
Abstract
Climate change represents an unprecedented global public health crisis with extensive and profound implications. The Lancet Commission identified it as the foremost health challenge of the 21st century. In 2015, air pollution alone caused approximately 9 million premature deaths worldwide. Climate change also exacerbates extreme weather events, displacement, mental health disorders, disease vectors, food insecurity, and malnutrition, particularly impacting vulnerable developing countries like Pakistan due to its agricultural reliance, diverse topography, and limited resources. This study assesses Pakistani medical students’ perceptions of climate change’s health impacts. Conducted in February 2024, a cross-sectional survey of 632 students using a standardized questionnaire was employed via online Google Forms. The questionnaire was validated and an Exploratory Factor Analysis identified seven subscales of environmental health consciousness. The mean participant age was 21.17 years, with a balanced gender distribution. Students showed high environmental health consciousness (Mean = 35.6, SD = 5.2), with 88% attributing climate change to human activities and 89.1% anticipating serious future health impacts. Significant concerns included air quality-related illness (91%), water-availability illness (86%), healthcare disruption (85%), cold-related illness (83%), and flooding-related displacement (87%). Psychological impacts were acknowledged by 68%. Household income, age, and gender were significant predictors. These results highlight the need for integrating climate change and health education into medical curricula to prepare future healthcare providers.
Plain Language Summary
This study aimed to understand how medical students in Pakistan perceive climate change and its impact on human health. With climate change posing a significant threat to public health, it’s crucial to assess how future healthcare professionals view this issue.
Climate change has become a pressing global concern, affecting various aspects of life, including health. Studies have shown that extreme weather events and environmental changes “can” lead to health problems. Pakistan, in particular, faces challenges due to its susceptibility to climate change and limited resources to tackle these issues.
The study involved a survey of 632 medical students from different academic years in Pakistan. Data was collected using online forms, and participants were asked about their perceptions and knowledge of climate change. Statistical analyses were conducted to explore relationships between demographic factors and students’ attitudes and knowledge.
Overall, the study found that most medical students had a positive attitude and good knowledge about climate change. Factors like age, gender, and family income influenced students’ perceptions. The findings underscore the importance of educating future healthcare professionals about climate change to address its health impacts effectively.
Medical students in Pakistan show a positive attitude and sufficient knowledge about climate change and its health effects. This highlights the importance of incorporating climate change education into medical curricula to prepare future doctors for addressing climate-related health challenges.
Introduction
Climate change stands as an unequivocal global public health crisis, with profound and far-reaching consequences that demand our immediate attention. Central to these consequences is global warming, a phenomenon primarily driven by human activities, particularly the extensive use of fossil fuels. This warming jeopardizes up to 30% of all plant and animal species, creating a perilous ripple effect through ecosystems. 1 The inaugural Lancet Commission underscored climate change as the paramount health threat of the 21st century. 2 Climate change exacerbates air pollution through various mechanisms. Rising temperatures enhance the formation of ground-level ozone, a key component of smog, linked to respiratory and cardiovascular diseases. Elevated temperatures also increase the emission of volatile organic compounds (VOCs) from vegetation and industrial sources, further contributing to ozone formation. 3 In 2015 alone, air pollution contributed to a staggering 9 million premature deaths. 4 Additionally, climate change impacts health through extreme weather events such as heatwaves, floods, droughts, and storms; it also indirectly affects health by causing displacement, mental health disorders, sociopsychological phenomena, the proliferation of disease vectors, food insecurity, and malnutrition.1,5 Most of these health issues disproportionately affect vulnerable developing nations 6 like Pakistan and may exacerbate global health inequalities.
Pakistan is particularly vulnerable to climate change due to its geographical location and reliance on rain-fed agriculture. The country’s diverse topography exposes it to extreme weather events like heatwaves, floods, and droughts. Economically, its dependence on agriculture—comprising a significant portion of its GDP and employment—makes it sensitive to climate shifts, affecting food security and public health. 7 Limited resources hinder Pakistan’s ability to effectively tackle these challenges. Recent studies highlight severe public health implications, with 44% of children experiencing growth stunting from malnutrition, directly linked to food insecurity exacerbated by climate variability. This underscores the urgent need for climate adaptation and public health strategies. 8
Despite the pressing nature of these issues, climate change remains underrepresented in scientific and policy discourse, creating a critical gap in addressing its staggering implications for human health. 9 Health professionals, as trusted advocates, are poised to play a pivotal role in addressing the impact of climate change on human health. Their knowledge and understanding are essential for global climate action. 1 Medical students, as the future healthcare workforce, are particularly important in this regard, yet there is a noticeable gap in research concentrating on their viewpoints. Assessing medical students’ perceptions of climate change is crucial, as they are at the forefront of future healthcare provision and will significantly influence public health strategies and policy development.
