
Abstract
Canada's occupational health and safety (OHS) legislative frameworks describe the general rights and responsibilities of employers and employees to ensure safe workplaces. However, the extent to which these OHS frameworks recognize and safeguard reproductive health and fetal development remains understudied. Protections for reproductive health and fetal development were evaluated in OHS legislation, employment standards, and associated regulations across Canada's federal and 13 provincial/territorial jurisdictions by a policy analysis, supported by a sex and gender-based thematic and content analysis. OHS and reproductive health keyword frequencies were also determined. Three major themes were identified: (1) inconsistent recognition of workplace risks to reproductive health, (2) job modification, and (3) employer-mandated pregnancy leave. Our review found that workplace protections were generally limited to pregnancy, with little recognition of workplace risks to fertility, suggesting gaps in workplace protections for reproductive health and fetal development. We recommend contemporary reform of Canada's OHS legislation and regulations to support universal, comprehensive, and inclusive protections for reproductive health and fetal development for all workers, regardless of sex and pregnancy status.
Introduction
Occupational health and safety (OHS) legislation is framed to protect workers from hazards that can cause injuries and illnesses. 1 The International Labour Organization (ILO) recognizes several categories of workplace hazards, including biological, chemical, ergonomics, psychosocial, physical, and radiation, 2 all of which may adversely affect reproductive health and fetal development.3–12 It is well established that many occupational hazards may contribute to adverse pregnancy outcomes, such as preterm labor, spontaneous abortion, and stillbirth,3–8,10,11 while others can diminish semen quality.3–5,7,12 Agriculture, manufacturing, healthcare, laboratories, personal care salons, gas stations, and construction are among the workplace settings associated with exposures to developmental and reproductive hazards.3–12 Mechanisms of reproductive harm can include chemical toxicity, carcinogenesis of the urogenital tract, endocrine disruption, gene mutations, epigenetic alterations to DNA, oxidative stress, developmental toxicity, infection-induced inflammatory and immune-mediated tissue damage, as well as physical trauma-induced spontaneous abortion.3–10,12 Less explored are workplace influences on dysmenorrhea, exacerbation of menopausal symptoms, or sexual dysfunction.
In 2023, Canada's labor force was over 20 million, 47 percent of whom were women, with a national employment rate, defined in Canada as the share of the total population aged 15 years and older that is employed, of about 61 percent. 13 Canadian employment is divided between the services-producing sector (79.4 percent in 2023) and the goods-producing sector (20.6 percent in 2023). Leading services subsectors include wholesale and retail trade [14.4 percent] and healthcare and social assistance [13.3 percent]. Leading goods subsectors include manufacturing [9.1 percent] and construction [7.8 percent]). 13
Workplace health protections are mandated by federal and provincial/territorial OHS legislation. 14 Most Canadian workplaces are governed by local provincial/territorial OHS legislation and related employment standards. About 6 percent of Canadian workers are employed in federally regulated businesses that are governed by federal legislation.14,15 This includes federal government departments, federal crown corporations, companies, or sectors that operate across provincial or international borders, such as transportation, broadcasting and telecommunications, and banking.14,15 Canada's OHS legislation aligns with international standards and practices, as reflected in agreements such as the Canada-United States Regulatory Cooperation Council 16 and Canada's role as a founding member of the United Nations’ ILO. 17
According to the hierarchy of controls (HoC), employers should employ the following strategies (from most effective to least effective): elimination, substitution, engineering controls, administrative controls, and personal protective equipment (PPE) to protect workers’ health. 18 Psychosocial workplace hazard mitigation may be integrated into the classic HoC by integrating organizational strategies such as redesign of work systems, supervision and training policies, with individual actions proposed to accompany PPE use, including skills development and personal coping strategies. 19 Although understudied, psychosocial stress is identified among the occupational hazards associated with risk of spontaneous abortion, dysmenorrhea, and altered menstrual cycles.3,5 Employer responsibilities for workplace health and safety, including incident reporting, training requirements, and compliance with relevant regulations, are described in OHS legislation.2,14 Protections for reproductive health and fetal development in the workplace are an essential topic for Canadian OHS legislation, given that workers may experience both biological vulnerability and gendered exposures to hazards based on their occupational and gender roles in the workplace. The mechanisms and extent to which Canadian OHS law specifically addresses developmental and reproductive risks and mitigation strategies remain understudied. This study aimed to evaluate protections for reproductive health and fetal development in Canadian federal, provincial/territorial OHS, and related laws and regulations. Specifically, language related to reproductive and developmental hazards, and the scope of protections for fertility, pregnancy, and reproductive organ health were identified. Our findings have important implications for the modernization of Canadian OHS law to provide better safeguards for workers’ fertility and perinatal health, as well as to reduce risks of reproductive cancers and other occupational diseases.
