
Abstract
Climate change is becoming a recognized health concern in the scientific community, as heat exposure poses escalating health risks to outdoor occupational groups, particularly construction workers. Heat stress and climate change may lead to adverse physical health outcomes and reduced workability among construction workers. This systematic review and meta-analysis aimed to (1) examine the prevalence of physical health outcomes of construction workers in relation to heat exposure and (2) analyze the association between physical health outcomes of heat exposure and work performance by sex and age. Following the PRISMA guidelines and using a PICO framework, we conducted a comprehensive search across APA PsycINFO, MEDLINE, Embase, CINAHL, and Web of Science. Seventeen studies met our inclusion criteria. Outcomes were grouped into dehydration, heat-related illnesses (HRI), kidney function impairments, and heat-related deaths. Random-effects models were used for the meta-analysis, and subgroup analyses were performed using demographic variables. Pooled meta-analysis and heterogeneity statistics are only provided for the HRI outcome, as all other outcomes are only represented by single eligible studies. Dehydration demonstrated the highest single-study prevalence (0.97, 95% CI: 0.88, 1.00), contrasting with HRI pooled prevalence (0.40, 95% CI: 0.24, 0.58) and kidney function impairment single-study prevalence (0.17, 95% CI: 0.05, 0.39), which showed much lower estimates. High heterogeneity was present in the HRI symptoms category (I2 > 95%). Meta-regression revealed that males reported lower heat disorder prevalences in studies with both sexes (ß = −2.09, P = .049). Heat exposure significantly impairs the physical health of construction workers, particularly through dehydration and heat-related illnesses. Sex-responsive, psychological, and intervention-based studies are essential for protecting this vulnerable occupational group from accelerating climate change.
Introduction
Extreme heat events, driven by climate change, are defined as periods of heat waves with temperatures reaching hotter than historical climate averages. 1 Long-term exposure to extreme heat can adversely affect population health, including worker health and physical and cognitive functioning.2 -4 Heat stress refers to the physiological strain an individual feels owing to overexposure to heat through various environmental and physiological factors, including body temperature. 5 In this review, the term “heat stress” is used to encompass both passive and environmental heat exposure, as well as work related heat strain arising from physical exertion and protective equipment. Such exposure without adequate protective measures, including hydration, can lead to heat-related illnesses (HRIs) and disorders, including heat exhaustion and heat stroke. 6 Long-term heat exposure can lead to other physiological complications, including acute kidney injury (AKI) and chronic kidney disease (CKD).7,8
Among some of the most vulnerable populations are outdoor workers, particularly those in the construction sector, whose labor often demands continuous exposure to harsh environmental conditions. 9 These workers also often perform physically strenuous tasks with limited access to cooling resources, making them susceptible to heat stress and related illnesses. 10 An increased risk can be seen when other factors such as tight deadlines, and the requirement to wear protective clothing, regardless of weather conditions, are involved. 11 Although protective clothing protects workers from sun exposure and physical harm, it also restricts the evaporation of sweat and traps heat within the body. 11 These factors are especially concerning in low- and middle-income countries, given the high prevalence of informal employment, limited focus on occupational health and safety, climatic differences, and economic necessity.12 -14 Therefore, it is crucial to understand the impact of exposure on workers’ health to develop effective policies and safety regulations to safeguard worker well-being.
