th century with the development and use of morphine for injured Civil War soldiers. In the late 1800s and early 1900s, there was reticence on the part of some physicians and some patients to use anesthetics and analgesics and instead to rely on nonpharmacologic measures. By the middle of the 1900s (with the return of the injured World War II soldiers), therapy was predominately pharmacologic, in part related to the same political and cultural ethos. 16
Bourke 11 has chronicled stories of acute pain before the widespread use of anesthetic agents such as ether and chloroform, whose use began in the late 1840s, and later in injured soldiers and civilians in the Civil War era. A dilemma arose in former soldiers who continued to use morphine after the war. This usage for ongoing chronic pain lead to restrictions on morphine in the early part of the 1900s and heroin in the 1920s.14,16
Usage of veteran’s services was modest before World War II. Henry Beecher and John Bonica, both anesthesiologists after the war, chronicled that soldiers with severe and sometimes lethal wounds, denied pain, and focused on a return to their comrades on the battlefield. Others in obvious pain improved with the use of barbiturates to relieve anxiety. These observations led to a renewed acknowledgment of the role of psychological, cultural, and social (eg, bonding on the battlefield) factors.11,12,15
Continued pain after the war injury and after return to civilian life posed increasing challenges to US society, which were manifested in a dramatic rise in the number of disabled veterans and the need to provide services for them. Wailoo documents the role that politics, both governmental and medical, played in decisions in the late 1940s and 1950s in the management of chronic pain and disability as its proxy. When the disability was due to the subjective symptom of pain, those who argued to believe the individual such as Beecher and Bonica were confronted by those seeking to quantify the problem for either monetary compensation or deny the existence of the problem. The confluence of veterans from WW I, WW II, and the Korean War led to a rise in the number with disabilities from 0.5 million in 1940 to 3 million by 1960. Tables 1 to 4 summarize key points from Wailoo’s work from the period of 1945 until 1979, which are important in understanding the path to the current epidemic. 15
Pain, politics, and regulation in the United States—1940-1959.

Abbreviations: C, Congress; D, Democrat; J, Judiciary; R, Republican; S, State.
Pain, politics, and regulation: 1960’s.

Abbreviations: C, Congress; D, Democrat; J, Judiciary; R, Republican; S, State.
Pain, politics, and regulation: 1960-1970’s.
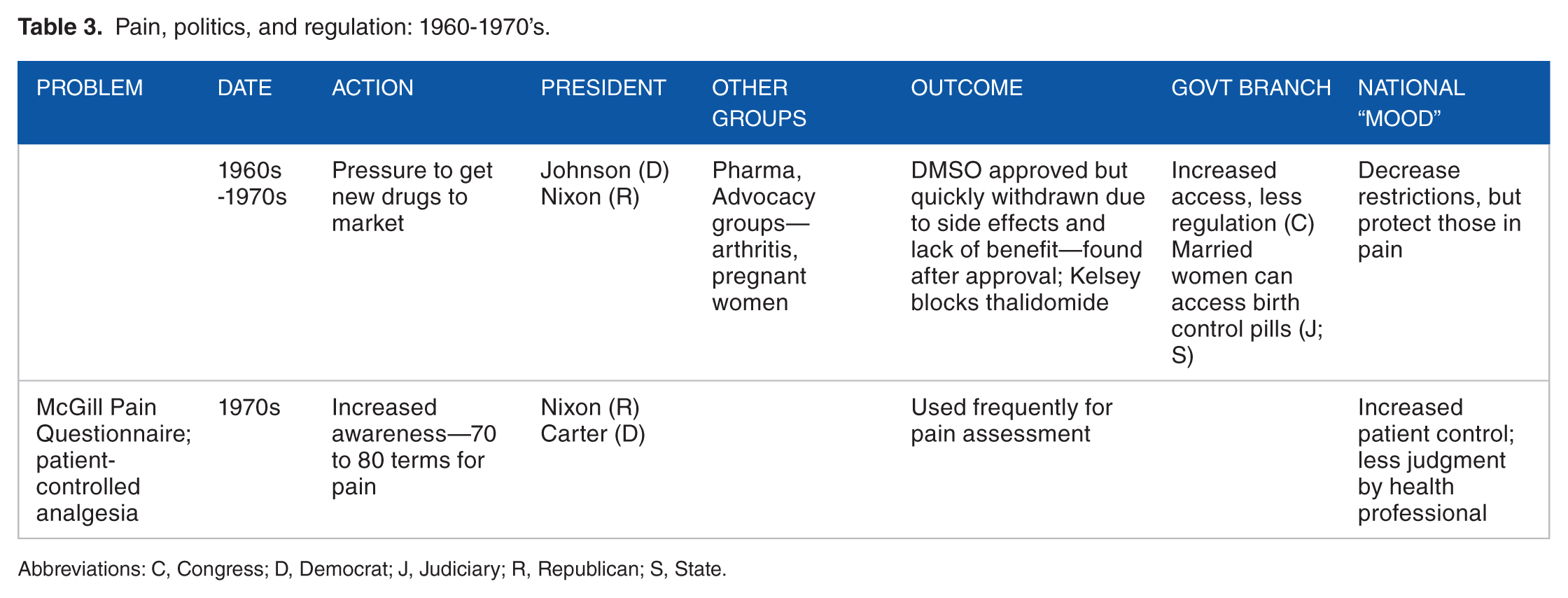
Abbreviations: C, Congress; D, Democrat; J, Judiciary; R, Republican; S, State.