Methods
Study Design
The design and analysis plan for our review of OHS protections for reproductive health and fetal development incorporated sex- and gender-based analysis plus (SGBA+)—a framework used in Canadian health research and policy to ensure inclusion of biological sex, gender, and other intersecting characteristics. 20 A policy analysis of multijurisdictional Canadian OHS and related law and regulations was performed by adopting the READ approach, a systematic procedure to ensure rigor in analyzing health policy documents. 21 The READ approach consists of four steps: (1) Readying the materials, (2) Extracting the data, (3) Analyzing the data, and (4) Distilling the findings. 21
Sample-Readying the Materials
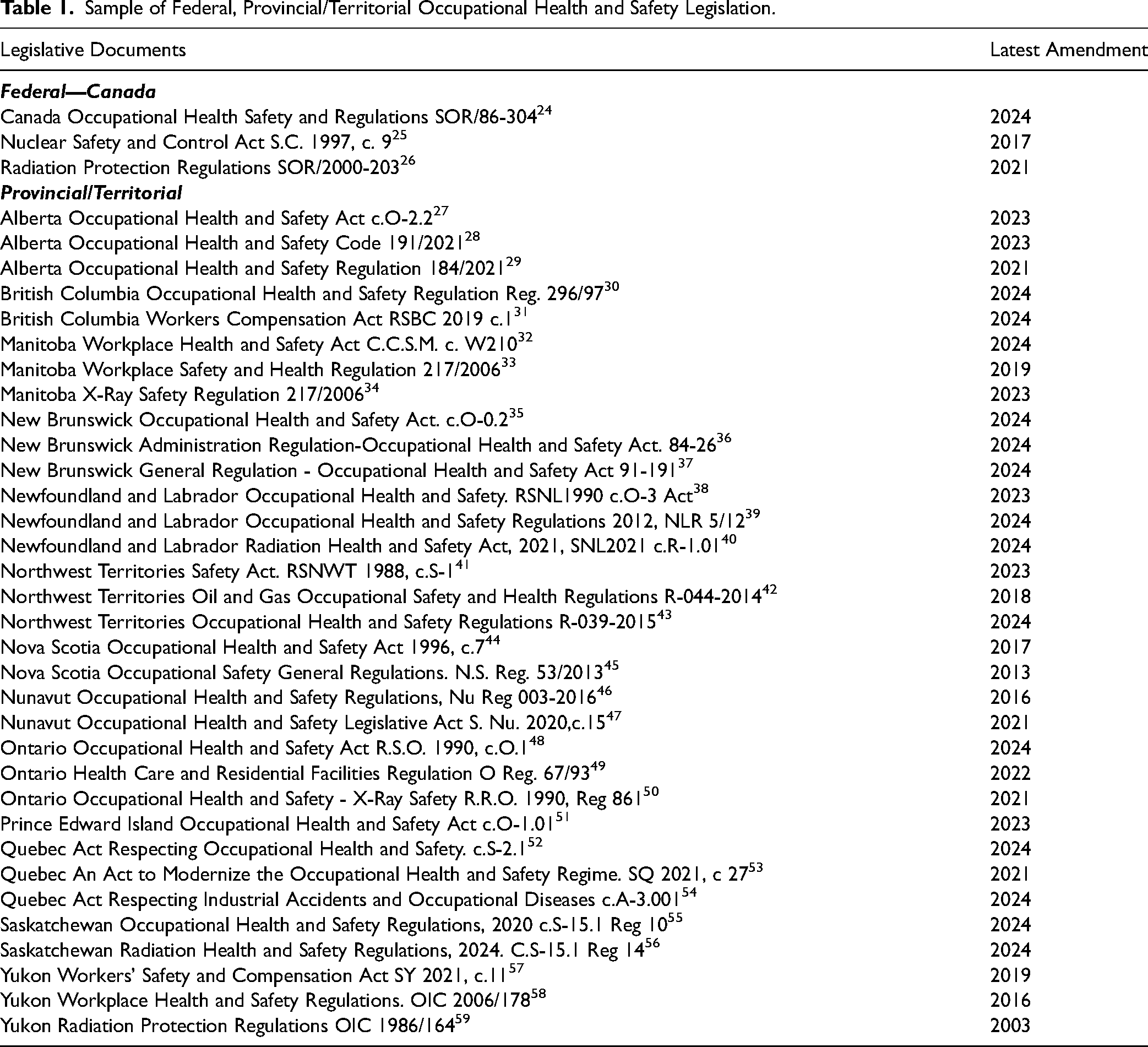
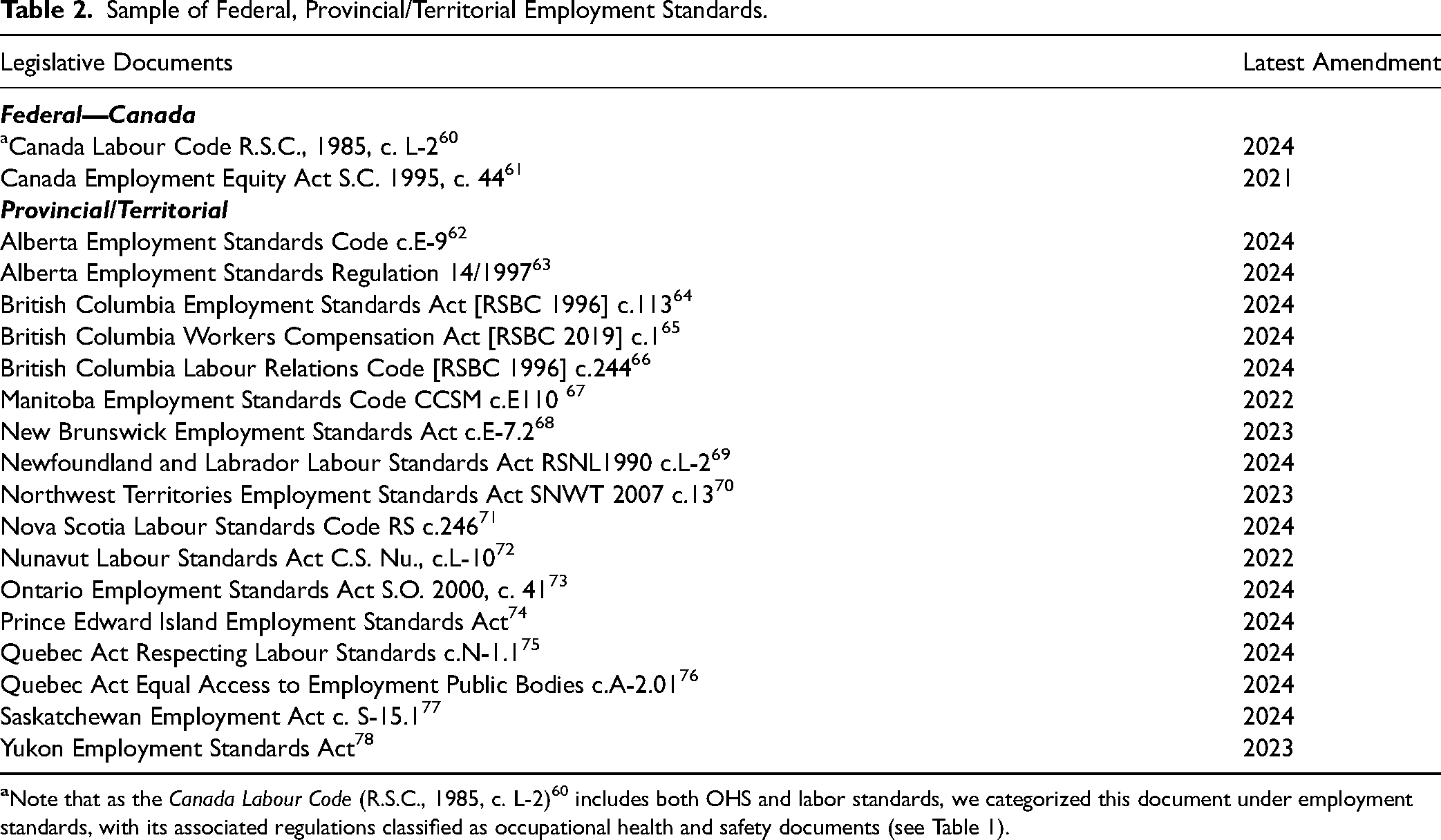
OHS legislation from the Canadian federal government and each province/territory formed the initial sample. Preliminary analysis of the initial sample of OHS legislation, along with consultation of provincial/territorial government websites and the Canadian Centre for Occupational Health and Safety (CCOHS)22,23 identified additional interrelated acts, regulations, and employment standards, which were subsequently included. The final sample included OHS acts, regulations (Table 1), and related employment standards (Table 2), organized by federal or provincial/territorial jurisdictions. Ethics approval was not required as these materials are in the public domain.
Sample of Federal, Provincial/Territorial Occupational Health and Safety Legislation.
Sample of Federal, Provincial/Territorial Employment Standards.
Data Extraction
Two health sciences reviewers (FJ and KPP) screened the sample using keywords to extract legislative text relevant to biological reproductive health outcomes consistent with our SGBA+ approach. 20 Keywords selected for this analysis included sex, gender, female/woman/women, male/man/men, fertility/infertility/sterility, pregnancy/pregnant, PPE—personal protective equipment, medical/treatment/first-aid, injury, bleeding, fetus/fetal, stillbirth, abortion/miscarriage, breastfeeding, pelvic/genital, birth defects, maternity/paternity/parental leave, job/duty modifications, and occupational disease.
Data Analysis and Distillation of Findings
The extracted text for each law or regulation was imported into (NVivoTM, QSR International Software, Burlington, Massachusetts, USA) and analyzed by the READ approach, 21 with thematic 79 and content analysis 80 used to identify major themes. Two researchers (FJ and KPP) performed the qualitative data analysis by coding extracted documents both deductively (related to keyword analysis) and inductively (deriving themes from patterns in the policy text). Codes were distilled into major themes and subthemes by consensus. Quebec legal materials were coded in both English and French by KPP. Evaluation of protections for reproductive health and fetal development by jurisdictional level (federal vs provincial/territorial) and type of legal material (e.g., OHS acts/regulations vs employment standards) was performed through keyword searches. For each jurisdiction, keywords relevant to major developmental and reproductive-related OHS topic areas were assessed across interrelated legal materials (i.e., OHS acts/regulations and employment standards) and scored as 1-topic present or 0-topic not addressed. Average proportional scores are presented for legislative type at either the federal or the provincial/territorial level.
Results
Our sample of legal documents included multiple interrelated OHS acts and regulations for each jurisdiction, typically accompanied by employment standards. More than half of the sample of English-language legal materials, across both federal and provincial/territorial jurisdictions, used gender-binary terms to describe pregnant workers (women, female, and she/her), pregnancy leave (maternity leave), and other gendered characterizations of employees. Three major themes emerged from our analysis: (1) inconsistent recognition of workplace risks to reproductive health, (2) job modification, and (3) employer-mandated pregnancy leave.
Inconsistent Recognition of Workplace Risks to Reproductive Health
The first major theme, inconsistent recognition of workplace risks to reproductive health, reflects our finding that the legal sample generally lacked references to specific workplace reproductive hazards, emphasized protections for pregnant workers, and typically did not recognize workplace risks to fertility (Figure 1).
