
Abstract
Objectives
Many cancer survivors experience chronic pain after completing curative-intent treatment. Based on available data, chronic pain may be undertreated in this context; however, little is known about cancer survivors’ experiences with clinical management of chronic pain. The purpose of this study was to better understand cancer survivors’ pain management experiences after curative-intent treatment.
Methods
We conducted 13 semi-structured interviews with a convenience sample of cancer survivors who had completed treatment for stage I-III breast, head/neck, lung or colorectal cancer. We used a thematic approach to qualitative data analysis.
Results
Participants described that chronic pain often goes unrecognized by their providers, potentially due to limitations in how pain is assessed clinically and the tendency of both cancer survivors and providers to minimize or invalidate the pain experience. To improve communication, participants suggested that providers ask more open-ended questions about their pain, help them to establish functional goals, and provide patients with options for pain management.
Significance of Results
This study demonstrates the importance of provider-initiated communication around pain management for cancer survivors to make them feel more supported in their care. Communication and shared decision-making interventions may improve cancer survivor-provider communication around chronic pain management, addressing an important gap in survivorship care.
Keywords
Introduction
The population of cancer survivors in the United States is expected to surpass 20 million by 2026. 1 The expansion of the cancer survivor population is largely due to clinical advances in cancer early detection and treatment and a growing elderly population at higher risk of disease. 2 Chronic pain is common among cancer survivors, with some studies estimating that 35% of cancer survivors experience long-term pain after completing treatment.3-6 Chronic pain reduces cancer survivors’ quality of life and is associated with employment-related challenges and increased financial hardship.4,7
Despite the demonstrated prevalence and impact of chronic pain, many cancer survivors may experience suboptimal chronic pain management. 8 There are several factors that may contribute to incompletely managed chronic pain in general. These include concerns about opioid addiction (particularly in the context of the ongoing overdose crisis),9-11 limited access to multimodal pain treatment, 12 and limited provider training in managing chronic pain.13-15 Patients may also under-report chronic pain to their providers during clinical encounters. 10 These challenges may be exacerbated in the cancer survivorship context, where care is often fragmented. 16 In addition, providers may underappreciate the prevalence of chronic pain following completion of cancer treatment and may feel that managing opioids or other narcotics is outside their expertise. 15 Yet few studies have actually documented cancer survivors’ experiences with chronic pain management,8,17-19 none of which explored strategies that may lead to more constructive interactions related to chronic pain management in cancer survivorship.
To help address these gaps in understanding, we conducted semi-structured interviews with cancer survivors with chronic pain to better understand their experiences. Our objectives were to explore (1) factors that facilitate effective chronic pain management; (2) challenges or unmet needs that may exacerbate chronic pain or impede its effective management; and (3) potential solutions to those challenges or unmet needs. We were particularly interested in cancer survivors’ interactions with providers, and how these interactions might facilitate or impede effective management of chronic pain.
Methods
Study Design
We conducted individual semi-structured interviews with cancer survivors with chronic pain who had received cancer treatment at the Duke Cancer Center, a large comprehensive cancer center in Durham, NC. Cancer survivors were eligible to participate if they (1) had been diagnosed with stage I-III breast, colorectal, squamous cell head/neck or non-small cell lung cancer in the five years prior to enrollment; (2) had completed curative-intent cancer treatment (surgery, radiation, and/or chemotherapy) at least three months prior to enrollment; and (3) described themselves as living with pain for three months or longer. Cancer types were selected based on the known prevalence of chronic pain among breast, colorectal, head/neck, and lung cancer survivors. 6 We chose to focus specifically on survivors who had completed primary treatment as their sources of pain are often different than those with active cancer and may include post-surgical pain, neuropathic pain or pain related to maintenance therapy. In addition, recommendations for pharmacological pain management are more conservative for those who have completed treatment vs those who are still in active treatment, especially as it relates to narcotics. 20
We used the Consolidated Criteria for Reporting Qualitative (COREQ) Research to guide data collection, analysis and reporting. 21 This study was approved by the Duke University Health System Institutional Review Board.
