
Abstract
According to some estimates, the United States wastes as much as 30% of health care dollars. Some of that waste can be mitigated by reducing certain costs associated with Medicaid. We chose 5 areas of savings applicable to Medicaid: (1) modification of physician payment models to reduce unnecessary care, (2) development of a medication adherence program for patients dually eligible for Medicaid and Medicare support (“dual eligibles”), (3) improvement in unnecessary admissions and readmissions for dual eligibles, (4) reduction in emergency department visits among children in Medicaid and dual-eligible beneficiaries, and (5) improvement in adoption of end-of-life advance directives. We chose the states from both ends of the spending spectrum: the 5 with the lowest annual Medicaid expenditures: Wyoming, South Dakota, Montana, Vermont, and Alaska, and those with the highest: California, New York, Texas, Pennsylvania, and Florida. This spectrum demonstrates the range of potential cost-saving measures, from US $23.6 million in Wyoming to US $3.4 billion in California. We conclude that there are a number of ways to reduce Medicaid spending and improve quality. To the extent that states have already adopted programs addressing the same problems, our approach may be supplementary but the total savings may be achieved with a combination of current initiative and those described here. As Medicaid creates savings, physician payment could be increased to attract more physicians into caring for Medicaid patients.
Introduction
According to the Institute of Medicine, 30% of dollars spent on health care is waste in the American medical system. 1 Berwick and Hackbarth 2 conducted additional analysis and placed a midpoint estimate of waste at 34% of national health spending. Although Medicaid programs operate with extremely low margins, and prospective savings will not approach 30%, savings are possible. Medicaid in the state of Texas, for example, represents just over 30% of the state budget and covers 4.4 million people. In 2016, Texas spent US $18 billion on Medicaid; with the Federal Medical Assistance Percentage (FMAP) at 57.13%, the federal government paid US $20.5 billion, for the total state + federal shares at US $38.5 billion. 3 Even with only a 5% reduction, annual savings could equal well over US $1 billion, which could be used to improve care and potentially redistribute funding to chronically underfunded areas, such as payments to physicians. In Alaska, where the FMAP is 50%, the total spending on Medicaid (including state and federal contributions) in 2016 was US $1.42 billion 3 ; Alaska’s portion of this payment is $710 million. Applying a 5% savings would yield US $35.5 million for other state programs and priorities.
This article adds to current work on Medicaid reform by exploring specific pathways to find and estimate savings that, at the same time, maintain or improve quality of care. These results should be applicable to Medicaid programs across the states, as well as to other parts of the US health care system. We use the “Wedges Model” for examining proposed reductions in health care spending, a framework Berwick and Hackbarth 2 refined to examine a variety of cost-saving initiatives to target wasteful spending in key areas such as failures in care coordination/delivery and overtreatment. The key areas identified in the Wedges Model led us to identify 5 approaches to savings, which could contribute to stabilizing health care spending through streamlining and strengthening care coordination and minimizing unnecessary treatment. The innovative initiatives highlighted are adaptable, relatively low-cost investments, yielding meaningful savings to Medicaid. The programs also aid vulnerable and costly health care populations. The proposed initiatives, applied to the 10-state sample to represent the full range of potential cost savings, include reduction in unnecessary care, improved medication adherence in dual-eligible beneficiaries, improved care for dual-eligible beneficiaries to reduce hospital readmissions, reduction in emergency department (ED) visits among children in Medicaid and dual-eligible beneficiaries, and improved coordination for end-of-life care.
Pathways to Savings
Health workforce initiatives
To reduce overutilization of EDs
The overuse of EDs is a large drain of health care dollars. Routine care provided in an ED setting can be 2 to 5 times more expensive than the same care provided in an alternate setting such as an urgent care clinic. 4 A Health Partners study discovered charges for treating strep throat in the ED to be US $328, US $130 at an urgent care center, and US $122 in a primary care office. 5 Clearly, based on these figures, it is critical to find ways to treat as many patients as possible outside of an ED due to the 261% price premium that ED care costs.
Massachusetts conducted an in-depth analysis of their ED usage and the emergent status of patient’s health when visiting the ED. Of all ED visits, 42% were classified as avoidable. 6 If we extrapolated this percentage to California, this would translate to 5 749 000 avoidable ED visits per year, and in South Dakota, this percentage would translate to 114 000 annual avoidable ED visits. 7 The Massachusetts report also highlighted disparities between incomes: the residents in the lowest income quartile, after adjusting for age and sex, had greater than 3 times the avoidable ED rate than residents in the highest income quartile. The lowest income quartile would represent uninsured and Medicaid populations.
