
Abstract
Primary care clinicians may be the only source of occupational healthcare for many low-wage, high-risk workers who experience disproportionate occupational hazards. The authors explored barriers to providing occupational healthcare and recommendations for overcoming these challenges. The team conducted six focus groups and eleven key-informant interviews in two community health centers and among clinicians, community health workers, and other personnel from similar settings. Clinicians reported not utilizing occupational information during clinical encounters and identified competing priorities, limited appointment time, and lack of training as key barriers. They cited workers’ compensation as a source of confusion and frustration. However, most participants recognized occupation as an important social determinant of health and expressed interest in additional training and resources. Participants agreed that referral mechanisms for occupational medicine specialists and worker centers and changes in quality performance measures and electronic health records would be useful and that workers’ compensation and immigration policies need reform.
Keywords
Introduction
Occupational illness and injury in the United States carry long-term consequences for affected individuals and their families, as well as direct and indirect costs that exceed those for cancer. 1 However, occupational health is often neglected in medical education and in primary care and specialty practice, despite the evidence that workplace exposures contribute to the development of chronic diseases, such as asthma, or complicate the management of other diseases, such as diabetes.2–5 Work is an important social determinant of health, and work characterized by low job security, high hazards, poverty wages, and limited labor rights contributes to health disparities. Global restructuring of work relationships over the last several decades has increased economic migration; temporary, contingent, and precarious employment; and wage stagnation.6,7 Low-wage workers are often in high-hazard industries such as construction, agriculture, and manufacturing and frequently face additional challenges associated with poverty and immigration.8–10 Among the estimated 25.7 million foreign-born workers in the U.S. labor force, nearly half (48.3 percent) are Latino, who experience fatal traumatic injury rates at least one-third higher than those for U.S.-born workers.10–11 Fear of job loss may be compounded by the fear of deportation.12,13
Baron et al. 14 have developed a social-ecologic conceptual framework to develop interventions aimed at addressing the needs of low-wage workers that includes safety-net health centers as potential sources of care. Workers at greatest risk for work-related illness and injury may have no access to formal occupational health services, but may be eligible for care in more than 1200 community health centers that offer a primary care safety net to more than twenty-four million people in 9200 rural and urban communities throughout the United States. 15 However, primary care clinicians may have limited experience caring for work-related illness and injury and identifying risk factors (such as heat or noise), or screening for work-related conditions. Studies in Massachusetts have shown that 63 percent of health center patients have never heard of Occupational Safety and Health Administration (OSHA), and that health centers rarely provide workers’ compensation services.16,17 A few primary care settings provide occupational health services, but they are usually associated with research training projects. 18
The Migrant Clinicians Network (MCN) functions as a national training and technical assistance organization for health centers, health departments, community-based organizations, and worker centers, with a focus on clinicians, health outreach workers, and other direct care providers. MCN conducted this study to explore perceptions of Federally Qualified Health Center (FQHC) personnel of the occupational health needs of their patients; barriers to the recognition, management, and prevention of work-related illness and injury; and recommendations to overcome those barriers.
Methods
Project investigators used qualitative methods including focus groups and key informant interviews to examine current practices, barriers, and facilitators to address and identify work-related health conditions as well as perceptions and attitudes about occupational health among clinicians and other health center personnel. In the manner of qualitative research, this study adopted a flexible research strategy that allowed the project team to proceed in an exploratory manner based on the themes that emerged. 19 The study explored occupational health issues encountered by health center personnel as well as larger contextual questions about current practices.
