
Abstract
Elevated preoperative distress is associated with adverse perioperative outcomes. This study examined how (1) patient, surgical, and anesthetic-related factors, and (2) physiological indicators of cardiovascular risk are associated with preoperative distress within a mixed non-cardiac surgery cross-sectional sample. We analyzed data from the VISION cohort–Mental Health Supplement (N = 997). The Kessler-6 item Psychological Distress scale assessed preoperative distress, and medical personnel assessed patient physiological and surgical factors. Independent samples t-tests and ANOVAs examined differences in distress across patient, surgical, and anesthetic factors. Bivariate correlations examined relationships between distress and physiological variables. Multivariable linear regressions examined associations between distress and (1) sample and surgery characteristics, and (2) physiological variables. After adjustments, female sex (b = 0.53), Indigenous ethnicity (b = 0.92), higher BMI (b = 0.03), orthopedic surgery (b = 2.25), and preoperative troponin (b = 1.46) were associated with elevated preoperative distress. Preoperative distress has associations with various perioperative factors and enhanced understanding may contribute to risk mitigation.
Keywords
Introduction
Surgery is a source of both psychological and physiological stress on the body that can result in adverse perioperative outcomes. Each year, more than 10 million non-cardiac surgery patients worldwide experience major cardiac complications, such as myocardial injury, within 30 days of surgery (Botto et al., 2014; Devereaux and Sessler, 2015; Kristensen et al., 2014). Indeed, major cardiac complications account for at least a third of perioperative deaths (Beattie et al., 2012; Botto et al., 2014; Devereaux and Sessler, 2015; Greenstein et al., 2007; Kazaure et al., 2012; McFalls et al., 2008; Rodseth et al., 2014). As such, to reduce perioperative complications, it is important to identify and mitigate factors that contribute to these adverse sequelae.
The effect of stress on the body is commonly referred to as the “fight, flight, or freeze” response, which often coincides with the subjective experience of psychological distress (Kessler et al., 2002). This response activates neurohormonal changes that serve to increase blood pressure, muscle blood flow, glycogenolysis, mental alertness, and decrease perfusion to the genitourinary systems (Kam et al., 2016). This sequence of changes alters pathophysiological inflammatory, hemostatic, metabolic, and hemodynamic factors implicated in surgical outcomes (Brotman et al., 2007). If triggered when facing an acute physiological or environmental stressor, to obtain allostasis, this response is often considered adaptive. Conversely, the “fight, flight, or freeze” response can be maladaptive if triggered frequently and/or if an individual fails to properly adapt to such stress/stressors (Brotman et al., 2007). In fact, research has demonstrated that, like chronic stress, acute stress can have deleterious effects on cardiovascular functioning (Brotman et al., 2007; Hamer et al., 2008; Kivimäki and Steptoe, 2018; Vaccarino et al., 2021).
Surgery represents an acute physical stressor, which is also commonly accompanied by some level of psychological distress (including anticipatory distress while awaiting surgery). Between 80% and 93% of surgical patients tend to report at least some degree of preoperative psychological distress (Aust et al., 2018; Mavridou et al., 2013; Mitchell, 2010; Zemła et al., 2019). However, estimates of clinically elevated levels of distress before surgery tend to range between 35% and 45% (Aust et al., 2018; Holland and Bultz, 2007; Mejdahl et al., 2015), which is notably higher than estimates among the general Canadian population of 1%–21% (Caron and Liu, 2010; Simpson et al., 2012; St-Pierre et al., 2019). Importantly, research has shown that preoperative psychological distress is associated with various adverse health-related outcomes including increased postoperative pain (e.g. mean difference: 0.74) and analgesic consumption, greater likelihood of perioperative complications (e.g. infection; AOR = 1.12, 1.7–2.3-fold increase), increased length of postoperative stay (e.g. b = 0.01, R2 = 0.15, f2 = 0.18), odds of rehospitalization (e.g. AOR = 1.07), and even mortality (e.g. AOR = 1.09) (Brotman et al., 2007; El-Gabalawy et al., 2025; Gil et al., 2018; Ip et al., 2009; Sorel et al., 2019). These relationships are often thought to be influenced by biological (e.g. stress-mediated physiological changes; Brotman et al., 2007; McEwen, 1998) and/or behavioral (e.g. engagement in unhealthy behaviors, poor adherence to medical recommendations; Allison et al., 1999; Burra et al., 2011; McEwen, 1998) mechanisms. However, mechanistic research on the relationship between preoperative distress and perioperative outcomes is limited, particularly for biological hypotheses. In order to shed light on potential mechanisms, it is important to understand the physiological correlates of distress in real time on the day of surgery, particularly physiological indicators of cardiovascular risk. Further, it is critical to understand which groups may be most impacted by distress for risk mitigation and for further mechanistic exploration. Finally, existing research largely lacks differentiation between chronic and acute distress within the perioperative literature. This distinction is important for understanding appropriate means of intervention for coping with or reducing distress.
