
Abstract
Background:
De Quervain’s tenosynovitis (DQT) is a growing ergonomic health issue among mobile phone users. It affects students’ thumbs and wrists, limiting their thumb movement and reducing work productivity. However, there is limited epidemiological data among students. Therefore, this systematic review and meta-analysis aimed to find the pooled prevalence of DQT among students in Pakistan.
Methods:
A careful search of cross-sectional studies that showed the prevalence of DQT among students in Pakistan was conducted. Studies found in PubMed, Semantic Scholar, HINARI, ScienceDirect, and Google Scholar were searched up to December 25, 2025. The recommended PRISMA 2020 guidelines were used for reporting items. Data were extracted using Excel 16 and analysed by STATA V17. The quality of the included studies was assessed by the JBI quality assessment tool. The random effect model was applied to find the pooled prevalence of DQT. Publication bias was evaluated by Egger’s regression test and the Begg’s funnel plot.
Results:
This systematic review and meta-analysis included a total of 14 studies with a sample size of 3,277. The pooled prevalence of DQT was found to be 46.33% (95% CI: 35.38, 57.28; I2 = 97.56%, P = .001). The subgroup analysis found that DQT varies highly among the included studies. High prevalence with significant heterogeneity was found in both university and college students. Leave-one-out sensitivity analysis indicates the consistency of the pooled finding.
Conclusions:
This systematic review and meta-analysis found a high prevalence of DQT among students in Pakistan. Therefore, early identification and preventive measures are recommended. These may include ergonomic education and digital health awareness campaigns focusing on the risks of mobile phone–related repetitive thumb and wrist movements, applying hand and wrist stretching exercises, and encouraging regular breaks.
Plain Language Summary
De Quervain’s tenosynovitis (DQT) is a prevalent musculoskeletal disorder among students. It affects their wrists, restricts thumb mobility, and diminishes productivity and work quality. However, there is limited epidemiological data among students. This study aimed to find the pooled prevalence of DQT among mobile phone-using students in Pakistan. A careful search of cross-sectional studies found in PubMed, Semantic Scholar, HINARI, ScienceDirect, and Google Scholar were searched up to December 25, 2025. The recommended PRISMA 2020 guidelines were used for reporting items. The study found that students are at high risk of DQT (46.33%). Therefore, early identification and preventive measures are required. This may include ergonomic education and digital health awareness campaigns, hand and wrist stretching exercises, and taking regular breaks.
Keywords
Contributions to the literature
De Quervain’s tenosynovitis (DQT) is an ergonomic health problem yet overlooked among students. This planned systematic review and meta-analysis estimate the pooled prevalence of DQT among students across different school levels in Pakistan. The result showed high prevalence of DQT. The findings give insight into emphasizing this overlooked ergonomic health problem. In addition, the findings inform the need for ergonomic preventive strategies in educational settings. It has notable implications for public health action by drawing attention to the ergonomic burden of DQT among mobile phone user students. Moreover, it can serve for the growing body of literature on ergonomics and the musculoskeletal health effect of DQT.