Understanding medical students’ awareness of climate change can inform educational curricula and public health campaigns, ensuring that future healthcare professionals are well-equipped to address climate-related health issues. Therefore, this study aims to address this disparity by examining the viewpoints of Pakistani medical students regarding the impact of climate change on human health, with a particular focus on the provinces of Punjab and Sindh. These areas face unique environmental challenges, including extreme weather events, rising temperatures, and water scarcity, which directly affect human health. This research not only fills a significant gap but also underscores the critical public health implications of climate change and the essential role of health professionals in mitigating its effects.
Methodology
Study design and participants
A cross-sectional survey was conducted among medical students in Pakistan, with approval obtained from the Institutional Review Board of Fazaia Ruth Pfau Medical College, Karachi (FRPMC). We focused on the provinces of Punjab and Sindh, which boast the highest concentration of medical institutes among the country’s four distinct regions. This decision was made to maximize the representativeness of our sample within the medical student population. The data collection was done in the month of Feb 2024. Students enrolled in MBBS (Bachelor of Medicine, Bachelor of Surgery) programs were included in the survey, as the focus was on future physicians. Students pursuing BDS (Bachelor of Dental Surgery) programs, nursing or other allied healthcare professions were excluded because the survey aimed to investigate aspects of medical student experiences that are more directly relevant to the practice of medicine. Participants were identified through convenient sampling methods. Online Google Forms were distributed via relevant medical school listservs to reach a broad range of students across the two provinces. All potential participants were informed about the study’s purpose and provided with the option to choose between anonymous and non-anonymous responses based on their comfort level. A total of 632 students met the eligibility criteria and were included in the study. We opted for a complete case analysis (all responses were retained without employing imputation methods).
Questionnaire development and validation
The standardized questionnaire utilized in this study was obtained with permission from the authors of the study, 1 aligning with our research objectives and the constructs to be measured. The questionnaire was translated into the National Language, Urdu, and was provided in both English and Urdu languages to eliminate any potential miscommunication and guarantee that all answers were provided after careful consideration. To ensure content validity, experts in the field were consulted to review the questionnaire for relevance, clarity, and comprehensiveness. Their feedback helped ensure that the questions adequately covered the intended constructs and were suitable for the target population. A pilot test was conducted by administering the questionnaire to a small sample of 20 individuals representing the target population. This pilot test aimed to identify potential issues, such as confusing or ambiguous questions, response options, or formatting problems. Feedback from pilot test participants was collected and analyzed. Based on this feedback, several changes were made to the questionnaire: ambiguous questions were rephrased for clarity, and formatting adjustments were made to enhance readability. These revisions ensured that the final questionnaire was clear, comprehensive, and user-friendly.
To ensure construct validity, the adapted 20-item questionnaire underwent an Exploratory Factor Analysis (EFA) to determine its underlying structure and ensure its relevance and clarity for our target population. The decision to run an EFA was driven by the need to validate the factor structure of the adapted questionnaire within our specific context and to uncover any latent constructs that may not have been identified in the parent study. EFA helps in understanding the dimensions underlying the responses and ensures that the items group together meaningfully, reflecting the constructs we aim to measure.
A sample of 300 participants responded to the full set of survey items. Principal Component Analysis (PCA) was chosen as the factor extraction method, identifying underlying factors that explain the common variance among the survey items. The suitability of the data for this technique was assessed using the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. The KMO measure yielded a value of 0.819, indicating strong sampling adequacy. Bartlett’s Test of Sphericity was statistically significant (χ2 = 2860.166, df = 210, P < .001), confirming that the correlations between variables in the dataset were significantly different from an identity matrix. These results collectively confirm the suitability of the data for factor analysis, supporting its use in identifying underlying constructs within the dataset.
To enhance the interpretability of the factors, orthogonal rotation (Varimax) was applied to ensure that factors are uncorrelated. Items were retained in the final questionnaire based on their factor loadings, with a predetermined threshold of 0.40. Items with low factor loadings or cross-loadings on multiple factors were scrutinized for potential removal or revision as shown in Supplemental Table 1. This iterative process aimed to ensure that each retained item clearly measured one specific construct related to medical students’ perceptions of climate change and its health impacts.
Following factor analysis, constructs were labeled and interpreted based on the content of the retained items and the underlying theoretical framework. This involved examining the items that loaded onto each factor and assigning meaningful labels to these factors, reflecting different dimensions of medical students’ perceptions. Finally, reliability of the reduced questionnaire with 18-items was assessed through internal consistency. Internal consistency was evaluated using Cronbach’s alpha coefficient, resulting in a coefficient of .76, suggesting a reasonably good level of internal consistency for the measurement instrument. Subsequently, the revised questionnaire, was administered to an additional 332 participants, resulting in a final sample size of 632 participants, inclusive of the initial 300. This expanded sample size further validates the findings and ensures the robustness of the identified factors.