This project purposefully included participants from a variety of health fields in order to provide a more comprehensive understanding of the barriers to occupational health at various levels of community health centers. Clinicians are defined as licensed healthcare professionals who provide direct patient care and may be further defined as physicians, nurse practitioners, nurse midwives, physicians assistants, and registered and licensed practical nurses. Other health personnel with direct patient contact include outreach and social workers, community health workers (CHWs), and medical assistants (MAs). CHWs and MAs often are members of the community served by the health center. Other support personnel include chief operating officers, chief financial officers, and information technology specialists; chief medical officers or medical directors are included among the clinicians. Clinicians and other health and support personnel were recruited from two FQHCs engaged with the MCN with distinct community profiles. One health center, located on the West Coast, serves mostly agricultural workers. In 2015, the clinic served 26,532 total patients and 77 percent of the patient population was living at or below 100 percent of the federal poverty level. The patient population is 89.6 percent Latino and 74.8 percent prefer to be served in a language other than English. The second health center, located in the Midwest, serves a more diverse worker population including workers in meatpacking, manufacturing, and housekeeping, among other industries. In 2015, the clinic served 35,557 total patients and 59.2 percent of the patient population was living at or below 100 percent of the federal poverty level. The patient population is 72.9 percent Latino ethnicity and 38.8 percent prefer to be served in a language other than English. Additional participants recruited included CHW participants participating in an MCN-sponsored conference in Washington State and experienced clinicians from additional federally qualified and other health centers.
An advisory group of six persons with expertise in occupational medicine, migrant health, primary care, and worker health and safety met by teleconference twice to review project materials. Key informant interviews, focus group questions, informed consent information, recruitment language, and the research protocol were developed and modified in response to the advisory group. All research project materials and recruitment methods were approved by the MCN Institutional Review Board. Health center administrators at the two FQHCs conducted Institutional Review Board-approved outreach to recruit individual clinicians and staff. CHWs were recruited via a Washington State state-wide network of CHWs, while MCN staff recruited the other participants.
All data collection took place between December 2014 and July 2015.
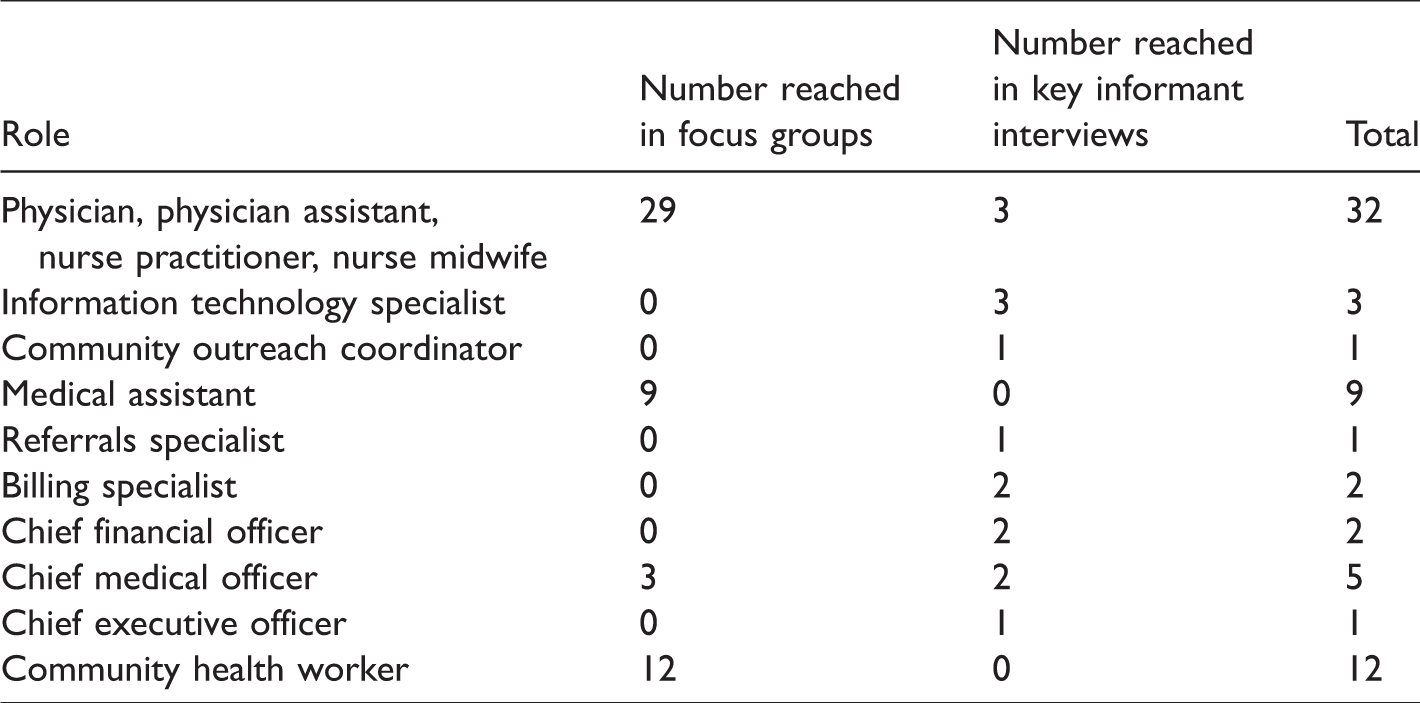
One focus group was conducted among clinicians and one among MAs at the rural health center; one focus group was conducted among primary care clinicians and a second among clinicians caring for pregnant women at the urban health center; a focus group was conducted among clinicians and clinician-administrators serving on the MCN Board of Directors; and a focus group of CHWs took place at a meeting hosted by MCN in Washington State. Key informant interviews were conducted among nine administrative, other support, and information technology staff at the two FQHCs and among two additional primary care clinicians affiliated with other centers who were interviewed by telephone (see Table 1).
Focus Group and Key Informant Interview Participants by Occupation.
