
Abstract
Introduction:
Workplaces are vital for Occupational Safety and Health (OSH) knowledge dissemination. This study examines OSH knowledge, attitudes, and practices among formal and informal sector workers in Freetown, Sierra Leone, and their associations with workplace characteristics.
Methods:
A cross-sectional survey was conducted using a validated, semi-structured questionnaire to collect data on sociodemographic characteristics, workplace safety factors, and occupational safety indicators. The survey assessed 3 primary outcomes variable adequate knowledge, good attitude, and good practice. Multivariable analyses were used at significant level (P < .05) to examined associations between independent and outcomes variables.
Results:
The study included 516 respondents, predominantly were male (84.3%). Educational attainment varied, with 23.6% having tertiary education and 4.7% non-formal education. Literacy rates showed 76.6% were literate. Significant disparities emerged between sectors: formal sector workers demonstrated higher rates of adequate knowledge (60.7%), good attitudes (54.9%), and good practices (77.3%) compared to informal workers. Formal sector employment was significantly associated with better OSH outcomes, including knowledge (aOR = 2.4, 95%CI: 1.43-4.15, P < .001) and practices (aOR = 16.2, 95%CI: 2.80-95.81, P < .002). These findings highlight substantial sector-based differences in occupational safety and health indicators.
Conclusion:
This study reveals substantial and significant disparities in occupational safety and health (OSH) between formal and informal sector workers. Formal sectors employment is strongly associated with better OSH outcomes, particularly safer practices, thus, underscoring an urgent need for targeted policy, tailored training programmes, gender-sensitive interventions, and regulatory interventions to protect vulnerable informal workers.
Introduction
Workplaces serve as critical settings for disseminating Occupational safety and Health (OSH) knowledge to safeguard worker well-being, improve productive, and job satisfaction.1-3 The norms, standards, and surveillance systems set up by important international and national organisations are what shape the global framework for occupational safety and health.4,5 The World Health Organisation (WHO) has a Global Plan of Action on Workers’ Health, and the International Labour Organisation (ILO) has conventions on occupational safety and fundamental principles and rights at work. These are the basic policies that make up the policy architecture.5-7 Regional agencies like the European Agency for Safety and Health at Work (EU-OSHA), which drives research and preventive strategies within the European Union, and research bodies like the National Institute for Occupational Safety and Health (NIOSH) in the United States, which sets evidence-based exposure limits and does important surveillance,8,9 help make that structure work. These groups work together to set global standards for worker safety, decent work, and hazard assessment.
It is therefore important to put a local socio-labour reality, like the formal and informal sectors in Sierra Leone, in this global institutional context. The ILO, WHO, and other related agencies set the rules and diagnostic tools that directly affect the professional growth of OSH practitioners and the enforcement of national laws. Examining the workforce in relation to these established frameworks that evaluate deficiencies in ILO convention ratification, conformity with WHO health promotion models, or the relevance of EU-OSHA risk assessment tools offers a crucial, standardised benchmark.10,11 This method goes beyond just looking at things on their own and gives a full picture of how local working conditions compare to global standards and how the international community is working together to make them better.
The Knowledge-Attitude-Practice (KAP) model is conceptually based on behavioural theories, including the Health Belief Model (perceived susceptibility, benefits, and barriers to safe practice) and the Theory of Planned Behaviour (subjective norms and perceived behavioural control). These theories elucidate the disparity between knowledge and actual safety practices.1,12,13 Recent implementations in Low- and Middle-Income Countries (LMICs) settings, particularly within the construction industry, validate the applicability of these models in forecasting safety compliance. 14 Additionally, risk perception theories explain how workers in informal settings may normalise high-risk environments, influencing their hazard assessment and precautionary behaviour, a phenomenon particularly pronounced in precarious employment.15-19
It is essential to examine this behavioural perspective through the macro-contextual determinants’ characteristic of LMICs. The significant disparities observed are not merely individual failures but are influenced by systemic factors: regulatory enforcement gaps that disproportionately impact the informal sector, severe socio-economic constraints that necessitate a trade-off between livelihood and safety, and entrenched gender norms that dictate exposure to and access to protective resources.10,12,20,21 Recent studies of the structural factors that affect worker health have shown that combining these theoretical and contextual layers offers a better explanation for why KAP outcomes differ so much between sectors. This shift moves the conversation from individual behaviour to the structural and social factors that affect workplace safety. 22
However, stark disparities exist between formal and informal sectors in low-resource settings such as Freetown, Sierra Leone. The literacy rate among informal workers is significantly lower (47%) compared to formal workers (78%). 23 In the formal sector, OSH knowledge is formalised and disseminated through compulsory training and regulations.24-26 On the other hand, people who work in the informal sector learn by doing, which means they don’t know about many dangers or their rights.27,28 This creates a fundamental gap in preventive safety understanding. Accountability and compliance culture shape how people in the formal sector think about OSH.24,25 In stark contrast, informal sector attitudes are characterised by a surviving mentality, perceiving safety as an expensive luxury and often embracing risk with fatalism. 29 Formal sector practices involve executing documented protocols, yet often deviate due to production pressure. 30 Informal sector work is defined by improvisation with inadequate PPE and unsafe environments, rarely meeting basic OSH standards.1,27