Measures
We employed a comprehensive questionnaire to assess the perceptions of medical students regarding climate change and its impacts on human health. The initial section gauged socio-demographic characteristics of the population, including age, gender, medical year, and total household income. An Exploratory Factor Analysis (EFA) revealed seven distinct factors, each representing a different dimension of environmental health consciousness related to climate change (see Supplemental Table 2). These factors, referred to as subscales, are described as follows:
Subscale 1: attitudes toward climate change
This subscale addresses whether respondents view climate change as good or bad, and its perceived impact on human health. Responses were measured on a 6-point Likert scale ranging from 6 (“very bad”) to 1 (“very good”). This subscale consists of 2 items, with a total score ranging from 2 to 12.
Subscale 2: belief in anthropogenic climate change and controllability
This subscale involves items regarding the belief that climate change is mainly caused by human activities, the increase in global CO2 concentration over the past 250 years, and the controllability of climate change. Responses were measured with three options: Correct (scored as 1), Incorrect, and I don’t know. This subscale consists of 3 items, with a total score ranging from 0 to 3.
Subscale 3: prediction of future impacts
This subscale comprises items about the anticipated seriousness of climate change’s health impacts in the community, Pakistan, and globally over the next 20 years. Responses were measured on a 6-point Likert scale ranging from 6 (strongly agree) to 1 (strongly disagree). This subscale consists of 3 items, with a total score ranging from 3 to 18.
Subscale 4: awareness of climate change evidence
This subscale assesses knowledge about historical temperature increases and CO2 concentration levels. Responses were measured with three options: Correct (scored as 1), Incorrect, and I don’t know. This subscale consists of two items, with a total score ranging from 0 to 2.
Subscale 5: perception of climate change’s direct impact on health
This subscale includes items related to flooding-related displacement, disruption of healthcare services during extreme weather events, air quality-related illness, cold-related illness, water-availability illness, and other climate change health-related impacts. Responses were measured with three options: Yes (scored as 1), No, and I don’t know. This subscale consists of five items, with a total score ranging from 0 to 5.
Subscale 6: perception of infectious disease concerns
This subscale includes items on vector-borne infectious diseases and food-borne diseases. Responses were measured with three options: Yes (scored as 1), No, and I don’t know. This subscale consists of 2 items, with a total score ranging from 0 to 2.
Subscale 7: perception of mental health impacts
This subscale includes items related to mental health conditions due to climate change. Responses were measured with three options: Yes (scored as 1), No, and I don’t know. This subscale consists of 1 item, with a total score ranging from 0 to 1.
This comprehensive questionnaire provides a robust foundation for capturing the multifaceted perceptions and knowledge of medical students regarding climate change and its implications for human health.
Data analysis
Data analysis was performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). The data analysis for the study was conducted in several stages to ensure a thorough understanding of the participants’ perceptions and the relationships between demographic variables and climate change perceptions.
Descriptive statistics
Descriptive statistics were employed to summarize and present the results. Categorical items related to the sociodemographic profile of the participants were reported as counts with percentages. Additionally, for the perception of climate change, descriptive statistics were calculated for all seven subscales of the Perception of Climate Change Scale. These statistics included the percentage of the scores, mean scores, and standard deviations (SD). This analysis helped to summarize the central tendencies and dispersions of the scores on each subscale and the overall perception of climate change among medical students.
Inferential statistics
Non-parametric tests were employed to assess the relationships between demographic variables and the various subscales of climate change perceptions. Specifically, the Mann-Whitney U test and Kruskal-Wallis test were used due to the potential for non-normal distribution of scores. The Mann-Whitney U test was used to compare differences between two independent groups (eg, gender) on each subscale of climate change perceptions. The Kruskal-Wallis test was used to compare differences between more than two independent groups (eg, medical year, total household income) on each subscale of climate change perceptions.
Spearman correlation analysis
Additionally, Spearman’s rank-order correlation was employed. Given the ordinal nature of the data and potential non-linear relationships, Spearman’s correlation was chosen as it is less sensitive to outliers and does not assume normal distribution. This non-parametric method allowed for the assessment of monotonic relationships between the ranks of demographic factors (such as age, medical year, and total household income) and the perception scores across the seven subscales. These coefficients provide insights into the direction and strength of associations, helping to highlight how changes in demographic variables are associated with changes in climate change perceptions among medical students. This analysis complements the regression findings, offering a comprehensive view of the data’s relational structure.
Regression analysis
To further understand the relationships between demographic variables and perceptions of climate change, regression analysis was conducted. Specifically, multiple linear regression models were utilized to predict the total perception scores and subscale scores based on the participants’ demographic characteristics, including age, gender, medical year, and total household income. This analysis aimed to identify which demographic factors significantly contribute to variations in climate change perceptions among medical students. The regression models were assessed for assumptions such as linearity, homoscedasticity, and absence of multicollinearity. This approach allowed for a deeper exploration of the predictive power of each demographic variable in explaining the differences in climate change perception scores among the study participants.