The most beneficial program to reduce ED usage is one that prevents unnecessary trips to the ED. This can involve enhancing programs such as “Grand-Aides” to assist patients in health care management and reduce their perceived need for ED treatment. Grand-Aides are nurse aides who are closely supervised by nurses and foster relationships with patients and family with the goal of appropriate use of the ED. Calculations indicate Grand-Aides could potentially reduce Medicaid ED visits by 74% in Medicaid children and patients dually eligible for Medicaid and Medicare support (“dual eligibles”). 8
To improve medication adherence among dual eligibles
About 50% of patients with chronic diseases take their medications appropriately. 9 Medication nonadherence among the other 50% generates a significant cost burden. Dual eligibles represent 15% of the national Medicaid population but require 33% of Medicaid spending. 10 This high level of spending can be partially attributed to the dual-eligible population’s vulnerability and complicated chronic health conditions. Significantly, the Grand-Aides program has achieved a 91% medication adherence in patients with heart failure 1 month after discharge. 11
To reduce avoidable hospitalization among dual eligibles
Dual-eligible beneficiaries are at a higher risk for potentially avoidable hospitalizations—admissions and readmissions. Among hospital visits in this population, just over one quarter (26%) of hospitalizations have been determined to be unnecessary, many due to readmissions. 12 The Grand-Aides program is one initiative achieving the aim of reducing readmissions with a demonstrated ability to reduce hospital readmissions by 58%. 11
Payment Initiatives
To reduce unnecessary care
Most physicians are still predominately paid on a fee-for-service (FFS) basis. Medicaid programs could propose new payment methods. For physicians who are already part of hospital systems or Accountable Care Organizations (ACOs) it would be reasonable to convert to a salaried system (at their current yearly income), with a relatively modest bonus (ie, 5%-10%) for quality. Physician income does not need to decrease with these changes. As Medicaid generates savings in this and other areas, physician payment should increase to attract more physicians into caring for Medicaid patients. Salary + bonus would be the dominant method of payment. For physicians not in systems, Medicaid could test the resultant effect on patient care of paying a certain amount per patient with a bonus for quality. It could also change to FFS payment with not only incentives for quality but also disincentives for doing what physicians’ own specialty societies determine in their guidelines to be unnecessary or harmful. The Centers for Medicare and Medicaid Services (CMS) has announced that by the end of 2018, more than half of Medicare dollars will be paid via alternative payment models that focus on reducing the negative incentives associated with paying physicians based on FFS. Of note, the health care systems in the United States that are routinely ranked the highest for quality (eg, Mayo Clinic, Cleveland Clinic, and Kaiser Permanente) have salaried physicians, some with and some without a bonus. Such systems have demonstrated savings between 20% and 46% due to a decrease in tests ordered and procedures performed.13,14 For the purposes of this analysis, we assume 15% savings.
Advance directives
To improve end-of-life care
Approximately US $205 billion is spent in the United States on patients in the last year of life or 13% of the annual total spending on health care. 15 A number of strategies are incorporated to improve the quality of a person’s last days. These approaches must be exquisitely sensitive to improving the quality of life of the patient and loved ones address the mislabeled “death panels” from the past. The most successful approach involves recording the wishes of the individual patient and family, broadly called “advance directives,” which fall into 3 categories: living wills, power of attorney and health care proxy. One calculation places the savings through advance directives at US $5585 per patient. 16 This figure was the most recent study reported from a 2016 systematic review of advanced care planning cost savings. Estimates in the review varied widely from US $1041 to US $64 830 per patient, based on the length of the study and the method for measuring cost. 17
These savings are realized by reduced usage of EDs and reductions of extraordinary life-saving measures while honoring the patient’s and their family’s wishes. Only 65% of nursing home patients have an advance directive. 18 There is a great opportunity, as up to 90% of nursing home patients and families will complete advanced directives if a physician initiates the discussion. 19 The percentage of patients aged 65 and older with recorded advance care plans or surrogate decision makers designated in their medical records is a quality communication and care coordination process measure in the Merit-Based Incentive Payment System for many disciplines.
Methods
Using Urban Institute calculations as of January 2017, based on CMS Form 64, the 5 lowest total Medicaid expenditure states (Wyoming, South Dakota, Montana, Vermont, and Alaska) and the 5 highest Medicaid expenditure states (Florida, Pennsylvania, Texas, New York, and California), were selected for evaluation. Note that North Dakota and Idaho were likely among the lowest Medicaid expenditure states, but they did not have complete reporting to generate adequate data for equal comparisons; therefore, these states were not used in this analysis. Enrollment figures for Medicaid, full dual-eligible beneficiaries, and children enrolled in Medicaid were obtained from the December 2016 MACPAC Databook for various calculations. 20 The FY17 FMAP was applied to reflect the state share of Medicaid savings. Each approach to savings was applied to the 10-state sample to evaluate potential cost savings. If all programs are implemented, the total financial benefit to states ranges from US $11.8 million in Wyoming to US $1.7 billion in California (Table 1).