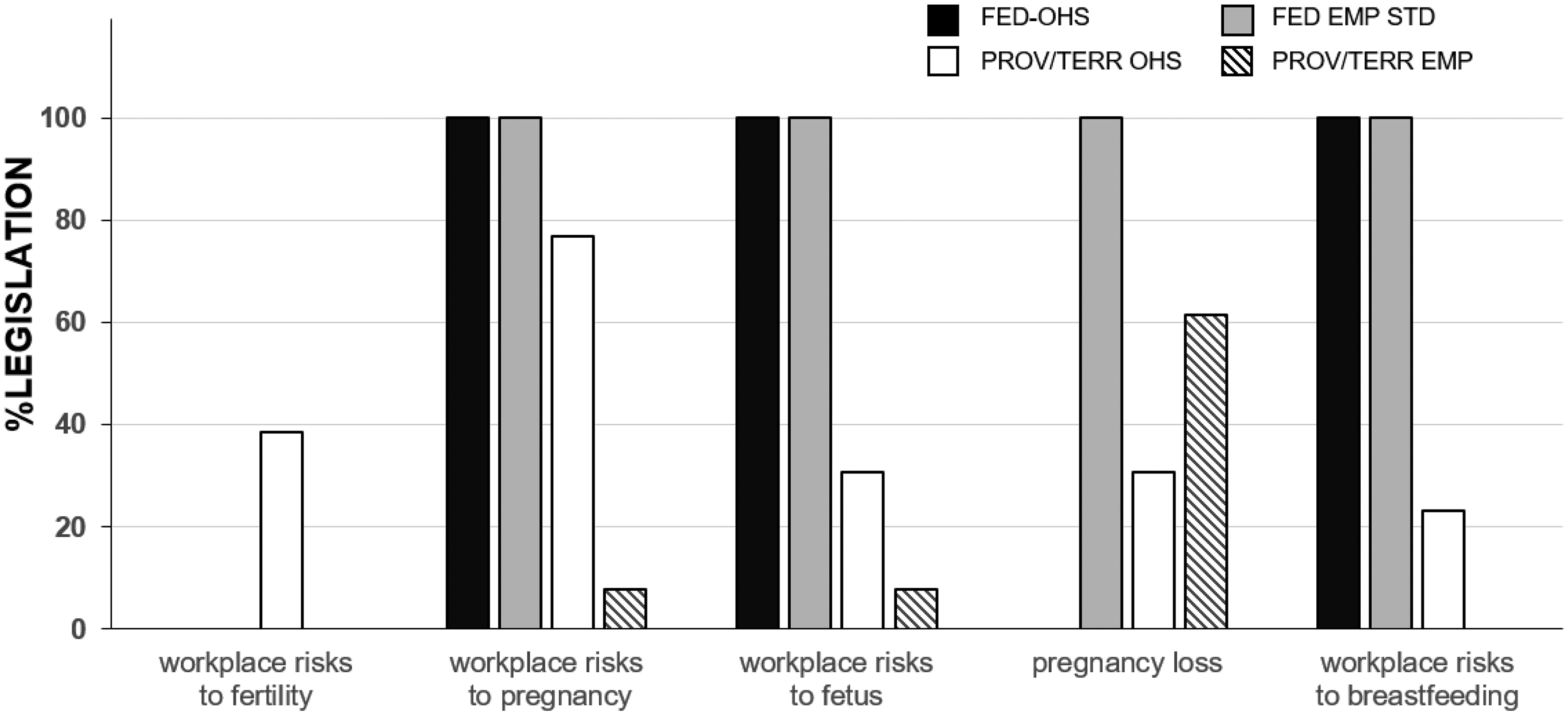
Canadian legislation reproductive health keyword analysis; shown, reproductive health keyword analysis was recognized in legislative documents evaluated. For each jurisdiction and legislation type, keyword analysis (1, present; 0, absent) was summed and presented as a proportion of the jurisdictional sample (e.g., federal vs 13 provinces/territories) (see Tables 1 and 2 for jurisdictional legislation groups). Abbreviations: FED-OHS, Federal occupational health and safety legislation; FED-EMP STD, Federal employment standards; PROV/TERR OHS (n = 13), occupational health and safety legislation from each province/territory; PROV/TERR EMP STD (n = 13), provincial/ territorial employment standards.
Exceptionally, the federal Radiation Protection Regulations did recognize the potential harms of radiation exposure on embryos, recognizing that even early pregnancy may be at risk:
Provision of Information. 7(2) Every licensee must inform each female nuclear energy worker, in writing, (a) of the risks associated with the exposure of embryos and fetuses to radiation and the risks to breastfed infants from the intake of nuclear substances; (b) of the importance of informing the licensee, as soon as feasible, in writing, that the female nuclear energy worker is pregnant or breastfeeding; (c) of the rights of a pregnant nuclear energy worker and the rights of a breastfeeding nuclear energy worker under section 11; and (d) of the applicable effective dose limits for pregnant nuclear energy workers prescribed by section 13. SOR/2020-237, s.7.
Both Ontario and British Columbia's OHS regulations more explicitly mention the possibility that workplace exposures may adversely affect fertility:
General Duty to Establish Measures and Procedures
9. (1) The employer shall reduce the measures and procedures for the health and safety of workers established under section 8 to writing, and such measures and procedures may deal with, but are not limited to, the following:
8. Measures to protect workers from exposure to a biological, chemical, or physical agent that is or may be a hazard to the reproductive capacity of a worker, the pregnancy of a worker, or the nursing of a child of a worker.
O. Reg. 67/93, s. 9.
Part 6- Substance Specific Requirements.
Reproductive toxins
6.47 If a worker is or may be exposed to a hazardous drug that is a reproductive toxin, an employer must develop
a written policy about the availability of protective reassignment, and a procedure for determining if protective reassignment is appropriate for workers who advise the employer of a pregnancy or an intent to conceive a child.
[en. B.C. Reg. 203/2023, s. 2.]
Reproductive health hazard protections specific to male biological sex were generally not found in OHS law; however, OHS acts from Saskachewan, 55 Northwest Territories, 43 and Nunavut 46 recognized “Male infertility resulting from exposure to glycol ethers, lead or pesticides” as “notifiable medical conditions resulting from occupational exposure,” with the same phrasing contained in appended Schedules. The sample of OHS legal material did not identify other reproductive hazards associated with infertility or mention female-factor infertility.
Workplace risks to pregnancy were recognized by federal law and by about three-quarters of provincial/territorial OHS acts/regulations. In contrast, workplace risks to the fetus and breastfeeding appeared less frequently, reflecting an apparent legislative emphasis on the pregnant workers’ rights and responsibilities in the context of employment. Across all jurisdictions, pregnant workers are required to inform their employer of their pregnancy, which subsequently results in the employer's assessment of the worker's ability to perform their job functions and the employer's duty to explore protective reassignment or job modifications.
Pregnant and Nursing Employees Cease to perform the job 132 (1) In addition to the rights conferred by section 128 and subject to this section, an employee who is pregnant or nursing may cease to perform her job if she believes that, by reason of the pregnancy or nursing, continuing any of her current job functions may pose a risk to her health or to that of the foetus or child. On being informed of the cessation, the employer, with the consent of the employee, shall notify the workplace committee or the health and safety representative. Consult a health care practitioner (2) The employee must consult with a health care practitioner, as defined in section 166, of her choice as soon as possible to establish whether continuing any of her current job functions poses a risk to her health or to that of the foetus or child. R.S., 1985, c. L-2, s. 132 R.S., 1985, c. 9 (1st Supp.), s. 4 2000, c. 20, s. 102018, c. 27, s. 441
81.5.1. Where there is a risk of termination of pregnancy or a risk to the health of the mother or the pregnant person or the unborn child, caused by the pregnancy and requiring a work stoppage, the employee is entitled to a special leave, without pay, for the duration indicated in the medical certificate attesting the existing risk and indicating the expected date of delivery. The leave is, where applicable, deemed to be the leave provided for in section 81.4 from the beginning of the fourth week preceding the expected date of delivery. 2002, c. 80, s. 36; 2022, c. 22, s. 165.