Visualization
To visually represent the distribution of responses across various questions within the seven subscales, lateral stacked bar graphs were created.
For all statistical analyses, a significance level of P < .05 was adopted as the threshold for determining statistical significance. Any P-values below this threshold were considered statistically significant. This comprehensive data analysis approach ensures a robust understanding of the environmental health consciousness of medical students regarding the perceived impacts of climate change on human health.
Ethical considerations
The study obtained ethical approval from the Institutional Review Board (IRB) of FRPMC (Ref No: FRPMC-IRB-2024-33). The research adhered to ethical standards outlined in the Declaration of Helsinki of the World Medical Association for trials involving humans, as per the authors’ statements. The consent section contained a debriefing statement in the Google forms, promoting transparency and communication. They were fully informed about the study’s purpose, the voluntary nature of their participation, and the measures taken to protect their privacy and confidentiality. Participants were made aware of their right to withdraw from the study at any point without consequences. Data security measures were rigorously implemented to safeguard participant information. To ensure the privacy and confidentiality of participants, all data collected was de-identified and stored securely. Personal information such as names, contact details, or other identifiers was not linked to the collected data. Only the research team had access to the data, and any published results or reports would not contain any information that could identify individual participants. The data was stored on secure servers and password-protected computers.
Results
Socio-demographic characteristics
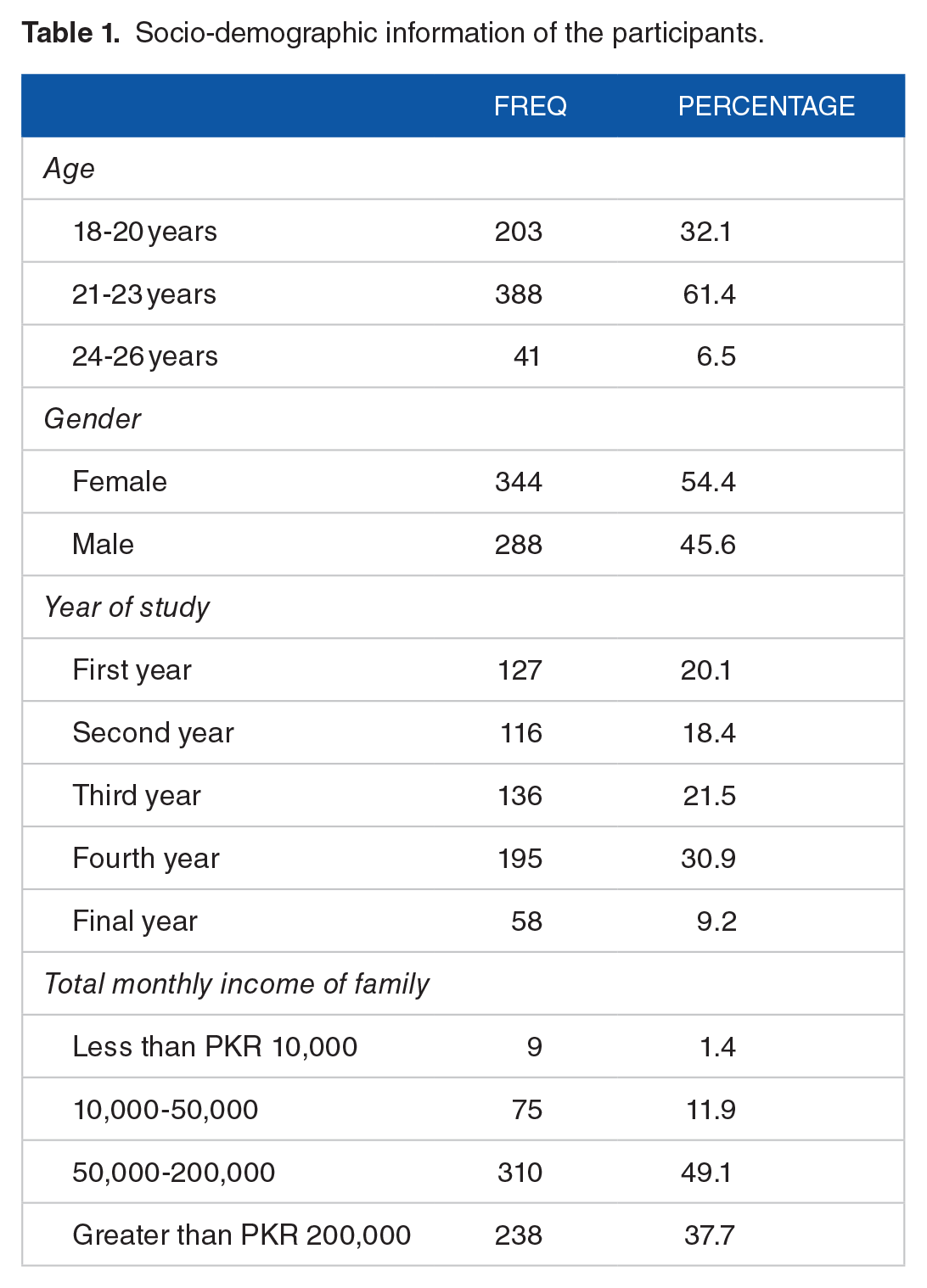
The study assessed the environmental health consciousness of medical students regarding the perceived impacts of climate change on human health. The socio-demographic characteristics of the study participants are presented in Table 1. The study participants (n = 632) exhibited a mean age of 21.173 years (SD = 1.6). Gender distribution was nearly balanced, with 54.4% identifying as female and 45.6% as male. Academic diversity was apparent, as students were distributed across various academic years, with the largest cohort in their fourth year (30.9%). Family income levels showed diversity, with 49.1% reporting incomes between PKR 50,000 to 200,000
Socio-demographic information of the participants.