Questions for both focus groups and for key informant interviews were designed as open-ended to elicit broad responses. Facilitators and interviewers followed up with clarifying questions to pursue areas of discussion and asked probing questions to gather information not volunteered by the participants. As an example, in the guide for the clinicians’ focus group session, the opening questions, “Do your patients complain of any work-related problems? Can you give examples?” often required probes such as, “Do you have patients with work-related musculoskeletal complaints? Asthma that is exacerbated by work? Skin conditions related to work? Other?”
Verbal consent was obtained prior to all research activities in each participant’s preferred language. The CHW focus group was conducted in both English and Spanish by fully bilingual facilitators; all other sessions were conducted in English. Data were collected using a recording device and note-taking by project staff. All audio recordings were transcribed in English. The transcripts were reviewed by facilitators to confirm accuracy. After each focus group, the facilitators and investigators met and discussed immediate impressions.
The team utilized ATLAS.ti Version 7 software to assist with analysis of the qualitative data. The qualitative data analysis was based on traditional qualitative research methods, using the constant comparative method within the framework of the Grounded Theory approach.20,21 This is an inductive approach to gathering information without a priori hypotheses that allowed the research team to analyze data throughout the data collection period and make adjustments accordingly.
Results
A total of sixty-eight clinicians, direct care support staff, and other clinic personnel participated in six focus groups and eleven semistructured interviews. There were thirty-two clinicians, including physicians, physician assistants, nurse practitioners, and nurse midwives; twenty-one direct care workers, including MAs and CHWs; and fifteen other health center personnel.
When initially asked about occupational health, most participants, including clinicians and other personnel, immediately thought of workers’ compensation and frequently equated the two. Workers’ compensation was considered a challenge by virtually all participants and is addressed in more detail under “Barriers.” Generally, clinicians did not raise occupational health considerations other than workers’ compensation until probing questions from interviewers expanded the discussion. Once these probing questions were asked, however, clinicians recognized work as a social determinant of health and identified work-related considerations related to musculoskeletal disorders, asthma and other respiratory conditions, health during pregnancy, behavioral health, and other issues. MAs and CHWs tended to be more familiar with work issues.
Common Occupational Health Topics
Musculoskeletal injuries, primarily back pain, were the most commonly reported work-related concerns identified by clinicians. The participants generally did not ask patients about occupation, but one clinician underscored the link between musculoskeletal injuries and workplace exposures and stated that if a patient came to an appointment with a musculoskeletal complaint, “the first thing I ask is ‘what do you do for work?’ [The patient will say] ‘oh, I clean’ or [some other job], and then I know.” One MA described the link between a patient’s complaint of back pain and specific work tasks, “If it’s field work they’re bending over like strawberry work, but there are other types of berries where you’re standing all day. So I usually put information about exactly what it is.” One CHW emphasized a personal connection with the clients, I used to be a farmworker when I was young and my whole family, we all suffer from upper back pains from carrying all those heavy loads. There were five of us who … all suffer [in] the same place.