Informal workers often lack access to basic sanitation, with only (32%) had handwashing facilities at their workplaces. 31 They are predominantly engaged in high-risk industries such as wood work, welding, artisanal stone or sand mining, street vending, and waste collection, often working without contracts, social security, or OSH training.6,32,33 These conditions exacerbate occupational hazards, with work-related injuries and diseases placing additional strain on health systems, reducing productivity, and deepening household poverty.32-35
Globally, occupational accidents and work-related diseases result in over 2.3 million fatalities annually.4,32,36 In Sub-Saharan Africa, (43.2%) of workers report having experienced at least one occupational injury in their lifetime. 37 The COVID-19 pandemic further exposed systemic weaknesses in worker protections, particularly in informal economies where social security coverage is minimal.38,39 While market-based OSH, services have been shown to improve cost-effectiveness, flexibility, and accident prevention, 40 their adoption in Sierra Leone remains inconsistent due to weak enforcement and poor employer-worker collaboration.41,42
Disparities in Knowledge, Attitudes, and Practices (KAP) on OSH Between Formal and Informal Sectors
Significant differences exist in OSH-related knowledge, attitudes, and practices (KAP) between formal and informal workers. Globally, only (6.4%) of workers demonstrated strong knowledge of COVID-19-related occupational risks, though over (90%) reported positive attitudes or practices.43,44 In Sub-Saharan Africa, permanent workers exhibit higher awareness of workplace hazards (87%) compared to non-permanent workers (66%), yet temporary workers display poorer safety attitudes (82% vs 38% in permanent workers). 1 In Sierra Leone, while (72.7%) of healthcare workers had good knowledge of COVID-19 prevention measures, only (58.3%) maintained positive attitudes, despite high compliance with hand hygiene (98.8%).43-45 However, no studies have systematically compared OSH-related KAP between formal and informal workers in Sierra Leone, particularly in high-risk non-healthcare sectors.
This workplace-based survey assesses KAP disparities between formal and informal workers in Freetown, Sierra Leone, to identify sector-specific gaps and inform targeted interventions. The findings will support evidence-based policies to improve OSH awareness, compliance, worker protection and promoting safety behaviour in underserved workplaces.
Methods and Materials
Study Design and Period
We conducted a cross-sectional study among workers in the formal and informal sector in Freetown, Sierra Leone – July 2023 to September 2023.
Study Area
Sierra Leone is in West Africa with a tropical climate and diverse environment. It is divided into 5 regions (Eastern, Northern, Northwest, Southern, and Western Area), with a population of 7 701 185 and (59%) living in rural areas and (41%) in urban areas. 46 This study was conducted in Freetown the capital city of Sierra Leone. Freetown is Sierra Leone’s major urban, economic, financial, cultural, educational, and political centre, as it is the seat of the Government of Sierra Leone, and its population is 1 055 964. 46
Study Population
The study participants for this study were selected from both formal and informal sectors in Freetown; where all workers (such as trainee, volunteer and gainfully employ) of any age category who were present in the workplace and were interviewed after informed consent.
Inclusion Criteria
All workers who had worked 6 months or more, consented to participate in the study, and are present during the data collection were included in the study and interviewed.
Exclusion Criteria
A worker who was on maternity/paternity leaves were excluded from the study.
Sample Size Estimation
We determined the sample size using the Western Area population of 1 055 964. We used a prevalence of occupational illness/injuries of (18.3%) for workers in the formal and informal sectors each. 46 Using the epi.info 7.2.5 Stat Calc., which can be found at http://www.cdc.gov/epiinfo, we calculated the sample sizes (n) for the formal and informal sectors, based on the following presumptions: Expected % frequency (P): (18.3%) in both formal and informal sectors; design effect: 1.0, confidence interval: 95%; margin of error (d): (5%). The sample size (n) calculated was 230 each for both the formal and informal sectors. Taking into account the (10%) non-response rate. We calculated the non-response rate adjustment using the formula N = n/1–R, where “N” represents the final sample size and “R” represents the anticipated non-response rate. A (10%) non-response rate of 26 for formal and informal sector each was calculated, and also, 2 each purposively were added up during data collection, and the final total sample size of 516 respondents was interviewed.
Despite the substantial workforce population in Freetown, the final analytical sample comprised 238 formal and 278 informal workers. This sample size was determined by predefined eligibility criteria, logistical challenges in accessing informal sector workers, and survey non-response rates. Participants were selected from the Western Area using a simple stratified sampling technique, which facilitated targeted representation across key occupational sectors while maintaining practical feasibility.
Sample Size Justification and Power
The “StatCalc” module in Epi Info™ version 7.2 was used to figure out the a priori sample size for a comparison of 2 proportions. The main goal was to compare the rates of “adequate knowledge” between sectors. We used 95% power, a 2-sided alpha of .05, and a 1:1 allocation. This calculation gave us n = 230 participants in each sector. The final analytic samples of 238 (formal) and 278 (informal) workers both meet or exceed this goal. The imbalance in the sample size was unintentional wherein the data collectors collected more than expected sample size. And the study investigators decided to maintained the additional number of the participants. This will not affect the precision of the study.
