
Abstract
In this article, the reader will get some insights into managing patient with implantable cardiac devices while undergoing noncardiac surgery. We will review basic concepts regarding normal function of pacemakers and implantable cardioverter defibrillators, understanding how their function will be influenced during noncardiac surgeries. You will be guided through management steps from preoperative, intraoperative, and postoperative aspects. In an ever-changing world of medicine, it is important to keep up with progress as more and more patients get implantable cardiac devices.
Introduction
The purpose of this document is to provide a basic understanding, to internal medicine physicians and hospitalists, as to how the functionality of cardiovascular implantable electronic devices (CIEDs) may be affected during noncardiovascular surgery. In the United States, every year, there are more than 100 000 implantable cardioverter defibrillators (ICDs) and 300 000 pacemakers implanted. 1 Due to this growing number, it is not uncommon that these patients will also undergo other types of surgeries during their lifetime. A good understanding on how these devices work will lead to safer noncardiac surgeries and diminish risk of adverse effects. This review article is mostly based on expert consensus statement that was adapted by Heart Rhythm Society and American Society of Anesthesiologists, but complex concepts were simplified or broken down. 2
This concise literature review provides internists and hospitalists with quick reference as to how to approach patients with CIEDs. Although it may seem to be overwhelming, during residency training there is little attention paid to this topic. Nevertheless, it is more common that patients with CIED are being managed by general practitioners, including evaluating them prior to noncardiac surgery. Knowing potential interactions between CIED and electrosurgery and how to manage them will improve patients’ safety during surgeries.
Basic Concepts
It is important to understand basic functions and differences between pacemakers, ICDs, and cardiac resynchronization (CRT) devices. There is one more, relatively recent, group of ICDs—subcutaneous ICD—that has no ability to pace the heart and only manage ventricular arrhythmias. Pacemakers are usually implanted due to sinus node dysfunction or heart block. Pacemakers can have either 2 (atrial and ventricular) or 1 (mostly ventricular, but in Europe atrial lead only may be implanted for patients with sick sinus syndrome) lead. If a patient is in permanent atrial fibrillation, then only a ventricular lead is implanted. The main function of pacemaker is to prevent the heart rate (HR) from falling below a certain limit (mostly below 60 beats per minute [bpm], but sometimes slower HR may be set). It is highly unlikely for pacemakers to be set for managing fast HR. However, ICDs are implanted for primary or secondary prevention of cardiac arrest, and their main function is to pace out ventricular arrhythmia or deliver ICD shock. All ICDs have the ability to pace the heart similar to pacemakers. However, unless the patient is pacemaker dependent, a lower rate of pacing for ICDs is set at or below 40 bpm. This concept is very important. For example, the absence of pacing spikes on an electrocardiogram (ECG), at baseline HR of 50 bpm, does not necessarily mean an abnormal pacing function of ICD. There is one more group of cardiac devices called CRT or sometimes referred to as biventricular device. The CRT device can be just a pacemaker (CRT-P) or more commonly ICD (CRT-D). The purpose of this device, in addition to a pacemaker or ICD, is also to synchronize contraction of the left ventricle to improve symptoms of congestive heart failure (CHF). It is expected that these devices provide constant pacing of the heart as appears on ECG, despite the fact that these patients, most of the time, are not pacemaker dependent.
Pacemaker dependence can be functional or absolute. If absolute pacemaker dependence is present, then without proper functioning of the device HR will not be stable enough to afford hemodynamic stability. Functional pacemaker dependence is a more complex concept. As mentioned above, CRT devices are forced to pace to synchronize the ventricle, but if pacing function is inhibited, there is usually an underlying rhythm that is stable enough to avoid hemodynamic instability. But prolonged absence of CRT pacing may lead to worsening of CHF. Another example of functional dependence is when without pacing, the HR will be less than set by lower rate pacing but will not lead to hemodynamic instability. An example of this may be a patient with sinus node dysfunction who needs acceleration of HR in the atrium to satisfy metabolic demands during exertion. Without proper pacemaker function, HR may be slow, but not slow enough to cause hemodynamic instability.