With these limitations of previous research in mind, the aim of this study was to examine the relationship between preoperative psychological distress and patient variables, including those relating to cardiovascular risk. The specific aims were to: (1) assess the relationship between patient-specific and perioperative factors including sociodemographics, type of surgery, type of anesthetic, and comorbidities (e.g. obesity, diabetes mellitus), and preoperative distress and (2) examine the associations between preoperative physiologic variables (e.g. hemoglobin, creatinine, glucose, blood pressure, heart rate, troponin) relevant to perioperative cardiovascular risk assessment, and preoperative distress. This study will attempt to better approximate the role of acute distress in these relationships through controlling for chronic distress in the form of existing mental health conditions.
Methods
Data
We analyzed data from the Vascular Events in Non-cardiac Surgery Patients Cohort Evaluation (VISION) Study – Mental Health Supplement. The VISION Study is an international prospective cohort study of non-cardiac surgery patients evaluating major complications after non-cardiac surgery (clinicaltrials.gov #NCT00512109). Research ethics boards at each participating site provided ethical approval and participants provided informed consent. Eligibility criteria included those ages 45 years and older, who were scheduled to undergo an elective, urgent, or emergency non-cardiac surgery under general or regional anesthesia. Those who did not require an overnight stay, were previously enrolled in the VISION study, or declined consent were excluded from participating. The VISION Mental Health Supplement included a cross-sectional subsample of 997 participants from a large tertiary care hospital (Health Sciences Centre) in Winnipeg, Manitoba, Canada. Between June 2011 and November 2012, trained research personnel administered supplemental mental health measures to participants on the day of surgery, approximately 1 hour before induction. These data were linked to the larger VISION database.
Measures
Mental health
Kessler’s 6-item Psychological Distress Scale (K6; Kessler et al., 2002) assessed preoperative distress (i.e. psychological distress during the period of awaiting surgery). The K6 is a reliable and well-validated 6-item screen for the severity of past-month distress. Items (e.g. during that past 30 days, about how often did you feel nervous?”) are rated on a scale from 0 [all of the time] to 4 [none of the time]. Items are reverse-scored and summed to derive a total score ranging from 0 to 24, where a score of 5–12 is indicative of moderate distress and a score of 13 or greater is indicative of severe distress (Prochaska et al., 2012). Clinically significant distress was defined as a score of ⩾5, which has been shown as an appropriate cut-point for identifying moderate distress that nonetheless warrants mental health intervention (Prochaska et al., 2012). Participants also self-reported whether they have a physician-diagnosed mood (i.e. depression, bipolar, mania, dysthymia, other) or a anxiety-related disorder (i.e. phobia, panic disorder, obsessive-compulsive disorder, posttraumatic stress disorder, other).
Sociodemographics
We assessed age continuously and categorized sex (i.e. male, female) and ethnicity (White, Canadian Indigenous peoples, other) based on prevalent groups.
Health status
Body mass index (BMI) was calculated using self-reported height and weight and was assessed continuously. Study personnel abstracted data from patients’ charts and interviewed participants to determine their history of medical comorbidities (i.e. coronary artery disease, congestive heart failure, cerebrovascular disease, diabetes mellitus, metastatic cancer, active cancer, hypertension, obstructive sleep apnea), whether they ever required dialysis, current impairment in functional status, history of tobacco use, and whether/when they stopped using tobacco before surgery. Investigators reviewed all clinical data to ensure accuracy.