A review of the literature by Acharya et al 15 found that construction workers are the second-most affected by heat stress after agricultural workers. Research shows that construction workers in the U.S. are 13 times more likely to die from heat-related illnesses than those in other industries, with roofers and road construction workers being the most vulnerable. 15 In fact, Bonauto et al 16 found that the highest rate of workers’ compensation claims for heat-related illnesses in Washington State was in the construction industry, which is only expected to rise with the worsening of climate change. These heat conditions further augment the risk of heat-related illnesses in occupational settings. 15 Additionally, a summary of the literature on the effects of heat exposure on outdoor workers found that many workers experienced dehydration, dizziness, nausea, heavy sweating, and headaches. 17 Long-term dehydration and heat exposure have also been linked to acute and chronic kidney diseases, kidney stones, and urinary tract infections among outdoor workers.12,18
Sex plays a role in influencing the health effects of heat exposure, with women generally experiencing higher risks of heat-related mortality and adverse health outcomes than men. 19 Studies have shown that women and men face different levels of heat stress owing to differences in thermoregulatory capacity, heat tolerance, and heat susceptibility. 20 Women are more susceptible to dehydration and cardiovascular consequences of heat stress.21,22 Previous studies summarized in the literature indicate that increased exposure to outdoor heat is associated with reduced productivity in construction work, 23 and that elevated physiological strain, including increased heart rate has been reported among female construction workers exposed to heat. 24 However, in one study, the rate of heat illness is significantly higher in men than in women. 25 Beyond biological differences, workplace factors such as gender roles and workplace norms may also affect work performance in both men and women. As the construction industry is primarily male-dominated, 26 with masculine expressions and codes of behavior typically encouraged, avoidance of help-seeking behaviors is common among men. 27 This may discourage men from taking necessary breaks and reporting heat-related injuries, leading to the worsening of health effects. 28 It is important to understand sex and gender differences in the impact of heat exposure among construction workers to develop more equitable and inclusive policies aimed at protecting the physical health and well-being of all workers exposed to heat.
Age also plays a role in influencing the prevalence of physical health outcomes of heat exposure for construction workers. Studies have shown that both young and older workers face increased risks due to heat exposure but for different reasons. According to Calkins et al, 29 younger workers are more susceptible to heat-related injuries because they are frequently assigned physically demanding tasks compared to older workers and may exert themselves more. In contrast, older workers were seen to be more prone to these effects due to factors such as decreased skin blood flow, reduced cardiac capacity and higher likelihood of pre-existing conditions. 29 Additionally, Karthick et al 30 found that workers aged 55 and older were more vulnerable to heat exposure. Their findings also showed that younger workers’ productivity was less impacted by heat compared to middle-aged and older workers, suggesting that older workers may be less tolerant to heat exposure, increasing the risk of heat-related illnesses or injuries. 31
Given these gaps, this systematic review and meta-analysis was designed to achieve 2 primary objectives: (1) examine the prevalence of physical health outcomes among construction workers in relation to heat exposure, and (2) analyze the association between physical health outcomes of heat exposure and work performance in this sector by sex and age.
Materials and Methods
Overview
The current systematic review and meta-analysis was registered with PROSPERO (Registration number CRD42025649025) and adheres to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 32 The Population, Intervention, Comparison, Outcome (PICO) framework 33 was used to develop and refine the research question, as well as to inform the search strategy and eligibility criteria for study selection.
Eligibility Criteria
Table 1 describes the inclusion and exclusion criteria, based on the PICO framework, for the articles analyzed in this study. There were no restrictions on the geographical setting and study design (eg, case-control, cohort, longitudinal, time-series, ecological, descriptive, retrospective observational, cross-sectional, experimental, quasi-experimental, or quality improvement approaches), allowing for a comprehensive and inclusive systematic review analysis. However, only articles published within the past 25 years were included to ensure the relevance and contemporary applicability of the findings of this study. Additionally, non-peer reviewed articles, non-empirical articles, dissertations, pilot studies, and articles were excluded.
Study Inclusion and Exclusion Criteria Based on the PICO Framework.

Search Strategy
The search strategy was developed in consultation with an experienced University of Toronto Librarian to ensure the comprehensive retrieval of relevant studies. Searches were conducted in November 2024 across 5 electronic databases: APA PsycINFO (Ovid), MEDLINE (Ovid), Embase (Ovid), CINAHL, and Web of Science. In alignment with the PICO framework (Population, Intervention/Exposure, Comparison, Outcome), keywords and subject headings were developed to reflect the key components of our research question and were applied consistently across all databases. The Population was represented by the term “construction workers,” the Intervention/Exposure by terms like “extreme heat,” “heat stress,” “heat strain,” “heat exhaustion,” and “heat stroke,” and the Outcomes by terms related to “physical health,” “fatigue,” and “stress.” Boolean operators (AND, OR) were used to combine the search terms appropriately. The complete search strategy is shown in Supplemental Table 1 for each database. Moreover, the reference lists of the included articles and relevant review papers were manually screened to identify any additional eligible studies.