CHWs and MAs shared concerns about their clients’ workplace exposures. One CHW reported that clients “sometimes are asked to do things without enough information or proper training, equipment, or materials.” Another noted, “People don’t get safety equipment instructions and they need it.”
When prompted, primary care clinicians and other health personnel described work-related asthma and other respiratory conditions among patients who had been exposed to factory air pollutants, low temperatures in meatpacking plants, and bleach and other cleaning chemicals. Clinicians reported managing asthma symptoms for these patients as they would for nonwork-related asthma.
When asked, clinicians reported that they regularly address ear and skin irritation related to the use of hearing protection or work exposures but generally did not document them as work-related in the patient chart. They said they did not discuss any anticipatory guidance regarding noise exposure or skin protection.
Nurse midwives frequently encountered work-related health concerns: their patients present with back and pelvic pain; express concern regarding chemical exposures; and often request work restrictions that limit squatting, lifting, pushing, and pulling in the third trimester of pregnancy. While one primary care clinician reported identifying chemicals from safety data sheets, most did not know how to obtain information regarding workplace chemical exposures.
Barriers to Caring for Work-Related Illness and Injury
Clinical priorities and time constraints
Clinicians reported other clinical priorities such as obesity, diabetes, or teen pregnancy, and limited appointment times as barriers. One stated: There is a focus on primary care that just does not include occupational health … major questions come up about workers’ compensation and there is frustration when people see how the system doesn’t satisfy the patient or the provider. Our pregnant patients have such a long problem list to address at an appointment, rarely do I think of bringing up their work environment unless they bring it up themselves … If they’re not bringing it up as a major concern, it falls way down below other concerns. I don’t think I ever bring it up. I’d write a note, and they would send it back and say the specific wording wasn’t correct … I spent a lot of my time outside of my clinic time doing this. And I felt it was a waste of my time … I think community health centers have always been an intersection between public health and primary care, but there is such a burden to collect data … that may or may not be relevant to the patient you have sitting in front of you.
Immigration status and job insecurity
Clinicians and other health personnel reported that a large portion of their patient population lack legal authorization to live and work in the United States; these patients fear job loss or deportation and do not want to report or record abuses or unsafe conditions in the workplace.
Other patients request notes regarding their visit, but, because many patients obtain employment using an alias, they request that the documentation be written for the name used at work. Some clinicians discussed their own fear of legal issues. One stated: [Sometimes] the most I can give someone is a blank work note that says ‘this person was here’ … and that patient can do with it what they will. We’re here to provide medical care and to maintain patient rapport so people will come here. It’s not our function [to verify immigration status]. We do not ask [about documentation status]. I have no idea how [the patient] got their numbers or if these numbers are correct. I just go with whatever they are giving me … I think we just decide not to ask.
Participants repeatedly emphasized that many patients choose not to make workers’ compensation claims because of the fear of job loss. One MA said, “ … they don’t want to get fired. So they don’t bring it up, or they don’t want to get in trouble or they don’t want to lose their job … they make comments like that.”
A CHW who works with domestic violence victims stated, … in general, our clients don’t know their rights as workers. For instance, if they have a court appointment they don’t know they have the right to miss work and that employers have to respect that … They are scared of losing their job, scared of immigration.
Similarly, the lack of paid time off increases the likelihood that patients will not present for follow-up visits: “If they are not in the fields, they don’t get paid. Period. And that’s … the problem we have getting them to community health centers.” One clinician reported filing Family Medical Leave Act for a patient so they could attend regular appointments for diabetes management without fear of losing their job.