Surgery characteristics
We categorized type of surgery according to surgical specialty: vascular (i.e. aorta reconstruction, aorto-iliac reconstruction, peripheral vascular reconstruction without aortic cross-clamping, extracranial cerebrovascular surgery, endovascular aneurysm repair), general (i.e. complex visceral resection, partial or total colectomy or stomach surgery, other intra-abdominal surgery, major head and neck resection for non-thyroid tumor), thoracic (i.e. pneumonectomy, lobectomy, other), major urogynecology (i.e. visceral resection, cytoreductive, hysterectomy, radical hysterectomy, radical prostatectomy, transurethral prostatectomy), major orthopedic (i.e. major hip or pelvic, internal fixation of femur, knee arthroplasty, above knee amputation, lower leg amputation), major neurosurgery (i.e. craniotomy, major spine), and low risk surgery. Those receiving surgery for cancer were also identified. Each anesthetic type was assessed dichotomously (i.e. yes vs no): general, spinal, epidural, nitrous oxide, nerve block.
Physiological variability
Study personnel collected data on patients’ preoperative hemoglobin, creatinine, glucose, blood pressure, heart rate, and troponin levels.
Analytic strategy
Independent samples t-tests and analyses of variance (ANOVAs) examined whether there were significant differences in preoperative distress according to patient-specific (i.e. sociodemographic, health status) and surgery-related characteristics (i.e. surgery type, anesthetic type). Bivariate correlations examined associations between preoperative distress and patient-specific continuous variables (i.e. age, BMI) and physiological variables. Multivariable linear regressions examined associations between patient-specific (reference for sex = male; reference for ethnicity = White) and surgery-related (reference for type of surgery = other; reference for type of anesthetic = no) characteristics and preoperative distress. A second set of multivariable linear regressions examined associations between preoperative distress and physiological variability. For all regressions, we conducted an unadjusted model (i.e. Model 1), a second model adjusted for sociodemographics (i.e. age, sex, ethnicity; Model 2), and a third model additionally adjusting for mental health conditions (i.e. any mood disorder, any anxiety-related disorder; Model 3). Upon examining the association between distress and physiological variability, Model 3 also adjusted for use of medications that alter the physiological variable of interest (e.g. diabetic medications, nitrates, angiotensin converting enzyme inhibitor/angiotensin II receptor blockers, beta-blocker, rate control calcium channel blocker, alpha 2 agonists). Statistical analyses were conducted using SPSS (version 24; IBM Corp, 2017) and STATA (version 14; Stata Corp, 2015) statistical software.
Results
With the exception of troponin, less than 6.0% of data for primary variables were missing, and case-deletion was employed (Schafer, 1999). With respect to troponin, only 48.4% (n = 483) had a preoperative troponin measurement and were included in analyses. Preoperative troponin was only assessed for a portion of the sample that consented to participate in a biobank sub-study. Those who had their preoperative troponin assessed were more commonly male (59.6% vs 46.9%, χ2 = 16.23, p < 0.001) and were older (M = 66.11 vs 62.51, t = 5.69, p < 0.001) compared to those who did not. There were no differences in ethnicity (χ2 = 1.53, p = 0.465) or preoperative distress (t = 0.71, p = 0.480) between groups.
Sample characteristics
The sample consisted of 997 non-cardiac surgery patients. There were similar proportions of males (53.1%) and females (46.9%), and participants were predominantly White (83.6%), with an average age of 64 years (SD = 10.15, range: 45–90), and a mean BMI of 29 (SD = 6.50, range: 13–58). Hypertension (50.9%), active cancer (38.9%), diabetes mellitus (20.4%), and coronary artery disease (15.8%) were the most common medical comorbidities, and 65.1% of participants reported a history of tobacco use. Cancer surgery (39.9%) and thoracic surgery (27.5%) were the most common types of operations performed, and participants primarily underwent general anesthesia (93.5%). The mean psychological distress score was 3.58 (SD = 2.92), with 24.1% reporting clinically significant (i.e. ⩾5) distress. See Table 1 for additional sample characteristics.
Sample characteristics and levels of preoperative distress.