Study Selection
As the search was completed and computed for each database, articles were imported into Covidence, 34 a web-based platform for systematic review management. Duplicate studies were automatically removed by Covidence; however, the remaining duplicates were manually checked and removed by a reviewer. Four independent reviewers (BNK, RP, CC, and AS) conducted the first phase of screening—title and abstract review—by assessing each article for relevance and potential eligibility based on the inclusion and exclusion criteria. In the second phase, full-text articles were reviewed independently by the same 4 reviewers to determine whether the studies met all eligibility criteria. If there was uncertainty about whether a study met the criteria, or if there were disagreements between reviewers, these were discussed until consensus was reached. The study selection process is outlined in the PRISMA flow diagram.
Quality Assessment
Critical appraisal was performed by 4 independent reviewers (BNK, RP, CC, and AS) for each of the included studies. Cross-sectional studies were assessed using the Agency for Healthcare Research and Quality (AHRQ) criteria, 35 while cohort and case-control studies were evaluated using the Newcastle-Ottawa Scale (NOS). 36 Each study was evaluated using a set of methodological criteria, with each item rated as “Yes,” “No,” or “Unclear.” Based on these assessments, studies were categorized as having low, moderate, or high quality. To be considered acceptable for inclusion, a study had to meet at least 50% of the applicable criteria. Studies deemed to be of low methodological quality were excluded from the final analysis. Any disagreements between reviewers were resolved through discussion. Seven studies were classified as low quality (29.2%), 15 studies were classified as moderate quality (62.5%), and 2 studies were classified as high quality (8.3%; See Supplemental Table 2 for the details of each study’s critical appraisal).
Data Extraction
Data extraction was performed independently by 4 independent reviewers (BNK, RP, CC, and AS) using a standardized, piloted extraction form based on the Joanna Briggs Institute (JBI) template. Data were entered into Microsoft Excel 37 and included the following variables: study characteristics (author, year, country, sample size, and study design), population characteristics (age, sex, and occupation), exposure characteristics (description of heat exposure), health outcomes (prevalence rates, incidence rates, and associated confidence intervals), and study quality indicators (risk of bias). These variables informed the synthesis of findings across studies and were used to organize data for descriptive analysis and, where appropriate, meta-analysis. A list of definitions and outcomes are reported in Supplemental Table 3.
Statistical Analysis
Meta-analyses were conducted using R version 4.4.2, employing the “meta” (version 7.0-0) and “metafor” (version 4.4-0) packages. Given that only a few studies have reported the incidence rates, the meta-analysis was conducted using prevalence rates. The studies examined a wide range of outcomes, ranging from heat discomfort and kidney function to heat-related deaths; hence, to control for the different nature of these outcomes, they were grouped into 4 categories: (1) heat-related mortality (deaths due to heat stroke), (2) dehydration, (3) heat-related illness (HRI) symptoms, and (5) kidney function impairments.
Overall, a range of sensitivity analyses were incorporated. We compared fixed- and random-effects models to verify effect size stability, and the subgroup forest plots included both models for each group of outcomes. In the end, random-effects models were employed to account for between-study variability and provide more generalized estimates. We also conducted leave-one-out analysis to observe if there were influential outliers and to observe how each individual study affected the pooled effect sizes. To further evaluate the robustness of the findings, publication bias was assessed using Egger’s test to determine the potential impact of unpublished or null studies on overall effect size. Additionally, age and proportion of males were included as moderators to explore whether outcomes differed across these groups, strengthening the study’s validity. An additional meta-regression was run for studies that were not entirely male to determine whether sex diversity within study samples modified the observed effects. Throughout the study, heterogeneity was quantified using the I2 statistic, with values categorized as low (0%-40%), moderate (40%-69%), and high (⩾70%).