Workers’ compensation
Most clinicians and other health center personnel could not articulate the difference between workers’ compensation and occupational health, and clinicians did not document work-related injuries and exposures in the patient chart unless the patient indicated that they would like to proceed with a workers’ compensation claim. One clinician noted: I think that [documentation is] something that we are confused on. Are we allowed to say that [something is work-related] and then are we going to be in trouble that we did not do a Doctor’s First [report]? … I think that sometimes [providers] avoid saying [an issue] is work-related because of that … Maybe we should [document if something is work-related] because then if the [patient] changes their mind then at least it is documented. I feel horrible about these two patients that I encouraged [to file for workers’ compensation] … It is probably going to be good in the long run, but in the two years until they finally get care, their life is really awful … Yes, long-term they are not going to have the option of getting surgery or getting appropriate care but maybe that is not what they really need right now if that means that they are not going to be able to pay their rent or they are not going to have food for their family, because they are waiting so long for their case to get open.
Clinicians also noted their patients need legal support to succeed with workers’ compensation claims. “We refer them to [local legal aid], and they have lawyers [there], but it takes a long time whereas if they had just filed for disability, within two weeks they would have gotten a check.” Another clinician noted: You may see somebody in the clinic, but they usually don’t get reimbursed [by workers’ compensation] … In most cases, if [the patient] continues with the process they will lose their job … It’s really frustrating to be quite honest with you… . And patients I deal with work year-round, their wives work year-round when they are not pregnant and a lot of them will have injuries but they’ll work through them and then they will have to retire early, like a football player [who] plays for ten years and [then is] done. These workers will work ten years, then they will have a bad back. It’s not a good experience.
Lack of Training/Resources/Referral Options
Participants in many roles emphasized their lack of training in occupational health. One nurse midwife stated: “I don’t feel comfortable … I don’t feel like I’ve been trained enough.” One clinician summarized the general discomfort dealing with work-related health as: I don’t know if any of us are super comfortable with the occupational medicine process. I can handle someone who is septic way easier than [I can handle] a work form. I just don’t know what to do. I think that there is a lot of hesitancy about how [to] make a change in work environment … I don’t know the nature of their work, and it takes a lot of explaining [for me to understand] what it is that they’re doing in this meatpacking plant … It’s a long conversation to talk about [possible accommodations] … Some of it is really hard to figure out and there isn’t a great resource for what I should ask of the company. I had clients that were given masks, but they weren’t given information on the dangers so they aren’t wearing them. So I am educating them and telling them that this is important—but I don’t even really know much about it.
Clinical uncertainty, chronic pain, and mental health
The absence of objective findings for many work-related health concerns was another point of frustration for clinicians. One stated, “Often the patient feels pain, and you’re basing restrictions based on a patient’s perception of pain as opposed to a certain medical technique.”
One clinician described the spiral that is often associated with workers who experience chronic pain due to a work-related injury as follows: “[A] musculoskeletal [injury] might make your depression worse and make you [less likely] to take your medicines on time, or you start using substances … It can cascade.” Another highlighted how the stress of low-wage work has a ripple effect: It’s time and stress … if a person is so busy and working three jobs … they don’t have time to take care of themselves, and then there is chronic stress that makes obesity … hypertension … [and] diabetes worse. All those other chronic conditions worsen as a physiologic response to stress. They have stress related to their jobs and … sometimes it is related to personal conflicts … with the supervisor [or] a coworker. People who just do not have a lot of control over their work environment [but still] have to work [feel] stuck with a situation where it can sometimes be a very hostile environment … there is an emotional toll when we see those kinds of issues. [Chronic pain] is where things get fairly uncomfortable for providers because we are often caught in the middle … You want to advocate for the patients and you want to do what is best for them. Sometimes what I feel is [that] the best [thing to do] is not just stay at home [when a patient requests to be excused from work for chronic pain] … And so for those patients it is really hard to know what the right thing to do is and it is hard to [deal with] employers who are sometimes very angry and demanding more and more documentation [of the injury] or documentation of who [the patient] really is … And quite frankly, there are some people who feel very wronged by their employers and that is also a big element of what I see.