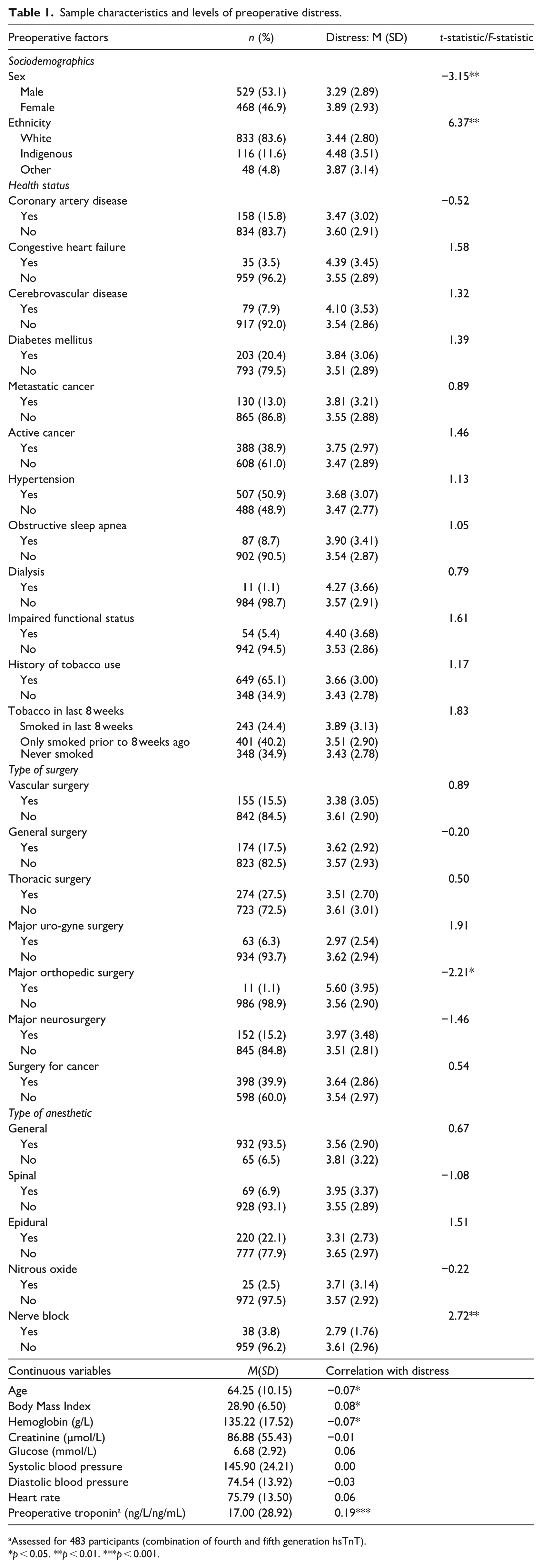
Assessed for 483 participants (combination of fourth and fifth generation hsTnT).
p < 0.05. **p < 0.01. ***p < 0.001.
Associations with psychological distress
Results of independent samples t-tests and ANOVAs revealed that mean distress scores significantly differed according to sex (t = −3.15, p < 0.01; female > male), ethnicity (F = 6.37, p < 0.01; Indigenous > other > White), whether the participant had orthopedic surgery (t = −2.21, p < 0.05; yes > no), and nerve block anesthetic (t = 2.72, p < 0.01; no > yes). Pearson bivariate correlations demonstrated significant associations between psychological distress and age (r = −0.07, p < 0.05), BMI (r = 0.08, p < 0.05), hemoglobin (r = −0.07, p < 0.05), and troponin (r = 0.19, p < 0.001; see Table 1).
Results of the first set of linear regressions examining patient and surgery-related characteristics are shown in Table 2. In the most stringent model (i.e. controlling for age, sex, ethnicity, any mood disorder, any anxiety-related disorder) female sex (reference = male; p < 0.01), Indigenous ethnicity (reference = White; p < 0.01), BMI (p < 0.05), and orthopedic surgery (reference = other surgery; p < 0.05) were significantly associated with increased preoperative psychological distress. In addition, active cancer was marginally associated with increased preoperative psychological distress (reference = no active cancer; p = 0.05) in the most stringent model only.
Associations between sample and surgery characteristics and preoperative distress.

Note. Values represent unstandardized regression coefficients and 95% confidence intervals; Model 1: unadjusted; Model 2: adjusted for sociodemographics (i.e. age, sex, ethnicity); Model 3: adjusted for sociodemographics and mental health conditions (i.e. any mood disorder, any anxiety disorder); aR2: adjusted R2.