Meta-analytic pooling was only performed for outcome categories having at least 2 independent studies contributing to the estimate. For categories represented by a single eligible study, we report the single-study estimates with 95% confidence intervals. Heterogeneity statistics (I2) and meta-regression pooled prevalences are neither calculated, nor presented for those outcomes.
Results
Figure 1 presents the PRISMA flow diagram of the included and excluded studies. A total of 1740 research articles were initially screened based on their titles and abstracts, after removing duplicates. Of these, 1569 articles were excluded due to not meeting the inclusion criteria, leaving 170 studies for full-text review. Following full-text screening, an additional 149 articles were excluded leaving 21 studies that met the inclusion criteria. A total of 7 studies were obtained from hand-searching that were not included in the search results, with 3 meeting the inclusion criteria. Of the 24 studies that met eligibility, 17 were assessed as having low risk of bias and were included in the review, with data aggregated for the meta-analysis.
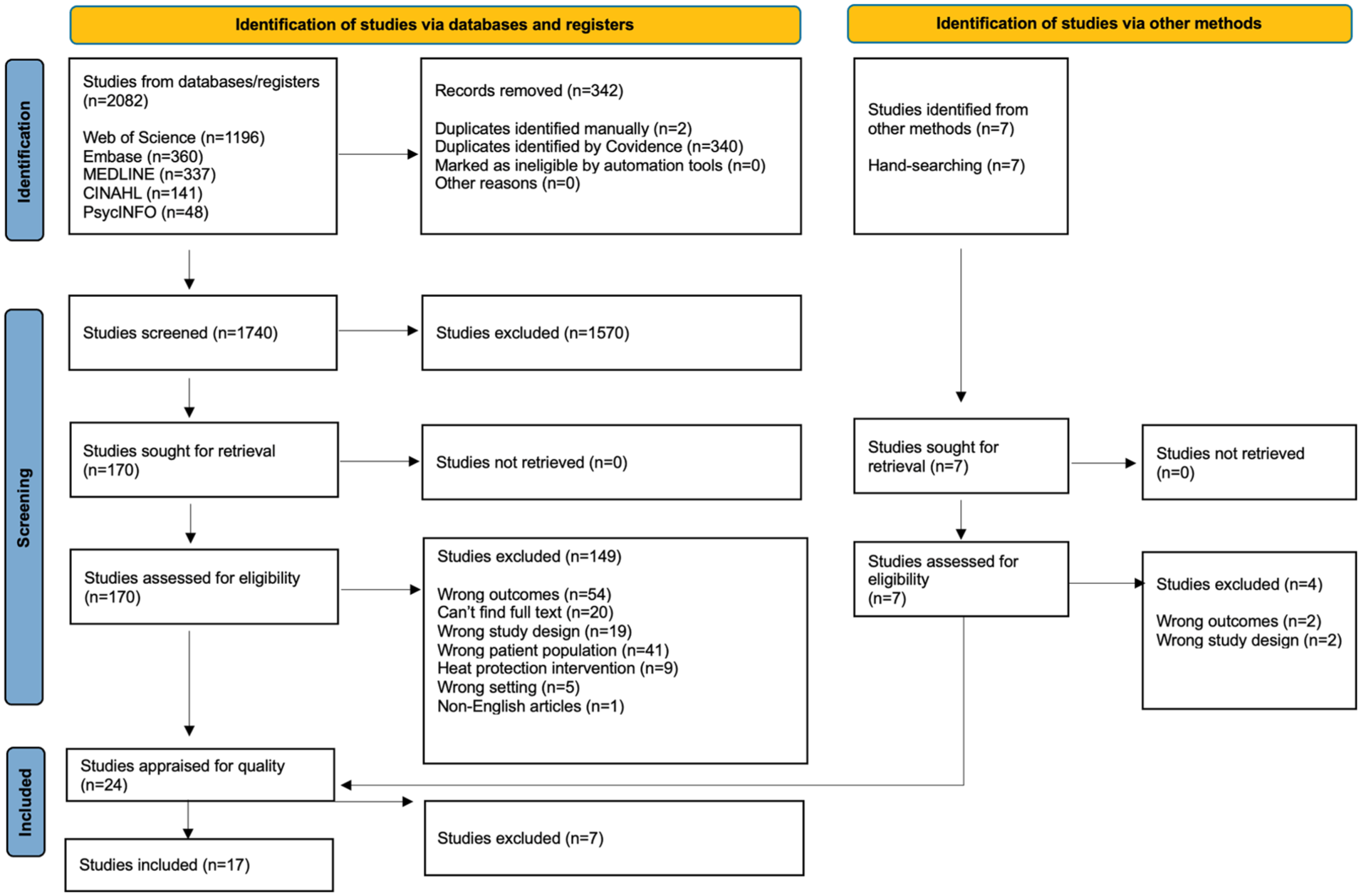
PRISMA flow diagram.