Part VI Occupational Health Requirements Hazardous substances 42. (10) Where a worker is exposed to a substance that is designated as a reproductive toxin or a sensitizer, an employer shall develop policy and procedures appropriate to the risk, which may include protective reassignment. 5/12 s42; 2019 c8 s20
Occupational illness/disease was defined by all jurisdictional OHS acts/regulations, but only three jurisdictions (Nunavut,
46
Northwest Territories,
43
and Saskatchewan
55
) explicitly described workplace-related pregnancy loss in OHS law, with the same phrase used by all three jurisdictions: “Spontaneous abortion resulting from exposure to ethylene oxide or antineoplastic drugs.” In contrast, respiratory disease/pathology associated with workplace exposures or injuries was described by 12 (92.3 percent) provincial/territorial and federal OHS jurisdictions. Pregnancy loss was included in federal and 8 (61.54 percent) provincial/territorial employment standards in the context of employee leaves (pregnancy, adoption, and miscarriage/stillbirth), but not in relation to workplace illness or injury.
81.1. An employee may be absent from work for five days at the birth of the employee's child, including a child born in the context of a surrogacy project, the adoption of a child, or where there is a termination of pregnancy in or after the twentieth week of pregnancy. The first two days of absence shall be remunerated. The employee must advise the employer of such an absence as soon as possible. 1990, c. 73, s. 34; 2002, c. 6, s. 236; 2002, c. 80, s. 31; 2005, c. 13, s. 83; 2018, c. 21 2018, c. 21, s. 321; 2023, c. 13 2023, c. 13, s. 561.
Respiratory Protection 12.13 (1) If there is a risk of injury or disease due to exposure to an oxygen-deficient atmosphere in a workplace, the employer must provide every person who is granted access to the workplace with respiratory protective equipment by means of which air will be supplied and that meets the following requirements…. SOR/2022-94, s. 4.
Employer Response to Workplace Risks to Pregnancy
Employer response to pregnant employees was captured by the second and third major themes, respectively: job modification and employer-mandated pregnancy leave. Canadian employers are required to provide employees with information about workplace risks to pregnancy, as described by federal law, and 9 (69.2 percent) provincial/territorial OHS acts/regulations (Figure 2).
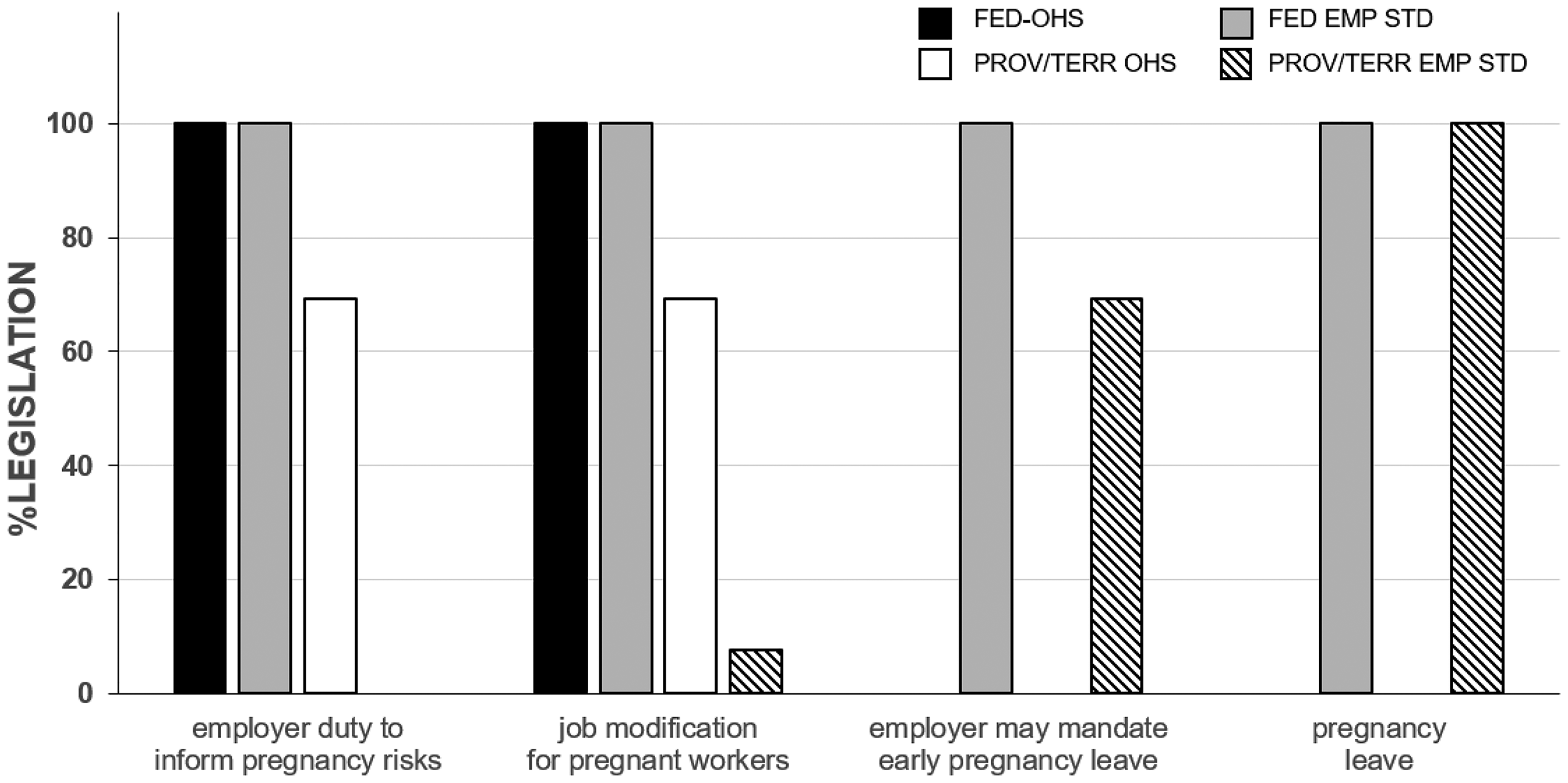
Canadian legislation pregnancy accommodation keyword analysis; shown, keyword analysis related to pregnant employees recognized in legislative documents evaluated. For each jurisdiction and legislation type, keyword analysis (1, present; 0, absent) was summed and presented as a proportion of the jurisdictional sample (e.g., federal vs 13 provinces/territories) (see Tables 1 and 2 for jurisdictional legislation groups). Abbreviation: FED-OHS, Federal occupational health and safety legislation; FED-EMP STD, Federal employment standards; PROV/TERR OHS (n = 13), occupational health and safety legislation from each province/territory; PROV/TERR EMP STD (n = 13), provincial/ territorial employment standards.
Pregnancy disclosure appears to be the regulatory prompt for the provision of relevant reproductive hazard information, discussions of job modifications, or protective reassignment. The second major theme, job modification, which also includes protective reassignment, describes employers’ responsibilities to minimize hazard exposure, and if necessary, reassign or modify the employee's duties to mitigate workplace risks to pregnancy. The language of these clauses framed job modification as employee-centered, with emphasis on reproductive risk reduction.
Pregnant or nursing workers
2.5 When a worker informs her employer that she is pregnant or nursing, the employer must
inform the worker of any known or foreseeable risk that conditions at the workplace pose or may pose to the safety or health of the worker or to her unborn or nursing child; and so far as is reasonably practicable,
take steps to minimize the exposure of the worker to the condition that creates the risk, or if alternate work is available that involves no risk or less risk and the worker is reasonably capable of performing that work, assign the worker temporarily to that alternative work without loss of pay or benefits.
Division VII Maternity-related Reassignment and Leave and Other Leaves Maternity-related Reassignment and Leave Reassignment and job modification 204 (1) An employee who is pregnant or nursing may, during the period from the beginning of the pregnancy to the end of the twenty-fourth week following the birth, request the employer to modify her job functions or reassign her to another job if, by reason of the pregnancy or nursing, continuing any of her current job functions may pose a risk to her health or to that of the foetus or child. R.S., 1985, c. L-2, s. 204; R.S., 1985, c. 9 (1st Supp.), s. 9; 1993, c. 42, s. 26; 2018, c. 27, s. 463. Employer's obligations 205 (1) An employer to whom a request has been made under subsection 204(1) shall examine the request in consultation with the employee and, where reasonably practicable, shall modify the employee's job functions or reassign her. R.S., 1985, c. L-2, s. 205; R.S., 1985, c. 9 (1st Supp.), s. 9; 1993, c. 42, s. 26; 2018, c. 27, s. 464.
In some cases, job modification clauses centered on the employer and the need for business continuity.