Pain, politics, and regulation—1970s.

Abbreviations: C, Congress; D, Democrat; J, Judiciary; R, Republican; S, State.
In the 1970s, the pendulum began to reverse from compassion to quantification.5,15 Initially, disability awards rose from 350 000 to 600 000 claimants.
With the election of Reagan in the 1980s, the pendulum swung to the right. 15 The Secretary of HHS—Richard Schweiker—removed nearly half a million individuals from disability rolls. Republican replacement of the subjective evaluation of pain and disability with only objective measures of limitation was now the standard. Wailoo 15 notes that while the rise in disability awards was unsustainable, those in power blamed the disabled, and not the political system. The courts increasingly set the standard for suffering. Regulations and enforcement increased. 15
It is in this climate that the 1990s began with the election of a liberal Democratic president, Clinton. Universal health insurance was again discussed. The AIDS epidemic highlighted the differences between those who felt that the illness was punishment for behavior and those who developed an infrastructure to care for individuals with the condition. 15
Two recent reviews of medical events beginning in the 1990s chronicle how the use of prescription opioids grew until the crisis was recognized in latter part of the current decade and officially declared an epidemic.13,15-17 It is important to note that as opioid use was extended from cancer and acute pain to chronic noncancer pain in the 1990s; guidelines counseled caution in their use. They specifically advised that opioids be used discriminately and that their use should occur in a clinical environment that offered behavioral and psychological care given the substantial mental health burden in patients with chronic pain. What was intended to be multimodal care, however, became unidimensional care in most settings with reliance almost completely on pharmacologic solutions to pain. The societal consequences ensued.
In 1980, a Letter to the Editor from the Boston Drug in the New England Journal of Medicine Collaborative claimed that only 4 patients of 11 882 (0.03%) developed addiction while receiving opioids in the hospital. The data were not further presented. 17 Another well-known, flawed, but often cited retrospective review of only 38 individuals on pain medications for chronic, noncancer-related pain by Portnoy and Foley, 18 both oncologists, showed that only 2 had problems with management due to prior substance abuse. The use of opioids in chronic noncancer pain began to increase. By the 1990s, the American Pain Society and other groups began developing guidelines for management of both acute and chronic pain that used mainly pharmaceutical approaches. Many of these groups (including the American Pain Society) received funding from Purdue Pharma, the manufacturer of Percodan (oxycodone and aspirin) and subsequently Oxycontin (long-acting oxycodone). 15
Individuals such as Stratton Hill, an oncologist at MD Anderson, came before the Texas State Legislature to try to improve the ability of patients with advanced cancer to obtain sufficient pain medication. 15 In Texas and California, this led to the passage of Intractable Pain Acts to protect physicians from prosecution for use of increased opioids. Reviews of pain management from the 1970s to the 1990s describe undertreatment of cancer and noncancer pain.14-16
From 1990 until 1995, there was an increase in 2 to 3 million opioid prescriptions yearly.14-16 In 1995, a key event occurred: Purdue Pharma obtained Food and Drug Administration approval for Oxycontin, a long-acting oxycodone, based on small underpowered trials. 19 The company heavily promoted this drug as nonaddicting.14-16
To assuage physician concern about causing addiction with opioids, Purdue Pharma’s representatives claimed that only 1 in 10 000 opioid-treated patients would become addicted if treated by a physician; no scientific data to support this was presented. Ultimately, Congressional hearings on the current opioid epidemic brought out information that Purdue Pharma knowingly disseminated false information, and in 2007, the company was fined 634.5 million dollars but by then the use of this drug had been responsible for fueling the rise in opioid use for chronic pain in noncancer conditions such as arthritis.16,19
Several key sequential regulatory interventions by governmental and nongovernmental organizations helped to propel increases in opioid use for chronic noncancer pain:14,16
The introduction of the fifth vital sign, by the American Pain Society in 1995, the Veteran’s Health Administration in 1999, and then in 2001, by the Joint Commission (responsible for certifying hospitals to receive Medicare payments) in 2001 overemphasized pain as a quantifiable measure. Subsequently, the use of pain as a vital sign was shown not to be helpful in pain control. 20
The release of a document from the Institute of Medicine that called for high-quality medicine in which patient satisfaction was a proxy for patient experience. Achieving satisfied patients required relief of pain, even if the overall experience was acceptable. The discordance between patient satisfaction and pain relief was not fully acknowledged.21,22
The creation by the Agency for Healthcare Research and Quality of the Hospital Consumer of Healthcare Providers and Systems (HCAHPS) Survey that incorporated patient satisfaction data as a proxy for quality with 3 questions related to pain in inpatients.