Background
De Quervain’s tenosynovitis (DQT) is a musculoskeletal disorder that affects the tendons on the thumb side of the wrist. It is a painful condition of the wrist caused by repetitive overuse of the wrist and hand. 1 It occurs when the sheath surrounding the tendons of the abductor pollicis longus and extensor pollicis brevis becomes inflamed.2,3
De Quervain’s tenosynovitis is a common yet often underrecognized ergonomic health issue. It causes pain and impairment of thumb function that affects daily activities and reduces work productivity and quality of life. 4 DQT was first described by Fritz De Quervain as a hand condition with inflammation and degeneration of the tendon sheath. 5 This ergonomic issue has different synonyms, such as De Quervain’s disease, gamers’ thumb, first dorsal compartment tenosynovitis, radial styloid tenosynovitis, texting tenosynovitis, and washer woman’s sprain.5 -7 It is more common among people who engage in repetitive hand and wrist movements, forceful gripping, and routine activities. Weightlifting, pinching, pulling, or pushing, and ergonomically stressful manual work are risk factors. 8 Occupational groups including students9 -12 and those in metallurgy, masonry, butchery, hairdressing, or waitressing, 13 volleyball players, and clinical physical therapists were more affected. 8 In addition, a high prevalence has been reported among individuals who work on a computer for a long time and athletes with high resistance training. 14 A study showed DQT affects women at a higher rate, 2.8 cases per 1000 person-years, compared with men at 0.6 per 1000 person-years, and Blacks are affected at 1.3 per 1000 person-years compared to whites at 0.8. 15 Females are more affected than men due to hormonal changes and fluid retention.16,17 Another study conducted among postpartum women elaborated that first pregnancy, first childbirth, length of pregnancy, and being female housewives are risk factors for DQT.17,18 The peak prevalence of DQT occurs from the ages of 40-59 years. 19 However, a study conducted among clinical physiotherapists was 25-35 years. 8
In Pakistan, the prevalence of DQT was 58.8% in the general population, 20 35% among cobblers, 21 and 71.6% 22 among weightlifters. Notably, this ergonomic health condition also affects students ranging from 13% to 78.3%.33,34 Literature shows that prolonged use of handheld devices, especially weighing around 100 g and needing continuous thumb musculature engagement, leads to DQT. 9 Individuals affected by DQT experience feelings of burning, tingling, numbness, and cramping around the thumb; thickening and myxoid degeneration of the tendon sheath; and difficulty moving the thumb and wrist. 23 It has been associations with rheumatoid arthritis. 24
The Finkelstein test is a widely used diagnostic test to identify the presence or absence of DQT. 25 A previous study demonstrated that the more frequent the usage of mobile phones, the higher the occurrence of DQT and the more positive the Finkelstein test result. 25
Students are more vulnerable to DQT. The accessibility and suitability of mobile phone technology link students with smartphone use for typing, texting, and playing video games that cause thumb overuse and increase the risk of DQT.9,20,26 Frequent usage and movement of the thumb from utilizing mobile phones or other electronic devices results in thumb load. This results in constriction-induced inflammation of the tendon sheath within the first dorsal compartment of the wrist. 27 When students hold their phones with 1 hand and type using only 1 thumb, they experience a non-neutral wrist posture. 28 Another study showed that nearly half of students typed with both thumbs and one-third typed with 1 thumb. 29 Spending 6-8 h/day on a smartphone, social media use, bilateral thumbs, bilateral horizontal-screen thumb gestures, and screen sizes were risk factors for DQT. 30
Although mobile phones enhance students’ lives through their diverse applications and features, the increased reliance on them has raised the risk of DQT. They are vulnerable due to prolonged screen time and gaming, repetitive typing, excessive texting, and academic demands. 31 In addition, the increasing burden of DQT among student populations has not received adequate attention in public health planning and ergonomic intervention strategies. Even though many studies have reported DQT among students in Pakistan, findings were varied in terms of prevalence, sample size, and school types. In addition, there is a limited pooled prevalence of DQT among students in Pakistan. This inconsistency in outcomes makes it difficult to draw common understanding and develop prevention or management strategies. Therefore, this systematic review and meta-analysis aimed to find the pooled prevalence of DQT among mobile phone-using students in Pakistan. The findings will be valuable for raising awareness and preventing DQT.
Methods
Reporting System and Registration
This systematic review and meta-analysis was aimed at finding the pooled prevalence of de Quervain tenosynovitis among mobile phone using students in Pakistan. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The review protocol was registered with PROSPERO (CRD420251040220).