During most surgeries, electrosurgery is being used for either cutting or to achieve hemostasis. Electrosurgery can be bipolar or, much more often, monopolar. Bipolar electrosurgery is used in ophthalmic surgery, neurosurgery, or microsurgery. Bipolar electrocautery has no interference with CIEDs. 3 Monopolar electrocautery use leads to electromagnetic interference (EMI). 4 Electrical current flows from stylus that is being used to cut or coagulate, through patient body, to a dispersion patch on the skin. This electrical current, when interferes with CIEDs, will lead to different outcomes depending on the type of device implanted. Pacemakers and ICDs respond differently to EMI. When EMI affects pacemaker sensing circuits, it may lead to the inhibition of pacing function as pacemakers will not be able to differentiate EMI from intrinsic heart activity. In absolute pacemaker-dependent patients, it may lead to very slow HR and hemodynamic instability. The ICDs react differently to EMI as sensing circuits also have different functions to detect and treat ventricular arrhythmia. In addition to inhibiting pacing function in patients who are pacemaker dependent, EMI can also lead to inappropriate ICD therapy (deliver ICD shock or antitachycardia pacing) as the device may erroneously interpret EMI as ventricular tachycardia (VT) or ventricular fibrillation (VF) (Figure 1). For the CRT devices, response to EMI will depend on whether it is a pacemaker or an ICD. There are other potential issues that may occur to CIEDs, but they are very rare, ie, device reset, pulse generator damage, or lead tissue interference (eg, increasing pacing threshold). If the electrosurgery current is at least 6 in away from CIED, this risk can further decrease. 5

Example of electromagnetic interference (EMI) on cardiac resynchronization (CRT-D), with inappropriate implantable cardioverter defibrillator (ICD) therapy. High-frequency artifact is noted on atrial lead (A) as well as right ventricular lead (RV) in patient with CRT-D device. This leads to erroneous interpretation of EMI in atrial lead as atrial fibrillation (AF) and ventricular fibrillation (VF) in the right ventricular lead. Eventually, it leads to inappropriate ICD shock (31 J Shk).
A magnet is one of the tools that can be used to eliminate EMI for CIEDs if placed over it. The magnet interacts differently with pacemakers and ICDs. If one places a magnet over a pacemaker, it will make it pace asynchronously and the pacemaker will ignore any intrinsic sensing and EMI. It will prevent a pacemaker-dependent patient from becoming hemodynamically unstable as HR will be at a manufacturer-determined magnet rate (Table 1). Placing a magnet over the ICD will lead to inhibition of all of its therapies for VT or VF, but most importantly, the pacing function will not be affected. For instance, if a patient with ICD is also pacemaker dependent, placing a magnet over it will prevent inappropriate ICD therapy due to EMI, but the patient may become bradycardic and hemodynamically unstable, as the device will not pace asynchronously.
Magnet rates for different manufacturers of CIEDs.
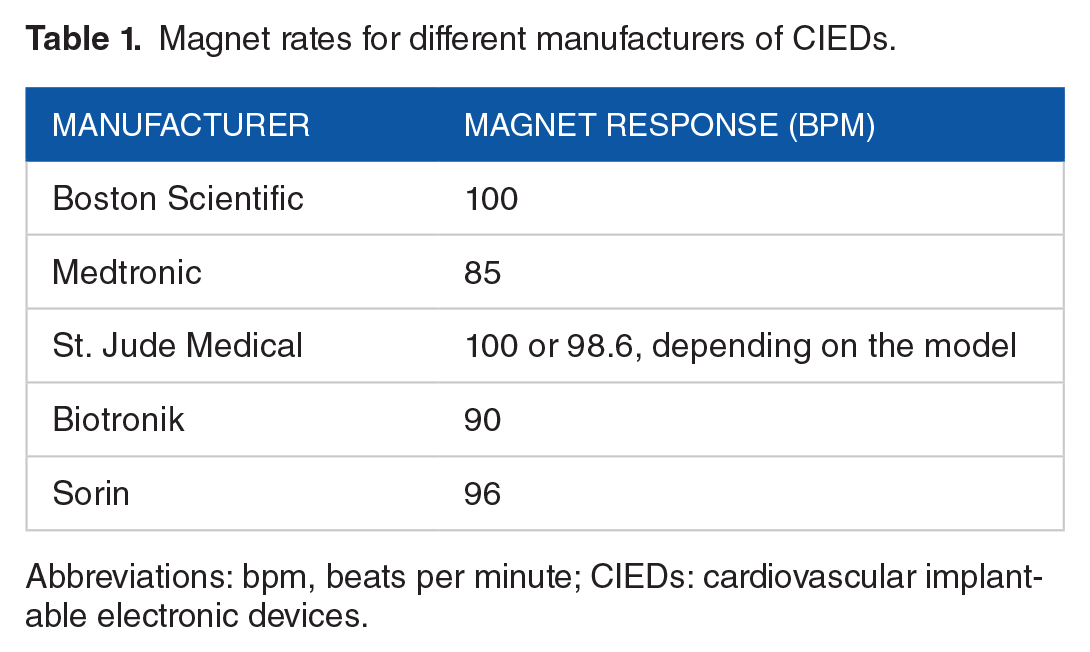
Abbreviations: bpm, beats per minute; CIEDs: cardiovascular implantable electronic devices.