Lack of patient educational resources
One nurse midwife stated that they are “lacking basic tools. Even a basic brochure about knowing your rights would be helpful so we [can] empower people. We need classes … so we can present tools to workers in a valuable way.”
CHWs reported having some work-related health materials in CD format, but that the format made the materials difficult to access; it was an arduous process to find the learning module in the appropriate language and topic for each patient. A primary care clinician reported that despite access to a large medical library of resources, few of the materials were in Spanish. Another participant reported that there were no work-related patient handouts in the clinic.
Facilitators to Caring for Work-Related Illness and Injury
Desire for resources/training/knowledge of local industries
Despite confusion, limited resources, and lack of training, clinicians and other health center personnel expressed general interest in work-related health. Participants overwhelmingly recognized that their patient population works in high-hazard industries and they acknowledged the importance of health services that better address work-related health needs. No participants stated that work-related health was not an important component of patient wellness.
Clinicians and other health center personnel expressed a desire for additional training and resources to handle work-related illnesses and injuries, specifically ones that would be relevant to their particular geographic location and local industries. Clinicians expressed the need for training to better understand best practices for managing work-related conditions, preferably with continuing education credits: the training “… wouldn’t be resented as much … [It’s] not painful because … it’s really relevant to the patients you are seeing, and you get credit.”
Participants were aware of the local industries employing most of their patients. As noted above, some MAs and CHWs had some information about both work hazards and preventive measures. However, most clinicians struggled to connect work and work-related hazards with their patients’ immediate health concerns. One nurse midwife stated, “Honestly, if you told me you were a meatpacker I would have no idea what you’re exposed to, other than meat … and maybe not even that.”
Existing Infrastructure for Outreach
When asked whether existing health education and outreach programs have the capacity to address work-related health, several participants felt that a specific work-related outreach program would be well received and could be implemented with funding for one dedicated part-time staff member and the development of a curriculum and training materials. Without a doubt we would be interested in working on [work-related health]. And I think it needs to happen because there’s a huge burden on providers, and the information they’re giving over and over again about work-related health issues—[community outreach staff] could easily address them. I hope that we can move to a model where everybody is performing … at the top of their licensure and part of that means maybe providers don’t need to give information on pain management and things like that for arthritis for pickers’ hands.
Nurse midwives at one health center described the Centering Pregnancy program, 22 in which small discussion groups are utilized to create safe spaces for pregnant women to discuss health issues. One stated: “… if there was any organization or person who could come in that group and give a presentation about occupational health, I would really love that. That is when we have time to talk to patients.”
Community partners and access to resources
Participants were asked about their knowledge of local worker centers, unions, or other community assets where patients could be referred for work-related assistance. Almost all mentioned referring patients with work-related concerns to an internal resource instead, such as the social work or outreach department.
Although information about workplace exposures was limited, some participants reported using web-engine searches for basic information about occupational exposures, nurse midwives reported using guidelines set out by the American Congress of Obstetricians and Gynecologists, and others used general resources, including UpToDate®, that occasionally include occupational health topics.
Participant-Proposed Solutions
Participants offered a number of solutions to better address occupational health at the health center level.
Framing Occupational Health
Participants emphasized the importance of framing work-related health and safety in a way that is relevant to clinical practice or as a social determinant of health. One clinician stated: We’re struggling with what are some of the broader social determinants of health, and … occupational health is one of those issues. It takes extra time and screening to develop that linkage [between work and health], and a lot of the EHR systems don’t have a great way to record that information or report on that information. Our strategic plan … encompasses five different things, [including] social determinants of health … It would seem like occupational health will fit under social determinants of health and quality of care, although it does not really show up on our strategic plan … that could be its potential place.
Clinician–Employer Relationship
Participants suggested that strengthening the relationship between healthcare providers and local employers might improve the comfort level of both patient and provider when managing work-related injuries and illness.
Training for Clinicians and Other Personnel/Training and Educational Materials for Patients
Participants indicated interest in occupational health clinical education that provided continuing education credits for clinicians and training for intake personnel and for community outreach workers. Such training should focus on the needs of local industries.