For physical health conditions, reference = no.
Reference = other type of surgery.
Reference = no.
p = 0.05, *p < 0.05, **p < 0.01, ***p < 0.001.
Within the second set of linear regressions (examining physiological variability), results of the most stringent model (i.e. controlling for age, sex, ethnicity, any mood disorder, any anxiety-related disorder, medications that influence physiological variability) revealed that preoperative psychological distress was associated with increased preoperative troponin (p = 0.001; see Table 3).
Associations between preoperative distress and physiological variability.
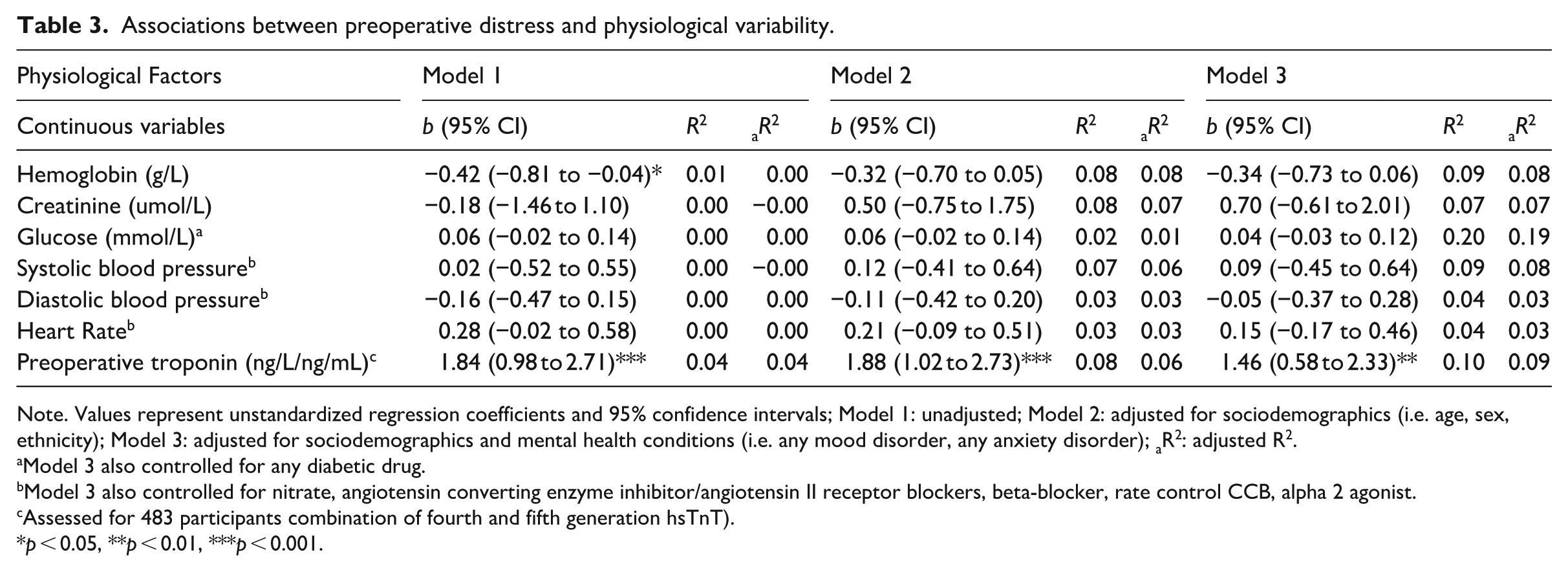
Note. Values represent unstandardized regression coefficients and 95% confidence intervals; Model 1: unadjusted; Model 2: adjusted for sociodemographics (i.e. age, sex, ethnicity); Model 3: adjusted for sociodemographics and mental health conditions (i.e. any mood disorder, any anxiety disorder); aR2: adjusted R2.
Model 3 also controlled for any diabetic drug.
Model 3 also controlled for nitrate, angiotensin converting enzyme inhibitor/angiotensin II receptor blockers, beta-blocker, rate control CCB, alpha 2 agonist.
Assessed for 483 participants combination of fourth and fifth generation hsTnT).
p < 0.05, **p < 0.01, ***p < 0.001.