Searches
A thorough search of cross-sectional studies was conducted on international databases, such as PubMed, Google Scholar, HINARI, Semantic Scholar, and Science Direct. Studies published from these databases up to December 2025 were included. The MeSH and search filters were included in the search strategies developed via the PMC Advanced Search Builder with keywords and Boolean operators: “De Quervain Disease” OR “De Quervain’s tenosynovitis” OR “De Quervain tenosynovitis” OR “De Quervain’s tendinopathy” OR “De Quervain syndrome” OR “stenosing tenosynovitis” OR “first dorsal compartment tenosynovitis” AND “mobile phone” OR “smartphone” OR “cell phone” OR “mobile device” OR “texting” OR “short message texting” OR “mobile usage” OR “handheld device” AND “student*” AND “prevalence” OR “epidemiology” OR “incidence” OR “burden” AND “Pakistan” (Supplemental file 1). In addition to the primary keywords, we employed synonyms, abbreviated symbols, and additional free-text keywords to enhance the search. Full-text articles published in English were incorporated in the review. The reference lists of reviewed papers were examined, and the “similar studies” were further identified for additional relevant studies. All included and excluded studies were screened using EndNote 20. The screening process began with an independent review of titles and abstracts, followed by a full-text screening of the selected studies by 3 authors. Any disagreements were resolved through consensus. The selection of studies was meticulously documented to enable the completion of a PRISMA 2020 flow diagram.
Inclusion Criteria
This systematic review and meta-analysis were framed by the CoCoPop mnemonic (Condition, Context, Population). Condition: prevalence of De Quervain’s tenosynovitis. Studies that diagnosed DQT using Finkelstein, or standardized questionnaires were included. Context: This review includes studies conducted in educational settings such as colleges, and universities in Pakistan. Population: This review included studies conducted among mobile phone using students. Studies examining the prevalence of de Quervain tenosynovitis among students were included.
Exclusion Criteria
Studies conducted among the general population were excluded if student-specific data were not found separately; studies among students outside Pakistan, preprints, unrelated research, and studies with poor methodological quality were excluded. Qualitative studies, editorial letters, and non-research materials were excluded from the meta-analysis.
Outcome Assessment
Estimating the pooled prevalence of de Quervain tenosynovitis in Pakistan was the primary objective of the study. Identifying potential sources of heterogeneity, evaluating publication bias, and performing sensitivity analysis were the second objectives of this study.
Quality Assessment and Data Extraction
After searching studies in the database, all articles were exported into EndNote 20, and then duplicate entries were removed. After the screening of relevant studies for eligibility by the 3 reviewers (AEB, KCA, and AK), the methodological quality of each study was evaluated by the Joanna Briggs Institute’s (JBI) critical appraisal checklist for studies reporting prevalence data. This checklist consists of 9 items that include whether the sample frame was appropriate to address the target population, whether the sample study participants were sampled in an appropriate way, and whether the sample size was adequate. It also evaluates whether the study subjects and the setting are described in detail and whether the sample and the data analysis are conducted with sufficient coverage of the identified sample. In addition, the checklist examines whether valid methods were used for the identification of the condition of interest and whether the condition was measured in a standard and reliable way. Moreover, the appropriateness of statistical analysis and the adequacy of the response rate were assessed. Each reviewer independently assessed the risk of bias for the studies. Then the risk of bias was classified as the sum of “yes” answers greater than 5 as low risk, 4 to 5 as medium risk and less than 4 as high risk. 32 Papers with low- to medium-risk quality scores were included in the quantitative analyses. To resolve any differences that arose during the quality assessment, the mean score from all reviewers was calculated. The remaining data were extracted using a standardized data extraction template. This form includes prevalence of DQT, sample size, sample size calculation or power analysis, study setting, school type, data collection tools, gender and age of participants, and daily phone use. Two authors (AEB and HW) were responsible for extracting data. Then 2 authors (AEB and AK) participated in cross-checking the extracted data.
Assessment of Publication Bias and Small Study Effects
To evaluate publication bias and the potential effect of small studies, we employed Begg’s funnel plots and Egger’s test. First, we visually examined the symmetry of the funnel plots. Second, we quantitatively assessed the likelihood of publication bias using Egger’s regression test.
Data Synthesis and Presentation
All analyses were conducted using Stata version 17. A random effect model along with corresponding 95% confidence intervals was applied to estimate the pooled prevalence of de Quervain tenosynovitis. This helps to account for substantial heterogeneity among the included studies. To harmonize the pooled prevalence of de Quervain tenosynovitis among the included studies, we ensure the measurement of the outcome with standard tools and procedures. Standard error adjustment for the overall effect size was conducted using the Šidák–Jonkman method and the Knapp–Hartung approach. This helps to get robust estimates of the pooled result. Heterogeneity among the included studies was assessed by the I2 statistic. I2 values below 50% show homogeneity and I2 of 50% or higher indicates the presence of high heterogeneity. We employ a 95% confidence interval (CI) and a P-value of less than .05 as statistically significant for the absence of publication bias and heterogeneity. Subgroup analyses were performed to investigate potential sources of heterogeneity. Additionally, sensitivity analyses were done to examine the validity and robustness of the summary measures. A leave-one-out analysis was performed by gradually eliminating each study to ensure that the overall findings were not unduly influenced by any single study.