Overall proposed cost savings.

Abbreviations: AK, Alaska; CA, California; FL, Florida; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Results
This research explored the states from both ends of the spending spectrum: the 5 with the lowest annual Medicaid expenditures—Wyoming, South Dakota, Montana, Vermont, and Alaska—and those with the highest—California, New York, Texas, Pennsylvania, and Florida. This spectrum demonstrates the range of potential cost-saving measures, from US $23.6 million in Wyoming to US $3.4 billion in California.
Reduction in Overutilization of EDs
Using a statistic of 24.8% of Medicaid children 21 and 44% of dual-eligible beneficiaries, 22 ED visits are calculated for each state for these populations. Next, 50% of the maximum possible reduction from the Grand-Aides program is applied, which is a 37% reduction. The savings applied include the cost of the Grand-Aides program. If the Grand-Aides program were implemented to assist these key populations (assuming 50% of the possible benefit = 37% reduction), it could result in Medicaid savings of US $243 million in this 10-state sample, with state savings ranging from US $409 000 in Wyoming to US $42 million in California (Table 2).
Savings calculations for reduction in emergency department use for children and dual eligibles in Medicaid.

Abbreviations: AK, Alaska; CA, California; FL, Florida; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Improved Medication Adherence
Improved adherence was calculated from 50% to 75% for 4 chronic conditions: hypertension, diabetes, heart failure, and dyslipidemia. 23 State populations for each chronic condition were estimated using data from the CMS Chronic Conditions Chartbook. 24 Assuming that 50% of patients take their medication appropriately, an improvement to 75% adherence would produce savings displayed in Table 3. These significant savings also incorporate increased drug cost as a result of drug adherence. Importantly, those expenses are offset due to overall reductions in health care expenditures for costly services such as ED visits, hospital admissions, additional diagnostic testing, and increased pharmacy expenses related to treatment. For patients with hypertension, potential savings in the 10-state sample equal US $2 billion; for heart failure, total savings equal US $1.55 billion; for diabetes, US $1.17 billion; and for dyslipidemia, US $260 million. The potential cost savings for state Medicaid range from US $5.2 million in Wyoming to US $1 billion in California.
Savings calculations for improvement in drug adherence by dual eligibles, by disease category.

Abbreviations: AK, Alaska; CA, California; FL, Florida; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Reduction in Avoidable Hospitalizations
Assuming the Grand-Aides program would achieve 50% reduction in hospital admissions, and calculating the cost of a readmission based on US $15,435, 25 the net savings to the Medicaid program could range from US $3.4 million in Wyoming to US $684 million in California, including the expense of operating the Grand-Aides program (Table 4). 26 ]
Savings calculations for reduction in hospital readmission costs for dual eligibles.

Abbreviations: AK, Alaska; CA, California; FL, Florida; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Reduction in Unnecessary Procedures
Assuming that paying physicians a salary plus bonus could result in a 15% reduction in tests and procedures; in the 10-state sample (based on the 2016 Medicaid expenditure data), 27 these measures result in state savings ranging from US $3.4 million in Wyoming to US $83.1 million in California (Table 5). Vermont classifies most of the Medicaid expenditures as “other services” so the state savings for this innovation are small, US $170 000.
Savings calculations for reduction in unnecessary care with salaried physicians.

Abbreviations: AK, Alaska; CA, California; FL, Florida; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Data obtained from KFF as of January 2017, The structure of Vermont’s Medicaid program formulates most of the state’s Medicaid expenditures in the category of “Other Services.”
Improved End-of-Life Care
About 21% of dual-eligible beneficiaries are in long-term services and supportive living according to the 2017 MedPAC Databook. 10 End-of-life care cost savings were estimated for each state by applying a 25% increase in advance directives among this population with the estimated saving of US $5585 per directive. This results in state savings ranging from US $1 million in Wyoming to US $203 million in California (Table 6).
Savings calculations for coordination of end-of-life care.