The 17 included studies were conducted in diverse geographic regions, primarily North/Central America and Asia, reflecting a range of climate conditions and occupational settings. Among these studies were 4 mixed method studies38 -41, 3 cross-sectional studies.31,42,43 The remaining studies included 2 cohort studies44,45, 2 field studies46,47, 2 observational studies24,48, 1 longitudinal study, 7 1 comparative and experimental study, 49 1 case study, 50 and 1 spatial modeling study. 51 These studies evaluated a wide range of heat-related health outcomes among construction workers, including symptoms of heat-related illness (HRI),24,43,46,48,50 dehydration, 49 kidney function impairments, 46 and heat-related death. 44 HRI symptoms included general HRI symptoms, heat exposure concerns, heat stress and strain and heat discomfort. . .These outcomes were measured using environmental indicators,24,38 -41,43,48,50,51 such as wet-bulb globe temperature (WBGT), physiological markers,24,42,43,45,48,49 such as body temperature exceeding 38°C and high strain (VO2 max) due to exertion in hot conditions, biomarkers,39,41,46,49,52 such as urine samples, self-report methods31,38,40,41 and mortality records. 44 The key characteristics of the included studies, including sample size, study design, male proportion, mean age, outcomes, and study locations, are summarized in Table 2.
Characteristics of Studies Included in the Meta-Analysis (n = 17).

Note. NA = Not available or not reported in the original study. The prevalence measures were grouped into broader categories for meta-analysis, namely, heat stress, heat-related illnesses (HRI), kidney function impairments, dehydration, and heat-related deaths. Other abbreviations used in the table include: AKI = Acute kidney injury; WBGT = Wet bulb globe temperature. General construction worker = worker specialization was not reported.
This meta-analysis examined the prevalence rates of various heat-related health outcomes across 17 studies assessing the impact of heat on health. Four studies52 -55 were excluded because they did not report the prevalence rates or sample sizes. To enhance interpretability, the reported outcomes were classified into 4 categories: (1) heat-related mortality (deaths due to heat stroke), (2) dehydration, (3) heat-related illness (HRI) symptoms, and (4) kidney function impairments. This classification allowed a structured examination of both acute effects (eg, HRI symptoms and dehydration) and longer-term outcomes (eg, CKD). Given the high heterogeneity in each subgroup, a linear random-effects model was used to estimate the pooled prevalence within each category, revealing statistically significant adversely effects of heat exposure on construction workers. The forest plot for HRI symptoms (Figure 2) presents the prevalence estimates for various HRI outcomes including heat stress and high body temperatures.

Forest plot by prevalence measure for HRI Symptoms.
Given the substantial heterogeneity observed across the HRI measures (I2 = 98.7.% for the overall model), a random-effects model was employed to account for the variability between studies.