Participant Sampling and Recruitment
We aimed to enroll at least 12 individuals, seeking thematic saturation. 22 We used several recruitment strategies. First, we identified potentially eligible cancer survivors using institutional cancer registry data linked with electronic health record data on cancer treatment and opioid use. Patients who had completed cancer treatment, had no evidence of recurrence or progression, and who received opioid prescriptions in each of the prior three months were included. Additional recruitment efforts included (1) referral by the treating oncologist and (2) contacting patients who had completed a randomized control trial of a behavioral intervention for cancer-related chronic pain. 23 Prospective participants were mailed a letter explaining the study. Those who did not opt out of further communication were contacted by a research coordinator to confirm eligibility and obtain informed consent verbally. After consenting, participants completed a basic demographic and health survey.
Of the 52 individuals mailed a recruitment letter, none opted out of future communication. Thirty were reached via phone for screening. Of those, 16 were confirmed eligible to participate, two of whom declined during consent. Fourteen individuals consented to participate and one was not included in the analysis as they were deemed ineligible to participate after consent.
Data Collection
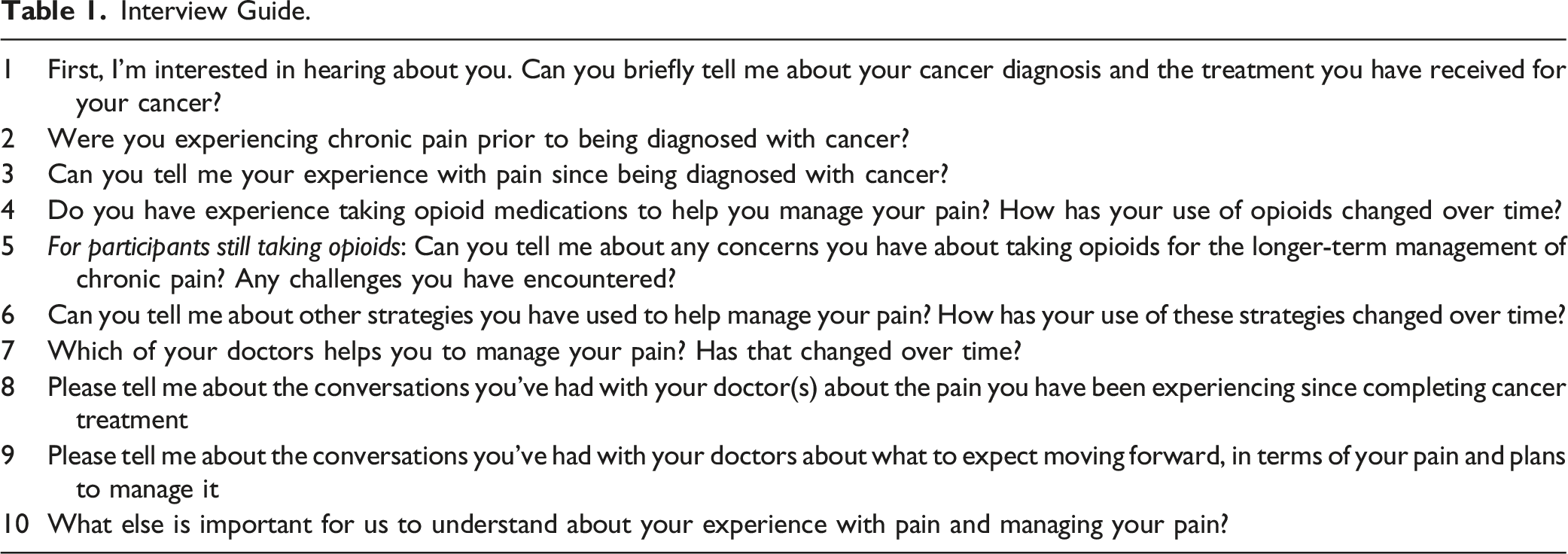
Interview Guide.