Results
Searching Process
A total of 1950 articles were identified using electronic databases and manual searching. After excluding duplicate sources, a total of 1856 studies were retained, and based on their titles and abstracts, 1803 studies were excluded. In addition, 39 studies were excluded based on the exclusion criteria. Finally, a total of 14 studies were included in this review. The selection process is summarized below by the PRISMA flow diagram (Figure 1).
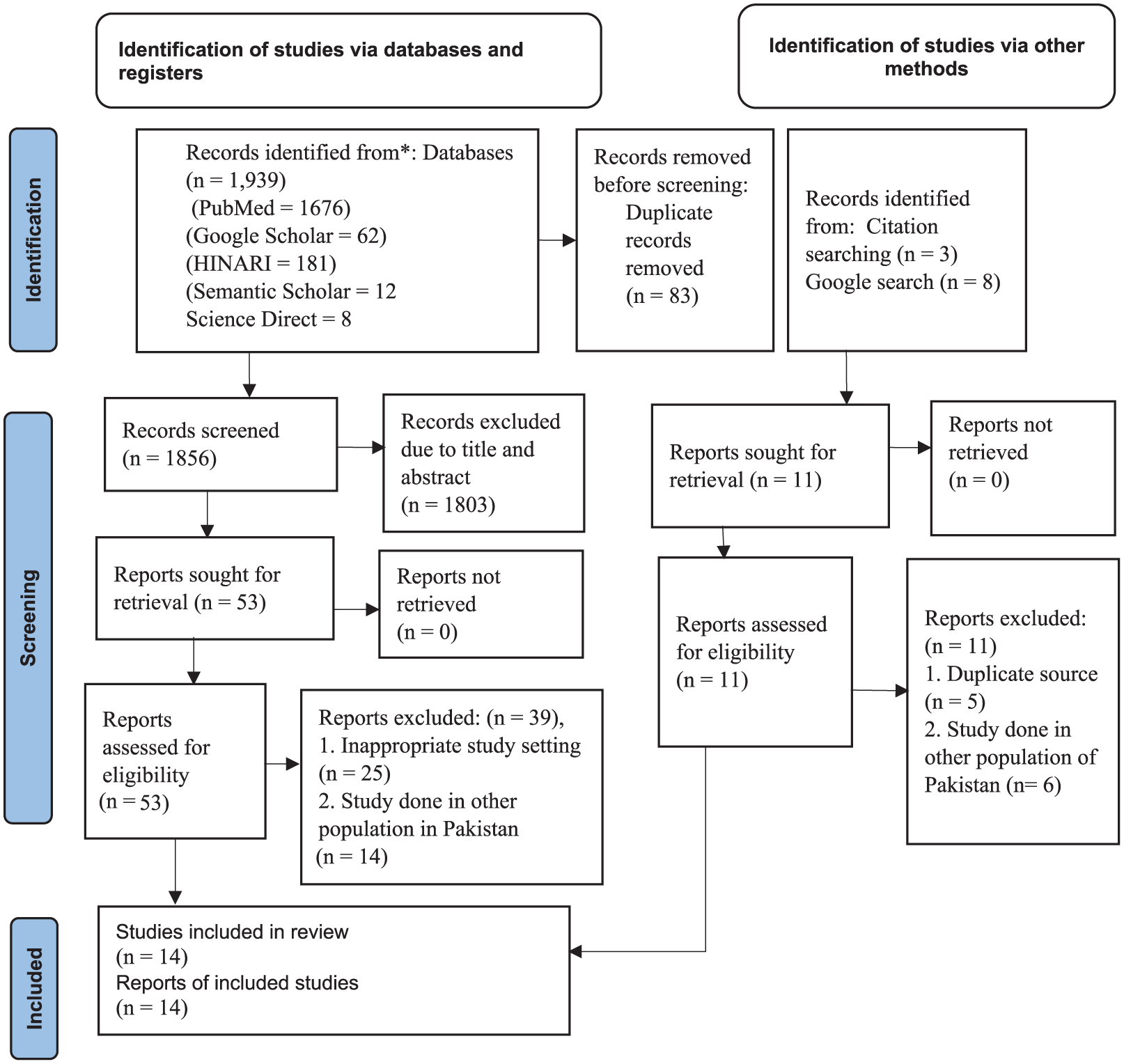
PRISMA flow diagram for the pooled prevalence of De Quervian tenosynovitis among students in Pakistan, 2025.