Overall, the prevalence of heat-related health outcomes varied considerably by category. Heat-related illness (HRI) symptoms (Figure 2) had a pooled prevalence of 40% (95% CI [0.24, 0.58]) and high heterogeneity (I2 = 98.7%) indicating substantial variability across studies. Specifically, heat stress and heat exposure concerns showed prevalences of 47% (95% CI: [0.18,0.77]) and 39% (95% CI: [0.30,0.48]), respectively, with the latter showing fairly consistent results across the studies (I2 = 98.7%). Categories represented by only a single study produced more extreme estimates: Kamaku et al (2021) reported high heart rate in 9% of workers, while Petropoulos reported elevated body temperature in 77% (95% CI [0.73, 0.80]).
Beyond HRI symptoms, Dong et al 44 showed a prevalence of 36% for heat-related deaths (0.36, 95% CI [0.31, 0.42]). Low prevalence was observed for the study on kidney function, Al-Bouwarthan et al 7 which reported a prevalence rate of 17% (0.17, 95% CI [0.05, 0.39]). In contrast, the study on dehydration showed the highest prevalence, estimated at 0.97 (95% CI [0.88, 1.00]). 49
Lastly, a few studies compared construction workers to other populations. For instance, Inaba and Mirbod 40 compared them to traffic workers and found that construction workers had a higher prevalence of work difficulty due to hot weather and higher rates of symptoms in the upper extremities. Moreover, Phanprasit et al 43 compared it to foundry workers and found that adverse health effects caused by the heat were more common among foundry workers than in construction ones.
We assessed the publication bias and potential moderators in our meta-analysis. Egger’s regression test (P > .05) and Begg’s rank correlation test (P > .05) were performed for the HRI symptoms outcome, which had a sufficient number of eligible studies. The results indicated no significant evidence of publication bias, suggesting that the results for this outcome are unlikely to be skewed by missing studies or small-study effects.
We also conducted meta-regression analyses to examine whether demographic factors explained heterogeneity in the meta-analysis results. However, neither the mean age of workers nor the proportion of males in the study had a significant moderating effect on heat-related outcome prevalence (both P > .05).
When restricting this to the studies that contained female participants, we found that studies with a higher proportion of male workers reported lower heat disorder prevalence (β = −2.09, P = .049). However, it should be noted that residual heterogeneity remained high in these models (I2 > 95%), indicating that other unmeasured factors likely contributed to the variability in outcomes between studies.
Discussion
The findings of this review reveal that heat exposure is associated with a wide range of adverse health effects in construction workers, ranging from acute conditions such as dehydration and HRI symptoms to longer-term kidney function impairments and even heat-related mortality. Among these outcomes, dehydration was the most prevalent. However, it must be noted that dehydration was only reported in one study. As a result, it cannot be generally interpreted as a robust pooled prevalence among construction workers. Nonetheless, all the identified heat-related health outcomes represent critical occupational hazards for construction workers and require urgent attention in workplace health and safety strategies. Additionally, our analysis did not find any significant differences in physical health outcomes across worker demographics such as age or sex.
Prevalent Health Issues
Our analysis identified a range of heat-related health issues that are highly prevalent among construction workers. Approximately half of the workers in the included studies experienced high levels of heat stress or heat strain (pooled prevalence, approximately 49%). A consistent body of research documents how prolonged heat exposure elevates heat strain, which is exacerbated by performing strenuous work tasks under heat. 52 In fact, construction workers have been documented as one of the occupational groups most affected by heat stress, second only to agricultural workers.15,56 Additionally, the results also revealed that HRI symptoms account for a prevalence rate of 36% across several studies with geographic and climatic differences. Previous studies indicate that construction workers are among the highest risk groups in occupational HRI.42,57 -59 Common mild HRI symptoms include dizziness, dehydration, and nausea; if these early signs go unrecognized or are left untreated, they can rapidly progress to more severe conditions, such as heat stroke or even death.60,61 Collectively, these results reinforce the notion that heat-related symptoms and heat stress are persistent occupational hazards in the construction sector. Although dehydration is ubiquitous, the prevalent conditions of heat strain and HRI still pose serious risks. This highlights the need for robust heat mitigation strategies and safety guidelines on worksites, for example, training workers to recognize early symptoms, implementing heat alert programs, and mandating rest/work cycles, to prevent these conditions from escalating.