Qualitative Analysis
Data were analyzed using both inductive and deductive thematic content analysis to identify emergent themes from participants’ responses. 29 First, the qualitative analysis team (DC, LF, AO, CM) reviewed the same 3 transcripts to become familiar with the data and develop the initial coding framework. Next, two coders (AO, CM) conducted line by line coding of two transcripts and met with the rest of the qualitative analysis team to discuss the transcripts and modify the initial coding framework. Then, the two coders double coded the remaining 11 transcripts, meeting regularly to discuss each transcript and reconcile differences, discuss themes and restructure the initial framework as needed. In the final stage, the team identified major themes and associated quotes to summarize the results. Organization of qualitative data analysis was conducted using Nvivo version 12 software.
Results
Clinical and Demographic Characteristics
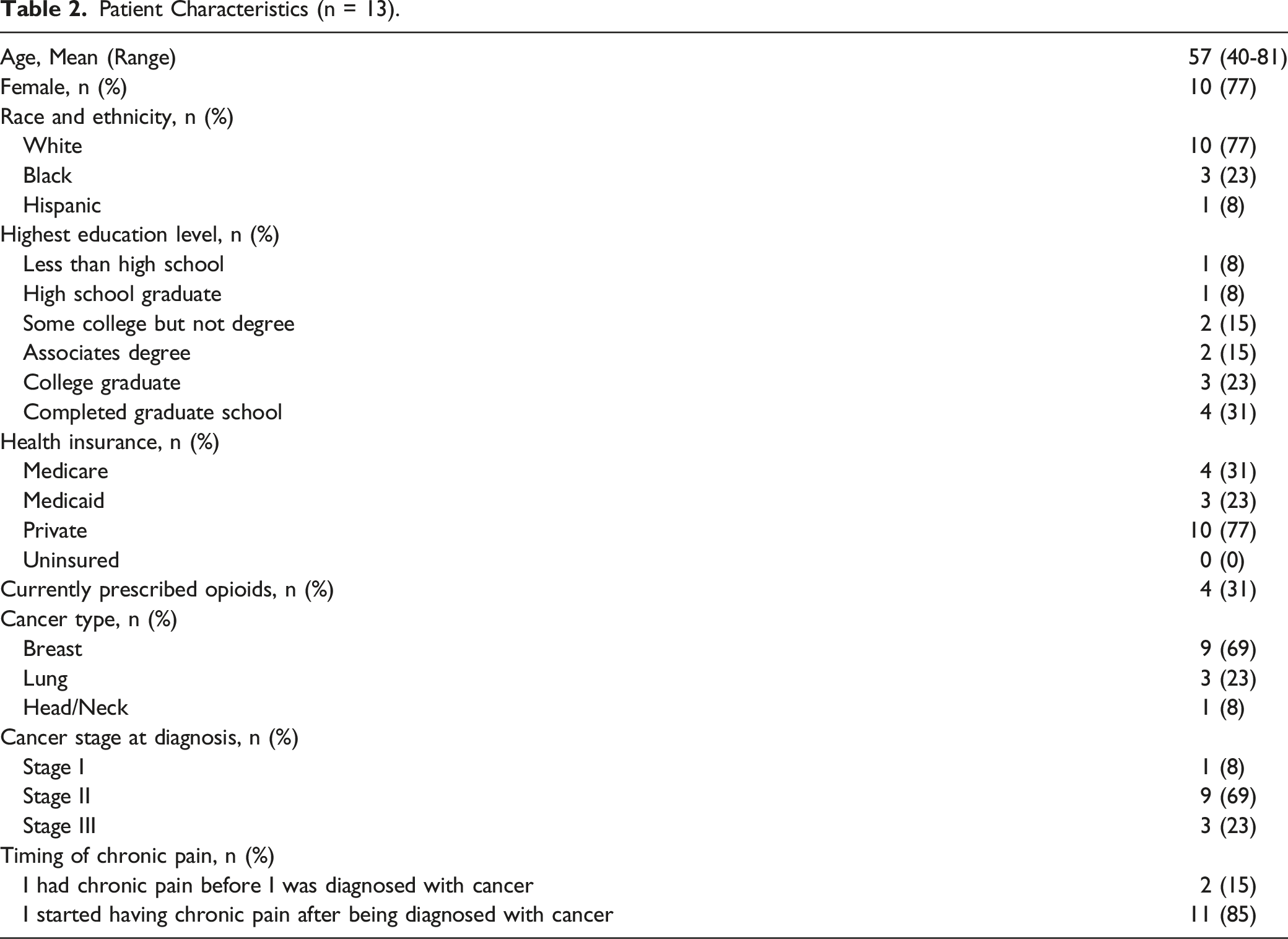
Patient Characteristics (n = 13).