Participants suggested training sessions for patients that might be delivered by various parties, including educators with expertise in workers’ rights. These trainings could cover hazards associated with particular work sites and effective preventive measures, among other topics. This week I have been seeing patients … and I have been thinking, ‘Gosh, we should have a class on how to be safe while working in the fields,’ because there are so many different things [the patients are] facing … The medications [for diabetic patients] change drastically in the summer because they are constantly exercising [in the fields] all day long … We don’t have any [educational materials] like that, but it would be really nice.
Referral Resources/Improved Systems/Electronic Health Records
Clinicians stated that they would welcome two levels of referral capabilities. First, they want to be able to refer patients to occupational health specialists either for formal evaluation or, at minimum, to obtain advice through curbside/telephone consultation. Second, they would like to refer patients to another member of the team (such as a health outreach worker) with skills to help the patient navigate legal, governmental, or community-based sources of assistance.
In the CHW focus group, participants were clearly interested in increasing their skills to assume a more active role in workplace prevention; the MA focus group agreed about the need for better patient information materials.
The information technology specialists at both health centers stated that the electronic health record (EHR) has the capacity to capture data about patient occupation, and one physician noted: Ultimately, the EHR is going to be there even when [there is] staff turnover … The occupational health questionnaire was [getting filled out regularly] … But now it’s like everybody is different and they’re [asking] ‘what is this form for?’ Then the [occupational health questionnaire] doesn’t get handed out. So, everything that is in the electronic health record tends to be a higher priority.
One clinician identified the need for a meaningful use requirement to ensure data capture and use.
Discussion
This study builds on previous work exploring the integration of occupational health into primary care settings, expanding the geographic range of sites and the health personnel included. It confirms a number of previously reported findings about challenges experienced by clinicians and other personnel from time constraints, competing priorities, lack of training, and lack of available referral networks, which is exacerbated by fear regarding patient job insecurity and immigration status in this safety-net setting.12–17 It sheds new light on the extent to which clinicians conflate occupational health with workers’ compensation and why this is a deterrent to offering care. Conversations about work-related injuries and the workers’ compensation process revealed feelings of hopelessness, frustration, and low expectations on the part of the clinician and unresolved health problems for the patient. These findings complement mounting evidence demonstrating persistent adverse effects of work-related illness and injury on work, functional capacity, relationships, mental health, and income, which often results in depression, disability, and adverse effects on family members.23–32 Workers’ compensation should offer wage replacement and access to specialized medical and rehabilitation care that would benefit the individual. However, reduction in benefits and programmatic changes that have made the process more adversarial have caused serious problems at the state level and calls for reform date back almost two decades. 33 While it is difficult to assess the accuracy of each of the statements made (e.g., the comment that disability claims can be adjudicated in two weeks may reflect misunderstanding or intended exaggeration), the consensus is clearly that the system is broken. The description of the antagonism inherent in the system, the interplay between chronic pain and depression and substance abuse serve to emphasize the importance of preventing occupational illness and injury in the first place. However, the health centers were not engaged in aspects of primary prevention and lacked understanding about hearing protection programs, heat injury prevention, or outreach to promote ladder safety, as examples. The inclusion of a single focus group each for MAs and for CHWs provides preliminary suggestive information but no conclusions. Unlike the MA focus group, the CHW focus group did not take place in a health center and it included state-wide leadership. CHWs were more critical of the efforts currently taking place in health centers and very interested in assuming a more active role in occupational health prevention.
However, clinic personnel did recognize the importance of work in their patients’ lives and the importance of work-related health conditions. They expressed interest in educational programs targeting the health and safety needs of their patient population and identified the need for low-literacy, culturally competent, occupation-specific materials in print and online formats for their patients. Primary care clinicians want and need access to occupational and environmental health specialists in the same way they utilize other subspecialists, both through telephone consultation and referral of complex patients for more in-depth care.