Preoperative evaluation
Prior to most surgeries, patients are being referred to physicians for preoperative risk assessment. During this time, it may be discovered that the patient has CIED. If the patient has CIED, further questioning and investigation are needed to assure safety of the patient during surgery. It is extremely important to determine what type of device the patient has: pacemaker, ICD, CRT-P, or CRT-D. This seemingly simple task can be sometimes challenging, especially if the patient cannot provide or does not know this information; for example, the patient is unconscious prior to surgery (Figure 2). There are a few ways to accomplish this. All patients, after the initial implantation of CIED, will be given an identification card with the description of their device. If this card is not available, reviewing patient’s chest x-ray (CXR) will help in differentiating the type of device and manufacturer, as well. 6 Knowing the manufacturer can be useful as companies have different magnet response rates of pacing (Table 1). If CXR does not yield conclusive information, one may call the manufacturer, which will provide all necessary information and is available 24 hours, 7 days a week (Medtronic, 18005515544; Boston Scientific, 18002273422; St. Jude Medical, 18006819293; Biotronik, 18005470394; and Sorin, 18776637674). Once the presence of the device and its type are established, it is also important to know the last time it was interrogated. If the device was checked within 6 months of the planned procedure, and it was functioning normally, recommendation regarding management of CIED can be given most of the time without reinterrogating it. 7

Difference between pacemaker and implantable cardioverter defibrillator (ICD) on chest x-ray: (A) dual-chamber pacemaker with leads in the atrium and right ventricle and (B) single-chamber ICD with radiodense coil (arrow) in the right ventricle.
To provide accurate recommendations regarding management of CIEDs during surgery, further clinical information should be gathered. Will electrosurgery be used during surgery, and what type? If bipolar electrosurgery is used or no electrosurgery is used, then no adjustments to CIEDs are needed, assuming that the device functions properly based on routine device checks. Furthermore, the location of surgery is important. If the surgery is below the umbilicus, it is highly unlikely that EMI will affect device function.8,9 The position of the patient during surgery is important because if a magnet cannot be safely secured over the CIED, then reprogramming of device will be necessary. There are pluses and minuses for both using a magnet and reprogramming periprocedurally (Table 2). The 12-lead ECG can reveal underlying rhythm and also give suggestion if a patient may be pacemaker dependent. If one sees that every beat in the ventricle is being paced, it should be assumed that the patient is pacemaker dependent, especially in emergent cases.
Magnet use vs reprogramming of CIEDs, benefits, and drawbacks.

Abbreviations: CIEDs, cardiovascular implantable electronic devices; ICD, implantable cardioverter defibrillator; VF, ventricular fibrillation.
Obviously, in an emergent situation, there may be no time for the arrhythmia team (most of the time led by electrophysiologist and supported by nurse practitioner or physician assistant) to evaluate the patient, and therefore, the emergency protocol is followed, as seen in Figure 3. For all emergent and nonemergent cases, it is important that the patient be monitored by electrocardiography and plethysmography or oximetry. All patients should have defibrillator pads placed on them in an anterior-posterior fashion with the ability to pace transcutaneously, if needed. The code cart must be readily available, as well as a magnet, in case it needs to be used.10,11 For all elective cases, it is preferred that the arrhythmia team evaluate the patient and provide recommendations. Communication between physicians caring for the patient plays a vital part in assuring an uneventful surgery. Utilization of manufacturer representative should not be considered as an option to provide recommendations prior to surgery, as these representatives are not clinicians and their knowledge is limited. 12

Protocol for CIED management in emergent noncardiac surgeries.