The requirement in 2005 by the Deficit Reduction Act for hospitals to submit the results of these surveys or incur a penalty in their reimbursement by Medicare.
In 2010, there was an expansion of the HCAHPS Survey data’s role in reimbursement by rewarding hospitals that scored high in clinical processes, outcomes, and patient experience. The third domain accounted for 30% of the overall score, making the 3 questions on pain, disproportionately important. The focus of the 3 questions was whether the patient got medicine for pain, was the pain controlled, and was everything done for their pain. This led to opioid use for minor procedures. Patients who were denied medication scored the institutions lower. 14
The number of pills on each prescription increased so that patients would get adequate amounts to control their pain.6,8,14,16 These practices increased the risk of opioid use disorders (OUD). A recent review found that ~80% of individuals using heroin had previously used prescription opioids for nonmedical reasons. 23 Pills were shared with family members. If patients could no longer get the prescribed medication, there was another source in illegal drugs including IMF or heroin.2,6,8,14
What is the solution? Several approaches have been taken: prescription drug monitoring programs, with some success, is being used to identify patients getting multiple prescriptions for opioids at the same time.24,25 Mandatory educational programs for relicensure of health care providers are in place in increasing numbers of states.26,27 As of 2018, insurers, public and private, are limiting payments, based on the amount of daily morphine equivalents in opioid prescriptions. The number of opioid prescriptions written per 100 persons has fallen.6,8,24-27 Recently, the use of naloxone has led to a decrease in overdose deaths in community analyses. 28 Use of combinations of opioid and opioid antagonist are being developed: buprenorphine and other Medication Assistance Therapies are being promoted.14,16,29 In individuals seen in emergency departments for overdose, 65% to 75% were classified as suicidal. 30 There are estimates of 65% to 75% of individuals who overdose having concomitant psychiatric disorders. 31 In an accompanying editorial to the article by Rummans, Srivastava and Gold, psychiatrists at the Mayo Clinic, note that there is a 15% recidivism rate among individuals who overdose. 32
Increasing recognition of predictive factors both in chronic noncancer pain clinics and cancer-related pain clinics has led to increased use of multiple approaches—including teams of providers and individual counseling.27,33,34At the medical board level, many states have limited the duration of first opioid prescriptions following surgery and for nonsurgical acute pain.35,36 Critical appraisal of the published research is occurring including a recent overview of opioids for chronic pain that showed only modest benefit on function and pain control for morphine and transdermal fentanyl and no benefit for oxycodone and hydrocodone. 37
The ability to identify patients who have potential for misuse is improving. 34 Recognition that issues with opioid use exist in dental and veterinary care is occurring. 38 Disparities in management across racial, sex, and ethnic groups are being explored. 39
Increasingly, a body of literature is accumulating with better quality data and improved statistical analyses.37,40 Critical reviews of the interventions are appearing. 41 Recognition of gaps in the evidence base and the quality of studies is increasing.42,43 National Institutes of Health’s efforts have focused on better understanding of mechanisms of pain that may lend themselves to therapeutic interventions. 44 Recent guidelines from the Centers for Disease Control and Prevention limit the quantity of medication given. 45 The scientific basis for these guidelines is modest.19,40 Other countries have ranked the guidelines by the quality of evidence.46,47 An increasing body of literature suggests that other nonopioid medications such as cannabinoids and nonpharmacologic interventions such as mindfulness therapy may be effective in pain control.48,49 These studies are often small and poorly controlled. The use of addiction services and other nonpharmacologic approaches such as cognitive behavioral therapy require additional resources.
Finally, there is increased recognition of the problem of OUD in patients with cancer.50-52 Similar to postoperative patients without cancer, evidence of OUD is emerging in patients with cancer who continue opioids after surgery or after chemotherapy.50,53 This may have implications for physician reluctance to prescribe opioids for the management of cancer pain.50,51,54 In outpatient clinics developed to manage pain in the cancer survivors, strategies are being developed to both identify and manage these issues. 33 Furthermore, as therapies for cancer have increased and become more effective, there are now nearly 16 million individuals who are identified as survivors with the number expected to increase to 20 million by 2040. 55 These individuals may have had multiple surgeries, courses of radiation, and chemotherapy leaving them with deficits in function but also pain due to scars and neuropathy. Recent guidelines developed by the American Society of Clinical Oncology for continued (chronic) use of pain medications in this group address this issue in the current era of reduction in opioid use. 54
Much of the corrective actions focus on health care providers and the pharmaceutical industry and restriction of use. However, as Dasgupta has pointed out, societal issues frame the opioid epidemic as part of the overall pattern of substance abuse in the United States. 5 Most disturbing is that the number of deaths from prescription opioids may be slowing but the number of deaths from heroin and fentanyl preparations has risen such that they account for more than half of the opioid overdose deaths annually.3,4,7-9,10,27 Whether these more fundamental issues—such as societal, cultural, and racial—can be addressed remains to be seen.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed equally to the content, design, interpretation, and writing.