Chronic Pain Characteristics and Experiences
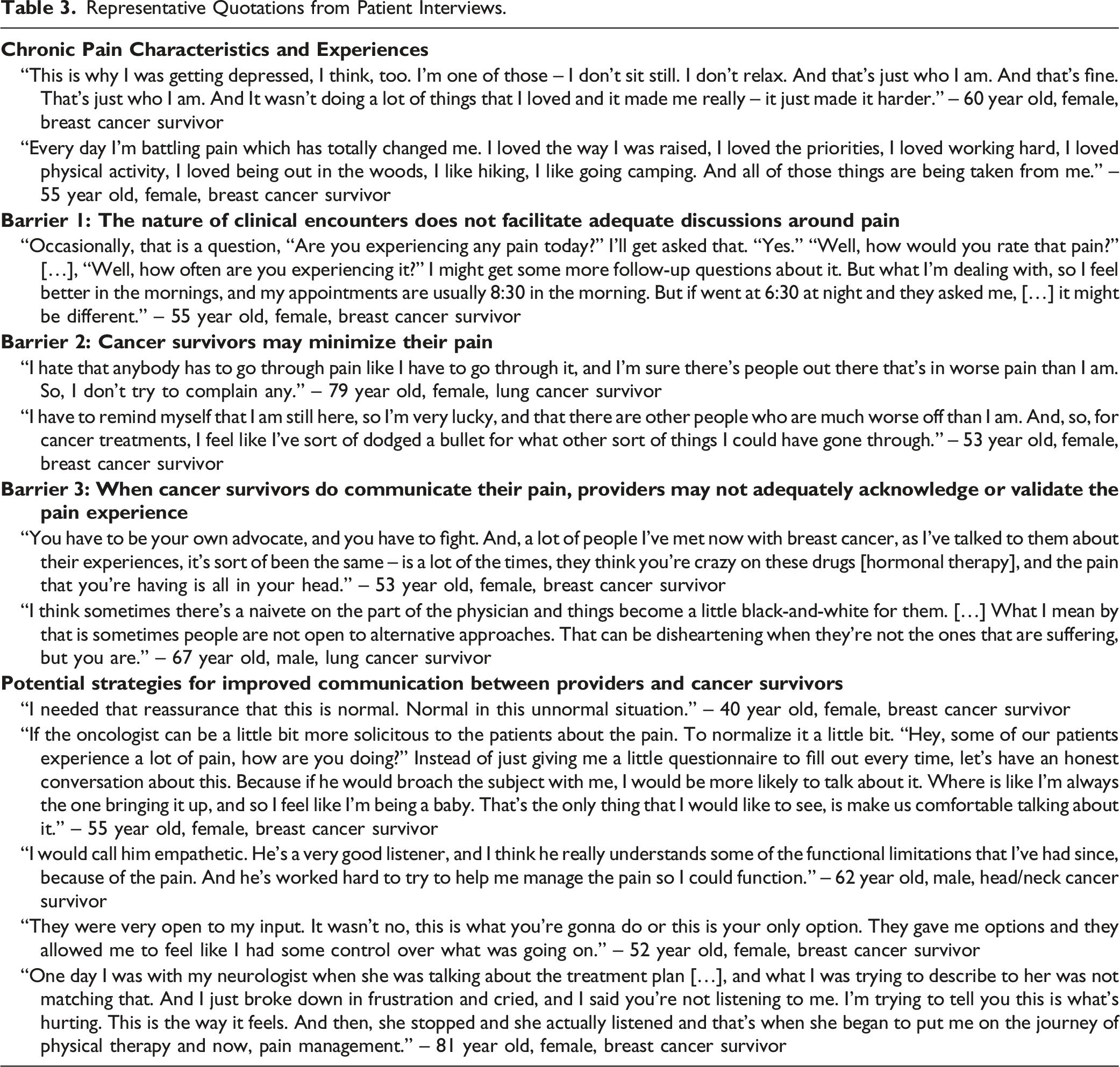
Representative Quotations from Patient Interviews.
Cancer Survivor-Provider Interactions
When describing pain management interactions with providers, participants emphasized the importance of feeling understood by their care team. Their care teams included a mix of primary care and specialty providers, including oncologists and palliative care providers as well as, occasionally, neurologists and pain specialists. In general, participants did not identify a specific provider or providers as their primary pain provider. A few participants described only positive experiences in which they felt validated and supported by their providers. The majority described feeling, at times, a disconnect between their own chronic pain experiences, with pain fundamentally altering their day-to-day lives, and limited communication with their providers around pain management. When they did communicate their pain to providers, participants described often feeling misunderstood. All participants discussed strategies that might support effective communication about pain and help cancer survivors feel understood in their pain experience. Below, we describe interview findings related to key barriers to effective pain communication and potential strategies to overcome them (Table 3).
Barriers to Effective Communication About Pain
Barrier 1: The nature of clinical encounters does not facilitate adequate discussions around pain
Participants described that their appointments are often short-“five minutes and that’s it”-and that pain management is not always prioritized. They reported being asked to provide a pain score only at some appointments, and did not feel this was an adequate measure to reflect the nuance of their pain experience, including pain fluctuating throughout the day and limiting their activities. Limited time and inadequate pain assessment made it difficult for participants to have open and candid conversations with providers about their pain.