Pregnant and Breastfeeding Nuclear Energy Workers. 11 (1) On being informed by a female nuclear energy worker, in writing, that she is pregnant, the licensee must, to comply with section 13, make any accommodation that will not result in costs or business inconvenience constituting undue hardship to the licensee. (2) On being informed by a female nuclear energy worker, in writing, that she is breastfeeding an infant, the licensee must, to limit intakes of nuclear substances by the worker, make any accommodation to the working conditions that will not result in costs or business inconvenience constituting undue hardship to the licensee. SOR/2007-208, s. 8(F)SOR/2020-237, s. 11
Subdivision 11 Employment Leave Maternity leave 2-49 (4) An employer shall modify an employee's duties or reassign the employee to other duties, without a decrease in wages or benefits, to accommodate a pregnancy if:
the employee's duties or pregnancy would be unreasonably interfered with, and
it is reasonably practicable to do so. 2013, c.S-15.1, s.2-49; 2019, c 20, s.6.
Whereas OHS acts/regulations from the federal and all provincial/territorial jurisdictions included provisions on the right to refuse unsafe work—most (10 of 13) ensuring continuity of income and benefits during investigation—only Quebec, 52 Saskatchewan, 77 and Manitoba 32 explicitly guarantee maintenance of wages during pregnancy-related reassignment. All jurisdictional employment standards grant protected leave for pregnancy, typically with provisions for parental leave for the pregnant person's partner, adoption leave, and, in some cases, leave for miscarriage/stillbirth (Figure 2). Typically, pregnancy leave is initiated by the employee, commencing proximal to anticipated childbirth to optimize both recovery and newborn care/attachment.
The third major theme, employer-mandated pregnancy leave, referred to clauses in employment standards that enabled employers to mandate early pregnancy leave, rather than identify job modification/protective reassignment (Figure 2). In response to workplace risks to pregnancy, federal and 9 (69.23 percent) provincial/territorial employment standards permit employers to judge the feasibility of job modification and assign early pregnancy leave if job modification is not practical, often with emphasis on business continuity.
Prohibition 208 (1) Subject to subsection (2), no employer shall require an employee to take a leave of absence from employment because the employee is pregnant. Exception (2) An employer may require a pregnant employee to take a leave of absence from employment if the employee is unable to perform an essential function of her job and no appropriate alternative job is available for that employee. Length of leave (3) A pregnant employee who is unable to perform an essential function of her job and for whom no appropriate alternative job is available may be required to take a leave of absence from employment only for such time as she is unable to perform that essential function. Burden of proof (4) The burden of proving that a pregnant employee is unable to perform an essential function of her job rests with the employer. R.S., 1985, c. L-2, s. 208; R.S., 1985, c. 9 (1st Supp.), s. 10.
20. Entitlement Commencement of maternity leave (3) Where the pregnancy of an employee would unreasonably interfere with the performance of the employee's duties, the employer may require the employee to commence maternity leave not more than three months before the estimated date of birth.
1992,c.18,s.20; 2018,c.43,s.1.
Leave of absence without pay 43(4) An employer may, where no alternative employment is available, before or after commencement of the period referred to in subsection (1), require the employee to commence a leave of absence at the time when the duties of her position cannot reasonably be performed by a pregnant woman or the performance of the work of the employee is materially affected by the pregnancy. 1984, c.42, s.24; 1988, c.59, s.16; 1991, c.52, s.1; 2002, c.23, s.1; 2011, c.26, s.1; 2018, c.14, s.1; 2022, c.33, s.18
Although Quebec labor standards
75
require employers to modify duties or assign early pregnancy leave based on safety, exceptionally, these standards explicitly enable pregnant employees to contest reassignment or leave through the provision of medical certification that the workplace conditions are not dangerous.
81.8. From the sixth week preceding the expected date of delivery, the employer may, in writing, require a pregnant employee who is still at work to produce a medical certificate attesting that the employee is fit to work. If the employee refuses or neglects to produce the certificate within eight days, the employer may oblige the employee to take the leave provided for in section 81.4 immediately by sending the employee a written notice to that effect, giving reasons. 1990, c. 73, s. 34; 2022, c.22 2022, c. 22, s. 1681 DIVISION II RECOURSE AGAINST PROHIBITED PRACTICES 1990, c. 73, s. 54. 122. No employer or his agent may dismiss, suspend, or transfer an employee, practise discrimination, or take reprisals against the employee, or impose any other sanction upon the employee (4) on the ground that such employee is pregnant; An employer must, of his own initiative, transfer a pregnant employee if the conditions of employment are physically dangerous to the employee or the employee's unborn child. The employee may refuse the transfer by presenting a medical certificate attesting that the conditions of employment are not dangerous as alleged. 1979, c. 45, s. 122; 1980, c. 5, s. 10; 1982, c. 12, s. 5; 1990, c. 73, s. 55; 1995, c. 18, s. 95; 2002, c. 80, s. 61; 2011, c. 17, s. 56; 2014, c. 3, s. 3; 2013, c. 26, s. 134; I.N. 2014-07-01; I.N. 2016-01-01 (NCCP); 2016, c. 34, s. 44; 2017, c. 10, s. 28; 11 2017, c. 11, s. 1481; 2018, c. 21 2018, c. 21, s. 401; 2018, c. 23, s. 779; 2018, c. 12 2018, c. 12, s. 21; I.N. 2018-06-30; 2018, c. 23, s. 811; 2018, c. 13, s. 41; 2018, c. 8, s. 194; 2017, c. 27 2017, c. 27, s. 2021; 2020, c. 12 2020, c. 12, s. 1561; 2022, c. 22 2022, c. 22, s. 1761a; 2022, c. 17 2022, c. 17, s. 941; 2024, c. 4 2024, c. 4, s. 211; 2024, c. 6 2024, c. 6, s. 331; 2024, c. 21 2024, c. 21, s. 471
Discussion
Canada has a robust OHS legislative framework; however, adverse outcomes for reproductive health and fetal development are inconsistently addressed. Interrelated OHS acts, enforced by OHS regulations and accompanying employment standards, protect employee health in the federal, provincial, and territorial jurisdictions. Our findings show remarkable harmonization of OHS language and policy across Canadian jurisdictions to address general workplace injuries and risks to pregnancy. Employment standards across all jurisdictions grant pregnancy leave, and typically, parental leave for the nonpregnant parent, adoption leave, and leave in the event of pregnancy loss or stillbirth. Across our sample, legislative gaps in male reproductive health, workplace risks to fertility, and recognition of adverse pregnancy outcomes as occupational illness/disease were identified.