The obtained sample yields over 85% power for the primary sectoral comparison. We recognised that the limited size of the smaller group (n = 238) constrains the number of covariates in multivariable models, which will be maintained in a parsimonious manner. The study lacks sufficient power for comprehensive within-sector subgroup analyses (eg, by specific job position).
Sampling Technique
We applied a stratified multi-stage sampling technique. First, Freetown was split into 3 regions (East End, Central, and West End), each subdivided into 3 zones based on administrative and economic maps, for a total of 9 zones. 47 The sampling frame of workplaces was then developed using municipal business registries and local government data, stratified by formal and informal sector within each zone.48,49
We randomly selected sample of 66 formal workplaces and 73 informal workplaces from the stratified zones list. Then, within each workplace (formal and informal workplaces), 2 to 3 workers were randomly selected for interview using a simple random sampling technique. The respond rate was 90.9% in the formal sectors and 93.2% in the informal sectors (see Figure 1. Participant recruitment flow diagram) below. While high response rates were achieved within the selected clusters, it is important to note that the final sample of 516 workers represents a small fraction of Freetown’s substantial workforce. The results are representative of workers within the sampled economic clusters of the 9 zones but should be generalised to the entire citywide workforce with caution, as isolated or home-based informal enterprises may be under-represented in the municipal registries that formed the sampling frame. To maintain the target sample size, any selected workplace that declined was replaced by the next workplace on the randomised list for that zone.
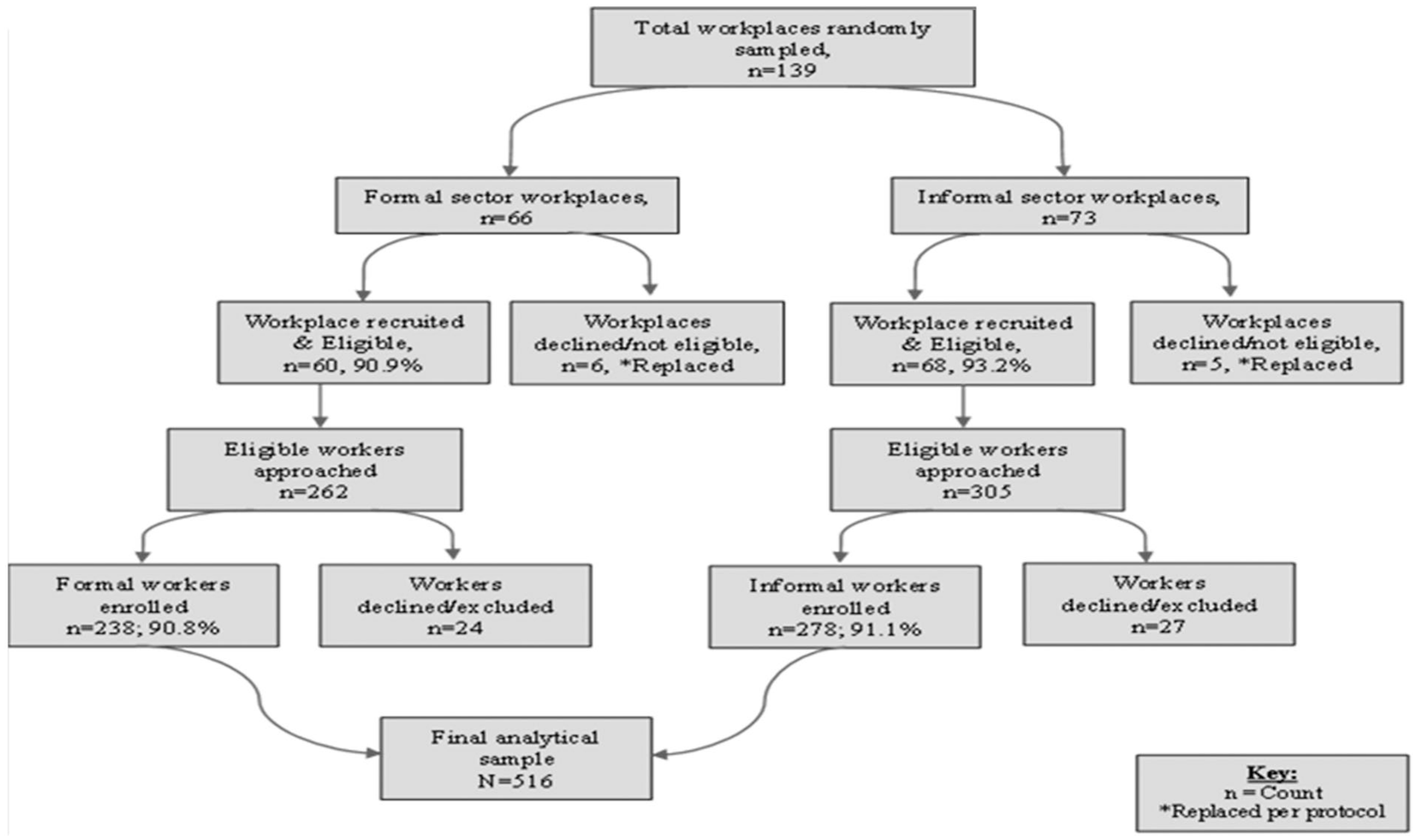
Participant recruitment flow diagram.