Barrier 2: Cancer Survivors may minimize their pain
Participants described sometimes minimizing their pain, both to themselves and to their providers. One reason for minimizing pain included a sense that they should feel ‘lucky to be alive.’ Participants also described feeling like they had already asked enough of their providers and the health system, and feared that bringing up their pain could be seen as ‘complaining’ or ‘being difficult.’
Barrier 3: When Cancer Survivors do communicate their pain, providers may not adequately acknowledge or validate the pain experience
When proactively seeking pain management, participants described sometimes feeling misunderstood or unheard by their providers. Participants described how providers may question the intensity or dismiss the origin of their pain. Some participants described encounters in which providers responded in disbelief to persistent pain. Participants explained that, if the provider could not identify the origin of a symptom, they may question its validity in a way that makes cancer survivors feel dismissed. This contributed to participants’ feelings of distress and anxiety.
Similarly, some participants described struggling to connect with providers who did not appreciate how exceptionally distressing their experience was. This was frustrating for cancer survivors with untreated pain. If their provider was unwilling to continue an opioid prescription and/or try alternative approaches, it indicated that they did not understand the suffering.
Potential Strategies for Improved Communication
Participants reported that they felt understood when providers recognized the impact of chronic pain on their lives, helped them to work towards functional goals and engaged them in identifying pain management options.