The study reporting on dehydration found that virtually all workers exposed to heat experienced dehydration, making it the most prevalent heat-related condition in this population. Dehydration remains a critical concern for construction workers, as insufficient hydration can have a myriad of secondary effects on work performance and health. Wittbrodt and Millard-Stafford 62 found that cognitive functioning, including concentration, motor coordination, and reaction time, were significantly impaired by it. Similarly, previous studies have found that encouraging regular fluid intake helps construction workers maintain their productivity, even under high heat conditions.63,64 These findings suggest that dehydration is an adverse health outcome associated with heat exposure, which demands prompt intervention (eg, improved access to water and scheduled rest breaks) to protect the health and productivity of construction workers globally.
Demographic Differences
Our meta-analysis did not find statistically significant differences in heat-related health outcomes between male and female workers, or between younger and older workers. These findings contradict existing trends in the literature, and are likely attributable to low statistical power in the meta-analysis. Han et al 4 found that women tended to be more sensitive to heat exposure than their male counterparts, with many women reporting cardiovascular strain, fatigue, headaches, and dizziness, which resulted in a 29% difference in productivity losses. Similarly, older workers have also been shown to have reduced productivity due to heat exposure,4,50 highlighting their vulnerability to adverse health risks amidst rising temperatures. Li et al 50 found that productivity on construction tasks decreased as workers aged and attributed this decline to increased fatigue, decreased physical ability, and older workers’ greater preference for less physically demanding tasks under heat stress. The lack of observable sex- or age-based differences in our results is likely due to limitations in the available data, notably the severe underrepresentation of women in the construction workforce sampled and the relatively narrow age range in many studies, which together limit the power to detect demographic effects. Nevertheless, evidence from the broader literature clearly indicates that females and older workers are particularly vulnerable to heat exposure, underscoring the need to prioritize protective interventions for these groups.
Limitations of the Study
This review had several limitations that should be considered when interpreting the findings. There was substantial heterogeneity among the studies and outcomes included. The included studies varied in whether heat stress reflected passive environmental exposure or work-related heat strain, and these could not be consistently distinguished across studies. The studies varied in their specific outcome definitions and measurement methods, and we had to group somewhat dissimilar outcomes into broader categories for meta-analysis. Some studies also lacked reporting on important quality risk-of-bias indicators, which introduces uncertainty regarding the strength of their evidence and complicates direct comparisons between studies. As noted above, drawing conclusions about differences by sex was challenging because of the very small number of female participants across the studies, reflecting the male-dominated construction industry. Similarly, large age ranges may have limited our ability to draw meaningful conclusions about age-based differences in physical health and work performance. Furthermore, the meta-regression results regarding sex proportions should be interpreted with extreme caution. These analyses were limited by low statistical power and minimal variability in the moderators across the included studies. Because these are study level associations, they are also susceptible to the ecological fallacy and cannot be used to infer individual-level risks. This highlights the need for more inclusive research in the future. Additionally, Eco-anxiety, or climate anxiety, is increasingly recognized as a mental health concern linked to emotional distress resulting from environmental change. Another relevant and emerging concept in the context of climate-related events is Solastalgia, describing the distress caused by environmental change impacting one’s sense of place. However, since the focus of our paper is on physical health outcomes, we have chosen not to explore these aspects in depth, representing important areas for future research.
Another major limitation is that multiple outcome categories (dehydration, kidney function impairments, and heat-related deaths) are only represented by single studies. Prevalence estimates for these are reported as single study-level estimates rather than pooled estimates. This severely limits the strength and generalizability of the evidence for these outcomes. In addition, the meta-analysis used a small number of studies which had limited variability of key moderators (eg, age and sex distribution). This leads to lower statistical power, increasing the chance of Type I and II errors. As such, findings relevant to the moderators should be cautiously interpreted.