Absence of an Approach Specific to Reproductive Health and Fetal Development
As with most OHS legal approaches, Canadian law emphasizes the rights and responsibilities of workers and employers. Our sample of OHS legal materials mainly included protections for general occupational illnesses, injuries, and accidents, with limited coverage of well-established developmental and reproductive hazards in the workplace, including biological, chemical, and physical hazards, musculoskeletal strain, and overtime work.81,82 ILO recommends that OHS law address sex-specific workplace risks, while ensuring protective measures do not produce gender-based inequities related to employment opportunities or treatment. 82 Developmental and reproductive toxicity, primarily related to chemical hazards, and, to a lesser extent, biological and physical hazards, are categorized by WHMIS—the Workplace Hazardous Materials Information System. 83 OHS law across most jurisdictions integrates WHMIS/Safety Data Sheets (SDS) requirements regarding product labeling, information provision, and worker education,83,84 however, we identified no reinforcement of WHMIS related to workplace risks to pregnancy. Although WHMIS effectively addresses chemical hazards, we focused our analysis on Canadian OHS legislative materials to obtain a broader and comprehensive overview of workplace protections for reproductive health, reflecting the multifactorial nature of adverse outcomes. Legal measures addressing adverse developmental and reproductive outcomes associated with musculoskeletal injuries, certain physical hazards, and emerging biological and chemical hazards are needed to complement WHMIS's robust guidance on chemical safety. 83 ILO calls on member states to ensure that OHS legislation identifies workplace activities that may carry reproductive risks, including requirements for workplace-specific risk assessments. 82
Canadian OHS law requires the combined actions of both the employer and the worker to ensure safety in the workplace.14,15 Inevitable gaps between safety procedures and workers’ interpretations, judgements, actions, and practice of these procedures may adversely impact reproductive health. Even with robust OHS protections for pregnant workers, a Swiss study reported that maternity protection legislation was often not implemented in practice due to poor compliance or perceptions that safety measures were inadequate, leading workers to adapt or develop new strategies to better safeguard pregnancy. 85 It is incumbent on the employer to assess the gaps between procedure and practice routinely, and to provide regular education and training to address miscomprehension, skill deficits, or organizational barriers to OHS compliance. 86
Sex and Gender Considerations
It is well established that there is a paucity of research examining occupational exposures through the lens of biological sex, with mechanistic gaps evident in terms of individual hazards and adverse health outcomes. Health and safety reference standards for toxic exposures, for example, may use extrapolation or correction factors to adjust for presumed sex-based anatomical differences, failing to consider significant diversity of body size and related physiologies within biological sex groups. 87 Beyond workplace risks to pregnancy and reproductive health, our OHS legal sample did not address the impact of pregnancy on susceptibility to workplace illnesses or injuries such as musculoskeletal disorders. Nor did it address the interaction of pregnancy with exposures such as prolonged standing or heavy lifting.87–89
Although all Canadian OHS laws in our sample included requirements for PPE, none mentioned the need to ensure proper fit to the worker's anatomical size, nor the need to adapt PPE for body shape changes during pregnancy. British Columbia's OHS Guidelines, 90 a companion to aid the interpretation of the provincial OHS legislation, recognizes diverse anthropomorphic PPE fit issues that may restrict movement, entangle, or distract the worker, thereby increasing the risk for injury. PPE cannot simply be rescaled to adjust for size differences but must consider body shape and proportions.91,92 Ill-fitting PPE can fail to protect workers, and may also create hazards by reducing flexibility, dexterity, and requiring frequent adjustments.91,92 A study of Canadian female workers identified a lack of fit, discomfort, and inadequate selection of female-specific PPE, with pregnancy and breastfeeding sometimes prompting self-made alterations to PPE. 91 Safety head coverings and eye protection were reported as problematic due to limited size ranges and poor accommodation of diverse workers. Design constraints of available PPE failed to accommodate African American hair textures and hairstyles in head coverings, as well as anthropometric variation in facial dimensions and nasal bridge profiles for safety glasses. 91 PPE designed for larger male bodies may pose safety risks if not suitably tailored for smaller frames or users with different anthropometric profiles. Further, limited availability of gender-affirming uniforms and PPE fails to recognize user diversity, including trans and gender-diverse workers. 92 Examples to improve effective PPE use include offering PPE in a range of fits and sizes, providing protective gear suitable for diverse hair types and religious or cultural head coverings, and incorporating inclusive imagery and language in training materials. Although proper fit is paramount for safety and protection, an intersectional approach to the availability of PPE with respect to color options, fit, and design may increase PPE use and acceptability by workers of diverse gender identities, sexual orientations, and cultures. 92
Workplaces are often gender- segregated with respect to occupational roles and related risks. 88 The Committee of Experts on the Application of Conventions and Recommendations (CEACR) makes clear that protections based on stereotypical interpretations of gender roles violate principles of equality of opportunity and treatment. 93 ILO recommends that legislation be drafted in gender-neutral terms, avoiding gendered pronouns to reduce sexism, while recognizing that consideration of biological sex remains essential in the context of pregnancy. 82 Gender is associated with many employment conditions such as occupation, employment sector, and work arrangements—including part-time, full-time, or shiftwork—which may in turn influence exposure to occupational hazards, the resulting injuries and illnesses, and experiences of sexism and sexual harassment. 88 Although gendered hierarchies in the workplace may privilege men by affording greater power and compensation, 88 we found significant gaps related to men's reproductive risks in our sample of Canadian OHS legal materials, consistent with earlier studies. 94 In the absence of a fetus to protect, fertility protections may not be prioritized;94,95 aligning with our finding that fewer than 40 percent of provincial/territorial jurisdictions specifically address workplace risks to fertility. As many hazards that impair reproductive capacity may also pose risks for genitourinary and reproductive cancers, OHS legislation must consistently recognize reproductive workplace risks beyond pregnancy.
Pregnancy Disclosure
Pregnancy disclosure by the employee serves as the impetus for workplace pregnancy accommodations, though not explicitly required in our sample of Canadian OHS legal materials. By social convention, pregnancies are typically announced in the second trimester due to the high risk of pregnancy loss in the first trimester. This delayed communication can limit opportunities for workplace risk mitigation and early intervention, given the vulnerability of fetal development during the first trimester to developmental toxicants and spontaneous abortion.8,85 For workers who choose not to disclose their pregnancies, employers and coworkers may perceive such actions as deceptive, leading to psychosocial stress associated with the demands of secrecy and concealment.96,97 As many individuals maintain separate and distinct career/job identities from their personal lives, pregnancy disclosure requires the integration of worker and parental roles, which can create identity-role conflict.95–98 The requirement to disclose a pregnancy to access workplace protections may infringe on a worker's privacy concerning the timing and manner of the announcement, due to the intersection of personal and professional social networks.96,99 Universal OHS strategies that safeguard reproductive health and fetal development for all workers could reduce the need for pregnancy and medical disclosures.
Many workers face gender-based discrimination, further exacerbated by pregnancy disclosure, which creates barriers to career progression, biased performance reviews, loss of benefits, bonuses, and other career opportunities, and, as discussed below, unwanted job modifications.85,96,98,100,101 Gender-based discrimination may discourage pregnant employees from refusing unsafe work or requesting mitigation of occupational pregnancy hazards due to fears that pregnancy-related accommodations could hinder career opportunities and advancement. 93 Pregnancy can perpetuate gender stereotypes and sexism, leading to perceptions from colleagues and supervisors that the pregnant worker is less productive, inefficient, and less engaged as a team member.97,98,101 By classifying pregnant and breastfeeding women as “vulnerable,” together with disabled and elderly workers, ILO's language perpetuates these stereotypes. 82 Although OHS law from the European Union (EU) similarly describes pregnant workers as “vulnerable,” it explicitly distinguishes pregnancy from “illness.” 102
Worker identity may influence the timing and decisions around pregnancy disclosure. For sexual and gender minorities, pregnancy disclosure may render workers vulnerable to homophobia and transphobia, harassment, and discrimination. 103 We noted that multiple documents in our sample used gender-binary terms, which can be perceived as prejudicial and inherently exclusionary. Although the ILO promotes equality and inclusive workplaces for sexual and gender minorities, emphasizing respect, dignity, and human rights,93,104 it does not specifically provide guidance regarding workplace pregnancy disclosures or accommodations for these workers.