Participants discussed strategies their providers had used, or that they wished their providers would use, to help them feel more comfortable communicating about their pain, and more supported and understood in their pain experience. Participants who reported barriers to effective communication suggested that providers could help by normalizing pain, and asking about it more regularly and in an open-ended way.
Similarly, those who reported positive experiences described how providers listened and asked open-ended questions about the pain experience. Setting functional goals with a provider was important to survivors in this sample and made them feel supported. In addition, having options made patients feel a part of the decision-making process. Participants appreciated working with a provider who was willing to try different things, reassess the strategy as needed and be realistic about the patient’s capacity.
Discussion
The purpose of this study was to explore cancer survivors’ experiences with clinical management of chronic pain during survivorship, with a particular focus on their interactions and communication with providers. Participants in this study described several communication challenges, including limited clinical assessment of pain, and both patients’ and providers’ tendencies to minimize or invalidate pain experiences, leading to dissatisfaction with the support they received from their care team and in turn, the pain management provided to them. Generally, participants felt more supported when providers initiated pain-related conversations and provided several options for pain management. Our findings highlight several potential opportunities for intervention development to improve chronic pain management in cancer survivorship. Interventions may be applicable to the range of settings in which cancer survivors receive their follow-up care, including primary care, oncology, and palliative care.
The cancer survivors we interviewed described chronic pain as having a profound impact on their daily lives, reducing function, and causing significant psychological distress. Some participants alluded to a sense of perceived injustice in which parts of their lifestyle had been taken from them by their cancer diagnosis and subsequent chronic pain. In prior studies, cancer survivors and patients receiving cancer treatment have reported similar feelings of perceived injustice and pain-related distress resulting in a lost sense of identity, reduced quality of life, and persistent worry about the future, even after becoming disease free.10,18,30,31 Similar to another study, 8 participants in our study reported sometimes feeling dismissed by providers when presenting with pain. They described inadequate pain assessment and some participants described minimizing their own pain for fear of being dismissed or seen as complaining to providers who may have saved their lives. One prior qualitative study reported a similar finding, where patients on active cancer treatment feared being fully forthcoming with their providers about their pain, potentially leading to incomplete pain management. 10 Since providers may not know that their patients have persistent or significant pain after cancer treatment, they may not prioritize its assessment during survivorship encounters.
Some participants in our study described the use of the 0-10 pain score as a vital sign to assess pain but felt it did not fully capture the multidimensional aspects of their chronic pain. Pain assessment could be improved by inviting patients to discuss their pain in a more comprehensive way, focusing on the impact of pain on daily functioning. This may be especially important for cancer survivors who have completed treatment and may be seeking to re-engage in roles and activities that were important to them before cancer diagnosis. Providers who care for cancer survivors could consider using a validated pain interference scale, like the Pain, Enjoyment of Life and General Activity (PEG) scale 32 or Brief Pain Inventory (BPI) 33 to better measure the nuanced pain experienced, improving subsequent pain management. For example, in one randomized trial, researchers found that using the BPI to assess pain in hospitalized cancer patients led to increased administration of opioid and non-opioid analgesics and greater pain reduction for patients, compared to standard care. 34 In a recent observational study of chronic pain management in primary care, patients with higher pain impairment, as defined by their PEG scores, were more likely to receive pain diagnoses, along with pharmacological and physical therapy interventions. 35 More research is needed to assess the feasibility and acceptability of using the PEG, BPI or other pain assessment tools with cancer survivors in survivorship care settings (eg, primary care, oncology, palliative care).