Characteristics of the Included Studies
A total of 14 studies conducted up to December 2025 were included. All the included studies were cross-sectional in design with 3,277 students, with sample sizes ranging from 80 to 384. The studies were published between 2014 and 2025 among college and university students. The higher prevalence of De Quervain’s tenosynovitis was found among undergraduate students of Gujranwala 33 and the lower prevalence was found among university students in Multan. 34 The included studies used Finkelstein’s test as the principal diagnostic tool and other pain or functional assessment instruments, such as the Patient-Rated Wrist/Hand Evaluation, Numeric Pain Rating Scale, Visual Analog Scale, and Smartphone Addiction Questionnaire. Studies used self-administered and structured interview-based questionnaires for data collection. Regarding sampling methods, many of the included studies used non-probability convenience sampling and other studies employed probability sampling (Table 1). In some studies, the majority of study participants were female students.12,33 From the included studies, the following findings were found. Increased use of smartphones increases DQT. 12 A significant association was found between writing and the Finkelstein test result 35 ; there was a correlation between frequent text messaging and thumb pain, 10 and game-playing hours increased DQT. 34 In addition, a significant association was found between mobile phone screen time and the severity of wrist pain 9 and female students were more affected by DQT than male students. 11 Despite methodological differences, the risk of bias was rated low and medium for all included studies (Supplemental file 2).
Characteristics of the Included Studies on the Prevalence of De Quervain’s Tenosynovitis Among Students in Pakistan, 2025.
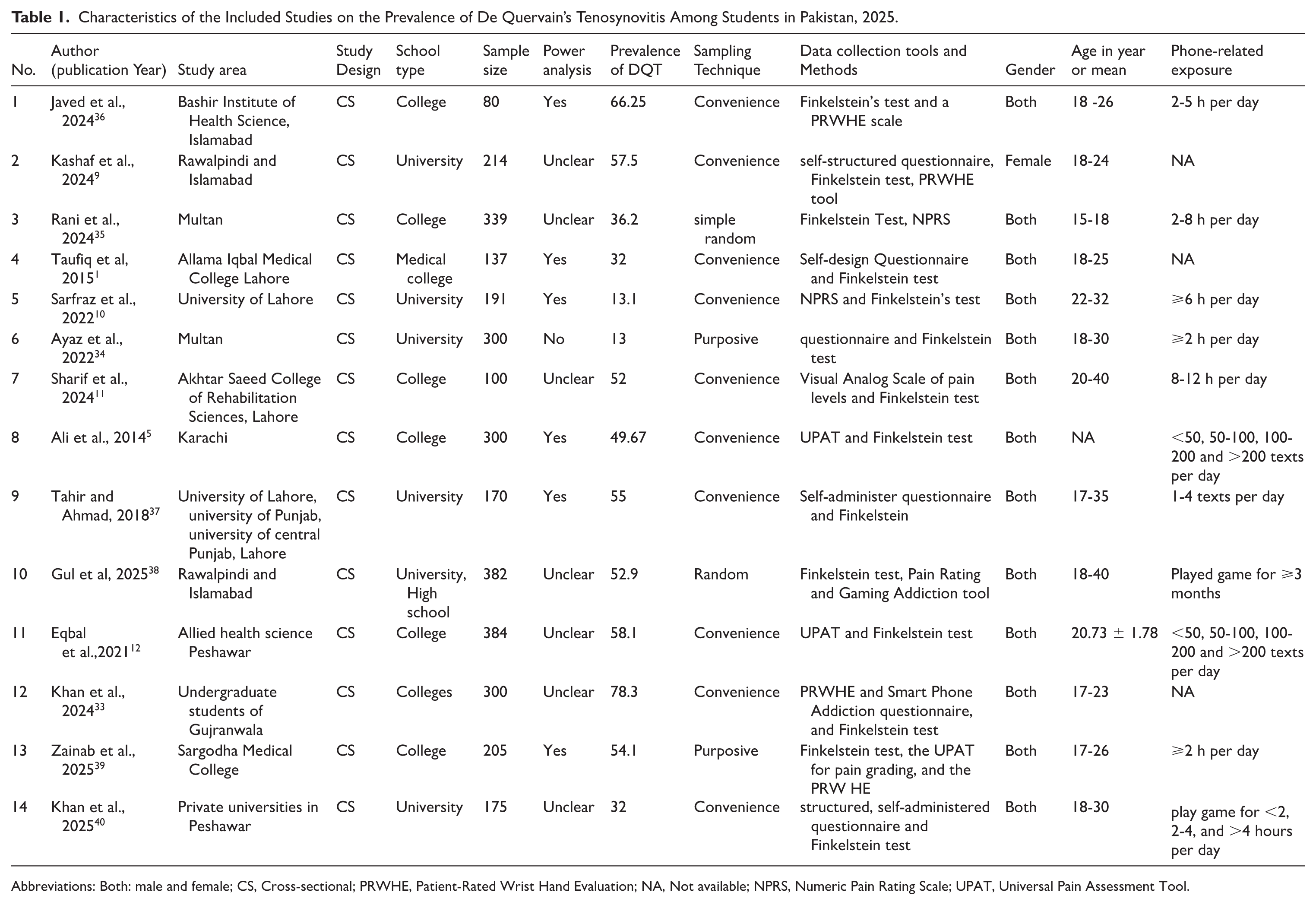
Abbreviations: Both: male and female; CS, Cross-sectional; PRWHE, Patient-Rated Wrist Hand Evaluation; NA, Not available; NPRS, Numeric Pain Rating Scale; UPAT, Universal Pain Assessment Tool.