Perception about climate change
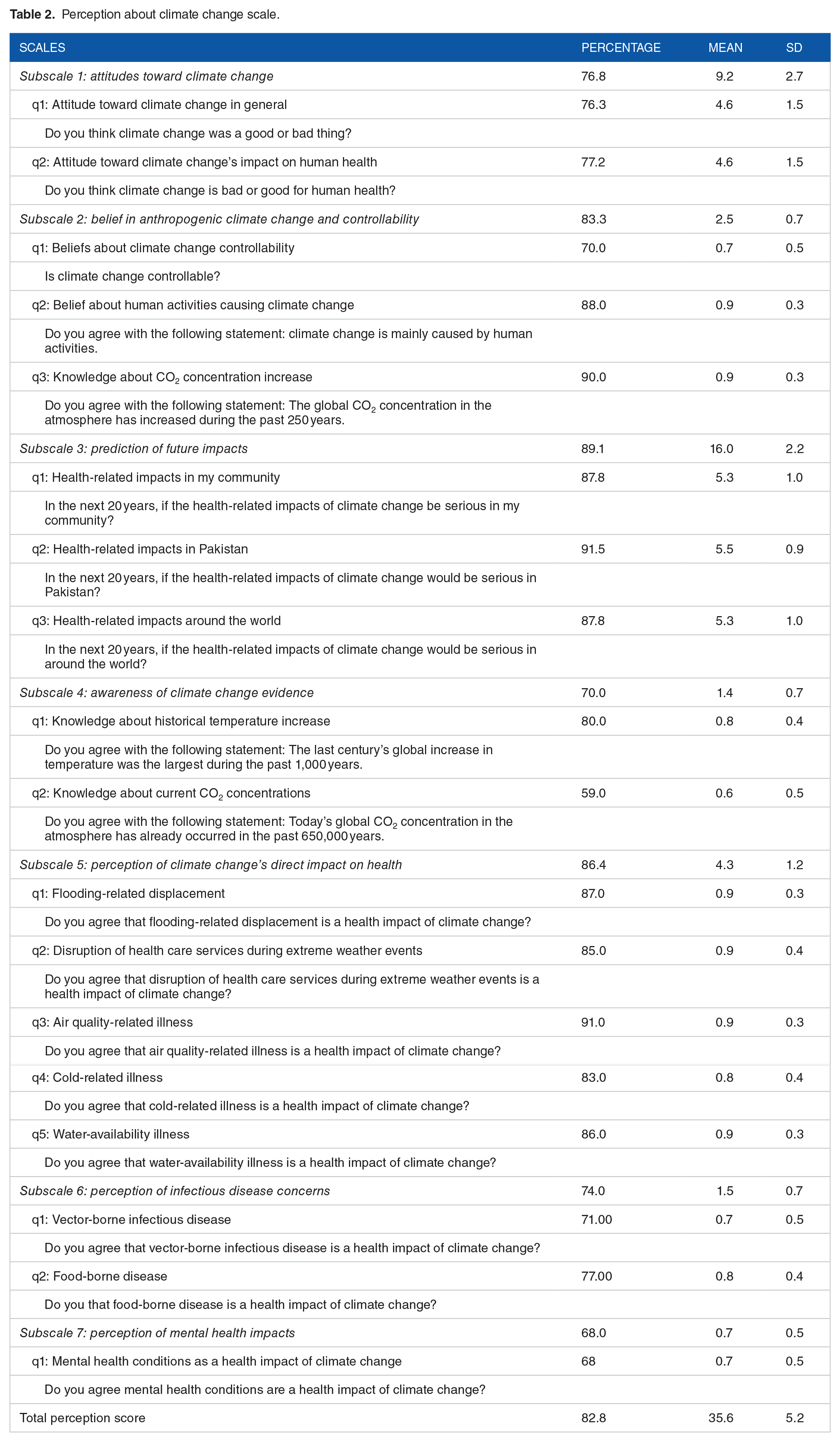
Table 2 provides a detailed overview of the student’s perceptions regarding climate change and its impacts on human health. The overall perception score, encompassing all subscales, was 35.6 (82.8%) with a standard deviation of 5.2. This composite score reflects an overall high level of consciousness and concern among medical students regarding the impacts of climate change on human health. The first subscale assessed general attitudes towards climate change (the responses are depicted in detail in Figure 1). The mean score was 9.2 with a standard deviation (SD) of 2.7, indicating a high level of awareness and concern. In terms of the belief that climate change is driven by human activities, the responses showed strong consensus, 88.0% agreed that climate change is mainly caused by human activities (the responses are depicted in detail in Figure 2). Students also expressed concerns about future health impacts due to climate change. This subscale had a mean score of 16.0 (SD = 2.2), with a high percentage (89.1%) predicting recognition of serious health impacts in the coming years. The highest concern was for Pakistan (91.5%), with a mean score of 5.5 (SD = 0.9), followed by local community impacts and global impacts (the responses are depicted in detail in Figure 3). Awareness of historical and current evidence related to climate change was moderately high among the respondents.