Intraoperative management
Once the surgical and anesthesia teams receive the necessary recommendations, they will need to provide appropriate monitoring during surgery and be aware of possible changes in the device behavior. Every patient should be connected to an electrocardiography monitor and pulse plethysmography or oximetry. During surgery, when electrosurgery is being used, it may affect not only the CIED but also the electrocardiography monitor. It is important to be able to record peripheral pulse during these interferences. Having more than one lead to monitor ECG may help to distinguish artifact from real arrhythmia. 13 A magnet should be readily available in those cases, when it was not recommended prior to procedure, for the pacemaker patient because one had stable underlying, nonpaced, rhythm. Sometimes, during surgery, due to sedation, the HR may become slow and placing a magnet over the device will initiate an asynchronous pacing and prevent bradycardia. 14
When a patient has an ICD and either magnet or reprogramming was used to deactivate its therapy, it is important to keep the patient on constant ECG monitor and have an external defibrillator readily available to deliver therapy, if needed. Defibrillator pads may need to be placed on the patient prior to procedure, as placing them during an emergency may compromise the sterile field (anterior-posterior placement of pads is preferred, as well as a distance of at least 8 cm from CIED). Alternatively, if VT or VF was detected on the monitor and a magnet was used to deactivate therapy, just removing it from ICD would make it fully functional and defibrillation will be delivered, if needed.
Monopolar electrosurgery use is the most likely cause of EMI with CIED. There are some techniques that should be used to diminish this interference. When placing a dispersion patch, it should direct current away from the CIED. For example, if the surgical site is on the left arm, the patch should be placed on the same arm, as opposed to placing it on the right arm and directing current, via tissue, that has CIED. Furthermore, limiting the duration of a single application to less than 5 seconds, with a few second pauses in between deliveries, would significantly decrease adverse interferences. 2 For example, if the patient is pacemaker dependent, even if short electrosurgery applications would lead to oversensing by pacemaker and inhibit its output, it would unlikely cause hemodynamic compromise. In view of recently published expert consensus statement for programming ICDs, to avoid unnecessary therapy, there is a delay between detection of tachycardia and therapy. 15 Hence, if electrosurgery application will be limited to less than 5 seconds at a time, it will unlikely lead to ICD therapy, as the device will declare this event as nonsustained.
Postoperative management
Once the surgery is complete, the patient is usually transported to a holding or recovery area. Patients should remain in an electrocardiography monitor at least until the magnet is removed from the CIED or reprogramming of the CIED is performed and the original, preprocedure, settings are programmed. Once this is accomplished, the length of further monitoring is decided on by the primary team. If reprogramming of the device was not done prior to procedure, most of the time it would be sufficient for the patient to be followed in the device clinic within a month. 2 Exceptions to this would be if abnormalities were noted on the monitor, it would suggest abnormal pacing or ICD function, hemodynamic compromise during surgery, cardiac arrest, emergent surgery, or an appointment cannot be arranged for the patient to visit device clinic within 1 month.
Conclusions
In conclusion, managing patients with CIEDs can be challenging, especially in emergent situations. When time is of essence, following protocol from Figure 3 may guide one during emergency noncardiac surgeries. If surgical cases are nonemergent and medical facility has electrophysiology team, it makes more sense to involve them. However, understanding concepts as described above affords better teamwork and collaboration. Dividing evaluation into preprocedure, intraprocedure, and postprocedure steps gives the opportunity to systematically approach these patients and avoid mistakes. Most of the evidence, as to interaction between CIEDs and electrosurgery, is based on case reports and information provided by engineers from device companies. Although it is not optimal or as strong as it used to be in other cardiology fields, it is the best available at this time. Nevertheless, extensive personal experiences in electrophysiology community lead to creating common sense recommendations that prepared patients with CIEDs to go safely through surgeries. As future technologies are knocking on our doors, we have to be ready to welcome them without compromising patient’s safety. As new technology develops and new devices are coming to the market (eg, leadless pacemakers), more prospective and randomized studies are necessary to assure patients safety.
Footnotes
Peer review:
Eight peer reviewers contributed to the peer review report. Reviewers’ reports totaled 2098 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have contributed equally to the article.