Data Collection Tools and Procedure
The study used the Kobo Collect tool to design a semi-structured questionnaire for interviews, collecting demographic information and compliance with OSH procedures. This questionnaire was adapted from the World Health Organisation (WHO) and International Labour Organisation (ILO) Joint Toolkit for Developing National Programmes on Occupational Health and Safety for Workers,50,51 incorporated modules on knowledge, attitude, practice, risk perception, and adherence. We conducted a pre-texted using the tool on 5% of the total sample size (13 per sector) in non-participating sites to ensure clarity and validity. We modified the tool based on pilot feedback, including simplifying technical terms and adding locally relevant examples of workplace hazards and procedures. The data collection teams included technical officers from the Ministry of Health who were trained on electronic-based data collection and informed consent. A face-to-face interview was conducted and the question were translated into local language (Krio). The principal investigator and research supervisor supervised the data collection process for quality assurance. Data was then downloaded for further analysis.
Study Limitation
This study has several limitations. First, while the sample size was sufficient for initial exploratory analysis, it may not comprehensively reflect the full heterogeneity of Freetown’s workforce. Second, the higher representation of specific informal sector subgroups could constrain the generalisability of the findings. thirdly, non-response bias may have influenced the results, as individuals who declined or were unavailable to participate might differ systematically from those included in the study. Finally, we acknowledge the temporal gap in the study period, and the manuscript submission date (2025) may not reflect the current condition of OSH in Sierra Leone. While OSH data reflects mid-2023 conditions, the core OSH challenges and structural factors identified likely remain relevant at that time, and a cross-sectional design captures a moment in time, not a trend. Self-reported data may overstate positive practices. Participants may have altered behaviour during observation. To mitigate information bias, the questionnaire was pre-tested and piloted to ensure clarity and validity. For each, we suggested a mitigation strategy for future research, such as random sampling of informal worksites or communities, longitudinal designs, and mixed-methods approaches to enhance validity.
Data Management and Analysis
The data was retrieved from the Kobo Collect server, stored, cleaned, and the database was stored on a password-protected computer. We analysed the data using Epi-Info 7.2.5, Microsoft Excel 2019, and SPSS 23. A Descriptive analysis such as median and range for age, proportions and ratios for categorical variables such as sex and among many others were computed. To build the multivariate model, covariates was selected based on the available literature. The measure of association, odds ratio (OR) and adjusted odds (aOR) analysis were performed to test for significant associations. The covariates include: workplace type, educational attainment, awareness of health and safety measures. The outcome variable were adequate knowledge, good attitude, and good practices, controlling for confounders (eg, age, sex, education, sector type, job position). For all of the analyses, the variables were considered statistically significant at P < .05. The analysis tested a priori hypothesis. Variance Inflation Factors confirmed no multicollinearity (all VIFs < 2). Model fit was good (H-L P = .42, AUC = 0.78). A pre-specified interaction was tested and excluded (P = .15). The reported adjusted odds ratios (ORs) for the primary exposure can therefore be interpreted as estimates accounting for the identified confounding structure, with reasonable confidence in model specification and stability.
Measurement of Outcomes and Validation
The KAP outcomes were categorised using a data-driven threshold: the overall sample mean score for each domain, to guarantee a clear and valid analytical method. This approach establishes a reliable standard for differentiating “adequate” from “inadequate” KAP in the absence of external criteria.13,45,52,53 All multi-item scales exhibited satisfactory to good internal consistency (Cronbach’s: Knowledge = .85, Attitude = .78, Practice = .65) and this was based on the mean cutoff. Therefore, this study used the mean scores to determine the outcome variables in which the level of knowledge describe as: adequate or limited; Attitude as: good or poor; and Practices as: good or poor. The mean cutoff point for knowledge was 43.3, attitude was 61.0, and then practice was 38.0. For knowledge: 24 questions were asked to assess respondents’ knowledge on OSH measures in the workplaces, each positive response was scored 1, otherwise scored as 0, with a maximum score of 24. Respondents whose mean scored was ⩾43.3 were coded 2 and classified as having adequate knowledge and those whose mean scored was <43.3 were coded 1 and classified as having limited knowledge. For attitude: 18 questions were asked to assess the attitude of workers towards OSH, each positive response was (Strongly Agree or Agree = 1 and Neutral, strongly disagree, or Disagree = 0). The maximum response was 18, with respondents whose mean scored was ⩾61.0 were coded 2 and classified having a good attitude and those whose mean scored was <61.0 were coded 1 and classified as poor attitude. And for practice: 22 questions were asked to assess the practices of workers of OSH measures, each positive response was scored 1, otherwise scored as 0, with a maximum score being 22. Respondents whose mean scored was ⩾38.0 were coded 2 and classified as having good practice and those whose mean scores was <38.0 were coded 1 and classified as poor practice.