Finally, the review may have been influenced by publication bias. Although the statistical tests did not indicate a significant problem for the HRI symptoms outcome, publication bias could not be formally assessed for single-study outcomes. We restricted our search to peer-reviewed literature in English, excluding gray literature and non-English publications. This exclusion could bias our results toward positive findings, since studies with null or negative results (often found in gray literature or local reports) are less likely to be published in academic journals. These limitations suggest caution in generalizing the exact prevalence estimates, although the overall trend of adverse health outcomes from heat is clear.
Future Research and Implications
This review underscores the critical need to further address the multifaceted physical health issues among construction workers. Given that the study findings only focused on the prevalence of physiological strain due to heat exposure, future studies should aim to test the associations between heat and physical health outcomes. Larger studies that include more female and older construction workers will enable a better assessment of whether (and how) heat differentially affects these subpopulations. Such data could inform more tailored interventions, considering both biological differences (eg, age-related thermoregulation or sex-specific physiological responses) and social factors (eg, work roles or cultural norms around taking breaks) in the design of occupational health policies. Longitudinal and interventional studies should also be prioritized in future research, as they allow for a better evaluation of the effectiveness of certain heat mitigation policies and strategies, such as mandatory breaks in well-shaded areas and heat acclimatization programs. This allows for a critical analysis of how certain occupational management practices influence workers’ conformity to workplace safety guidelines. From a policy perspective, it is crucial to emphasize the importance of implementing stronger safety strategies that consider climate change and heat exposure. Health agencies and government sectors must collaborate with each other to enforce labor protection and establish safety guidelines.
Conclusion
This systematic review and meta-analysis highlights the prevalence of heat exposure on the physical health and safety of construction workers. While several estimates are single study only, we found that dehydration, heat stress, and heat-related illness symptoms emerged as prevalent issues, alongside evidence of their association with kidney function. These conditions pose serious risks to workers and can impair their well-being and productivity. Addressing this gap in future research is crucial to gaining a more comprehensive understanding of how this population is affected by heat exposure. Additionally, there were no significant differences in health impacts by sex and age, potentially due to the underrepresentation of women in the construction sector. As a result, future research should also focus on women in the construction industry to explore how sex- and gender-specific factors might influence different health effects and to ensure those challenges are addressed through tailored interventions.
In the context of climate change, construction workers are on the front lines of heat exposure, and their health and performance are increasingly at risk as temperatures continue to rise. Our review underlines the need for targeted, evidence-based strategies to mitigate heat-related risks in construction. This may include implementing practical interventions on worksites (eg, hydration programs, rest breaks, and cooling measures) and strengthening occupational safety regulations to protect workers during periods of heat exposure. Such measures will not only improve day-to-day working conditions but also serve as essential adaptations to a warming climate, helping to safeguard the well-being of this vital workforce in the years to come.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302261426720 – Supplemental material for Heat Exposure and Health Outcomes in Construction Workers: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ehi-10.1177_11786302261426720 for Heat Exposure and Health Outcomes in Construction Workers: A Systematic Review and Meta-Analysis by Behdin Nowrouzi-Kia, Vijay Kumar Chattu, Thankam S. Sunil, Nancy Carnide, Heather Thomson, Raihana Premji, Aishvinigaa Sathananthan, Charlene Choi and Javier Mencia-Ledo in Environmental Health Insights
Footnotes
Acknowledgements
We gratefully acknowledge Bao-Zhu Stephanie Long and Kishana Balakrishnar for their contribution to this study.
Author Contributions
BNK conceptualized the study. The study’s conceptualization was endorsed by all authors (BNK, VKC, TS, NC, HT, RP, AS, CC, JML). Author JML conducted data analysis and authors RP, AS, and CC provided interpretations of the findings. BNK prepared the initial draft and RP, AS, CC, and JML assisted in revising and editing the final draft of the manuscript. All authors have made significant revisions to the manuscript. Author BNK provided supervision throughout the development of this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Seed Grant for Climate, Health & Sustainable Care at the University of Toronto.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Review Registration
The protocol has been formally registered with PROSPERO under CRD42025649025.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.