Meta-Analysis
The Pooled Prevalence of De Quervain’s Tenosynovitis Among Students in Pakistan
The pooled prevalence of DQT was estimated by pooling fourteen studies.1,5,9 -12,33 -40 Then the pooled prevalence was found to be 46.33% (95% CI: 35.38, 57.28; I2 = 97.56%, P = .001) and the 95% prediction interval ranged from 4.3 to 88.4 (Figure 2 ).

Forest plot for the pooled prevalence of De Quervain tenosynovitis among students in Pakistan, 2025.
Heterogeneity and Subgroup Analysis
This meta-analysis found high heterogeneity among the included studies. To identify the possible source of heterogeneity, subgroup analysis was conducted based on school type. The finding showed that 53.32% (95% CI: 40.71, 65.93, P = .001, I2 = 95.49%) and 37.14% (95% CI: 15.25, 59.03, P = .001, I2 = 98.23) were among college and university students, respectively (Figure 3).

Subgroup analysis of the pooled prevalence of De Quervain’s tenosynovitis among students in Pakistan, 2025.
Publication Bias
We assessed the presence of a small study effect through a Begg’s funnel plot and Egger’s regression test at a P-value < .05. As a result, the funnel plot looks asymmetrical, and the Egger’s test was not statistically significant (Figure 4). This indicates no strong evidence of publication bias. However, this finding should be interpreted with caution. This could be the presence of high heterogeneity between studies and the limited power of the funnel plot, which showed asymmetry in the absence of publication bias.

Funnel plot for the pooled prevalence of de Quervain tenosynovitis among students in Pakistan, 2025.
Sensitivity Analysis
Sensitivity analysis was assessed by the leave-one-out analysis to evaluate the effect of each study on the overall pooled prevalence. Finally, the leave-one-out analysis indicates that despite some studies having an effect on the pooled effect size, the finding is robust and consistent, approximately between 43% and 48% (<10% prevalence change). This indicates no single study substantially influenced the pooled effect estimate (Figure 5).