A post-hoc regression examined all variables significantly associated with psychological distress within a single model (i.e. sex, ethnicity, BMI, orthopedic surgery, active cancer, troponin), while controlling for age, any mood disorder, and any anxiety-related disorder. Results revealed that Indigenous ethnicity (reference = White; b = 1.02, 95% CI [0.10–1.93], p < 0.05), BMI (b = 0.04, 95% CI [0.00–0.09], p < 0.05), and troponin (b = 0.02, 95% CI [0.01–0.03], p < 0.01) were significantly associated with increased preoperative psychological distress. Female sex, orthopedic surgery, and active cancer were no longer associated with preoperative psychological distress.
Discussion
To our knowledge, this is the first study to examine indicators of physiological variability alongside patient and surgery characteristics that are associated with acute preoperative psychological distress. Strengths of this study include its large and diverse surgical sample. Results highlight two patient characteristics (i.e. Indigenous ethnicity and BMI) and one physiological factor (i.e. preoperative troponin, a biomarker used to detect cardiac injury) that were consistently associated with increased preoperative distress across our statistical models. These results may inform screening and intervention strategies to reduce preoperative distress and mitigate clinically relevant adverse cardiovascular outcomes.
With respect to sociodemographic factors, female sex and Indigenous ethnicity were associated with increased preoperative distress after adjusting for other sociodemographic factors and mental health conditions. A large body of research, including studies with surgical samples, has identified a sex difference in psychological distress; with females consistently demonstrating increased distress compared to males (Bougie et al., 2016; Caron and Liu, 2010; Kindler et al., 2000; Lacey et al., 2014; Masood et al., 2016; Matud et al., 2015; Mitchell, 2012). This is also in line with more general sex differences across the majority of anxiety and depressive disorders (Altemus et al., 2014), with females at elevated risk. Researchers have hypothesized that sex differences in coping styles (Chandler et al., 2007) and neuroendocrinology (Altemus et al., 2014) may be implicated in these findings. Interestingly however, results of the post-hoc analysis demonstrated that female sex was no longer associated with psychological distress once it was included in the same model as other correlates of distress. This suggests that the initial association between female sex and distress may be better accounted for by other factors, such as ethnicity. In fact, a slightly larger proportion of females were Indigenous compared to males, which may support this possibility.
Indigenous ethnicity was also associated with higher levels of preoperative distress and this association remained significant in the post-hoc model. This finding is noteworthy, given the lack of research examining Indigenous peoples’ mental health in a surgical context. This is consistent with extant literature highlighting mental (and physical) health disparities between those who are Indigenous and those who are not, with poorer health, including increased distress, elevated prevalence of mental health and physical health conditions, alongside lower life expectancy, evident among Indigenous populations (Canadian Indigenous: Caron and Liu, 2010; Martin et al., 2018; Nelson and Wilson, 2017; North American Indigenous and New Zealand Maori: King et al., 2009; Australian Indigenous: McNamara et al., 2018). Thus, the present finding of elevated preoperative distress among Indigenous study participants is unsurprising. This may partially pertain to pre-existing elevated generalized distress in this subgroup and/or surgery-specific distress related to poorer preoperative health status and subsequent risks associated with undergoing surgery or poorer prognosis. Some researchers have suggested that this disparity is driven by greater physical morbidity and disability among those who are Indigenous (McNamara et al., 2018), while others have pointed to the negative health consequences of marginalization, racism, colonialism, and intergenerational trauma (King et al., 2009: 2; Nelson and Wilson, 2017). Any of these factors could contribute to increased distress before surgery, whether distress specific to an individual’s health status and surgical risk or distress associated with navigating a health system where prejudices and racism toward Indigenous populations still exist (Cooke and Shields, 2024). Future research should explore these possibilities using culturally appropriate methods. Recent research has also underscored the barriers limiting Indigenous peoples’ access to surgery in Canada, which could contribute to heightened distress (McVicar et al., 2021). Importantly, these contributing factors are also interconnected, further amplifying distress within this population. Researchers have highlighted the importance of developing, evaluating, and implementing anti-racism interventions within healthcare settings (Hassen et al., 2021), which may help mitigate some of these health disparities, including distress.