Ethical Consideration and Confidentiality
We obtained ethical clearance from the Sierra Leone Ethics and Scientific Review Committee (SLESRC No: 020/02/2023). Workplace managers/supervisors were informed about the study. All workers who were present during the survey and of any age category were given a verbal or written informed consent and signed a consent form before participating in the study. For participants who cannot read or write, the consent form was read for them and a co-worker or friend designated by the participant signed the consent form. Respondents were informed to decline any questions they found uncomfortable. Confidentiality was assured, under no circumstances was the questionnaires with identifiers shared with anyone not involved in the research. Once the information is entered into the main database, personal identifiers (names and workplace addresses) were removed. The electronic database was stored in password-protected computer.
Results
Demographic Characteristics of Respondents
A total of 516 respondents (238 in the formal and 278 in the informal sector) were surveyed. Four hundred and thirty-five (84.3%) were male, and the median age was 32.0 years (range: 12-67 years). The educational level was senior secondary 130 (25.2%), tertiary 122 (23.6%), and non-formal education 24 (4.7%). Also, the literacy level was 121 (23.4%) illiterate and 395 (76.6%) literates. Of the total, 365 (70.7%) had at least between 0 and 9 years of working experience. Occupation-wise, aluminium/metal work emerged as the dominant unit, 121 (23.4%), followed closely by automotive, 107 (20.7%), and hospitality, 98 (19.0%), with workers 278 (53.9%), indicating the labour-intensive nature of these industries. Of the 139 workplaces visited (66 in the formal and 73 in the informal sectors), 91 (65.5%) of the study subjects reported that solid waste is safely collected and disposed of accordingly. Also, 245 (47.5%) reported that there is a handwashing facility available in their workplaces, 76.9% in the formal sector of workplaces versus 22.3% in the informal sector of workplaces. Personal hygiene and comfort, such as showers and bathing areas, were reported by 320 (62.0%) of the study subjects in the workplace: 84.0% in the formal versus 43.2% in the informal sector. Additionally, 391 (75.8%) of the study subjects reported the availability of cloak/changing rooms, 92.0% in the formal sectors versus 61.9% in the informal sectors. Of the total, 56 (40.3%) of the workplaces by observation strictly followed hand hygiene practices, 75.8% of formal sector workers versus 8.2% of informal sector workers. Table 1. Demographics and hygiene practice of participants in the workplaces, Freetown, Sierra Leone).
Demographics and Hygiene Practice of Participants in the Workplaces, Freetown, Sierra Leone, n = 516.

Sex by KAP on OSH Level in the Workplaces
Figure 2 (Sex by KAP on OSH in the workplaces, 2023, Freetown, Sierra Leone) below illustrates gender disparities in OSH KAP. Adequate knowledge was found in 15.7% of females and 84.3% of males. A good attitude was held by 19.7% of females and 80.3% of males. Good practice was demonstrated by 23.9% of females and 84.3% of males, indicating notable gender-based differences for workplace safety and organisational culture. Policymakers have a role to play by enacting regulations that promote gender equality in the workplace and mandating comprehensive OSH education for all employees.
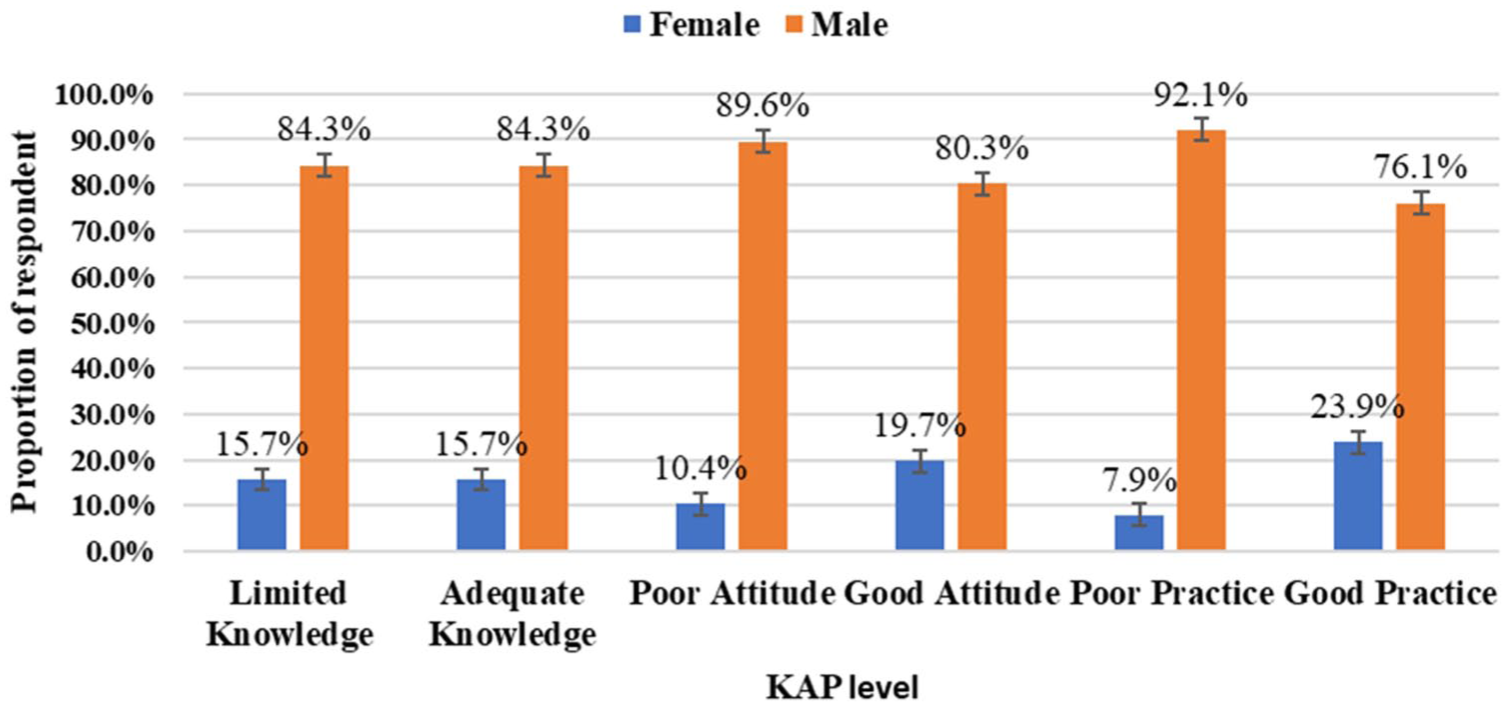
Sex by KAP on OSH in the workplaces, 2023, Freetown, Sierra Leone, n = 516.
Workplace Type by KAP Level in the Workplaces