Sensitivity analysis for pooled prevalence of De Quervain’s tenosynovitis among students in Pakistan, 2025.
Discussion
De Quervain’s tenosynovitis is an emerging ergonomic health problem that affects the productivity and quality of work.20 -22 Its presence affects thumb and wrist movement in grasping and pinching activities. This ergonomic health problem negatively affects students’ health. Therefore, this study aimed to find the pooled prevalence of DQT among students in Pakistan. As a result, the pooled prevalence was 46.33% (95% CI: 35.38-57.28, I2 = 97.56%) with high heterogeneity among the included studies. The high prevalence indicates a considerable ergonomic burden of DQT among the included studies in academic settings. This level of heterogeneity shows that DQT varies among the reviewed studies and has affected students to different extents. The possible reasons may include variations in age, text typing speed, academic level, field of study, and gender composition among the included studies.12,33,39 In addition, differences in exposure patterns, such as duration, frequency, and types of mobile phone and digital device use, may have a role in this heterogeneity. Students in the included studies have different daily screen times, texting frequencies per day, and gaming experiences.38,40 Moreover, this heterogeneity may be explained by differences in sampling techniques, study quality, and sample sizes. In this review, most studies used non-probability (convenience) sampling with small sample sizes, while others used probability sampling. Convenience sampling does not adequately represent the target population and may introduce sampling bias. In contrast, other studies used probability sampling that may yield representative estimates. 41 Pooling these studies together may increase between-study variability. Meta-epidemiological data show that studies with small sample sizes tend to show variability between studies and contribute to greater heterogeneity in meta-analyses. 42 Moreover, colleges and universities may differ in academic workload, ergonomic awareness, and access to mobile phone technology, digital devices, and the internet, which may contribute to this inconsistent result. 43
The pooled prevalence found in this review was higher than primary studies in Jeddah (19.1%) 44 and in India, 40% 45 of participants experienced DQT. The possible reasons may be prolonged screen time, repetitive texting, 5 playing games, 34 and excessive mobile phone use such as gripping, scrolling, and typing. 9 In addition, this could be due to a lack of awareness of healthy digital device use, the availability of smartphones, and the free accessibility of the internet. 46 Accessibility and adoption of smartphones require constant thumb abduction and ulnar deviation that strain the first dorsal compartment of the wrist, which leads to DQT. 47 Indeed, students often lack or overlook ergonomic interventions that make them more susceptible to musculoskeletal strain. 48 Moreover, this systematic review and meta-analysis includes mobile e-gamers 40 and medical students who used their wrists in repeated and sustained bending postures. 1 However, the pooled prevalence found in this review was lower than in a study conducted among the general population in Pakistan, 58.8%, 20 and in China, 52% of students tested positive for DQT. 30 This discrepancy may be due to sample size, tool and population differences, mobile device usage patterns, and ergonomic practices.