Active cancer was marginally associated with increased preoperative distress after adjusting for sociodemographics and mental health conditions, though surprisingly, the bivariate association was non-significant. There is considerable research establishing the relationship between cancer and distress (Sun et al., 2022; Zabora et al., 2001), such that the National Comprehensive Cancer Network considers distress as the “sixth vital sign” (Holland and Bultz, 2007) and recommends distress screening as part of routine oncological care. Orthopedic surgery was also associated with distress, within the same adjustment model. Within this sample, orthopedic surgeries were primarily complex trauma. The nature of the circumstances contributing to the need to undergo trauma-related surgery are often in and of themselves psychologically distressing (Vincent et al., 2015). In addition, patients undergoing orthopedic trauma and/or who have active cancer share similar potentially life-altering diagnoses, which may account for a proportion of the elevated distress found in these groups. This is further accompanied by additional burden due to potential temporary or permanent loss of employment, functional impairment, and associated loss of independence, all of which may amplify distress (Kitano et al., 2021; Zhang et al., 2020). However, neither active cancer nor orthopedic surgery remained significant in the post-hoc model, suggesting there are other factors that account for more significant variability in distress levels before surgery.
Results also revealed a significant positive association between BMI and preoperative distress, which also maintained significance in the post-hoc model. Prior research has demonstrated a curvilinear association between BMI and distress, where relatively low and high BMIs (i.e. underweight and obese) were associated with the highest levels of psychological distress (Martínez et al., 2014; Sutin et al., 2021). This is partially in line with the results from the current study, suggesting a relationship between high BMI and increased distress. Other studies have only found that higher BMIs were associated with preoperative distress (Brandheim et al., 2013; Liu et al., 2018), consistent with the current study, though these studies did not specifically test for curvilinear relationships. Prior research examining the relationship between obesity and depression has considered the roles of biological (e.g. inflammation), behavioral (e.g. unhealthy eating habits as a form of coping), and psychosocial (e.g. low self-esteem, stigma/discrimination) mechanisms (Luppino et al., 2010), which may help elucidate the emergent association.
Finally, results also identified a significant association between higher levels of preoperative troponin and elevated preoperative distress. This relationship remained significant in the post-hoc model. This finding aligns with prior research identifying a link between elevations in cardiac biomarkers and mental health conditions (e.g. generalized anxiety disorder, major depressive disorder, posttraumatic stress disorder; Bankier et al., 2008, 2009; Xue et al., 2012), although future research is needed to clarify these relationships. Research has also identified dose-response relationships between psychological distress and adverse cardiovascular events and ischemic heart disease (Jackson et al., 2018; Welsh et al., 2017), and elevated troponin is often found in those experiencing adverse cardiovascular events (Bergmark et al., 2022; Vafaie, 2016). The relationship between distress and cardiovascular functioning is complex. While some researchers suggest that distress is more likely a consequence or confounding correlate of cardiovascular complications (Welsh et al., 2017), others consider distress as a causal risk factor for cardiovascular events (Jackson et al., 2018). Further, research examining takotsubo syndrome, also known as stress-induced cardiomyopathy, considers stress as a direct trigger of cardiovascular symptoms (Borodzicz et al., 2019; Brotman et al., 2007; Lagan et al., 2015; Madias, 2013), including elevations in troponin (Lagan et al., 2015; Lyon et al., 2021). Panic attacks may be implicated in this relationship (Madias, 2013), which are known to impact sympathetic nervous system functioning (triggering cardiovascular symptoms) as part of the fight-flight-freeze response (Esler, 2022).
Implications
Taken together, results have noteworthy implications for perioperative care practices. The association between preoperative distress and troponin is novel, and warrants additional investigation, but importantly, it highlights potential health implications of monitoring distress perioperatively to enable intervention. Prior research examining data from the larger VISION trial revealed that elevated postoperative troponin was a risk factor for 30-day postoperative mortality (Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators et al., 2012). Further, other research has shown that mental health conditions in general, and posttraumatic stress disorder in particular, are associated with elevated cardiac biomarkers and subsequent increased mortality, in a non-perioperative context (Xue et al., 2012). Taken together with the current results, preoperative distress (which may be more commonly elevated in those with underlying mental health conditions) may potentially be a modifiable marker for adverse perioperative health outcomes. Additional research is warranted to examine this more comprehensively and elucidate possible mechanisms.