Clinicians also need to be able to refer patients with work-related exposures for non-clinical occupational safety and health services. CHWS offer an evidence-based model to promote culturally competent health education and might be used to address occupational health. This is particularly relevant for non-English-speaking vulnerable populations, including those who speak indigenous languages. Worker rights training has been combined with safety and health training and offered as part of peer-educator participatory hazard awareness training through immigrant worker centers and through FQHCs that train CHWs as peer educators for outreach to workers in different occupations, ranging from construction day labor to home care and nail salon work.34–37 This model appears ripe for expansion.
Although participants objected to increasing demands for data, they recognized the importance of targeting specific quality measures for conditions such as asthma and seemed willing to collect additional data if the information were demonstrated to be clinically relevant.
This study has a number of limitations. Although it included a broader geographic and professional range for participants than previous studies, the range of FQHCs was by no means covered. Resource constraints limited the number of focus groups so that saturation was achieved only for clinical personnel and prevented a return visit to a subset of initial participants to ensure that we “got it all/got it right.” However, the information obtained provides useful insight that can help guide next steps.
Long-range policy interventions that would foster improved integration of occupational health into primary care would include major workers’ compensation reform and other contextual changes to improve job security and effect immigration reform. More immediate policy changes targeting the health centers directly would include making occupational safety and health information a Healthcare Effectiveness Data and Information Set (HEDIS) performance requirement for FQHCs, such as flu vaccination rates for adults, or other data that measure healthcare effectiveness. The Health Resources and Services Administration requires FQHCs to submit these measures, and it would change health center practice simply to include occupational health information in a number of disease categories. 38 Similarly, including work site information as meaningful use data for specific conditions in the EHR would encourage clinicians to identify opportunities for prevention and is currently being explored.39,40
At the health center level, developing support systems for clinicians, outreach workers, and patients are necessary next steps. Clinicians need telephone support from occupational medicine experts and the ability to refer patients for specialty occupational medicine care as well as to refer patients for safety and health training and legal and other support. CHWs will need support to offer training and help with hazard identification and management. Further research should be conducted to explore the role of MAs, especially in health centers that do not employ CHWs.
Patients need services as well as peer support and protection from job loss or deportation. They will require demonstration projects with process and outcome evaluations and will require resources to implement at scale, but many of the pieces are already in place. The Association of Occupational and Environmental Clinics, the National Institute for Occupational Safety and Health-funded Training Program Grants and Education and Research Centers, and the American College of Occupational and Environmental Medicine’s Section on Underserved Occupational Populations may be able to provide telephone consultation to assist with specific questions and some will be available for patient referral. Both Washington State and New York State have state-wide networks of centers that provide high-quality, subsidized occupational health services for referred patients. Area OSHA offices offer outreach for training and OSHA funds other entities to offer free safety and health consultation to small businesses. The Interfaith Worker Justice Network and the National Day Laborers Organizing Committee offer links to worker centers in many locations. A number of unions, including the United Food and Commercial Workers Union, the Laborers International Union of North America, and the Service Employees International Union are working with low-wage workers to improve both policy and local members’ working conditions and pay.
At the individual level, a wide range of training materials are already available to clinicians, CHWs, and patients through written materials, webinars, and outreach training opportunities, but mechanisms to increase uptake and match offerings with need are required.
Conclusion
Clinicians and other personnel serving vulnerable populations in safety-net health centers confirm the toll that unsafe work and lack of job security take on their patients. They identified extensive barriers to incorporating occupational health services into the primary care setting but recognized work as a social determinant of health. They identified several concrete steps that would enhance their ability to meet the needs of their working patients.
Footnotes
Acknowledgments
The authors are grateful to the support from Dr. Leslie Nickels, Christy Forrester, MS, and Nura Sadeghpour, MPH, at the National Institute for Occupational Safety and Health, as well as to the MCN Board of Directors and staff members, especially Deliana Garcia, MA, Dr. Ileana Ponce-Gonzalez, and Jillian Hopewell, MPA, MA. The authors also extend their gratitude to all of the participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Occupational Safety and Health contract 254–2014-M-59767.