Perception about climate change scale.

Distribution of responses across subscale 1: attitudes towards climate change.

Distribution of responses across subscale 2, 4, 5, 6 and 7.

Distribution of responses across subscale 3.
The perception of direct health impacts due to climate change was notably high, with a mean score of 4.3 (SD = 1.2). The specific impacts most recognized included air quality-related illness (91.0%), water-availability illness (86.0%), and disruption of healthcare services during extreme weather events (85.0%). Cold-related illness (83.0%) and flooding-related displacement (87.0%) were also significant concerns. Regarding the impact of climate change on infectious diseases, the students agreed that food-borne diseases could be exacerbated by climate change, moreover, they showed concern about vector-borne infectious diseases. Finally, the mental health implications of climate change were recognized by 68.0% of the respondents. This indicates a low but growing awareness of the psychological toll that climate-related events can exert on individuals.
Perception about climate change across several demographic variables
The study also assessed the perceptions of medical students regarding the impacts of climate change on human health across several demographic variables, including age, gender, year of study, and total monthly income of the family. Table 3 provides a comprehensive overview of the non-parametric test statistics (P-values) and correlation coefficients for various subscales related to climate change perceptions against demographic variables. The total perception score, representing an aggregate measure of the various subscales, showed significant positive correlations with age (P < .01, r = .203), year of study (P ⩽ .01, r = .164), and total monthly income (P < .01, r = .228). Gender did not exhibit a significant correlation with the total perception score. The results highlight that demographic factors such as age, gender, year of study, and total monthly income of the family significantly influence medical students’ perceptions of climate change and its impacts on human health. Age and total monthly income consistently showed significant correlations across multiple subscales, emphasizing their role in shaping environmental health consciousness.
Non-parametric test and correlation statistics of perception scales on climate change across demographic variables.
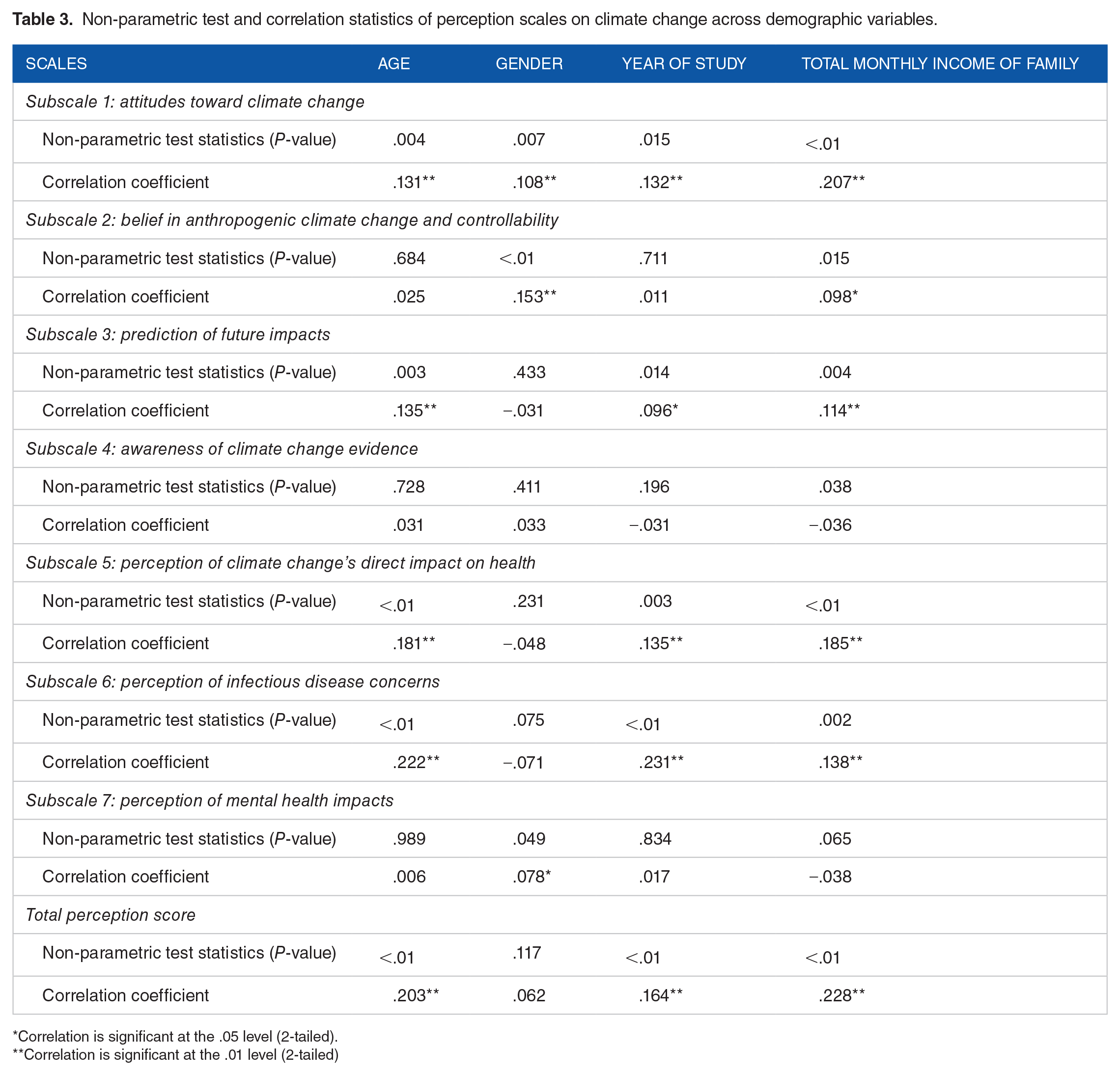
Correlation is significant at the .05 level (2-tailed).
Correlation is significant at the .01 level (2-tailed)
In our analysis of environmental health consciousness among medical students concerning the perceived impacts of climate change on human health, a multiple linear regression model was employed (presented in Table 4). The model, incorporating predictors such as household income, age, gender, and medical year, demonstrated a moderate fit with an R value of .327. The R 2 value indicated that 10.7% of the variance in environmental health consciousness could be explained by these variables (R2 = .107, Adjusted R2 = .101). Notably, household income, age, and gender emerged as significant predictors, with higher household income, older age, and male gender associated with increased environmental health consciousness. In contrast, the medical year of study did not significantly predict this consciousness. These findings suggest that socioeconomic factors and demographic characteristics play a crucial role in shaping medical students’ awareness of the health implications of climate change, highlighting the need for targeted educational strategies to enhance environmental health literacy within this population.
The regression coefficients for the predictors of environmental health consciousness among medical students regarding the perceived impacts of climate change on human health.