The chart below with respondents of 238 in the formal sector and 278 in the informal sector shows that the formal sector had 144 (60.7%) with adequate knowledge and 109 (39.3%) in the informal sector had adequate knowledge. Also, 125 (45.1%) of them in the informal sector had a good attitude, and 131 (54.9%) in the formal sector had a good attitude. Furthermore, 63 (22.7%) of respondents in the informal sector had good practices, and 184 (77.3%) in the formal sector have good practices on OSH measures (Figure 3. Types of workplaces by KAP on OSH level).

Types of workplaces by KAP on OSH level, n = 516.
Prevention and Precautional Strategies by Knowledge and Practice Level
Out of the total 516 respondents, 61.8% had adequate knowledge on national OSH policy, 94.8% of them had adequate knowledge on health and safety measures, 65.5% had adequate knowledge on safety signs and symbols, and 98.5% had adequate knowledge on the health Effects related to the job. Of the 516 respondents, 64.9% had good practices on safety signs/warnings, 62.9% had good practices on accident investigation and reporting, and 68.9% had good practices on health and safety monitoring or audits. 86.5% had good practices on first aid or medical services availability, and 96.4% had good practices on cloak/changing room availability. (Table 2. below: Prevention and precautional strategies by Knowledge and Practice on OSH in the workplaces).
Prevention and Precautional Strategies By Knowledge and Practice on OSH in the Workplaces, n = 516.

Bivariate Analysis of Factors Associated With OSH Measures by Sex and Educational Level
The study finding shows that the odds of adequate knowledge among males is 1.0 times, showing no significant difference compared to females (cOR = 1.0; 95%CI: 0.63-1.62, P = .98). However, the odds of poor attitude among males were 2.1 times higher compared to females (cOR = 2.1; 95%CI: 1.25-3.54, P < .005). Also, the odds of poor practices among males were 3.7 times higher compared to females (cOR = 3.7; 95%CI: 2.15-6.21, P < .001). The odds of adequate knowledge among workers with university education were 4.4 times higher compared to junior education (cOR = 4.4; 95%CI: 1.87-10.56, P < .001). The odds of a good attitude among workers with a university education were 2.3 times higher compared to junior education (cOR = 2.3; 95%CI: 1.02-5.18, P = .045). Also, the odds of good practices among workers with university education were 3.7 times higher compared to junior education (COR = 3.7; 95%CI: 1.63-8.54, P < .002). (Table 3. Analysis of Factors Associated with OSH Outcomes)
Analysis of Factors Associated with OSH Outcomes, n = 516.

Abbreviations: cOR, combine odds ratio; aOR, adjusted odds ratio; CI, confidence interval; Ref, reference category.
Statistical significance (P < .05) in the multivariate model.
Bivariate Analysis of Factors Associated With OSH Measures by Type of Workplaces and Job Position
The odds of limited knowledge in the informal sector were 3.5 times higher compared to the formal sector (cOR = 3.5; 95%CI: 2.44-5.06, P < .000). The odds of a good attitude in the formal sector were 2.3 times higher compared to the informal sector (cOR = 2.3; 95%CI: 1.62-3.33, P < .000). Moreover, the odds of poor practices in the informal sectors were 17.1 times higher compared to the formal sector (cOR = 17.1; 95%CI: 11.03-26.49, P < .000). The odds of adequate knowledge of workers were 1.3 times higher compared to apprentices (cOR = 1.3; 95%CI: 0.86-1.96, P = .21). The odds of a good attitude of managers/supervisors were 1.4 times higher compared to apprentices (cOR = 1.4; 95%CI: 0.85-2.16, P = .209). The odds of good practices of managers/supervisors are 0.5 times lower compared to apprentices (cOR = 0.5; 95%CI: 0.29-0.75, P < .002; Table 3. analysis of factors associated with osh outcomes).