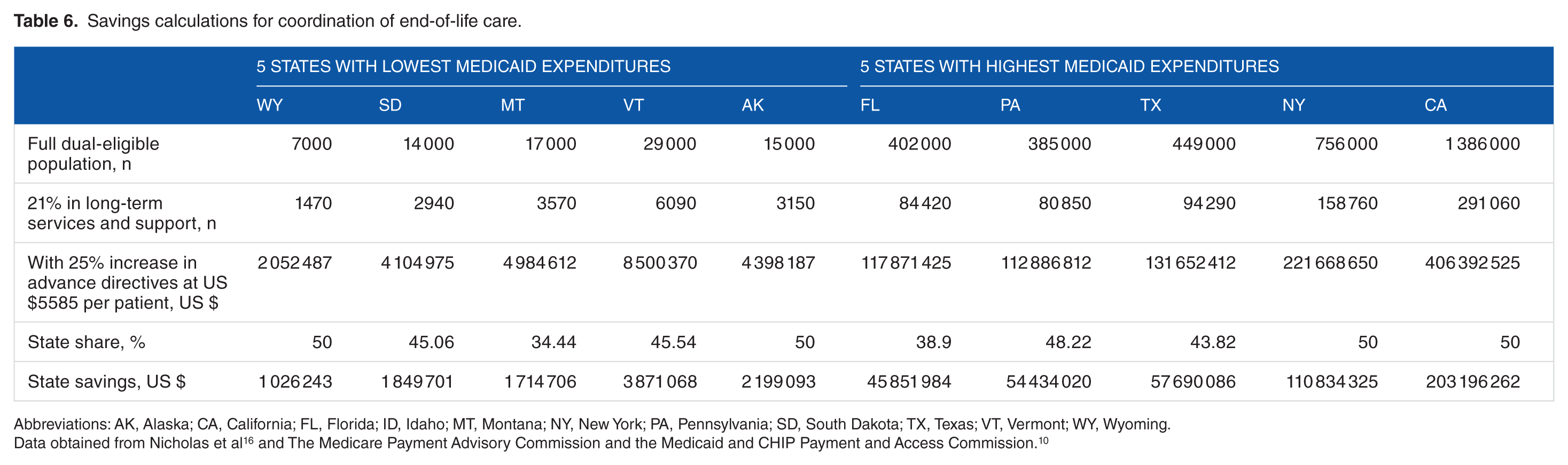
Abbreviations: AK, Alaska; CA, California; FL, Florida; ID, Idaho; MT, Montana; NY, New York; PA, Pennsylvania; SD, South Dakota; TX, Texas; VT, Vermont; WY, Wyoming.
Discussion and Conclusions
Several caveats are important related to the estimated improved adherence calculations: first, the savings are in the short term (ie, hospital admissions over several years) and do not take into account the cost of future disease if the current disease is well-controlled (eg, hypertension is well-controlled and a stroke is avoided, only to have the patient get cancer). Second, there is clear overlap in the patient diagnoses (ie, many patients with diabetes have heart disease). Improvement (and medication adherence) in one of these diagnoses will likely have a positive effect on the other diseases in the patient and therefore these are, again, maximal numbers. Personal reinforcement and teaching are among the most promising approaches to improving medication adherence, as the American Diabetes Association recognizes and recommends. 28 Programs such as Grand-Aides with a 91% medication adherence could be extremely beneficial.
Physician Payments
Although combining alternative physician payment models are the basis for part of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), it is unwieldy. In addition, there will be added expenses as managed care companies and physicians switch to a value-based payment system because the data infrastructure to track these metrics must be in place. These expenses must be netted against potential savings (ie, paid to systems and physicians) as the requirements for financial outlays are real. This issue should be addressed through more sophisticated and interoperable Electronic Health Record (EHR) systems, which are, unfortunately, likely a decade away.
An alternative method to reduce unnecessary care would be to examine the 20 most expensive procedures and tests (because of high volume, high price, or both) and compare the indications for the tests or procedures reported by the ordering physician to national guidelines produced by the physician’s specialty society. A recent such analysis revealed that 34% of echocardiograms performed on preoperative patients were unnecessary and were outside the recommended practice guidelines. 29 We are recommending the physician payment change because it could be achieved more simply (eg, the MACRA regulations could provide an incentive for programs in which at least 50% of their physicians are salaried).
These estimates do not take into account existing state programs that could have already achieved some of the savings. The program overlap poses a significant limitation (ie, the same savings may be attributed to more than one program), as well. The data are likely to be correct within an order of magnitude; rather than focusing on the exact amounts, we suggest that “large (say, 10%), medium (5%) and small (2.5%)” be attached to the possible program savings and be made available as a potential supplement to the cost-saving work already being done by the state Medicaid programs.
We have examined a number of possible approaches to reducing the expense of Medicaid. These savings should remain in the Medicaid program and, for example, help to cover more people and increase physician reimbursement. Increased reimbursements will enhance the number of physicians seeing Medicaid patients, thus improving access for the underserved. If all programs are implemented, the total financial benefit to states ranges from US $11.8 million in Wyoming to US $1.7 billion in California, as illustrated in Table 1. These 5 initiatives also could be applied to commercially insured patients or those covered by Medicare, resulting in major savings across the United States. Realizing these savings in achievable ways suggested in this article could make a major dent in the rising cost of health care.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AG, original concept, design and intervention sections. KF, data sampling and simulation method. KA, expanded data gathering, analysis, results section. SHL, overall organization, integration, discussion and conclusions.