Discussion
The cross-sectional study highlighted key aspects regarding perception amongst medical students who represent the future leaders in healthcare. Our results highlighted that 78.6% of medical students view climate change as a negative factor contributor, and were worried about its direct implications on health. This was in accordance with a recent survey done on young adults in 2021, of similar age groups ranging from 16 to 25 which revealed the increasing climate anxiety in which 59% were very or extremely worried and 84% were at least moderately worried. 10 This portrays a particular sense of responsibility amongst youth, which is a positive factor contributing to mitigation of climate change.
The same survey shed light on the mental health implications, where 45% of respondents expressed the negative effects of climate change on their daily life and functioning. A mixture of worry, fear, anger, grief, despair, guilt, and shame, as well as hope, were recognized. This was in accordance with our study which revealed that 68% of the medical students recognized mental health implications of the momentously accelerating climate change. It was interesting to note that the more participants perceived environmental changes, the more impacts they felt. 11 This plays a crucial role in advocating the importance of considering mental health within climate change.
The general perception of medical students was of the belief that climate change was a result of human activities. This is consistent with another survey where 81% of participants think climate change is mostly or entirely caused by human endeavors. 12 Previous studies involving healthcare professionals, such as a survey conducted among members of the American Thoracic Society (ATS), revealed a consensus that climate change is a present reality impacting patients, and the majority foresee these climate-related health impacts worsening over the next two decades. 13
The majority (91.5%) of medical students predict the devastating effect on a Low middle-income country like Pakistan. This situation is compounded by Pakistan’s position as one of the five countries most severely affected by climate change. Consequently, there is an immediate need for Pakistan to take decisive action to mitigate the impacts of climate change. The spread of waterborne diseases such as malaria, dengue, Zika virus, typhoid, cholera, and asthma further exacerbates these challenges. This was consistent with our findings where 74% of the medical students revealed adequate concerns over the risk of rising infectious diseases. Besides disease outbreaks, alterations in climate are anticipated to amplify the difficulties concerning water availability and exposure to unsafe water. Projections of future climate extrapolated from prevailing rates of climate change, as predicted in a 2022 study, forecast heightened increase in precipitation patterns and glacial meltings, precipitating a surge in pathogenic content within existing water ecosystems in Pakistan. 14
Our results revealed that year of study positively correlated with good perception score regarding climate change amongst medical students. Another similar study done on German final year medical students revealed showed higher levels of agreement over expected consequences (75.6 ± 18.4), individual responsibility (75.1 ± 20.6) regarding climate change, but a professional responsibility as physicians to patients or society displayed weaker agreements. 15 Similarly, a study done on public health workers indicated that many of them acknowledged that climate change is a relevant threat for public health, but very often they lacked information, expertise, or resources to address that threat. 16 This necessitates the need to highlight the role of healthcare professionals in mitigating climate change effects.