Subgroup analysis by school type showed no significant difference exists, but the heterogeneity was high in both college and university students. This indicates the widespread occurrence of DQT in both college and university. The possible reasons may include prolonged smartphone use, repetitive thumb movements, and predominant usage of the thumb while texting, which are risk factors for upper-extremity musculoskeletal disorders. 49 Prolonged writing and frequent usage of mobile phones for texting and other overuse conditions could contribute to an increase in DQT among students. In some studies, female students were more involved and may report higher prevalence due to gender-based differences in DQT risk.1,9,12,33 The type of mobile phone task, such as holding the phone versus texting, affected muscle activity and thumb positions. 50 Indeed, overuse of smartphones causes pain in the thumb and affects hand functions of students in educational settings. 51
Slightly lower heterogeneity was found among college students. Possible explanations include lifestyle and age-related differences that may affect the level of DQT. The type of mobile phone may cause this heterogeneity. Students used cell phones and QWERTY keypads, and others used touch screens for texting, and variation in the number of messages per day and use of internet frequency per day may cause this variation. 5 Variation in mobile phone use frequency and unequal samples of the male-to-female ratio may cause this heterogeneity. 1 On the other hand, high heterogeneity exists among university students. This may be due to variations in smartphone use patterns, texting and gaming, sample size, and academic workloads in university, which may increase musculoskeletal complaints.52,53 In addition, the rapid proliferation of smartphones, cultural variation among students, and academic activities such as research and thesis writing may expose them to repetitive hand or wrist movements that cause musculoskeletal pain and discomfort in the wrists. 54 Prolonged smartphone use in awkward postures can cause the development of musculoskeletal disorders, including thumb pain and DQT. 53 Students may vary in use of mobile phones with excessive texting and repetitive movements of the thumb that cause static loads and risk for wrist/thumb pain and DQT. 55 Furthermore, university students overuse their smartphones and engage in multitasking, such as simultaneous typing, browsing, and repetitive scrolling through the screen, which contributes to hand/wrist pain and tendon strain.44,56
Implications for Practice and Policy
The result of this review has notable implications for addressing De Quervain’s tenosynovitis among students in Pakistan. It provides evidence for public health and occupational health expertise for awareness campaigns on safe mobile phone use. For healthcare providers, it helps to inform the growing burden of DQT and to consider mobile phone-related repetitive strain injuries during diagnosis. Within educational sectors, it helps to promote healthy digital practices and implement ergonomic interventions. Finally, for mobile phone and application designers, it helps to inform the effect of prolonged use of mobile phones by voice commands and digital well-being features to reduce thumb strain.
Strengths and Limitations
The study provides valuable evidence on underrecognized occupational and ergonomic health problems. However, the result should be interpreted with caution due to significant heterogeneity among the included studies. To address this, we conducted subgroup and sensitivity analyses to check the robustness of the pooled result. In addition, the result is constrained due to the cross-sectional nature that limits causal inference. Self-reported measures of the included studies may cause recall bias. Moreover, most of the included studies were collected by convenience sampling techniques that may introduce selection bias and limit the generalizability of the pooled finding. This review does not assess mobile phone usage patterns. Furthermore, including only English-published studies may miss studies published in other languages. Future longitudinal and interventional studies are required to establish causal relationships and to assess the determinants and impact of DQT.
Conclusion
This systematic review and meta-analysis found a high prevalence of DQT among students in Pakistan. Therefore, early identification and preventive measures are recommended. These may include ergonomic education and digital health awareness campaigns focusing on the risks of mobile phone–related repetitive thumb and wrist movements and using alternate hands when holding devices and during texting. In addition, apply hand and wrist stretching exercises, encourage regular breaks, and use mobile phone holders during conversations or texting.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302261438260 – Supplemental material for Prevalence of De Quervain’s Tenosynovitis among Mobile Phone Using Students in Pakistan: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ehi-10.1177_11786302261438260 for Prevalence of De Quervain’s Tenosynovitis among Mobile Phone Using Students in Pakistan: A Systematic Review and Meta-Analysis by Anmut Endalkachew Bezie, Awoke Keleb, Halid Worku Jemil and Kassaw Chekole Adane in Environmental Health Insights
Supplemental Material
sj-docx-2-ehi-10.1177_11786302261438260 – Supplemental material for Prevalence of De Quervain’s Tenosynovitis among Mobile Phone Using Students in Pakistan: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-ehi-10.1177_11786302261438260 for Prevalence of De Quervain’s Tenosynovitis among Mobile Phone Using Students in Pakistan: A Systematic Review and Meta-Analysis by Anmut Endalkachew Bezie, Awoke Keleb, Halid Worku Jemil and Kassaw Chekole Adane in Environmental Health Insights
Footnotes
Acknowledgements
The authors acknowledged the included papers in this study. In addition, we thank the database providers such as Google Scholar, PubMed, HINARI, Science Direct, and Semantic Scholars.
Ethical Considerations
This study is a systematic review and meta-analysis registered with PROSPERO (ID CRD420251040220) and no ethical approval was required.
Consent to Participate
This study used secondary data from previously published studies and consent to participation was not applicable.
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analysed during this study are included in this manuscript and its Supplemental Materials. Further inquiries can be directed to the corresponding author
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.