Though these results need replication, they offer promising evidence that screening for preoperative distress may be associated with physiological indicators of cardiovascular risk. Screening for preoperative distress can be a fast, easily scalable, and inexpensive tool to identify patients at risk for negative cardiovascular outcomes, compared to biomarker testing, which typically involves intensive resources (e.g. specialized equipment, lab processing, trained personnel to interpret results). Future research should examine the effects of allocating evidence-based preoperative interventions to those identified as at-risk to determine if this reduces risk of poor cardiovascular outcomes.
Results of the current study also highlight certain subgroups who may more commonly present with elevated distress, including those who are Indigenous and those with elevated BMIs, alongside potentially those who are female, those with active cancer, and those undergoing orthopedic surgery. Preoperative screening for psychological distress would identify at-risk patients who may benefit from closer perioperative monitoring and/or psychological intervention to mitigate adverse outcomes. Results also support the importance of identifying culturally suitable practices for distress monitoring and intervention in a perioperative setting.
Limitations
Despite the strengths of this study including the use of a large surgical sample, the assessment of indicators of physiological variability, and the inclusion of preoperative distress assessment using a widely validated screening tool, alongside the identified noteworthy implications, this research is not without limitations. First, this study was cross-sectional and therefore causal (and in some cases temporal) assumptions cannot be made. Second, preoperative mental health (psychological distress and mental health conditions) was assessed using self-report, and although psychological distress was evaluated using an empirically validated measure (K6), this may still result in some biased responses (e.g. under-reporting/social desirability or over-reporting, recall bias). Relatedly, although the inclusion of a measure assessing state-level (i.e. situational) distress on the day of surgery is a strength in understanding correlates of relatively acute preoperative distress, the K6 measure in particular assesses distress in the past 30-days. The inclusion of a present-moment assessment of distress would be more temporally relevant in understanding acute preoperative physiological indicators and their relation to distress. Third, participants were derived from a convenience sample, which may also be associated with biased results (e.g. distressed patients may be less likely to participate in the additional mental health component). Fourth, some variables examined had small cell sizes (e.g. dialysis, orthopedic surgery), thus reducing statistical power. Other variables had unequal group sizes. Although this may be typical of certain surgical characteristics within this population (e.g. anesthetic type), it may have reduced the accuracy of statistical estimates with these groups. These results should be interpreted with caution. Fifth, given the novel and exploratory nature of this study, we examined a large number of potential correlates of preoperative distress, which may have increased the chance of type I error. Additionally, the results were collected from a single site in Canada, limiting generalizability of findings. Finally, although we were able to examine the relationship between sex and preoperative distress, gender was not assessed within the current study. It would be informative for future research to assess gender differences in preoperative distress.
Conclusion
Our study highlights the unique relationships between patient factors (such as Indigenous ethnicity and high BMI) and preoperative psychological distress. In addition, this study suggests that psychological distress may be linked to elevated troponin levels before surgery. Together, these factors may assist in early identification of subpopulations with increased risk for adverse perioperative outcomes. Future research should attempt to understand the mechanisms implicated in relationships between preoperative distress and patient, surgical, physiological, and other health correlates.
Footnotes
Acknowledgements
The authors acknowledge the VISION research group for their contributions.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by Health Research Ethics Board, University of Manitoba (approval No. # clinicaltrials.gov #NCT00512109).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Participants were informed, through the consent form, that the anonymized findings would be submitted for publication.
Author contributions
Jordana L. Sommer: Methodology, data analysis and interpretation, writing original draft and editing ; Karen Mac Donald: Conceptualization, writing and editing; Jitender Sareen: Conceptualization, methodology, reviewing draft and editing; Corey S. Mackenzie: Conceptualization, reviewing draft and editing; PJ Devereaux: Conceptualization, methodology, data collection, reviewing draft and editing; Sadeesh Srinathan: Conceptualization, methodology, data collection, reviewing draft and editing; Renée El-Gabalawy: Conceptualization, methodology, data collection, reviewing draft and editing, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by University of Manitoba Start-Up Funds (El-Gabalawy).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data from the VISION study may be available upon request to PJ Devereaux