For pregnant migrant or undocumented workers, legal status and job insecurity may also influence decisions to disclose pregnancy status and request workplace accommodations. Migrant workers to Canada, also termed “temporary foreign workers” or “seasonal workers,” face numerous challenges in the workplace, including language barriers, social isolation, lack of access to healthcare, xenophobia/racism, and violations of their rights.105,106 Undocumented workers are often employed in temporary or unstable jobs, with poor remuneration and in workplaces with typically little to no compliance with OHS and labor standards.82,107 Pregnant migrant workers are particularly vulnerable as their access to health services in Canada is dependent on their work visa or permit.105,106 Undocumented workers in Montreal, Canada, reported that pregnancy threatened their job security, and created financial instability given their lack of pregnancy-related benefits. 107 ILO explicitly recognizes the vulnerability of migrant and foreign national workers, affirming their dignity, freedom from discrimination, and right to safe workplaces. 82 Social hazards such as workplace harassment, stigma, and discrimination can prevent marginalized workers from exercising their rights to OHS training, pregnancy protections, and prevention. 104
Job Modifications/Preventative Leave
The right to refuse unsafe work is a core tenet of Canadian OHS, 108 described throughout our sample of materials, with most jurisdictions affirming that redeployment or accommodations should not result in loss of wages. Work can be made safe for most pregnant employees, with many able to carry out their responsibilities throughout pregnancy.9,100 Job modifications are used by Canadian federal and most provincial/territorial OHS legislation as a strategy to protect pregnant workers from workplace risks, consistent with international conventions.81,93 Most pregnancy accommodations such as schedule modifications, more frequent breaks for resting or use of bathroom facilities, and simple physical adaptations related to prolonged sitting or standing may have little to no added expense for the employer. 109
In the United States, the Pregnant Workers Fairness Act (PWFA), 110 and its implementing regulations, 111 provide for accommodations including job restructuring or temporary suspension of one or more essential functions for pregnancy, childbirth, and related medical conditions. The PWFA 110 broadens “pregnancy” to include current, past, potential, or intended pregnancy, in addition to explicit mention of infertility and fertility treatments. The PWFA regulations 111 define “related medical conditions” with a nonexhaustive list which includes complications of pregnancy or childbirth; adverse health outcomes associated with pregnancy termination; antenatal mental health conditions; vaginal bleeding and menstruation; and lactation-related conditions. The PWFA regulations provide examples of workplace accommodations to reduce or prevent occupational risks, including avoidance of hazardous chemical exposures, assistance with manual labor, additional rest breaks, and provision of seating, with the caveat that these accommodations should not cause the employer “undue hardship.”109–111 Canadian legislation uses similar language to require employers to accommodate pregnancy if these measures are “reasonably practical.” Policy divergence is evident with respect to mandatory early pregnancy leave provisions. Whereas Canadian federal and most provincial/territorial employment standards allow employers to mandate early pregnancy leave if job modifications are deemed unfeasible, too costly, or otherwise disruptive to the workplace, this provision is not included in the US PWFA.109–111
Healthcare providers play an essential role in pregnancy evaluation and are often called upon to provide information and resources for risk assessment and mitigation options.100,112 In the absence of suitable job modifications, sick leave is a strategy used by pregnant workers to accommodate musculoskeletal and other physical stresses.98,112 Appropriate occupational risk assessments and customized job modifications can reduce pregnant employee absenteeism and may extend the period of work before pregnancy leave.98,99 For high-risk pregnancies or jobs involving exposures to developmental and reproductive hazards, healthcare providers may recommend specific workplace accommodations or extended medical or preventative leave.100,112 A narrative review of Canadian and European implementation of maternity protection legislation suggests that workers may opt for early pregnancy leave rather than job modification, perceiving leave to be the safest choice for the pregnancy. 99 Employers cited significant economic and organizational challenges associated with pregnancy-related job modifications, preferring the advantages of preventative leave, such as the ability to hire nonpregnant replacement workers, or the availability of government welfare-coverage for employees on leave.99,112
As discussed, for some pregnant workers, job modifications may hinder career advancement. 97 Discourse about pregnancy and workplace risks is framed in terms of “protections,” with often greater emphasis on the developing fetus than the pregnant employee. 94 Pregnant workers may avoid requesting job modifications to reduce negative career impacts and to prevent discrimination from both employers and coworkers. 98 Frequent absenteeism due to medical appointments or temporary leave can also contribute to resentment among colleagues who assume additional responsibilities, further contributing to gender-based and pregnancy discrimination.98,112 Although intended to mitigate workplace risks to pregnancy, preventative leaves may unintentionally reinforce gender-based segregation of occupational roles by removing women from the workplace. 99 Since pregnancy/parental leaves are typically renumerated at less than 100 percent of salary and may have a finite duration, preventative leave not only results in financial loss 99 but also, by beginning before birth, reduces the time available for parent–infant bonding before returning to work. 100 In Canada, most pregnant workers placed on preventative leave receive income through Employment Insurance (EI), which provides up to 55 percent of earnings during standard maternity and parental leaves across all jurisdictions except Quebec. 113 The Quebec Parental Insurance Plan (QPIP) provides 55 to 75 percent income replacement for standard parental leave. 114 In both programs, income replacement is reduced to 33 percent for extended leaves, with defined maximum leave durations for each parent.113,114 While some employers may supplement pregnancy or parental leave benefits, preventative leave may still compel workers to choose between partial financial loss or reduced postnatal leave, potentially limiting leave available to the co-parent. Thus, preventative leave policies create conflict between fetal health protections and equal opportunities for pregnant workers. 94 Workplaces that are made safe for pregnant workers would eliminate this policy misalignment.
To summarize, there are several consequences of job modifications that can impact job stability and career advancement. Reassignment can reduce opportunities for skills development and experience in a specialized role working with technologies, equipment, or personnel, which later could hinder career advancement. Accommodations might require coworkers to assume additional responsibilities, contributing to workplace discrimination. Job modifications can be associated with income loss, lack of eligibility for overtime, or bonuses. Preventative leave may result in changes to the gender dynamics of the workplace, particularly in male-dominated settings. For the pregnant worker, preventative leave can further exacerbate career and income stability, in addition to reducing pregnancy/parental leave postbirth and leave available for the co-parent.
In Canada, there is a range of legal, institutional, and workplace-based resources that, in some circumstances, can be used to protect employees adversely affected by pregnancy-reassignment or preventative leave. OHS legislation from most Canadian jurisdictions describes joint worker-employer health and safety committees, generally limited to workplaces with more than 20 employees.115–116 These committees provide formal mechanisms for employees to identify concerns about unsafe working conditions, potentially negating reliance on differentiated protections, which in this context, are OHS policies recognizing pregnant workers as a distinct group. 99 As described, Quebec, 52 Saskatchewan, 77 and Manitoba 32 guarantee maintenance of wages during pregnancy-related reassignment, which would ensure income stability for pregnant workers in these provinces. Similar measures are needed for all Canadian OHS jurisdictions, which would expand workplace protections for pregnant employees. For unionized workplaces, specific measures related to job modifications, preventative leave, and leave benefits associated with pregnancy may be described in collective bargaining agreements, with employees able to appeal or grieve employer decisions. 117 If disputes cannot be resolved at the workplace level, ultimately, employees may file a human rights complaint based on pregnancy-related workplace discrimination (grounds of sex, gender, or pregnancy) to their provincial/territorial or federal tribunals, depending on the workplace jurisdiction.117,118 All Canadian human rights laws, federal, provincial, and territorial, include provisions for the duty to accommodate with respect to prohibited grounds of discrimination, relevant here in the context of workplace protections for pregnancy.117,118 For most Canadian jurisdictions, pregnancy and childbirth are subsumed as protected grounds under “sex” or “gender” (Alberta), with pregnancy exceptionally recognized as a separate ground of discrimination in Quebec and Nunavut.117,118 It must be acknowledged that pregnant workers marginalized by precarious employment, limited formal education, poverty, and/or citizenship, for example, may have limited capacity or legal standing to pursue legal pathways to redress discriminatory workplace practices, including termination or loss of wages due to pregnancy redeployment or other accommodations. 106 Continued advocacy is needed to ensure equitable workplace protections for pregnant workers at the margins, particularly for undocumented and migrant workers.82,106
Policy Recommendations
Canada's lack of overarching federal OHS legislation and its 14 separate jurisdictions complicate protections for workplace safety, including reproductive health and fetal development. Despite independent, historical trajectories, the principles of OHS across provincial/territorial jurisdictions are remarkably similar.115,119 This is largely due to pan-Canadian unions, which have successfully lobbied for workers’ rights, and the adoption of WHMIS by federal and provincial/territorial jurisdictions, which provided a baseline for workers’ right to knowledge of workplace risks. 119 OHS harmonization was further advanced by the creation of the CCOHS in 1978, a tripartite institute which brings together governments, labor, and employers to promote workplace health and safety, facilitate interjurisdictional cooperation and labor participation, assist OHS policy and program development, and to serve as a national center for the collection, analysis, and evaluation of OHS data.115,119,120
ILO recommends a holistic approach for OHS legal protections for workers’ reproductive health, which includes pregnancy and parental leave, workplace accommodations for physical supports, rest and breastfeeding, and access to childcare. 83 Canada's OHS legislation and regulations align with ILO standards and can be characterized as “differentiated protection policies.”99,115 Differentiated protections,99,121 specifically intended to protect the developing fetus, may be ineffective due to the lack of early indicators of fetal neurotoxicity, developmental toxicity, or epigenetic effects of exposure to workplace hazards. It can also be argued that differentiated protections, such as pregnancy job modifications and leave policies, reinforce and exacerbate workplace discrimination against pregnant workers. 121 Further, given that many pregnancies are unplanned and that pregnancy discrimination may delay disclosure, it may be impossible to implement occupational risk assessments and appropriate accommodations early enough to prevent developmental toxicity. 98 Recognizing the limitations of differentiated protections in ensuring equal opportunity in the workplace, a universal approach to OHS may be a more appropriate strategy to safeguard reproductive health and fetal development for all workers.