Dr. Pencheon, Founding Director of the National Health Service (NHS) Sustainable Development Unit, presentations on the role of future doctors in transforming healthcare systems into environmentally stable entities, including aspects like carbon accounting, transformative changes in healthcare systems, and creating a sustainable health system, emphasize the importance of healthcare professional responsibility in mitigating climate change impacts. 17
Educational programs and awareness sessions could play a role in advancing knowledge and improving perceptions regarding the disastrous effects of changing climate. Saudi nursing students were noted for their more positive attitude towards integrating environmental sustainability in healthcare and stressed the significance of incorporating climate change into the curriculum. 18 Insights from Nigerian studies further support these findings, with over 71% of respondents advocating for comprehensive climate change studies in both undergraduate and postgraduate medical education programs. 19 These studies underscore the urgent need for educational reforms aimed at equipping future healthcare professionals. By integrating robust climate change education into the curriculum, medical students can bridge knowledge gaps and actively contribute to safeguarding public health amidst escalating climate challenges.
The evolving landscape of healthcare demands a proactive approach in preparing medical practitioners for the intricate challenges brought about by climate change. This pioneering cross-sectional study, engaging a multidisciplinary approach across multiple institutions, focused on Pakistani medical students—an essential cohort set to navigate the unfolding impacts of climate change on human health. It rigorously assessed the awareness levels and knowledge gaps within this demographic, revealing critical insights into their readiness to confront the imminent health consequences of environmental shifts. The study’s inclusive participant pool ensures broader applicability, underlining the urgency to equip the future medical workforce with the requisite skills and knowledge to address the intricate nexus between climate change and human health in Pakistan.
Limitation and Future Recommendation
While this study offers valuable insights into medical students’ perceptions of climate change and its impact on health, it has limitations to acknowledge. Firstly, it used a cross-sectional design, which doesn’t capture changes over time. Future research should consider longitudinal studies for a more comprehensive understanding of how students’ views evolve. Secondly, relying on self-reported data may introduce response bias. Efforts were made to minimize this through anonymity, but this potential limitation should be noted. While the translation was included to enhance accessibility, psychometric testing of the Urdu version was limited to content and face validity. This decision was based on the broad understanding of English in the Pakistani medical education system; however, future research may consider additional reliability and validity testing for language-specific contexts during pilot testing. Furthermore, some subscales consisted of only one or two items, potentially impacting the depth of construct measurement. We addressed this concern by ensuring satisfactory internal consistency for the overall scale, yet future studies might benefit from further refinement of these subscales. Lastly, the study focused solely on MBBS students, but future research should incorporate other medical fields for a broader perspective. Future studies should prioritize developing tailored climate education programs in medical schools, fostering knowledge and advocacy among students.
Conclusion
This cross-sectional study provides valuable insights into Pakistani medical students’ perceptions and knowledge regarding climate change and its impact on human health. The findings indicate an overall adequate concern regarding climate change and sufficient knowledge about the serious implications of climate change on Pakistan which is already affected by infectious diseases, scarce water supply and malnutrition. The research emphasizes the role of future doctors in transforming healthcare systems to be environmentally sustainable. Future recommendations could involve exploring various specialties and other pertinent factors to identify gaps in knowledge for developing an effective action plan.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302241310031 – Supplemental material for Insight into the Environmental Health Consciousness of Medical Students Regarding the Perceived Impacts of Climate Change on Human Health
Supplemental material, sj-docx-1-ehi-10.1177_11786302241310031 for Insight into the Environmental Health Consciousness of Medical Students Regarding the Perceived Impacts of Climate Change on Human Health by Yumna Shariff, Muneeba Mushtaq, Syed Muhammad Abdullah Shah, Hurais Malik, Muhammad Abdullah, Muhammad Usama Jamil, Abdul Rehman, Muhammad Hudaib, Manahil, Ahmad Umais Ahad, Sanila Mughal and Mohammed Mahmmoud Fadelallah Eljack in Environmental Health Insights
Footnotes
Acknowledgements
During the preparation of this work the authors used Generative AI for paraphrasing parts of the manuscript to improve readability and language.
Author Contributions
All authors contributed equally to the drafting of this manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.