Multivariate Analysis of Factors Associated With KAP on OSH in the Workplaces
Factors that were statistically significant at the bivariate level were chosen for multivariate analysis, and 12 were statistically significant in influencing knowledge, attitude, and practice in the workplaces. The study reveals that the odds of adequate knowledge among workers with university education were 3 times higher compared to those with no formal education (aOR = 3.0; 95%CI: 1.11, 10.40, P < .032). Additionally, the odds of adequate knowledge with vocational education were 6.6 times higher compared to no formal education (aOR = 6.6; 95%CI: 2.05, 21.51, P < .002). The odds of adequate knowledge of the formal sector were 2.4 times higher compared to the informal sector (aOR = 2.4; 95%CI: 1.43, 4.15, P < .001). The odds of the formal sector having good practices were 16 times higher compared to the informal sector (aOR = 16; 95%CI: 2.80, 95.81, P < .002). The odds of good practices of managers/supervisors were 9.7-time higher compared to apprentices (aOR = 9.7; 95%CI: 1.97, 47.83, P < .005; Table 3. analysis of factors associated with OSH outcomes).
Discussion
This study reveals critical disparities in Occupational safety and Health (OSH) knowledge, attitudes, and practices (KAP) between formal and informal sectors in Freetown, Sierra Leone, with significant implications for policy and workplace interventions.
This study of 516 Sierra Leonean workers (238 formal, 278 informal) revealed stark occupational health disparities. Majority of our respondents were male, median-aged (32 years) workforce showed higher illiteracy in informal sectors.23,31,33 High-risk occupations dominated by metalwork and automotive with inadequate safety oversight. 6 Critical infrastructure gaps emerged: only one-fifth of informal sectors had handwashing facilities versus majority of the formal sectors, 39 while hygiene amenities (showers, changing rooms) were 2 to 3 times more available in formal sectors. 54 Alarmingly, hand hygiene compliance was lower in informal sector reflecting systemic enforcement failures.33,55,56 Although more than half, practiced safe waste disposal, informal sector deficiencies in hazardous industries like metalwork pose significant environmental health risks. 57
According to our findings, the majority of workers in the study exhibited gender-based disparities in knowledge, attitude, and practice (KAP) regarding Occupational Safety and Health (OSH). In terms of knowledge, this study revealed that males and females had similar levels of OSH knowledge, as both genders had near-identical distributions in terms of having either limited or adequate knowledge. This finding aligns with similar research conducted in Ghana, which also found no significant gender difference in general OSH knowledge, although it did suggest that males had more access to training in male-dominated sectors such as mining and construction. 58 This study findings showed that males were more likely to exhibit poor attitudes towards OSH, being times more likely than females to have a negative attitude towards safety. This result was found in consistent with studies conducted in Nigeria, where males in high-risk occupations such as construction were more likely to have complacent attitudes towards safety regulations. 59 Additionally, a research conducted in Kenya suggested that females were more likely to display positive attitudes towards OSH, particularly in healthcare settings, where they showed greater concern for safety, possibly due to gendered perceptions of vulnerability. 60 The study revealed a substantial gender disparity, with males being more likely to exhibit poor safety practices. This finding is in line with studies conducted in Egypt and India, which found that male workers in construction and mining industries were more likely to disregard safety measures compared to females. This gender-based difference in practice could be attributed to traditional male roles in high-risk sectors, where risk-taking behaviours are often normalised.57,61
The study revealed substantial sectoral disparities in OSH knowledge, with formal sector workers demonstrating significantly better understanding than their informal sector counterparts. Over two-fourths of formal sector participants reported adequate OSH knowledge, 62 compared to substantially lower levels in informal workers. These findings align with research conducted in Ethiopia, which attributes the level of knowledge to education and links the gap in formal sectors to structured training systems and better resource allocation. 63 The knowledge deficit in informal sectors reflects systemic challenges in OSH training provision, as noted in South Africa, which documented limited exposure to safety programmes among informal workers.54,64 Importantly, educational attainment emerged as a critical predictor, with university-educated workers after adjustment showing greater odds of adequate knowledge, the finding is in support of a study conducted in Spain, which found the role of education in safety protocol understanding.61,65 These findings underscore the need for targeted knowledge interventions in informal sectors, particularly through accessible, low-literacy training programmes that address the specific needs of less-educated workers and apprentices. Workers also demonstrated better knowledge than apprentices, likely due to greater workplace experience. 66 Notably, gender analyses revealed no significant differences in knowledge levels, suggesting equitable access to basic OSH information across genders.56,58
Significant differences emerged in safety attitudes across sectors and demographic groups. Formal sector workers were more likely to exhibit positive OSH attitudes, contrasting with a study conducted in Indonesia shows findings about informal workers’ poor attitudes stemming from limited OSH understanding.64,67 Gender disparities were particularly striking, with males are more likely to hold negative attitudes, this was in consistent with studies linking male-dominated industries to risk-normalisation behaviours.60,68 Experienced workers demonstrated better attitudes than apprentices, highlighting the role of workplace tenure in safety culture development.69,70 These attitude patterns have important implications for intervention design, suggesting the need for gender-sensitive approaches that specifically target male workers in high-risk occupations and address the unique challenges of informal sector work environments. Behavioural change campaigns should leverage positive role models and peer influence to shift safety attitudes in these populations.