A universal OHS strategy should recognize that all employees are biologically vulnerable to workplace exposures, injuries, and conditions that may impair fetal development, reproductive function, or cause disease of reproductive organs. This acknowledgement provides a strong prima facie rationale for universal protections in the workplace. OHS policy measures that eliminate, substitute, or control developmental and reproductive hazards would align with our evolving understanding that not only are the embryo and fetus sensitive to workplace exposures, but also the quality and viability of gametes. 9 Hazardous exposures before conception can contribute to adverse pregnancy outcomes, including congenital anomalies.9,11 OHS policies that reduce or prevent such hazardous exposures for all workers across the reproductive life course can decrease adverse outcomes for fetal development and reproductive health.
ILO categories of occupational injury or disease classifications do not currently include developmental and reproductive endpoints. 122 Integration of developmental and reproductive outcomes within the ILO classification scheme would provide international reference definitions to support surveillance, reporting, and comparisons across jurisdictions. Formal classification of such endpoints as reportable occupational injuries or diseases within a universal OHS framework could improve surveillance, enabling provincial/territorial and federal governments to prioritize research and allocate healthcare funding more effectively. Recognition of these endpoints as occupational injuries or disease by ILO and, in turn, provincial/territorial and federal OHS policies could further facilitate workplace injury and illness reporting, expand the content of employee education and training, and inform comprehensive risk mitigation and management. Such classification could also strengthen workers’ compensation claims related to injuries or diseases adversely affecting reproductive health and fetal development, thereby expanding workplace protections for all workers.
A broad and comprehensive perspective for the identification and characterization of developmental and reproductive hazards provides a foundation for a universal OHS framework. The Globally Harmonized System of Classification and Labelling of Chemicals (GHS) 123 is a risk classification scheme for chemical hazards implemented in Canada as WHMIS/SDS, 83 in the United States as Occupational Safety and Health Administration (OSHA)'s Hazard Communication Standard (29 CFR 1910.1200), 124 and in the EU as the Classification, Labelling and Packaging (CLP) Regulation ((EC) No 1272/2008). 125 The GHS includes germ cell mutagenicity and reproductive toxicity among the health hazard classes, 123 which aligns with our assertion that preconception exposures must be incorporated in a universal OHS strategy. The GHS also includes relevant hazard statements, including H360: may damage fertility or the unborn child; H361: suspected of damaging fertility or the unborn child; and H361d: Suspected of damaging the unborn child. 123 The phrase “classification not possible” is used when there is insufficient data/information to assess toxicity. 123 The German “MAK commission” 126 (Commission for the Investigation of Health Hazards of Chemical Compounds in the Work Area) similarly defines three pregnancy risk groups—group A: there is unequivocal evidence for damage to the embryo or fetus at occupational exposure limits; group B: damage to the embryo or fetus cannot be excluded; and, group C: damage to the embryo or fetus is unlikely. Recognizing that many chemicals have not yet been studied or classified in terms of developmental or reproductive endpoints, 127 the German MAK Commission defines a fourth pregnancy risk group, group D, to classify substances for which there is either insufficient or unavailable data for classification in groups A to C. 126 The Commission's Group D classification operationalizes the precautionary principle and is accepted as a model of transparency in risk assessment.128,129 To ensure protections for reproductive health and fetal development, and in alignment with best practices in occupational risk assessment, hazard characterization should account for multiple routes of exposure, including direct, incidental, and accidental, as well as temporal effects, recognizing that exposures may occur before conception, and in early pregnancy. 129 Reduction or elimination of the sources of developmental and reproductive hazards in the workplace depends on evidence-based hazard identification and risk characterization, which is particularly important for novel and engineered materials.
As risk characterization and exposure science evolve, we now understand that some chemicals can cause adverse health effects at very low doses, may accumulate in the body over repeated exposures, or interact to form chemical mixtures. 127 Adaptation of frameworks such as the Threshold of Toxicological Concern, a risk assessment model that defines chemical exposure levels below which human health risks are minimal, has been proposed as a relevant approach for fertility and developmental endpoints, applying conservative uncertainty factors (∼100).130–132 A recent review of European occupational exposure limits reported that developmental and reproductive endpoints are not always the most conservative basis for threshold-based approaches, with adverse health effects sometimes occurring below reproductive toxicity thresholds. 128 Application of evidence-based hazard thresholds to safeguard reproductive health and fetal development in the workplace, supported by the precautionary principle where necessary, would reduce reliance on differentiated protections.
There is support for broad, comprehensive OHS strategies to ensure reproductive health and optimize fetal development for all workers.99,121,129 Differentiated protections could be used as exceptions rather than standard practice, with more specific guidance available in workplaces with potential or known developmental and reproductive hazards.99,121 A universal approach would operationalize the ILO's principle of equal opportunity, 93 recognizing that all workers experience biological vulnerabilities to developmental and reproductive hazards and therefore share responsibility for workplace health and safety. In large workplaces, implementing universal OHS protections may yield financial and operational efficiencies compared with individualized accommodations, given that multiple employees may simultaneously be trying to conceive, be pregnant, or be breastfeeding. Moreover, universal protections for reproductive health and fetal development avoid the privacy challenges associated with pregnancy disclosure, since comprehensive hazard mitigation would not rely on individual accommodations. A universal OHS strategy that integrates broad, comprehensive hazard identification and risk management, guided by exposure science and the precautionary principle, would reduce workplace exposures, thereby decreasing adverse outcomes related to reproductive health and fetal development. It must be acknowledged, however, that in many workplaces, developmental and reproductive hazards have yet to be fully characterized, making the elimination of all such hazards challenging. For occupational settings involved in the production and handling of novel chemicals, emerging biological agents, and engineered materials, the application of the precautionary principle and targeted differentiated protections may still be necessary to safeguard employee health. Creating a universal framework for harmonizing protections against developmental and reproductive hazards across Canada's 14 OHS jurisdictions would require coordinated legislative amendments. As with previous consolidation efforts, this process would also require the engagement of pan-Canadian labor movements and commitments from local and federal governments.115,119
Strengths and Limitations
The strengths of our study include our multijurisdictional approach to evaluate a broad sample of Canadian OHS and employment standards using an SGBA + lens. However, we acknowledge several limitations to this work. First, the legislation and regulations in our sample will continue to evolve, informed by relevant Canadian legislation as well as international labor policies. Second, the limited scope of our evaluation did not permit us to evaluate legislation, such as WHMIS, that was referenced within OHS legislation. Further research is required to evaluate workplace implementation of WHMIS, given its explicit categorization of developmental and reproductive hazards. Third, because we did not apply an OHS-specific framework, such as HoC, to guide our policy analysis, our keyword search may not have systematically captured higher-level controls (e.g., elimination, substitution, or engineering controls) relevant to protections for reproductive health and fetal development. We focused on lower-level measures (PPE and administrative controls), as these are often applied to individual workers, and are more likely to incorporate sex- or pregnancy-specific considerations. Finally, we did not review complementary guidelines or procedures that help employees and employers interpret and apply OHS legislation and employment standards. Given the complexity of Canada's 14 OHS jurisdictions, an interdisciplinary legal analysis of all relevant Canadian OHS legislation, regulations, and related policies, together with their alignments with international agreements, is required for a full understanding of protections for reproductive health and fetal development, and to identify opportunities for harmonization.
Conclusion
Canadian OHS legislation, regulations, and employment standards broadly address workplace risks during pregnancy, outlining job modifications and preventative leave as risk mitigation options. However, adverse developmental and reproductive outcomes, including injury or disease to the reproductive organs resulting in infertility, miscarriage, or reproductive cancers, remain poorly recognized as endpoints of occupational exposures. To advance principles of equality of opportunity and treatment, we recommend the modernization of Canadian OHS legislative and regulatory frameworks to support universal, comprehensive, and inclusive protections for reproductive health and fetal development for all workers, regardless of sex or pregnancy status.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.