Routine use of meaningful pain interference measures in cancer survivorship care settings may also support more effective communication about chronic pain and improve cancer survivors’ satisfaction with communication. Routine assessment may be particularly helpful for effective communication about pain if coupled with supportive interventions targeting cancer survivors and/or providers. For example, self-management interventions empower cancer patients to communicate with providers about their pain, while educating and training providers on pain assessment and management to improve their skills and confidence. 36 Shown to reduce pain among cancer patients in active treatment 37 -these interventions could be adapted for the survivorship setting and triggered by high pain inference scores. At the provider level, high pain interference scores could trigger decision support38-40 not only around management strategies but also communication prompts to foster patient-centered management plans using shared decision-making.
Relatedly, participants in our study wanted to be involved in identifying and working towards realistic functional goals with the support and encouragement of their provider(s). This perspective is consistent with the American Society of Cancer Oncology’s patient-provider communication guidelines, 41 establishing a practice of shared goal-setting and decision-making may help survivors feel more supported by their care team. In a recent survey study of cancer patients and survivors, most reported that they expected their providers to discuss treatment preferences and functional goals but felt reluctant to share them unsolicited as they did not feel providers were interested or had time to discuss with them. 42 Shared decision-making (SDM) interventions, in which both the patient’s and provider’s preferences and expertise contribute to mutual agreement, 43 may be appropriate for chronic pain management in survivorship context. SDM tools and decision aids have been linked to improved patient knowledge, treatment adherence and patient satisfaction in diverse settings44-46 but more research is needed to develop and test an intervention specific to chronic pain in the cancer survivorship setting.
Finally, although we asked participants which provider or providers helped them to manage their pain, most did not identify a specific provider or providers as primarily responsible for pain management. This suggests cancer survivors may benefit from more proactive planning (eg, as part of survivorship care planning) to clarify which member of the care team can help to manage ongoing pain. Proactive planning may also help to elucidate gaps in chronic pain management expertise on the care team. For example, most patients in our sample experienced significiant distress related to their chronic pain, highlighting the importance of multidisciplinary care teams that incorporate pain psychology.
Given limited research on cancer survivors’ pain management experiences, our study was exploratory in nature. The use of a convenience sample of cancer survivors receiving care at one medical center limits the generalizability of these findings, as survivors from other settings may have different experiences. However, it is important to note that qualitative studies are not intended to be generalizable 47 and our results are in alignment with the peer-reviewed literature. Of note, the majority of our sample were white, well-educated women with breast cancer. It is reasonable to expect that a less privileged group of cancer survivors may report experiencing even greater barriers to effective management of chronic pain. For example, providers are even less likely to recognize the presence and severity of pain, and thus undertreat pain, in racialized and minoritized groups, a phenomenon well documented in the literature.48-50 Additional research is needed with a more demographically and clinically diverse group of cancer survivors to further explore their unique pain management experiences with providers.
Survivorship is an important phase of care that requires strong patient-provider communication to improve pain and quality of life outcomes for cancer survivors. Ensuring that cancer survivors feel comfortable communicating with their care teams about their pain requires provider-initiated pain assessments, including pain interference measures, and prioritization of pain management in health care planning. Interventions directed at both patients and providers that include elements of self-management and shared decision-making may benefit survivors as these tools are meant to facilitate communication by training both patients and providers to make pain-related conversations as satisfying and constructive as possible. Additional research is needed to explore the feasibility and acceptability of such interventions in a range of outpatient settings in which cancer survivors may be treated (eg, primary care, oncology, palliative care).
Footnotes
Acknowledgments
We would like to thank the study interviewers, Margaret Falkovic and Sam Farley, along with all our participants for their contributions to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is included as part of the Duke University School of Medicine Opioid Collaboratory portfolio, grant funded by the Duke Endowment and administered through the Duke Department of Population Health Sciences. The Collaboratory’s mission is to save lives and reduce the harmful impact of opioids in North Carolina through the development, implementation, and evaluation of system-level interventions. We acknowledge support from the Duke Cancer Institute Behavioral Health and Survey Research core as part of the P30 Cancer Center Support Grant (Grant ID: P30 CA014236) and from the Center for Onco-Primary Care at the Duke Cancer Institute.