The most pronounced disparities emerged in actual safety practices, with informal sector workers showing alarmingly poor compliance. Informal workers were more likely to engage in unsafe practices than their formal sector counterparts, reflecting inadequate training and protective measures.54,67 Formal sector workers demonstrated higher odds of good practices, attributable to stronger regulatory oversight. 57 Gender differences were again significant, with males are more prone to unsafe practices than females, mirroring global trends in high-risk industries.61,64 A positive finding was participants’ relatively strong first aid knowledge, aligning with an observations made a study in Gaza and Iran.62,69,71 These practice patterns highlight the urgent need for practical, hands-on training interventions in informal sectors, coupled with improved access to personal protective equipment and safety infrastructure. Policy measures should focus on extending regulatory protections to informal workers while developing context-appropriate compliance strategies that account for the realities of informal work arrangements.
The ILO’s Decent Work Agenda and the WHO’s emphasis on universal health coverage for all workers. The study found a profound disparity in OSH knowledge, attitudes, and practices (KAP) between formal and informal sector workers,5,7,39,72 as starkly evidenced by the study findings where informal sector workers had 2-fold lower odds of adequate knowledge of OSH measures and 16-fold higher adjusted odds of poor OSH practices in the informal sector. These findings underscore a significant implementation gap, where global policies have not equitably translated into protective realities for a large portion of the workforce, particularly those in informal employment. This disconnect highlights that the primary challenge in this context is not a lack of international standards but rather systemic failures in localisation, enforcement, and resource allocation aligned with the specific vulnerabilities documented in this study. These global policies are defined by the normative frameworks of the International Labour Organisation (ILO), which promotes fundamental principles and decent work,4,7,73 and the World Health Organisation (WHO), which advocates for universal health coverage for all workers.74-76 Their perspectives converge on the principle of equitable protection for all workers.
The study revealed a severe deficit in basic safety infrastructure in the informal sector workplaces and significantly poorer safety practices, directly challenging the equitable realisation of these international agendas, underscoring a systemic failure in a low-resource setting and enforcement. 39
The operational focus of technical institutions further highlights this divergence between normative policy and on-ground reality. Workers in the informal sector often operate outside the purview of national labour laws and Ministry of Labour and Social Security (MLSS) oversight. While agencies like the European Agency for Safety and Health at Work (EU-OSHA) drive preventive strategies and the National Institute for Occupational Safety and Health (NIOSH) sets evidence-based limits,9,77 their influence is markedly absent in the informal economy, which operates in a regulatory void. 4 These institutions collectively shape a global policy agenda. The compounded vulnerabilities linked to employment status and gender, where female workers demonstrated notably lower levels of adequate knowledge and good practice, and education level further highlighted that current top-down frameworks are insufficient. Furthermore, the lack of social protection exacerbates the economic instability of informal work, leading individuals to prioritise their daily income over safety investments. Long-standing gender norms make these differences even worse by putting females in the most dangerous jobs with the least access to training or safety gear. 78
Therefore, for global standards to translate into protective realities, future institutional guidelines must pivot towards targeted, context-sensitive interventions that mandate inclusive regulatory coverage, invest in literacy-appropriate OSH training for the informal sector and female workers, and promote enforceable minimum standards on workplace infrastructure, thereby addressing the core inequities (social protection and gendered job segregation) documented in this study. 39
We acknowledge the temporal gap in the study period, and the manuscript submission date may not reflect the current condition of OSH in Sierra Leone. While OSH data reflects mid-2023 conditions, the core OSH challenges and structural factors identified likely remain relevant at that time, and a cross-sectional design captures a moment in time, not a trend.
Conclusion
This study highlights significant disparities in occupational safety and health between formal and informal sector workers in Freetown. Informal workers demonstrated poorer safety knowledge, attitudes, and practices, compounded by inadequate infrastructure and gender-based risk behaviours. Thus, we recommend developing tailored OSH training, gender-sensitive interventions, affordable PPE access, and strengthened informal sector oversight. These actions require a multi-stakeholder approach involving Ministry of Labour, Employers’ Federation, workers’ unions, and NGOs, UN like ILO) and addressing contextual challenges such as resource constraints in the informal sector.
Footnotes
Acknowledgements
The authors would like to thank the management and supervisors of the various workplaces we visited for their support and cooperation during the study. We also thank the workers who participated in the study for their time and valuable insights. Special thanks to the Occupational safety and Health Programme staff for their support and the Sierra Leone Research and Ethics Review Board for their guidance and approval.
Authors Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the principal investigator.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study’s data will be made available upon a reasonable written request to the corresponding author and the unidentified data will be shared.*