
Abstract
Pediatric end-of-life care (EOL care) entails challenging tasks for health care professionals (HCPs). Little is known about HCPs’ experiences and needs when providing pediatric EOL care in Switzerland. This study aimed to describe the experiences and needs of HCPs in pediatric EOL care in Switzerland and to develop recommendations for the health ministry. The key aspect in EOL care provision was identified as the capacity to establish a relationship with the dying child and the family. Barriers to this interaction were ethical dilemmas, problems in collaboration with the interprofessional team, and structural problems on the level of organizations. A major need was the expansion of vocational training and support by specialized palliative care teams. We recommend the development of a national concept for the provision of EOL care in children, accompanied by training programs and supported by specialized pediatric palliative care teams located in tertiary children’s hospitals.
Keywords
Introduction
Caring for children in a palliative situation, as well as for their families, is a highly demanding and stressful task, especially when the health status of the affected child deteriorates and the care needs to be directed toward end-of-life (EOL) care. End-of-life care as part of pediatric palliative care (PPC) aims at providing the best possible care for a child and optimally supporting the family to cope with such a devastating experience. 1 A variety of physical, psychological, spiritual, and social needs are expressed by dying children and their families. Therefore, an interprofessional team of health care professionals (HCPs) is entrusted with providing holistic care.2,3
Professionals need to be well prepared and trained to take over such challenging and emotionally draining tasks as those encountered in pediatric EOL care. A family-centered approach is compulsory, specialized knowledge and communications skills are needed, and individual coping strategies should be developed by each member of the interprofessional team. Therefore, specific experiences and needs may arise, affecting the provision of EOL care. Previous studies have revealed some of the needs and supporting factors professionals report on delivering EOL care, as well as some of the barriers they face.4–10
Emotional distress is an afflicting experience when providing EOL care. In some studies, emotional distress in HCPs is described along with the stressors evoking it, for example, having to give care that is not in the best interests of the child; 11 most notably if the treatment is expected to cause discomfort or pain.12–14 These ethical dilemmas and conflicting opinions within members of a team may evoke a feeling of powerlessness in the person affected and thus increase the risk of distress.15–17 In addition, the quality of a patient’s death is reported to influence the level of distress. 10
In Switzerland, specialized PPC is offered in only 2 of 5 Swiss university children’s hospitals and 1 regional hospital. Similar to other developed countries, the consultative model of PPC is the favored model in Switzerland.18,19 A consultative service consists of a multiprofessional specialized team that provides support and advice to the child’s primary care team, particularly in the hospital setting. For home care, PPC teams are often more directly involved. 20
In the year 2010, the Swiss Federal Office of Public Health and the Conference of Cantonal Directors of Public Health fostered PC and PPC in Switzerland 21 by developing national guidelines and putting PC on the top list of priorities needing further strengthening in the Swiss health system. The Swiss National Strategy 21 that was developed stipulates that more basic and applied research is needed in specialized areas of PC, such as pediatrics, to develop guidelines for supporting and training HCPs.
No systematic research has been done so far in Switzerland on the experiences and needs of HCPs involved in pediatric EOL care. The aims of this study were therefore to (1) explore HCPs’ experiences of and needs of for institutional support and training in communication and in coping with emotional distress and interprofessional work in different pediatric EOL care settings in Switzerland and (2) develop recommendations for providing further training and education as well as support for HCPs on both the institutional and national levels.
Method
This study was an integral part of a nationwide observational study entitled, “Pediatric End-of-Life Care Needs in Switzerland” (Pediatric End-of-Life Care Needs, 2012-2015, NCT 01983852). The overall project aimed to provide a comprehensive overview of pediatric EOL care in Switzerland and to reveal and describe parents’ experiences and needs across the country, 22 whereas the focus of the study presented here was to disclose experiences and needs of HCPs involved in pediatric EOL care. End of life was defined as the last 4 weeks of a dying child in this study.
Design
A qualitative interpretative approach was chosen. The qualitative paradigm aims to explore and understand human experiences and behaviors in different situations 23 and how individuals perceive and interpret them. Our research approach was inductive. 24 Six interprofessional focus groups were organized with HCPs providing EOL care but without particular training from across Switzerland, including the German, French, and Italian language regions. Focus groups are especially suitable for exploring people’s opinions and attitudes on a clearly defined topic by the interaction among the participants. 25 Furthermore, they facilitate in an interactive way a discussion among participants, which allows to move away from preexisting researcher dominated questions. For this study, we expected focus groups to have more power to explore on organizational and interprofessional aspects in EOL care than compared with individual interviews.
Setting
In total, 4 university and 2 regional hospitals were selected, including their corresponding community care settings and some outpatient pediatricians. Potential participants were contacted by a collaborating researcher of each hospital. The university hospitals were overrepresented, as most dying children are treated in specialized settings in Switzerland. The research team collaborated with the local researchers to facilitate the coordination and organization of the interviews.
Participants
Participants were recruited purposively between September 2014 and January 2015 and represented the broad spectrum of HCPs most often involved in pediatric EOL care: pediatricians and pediatric nurses, including community nurses and associated health/social professionals (psychologists, social workers, physiotherapists, pastors, and hospital teachers). The main inclusion criterion was whether the professional had cared for at least one dying child in the previous year, but participants were also required to be fluent in the language of the focus group.
Data collection
An interview guideline was drawn up in German based on a review of the literature and on the research team’s expertise, as well as on the recommendations of Krueger and Casey. 26 The interview guideline was then translated into French and Italian. It included the introduction given by the people chairing the groups, the interview questions, and a description of the facilitator’s role. To start the discussion, each participant was asked to describe one of the most impressing experiences they had gone through in EOL care. The introduction was followed by a main question related to what constitutes good EOL care and what kinds of difficulties on the personal, institutional, and national levels they are experiencing in the provision of good EOL care. The final question was intended to elicit participants’ ratings of their main needs in pediatric EOL care. The interviews were held in the participants’ mother tongue.
The 6 focus group interviews, which each took 90 minutes, were audiotaped and transcribed verbatim. Before the discussion began, all participants were asked to fill out a short questionnaire with demographic information.
Data analysis
To handle our multilingual data, recommendations of Baumgartner 27 were followed with the original, mediating, and target languages defined and points of translation specified. To ensure that the data were rich, we transcribed and analyzed the interviews in the original language. Team members with appropriate language skills (German, Italian or French) analyzed and discussed the interviews. Because German was the dominant language, it was considered as the mediating language, also for the codes used in synthesizing the data. The findings and citations were translated into English as the target language. 27 ATLAS.ti software (version 7) 28 was used to organize the data.
The data were analyzed using the iterative thematic analysis approach by Braun and Clarke, 29 which allows crucial contents to be identified. The analytic process involved 6 phases and included analysts with different professional backgrounds for better quality, objectivity, and plausibility. 24 Members of the analysis group read and reread the interviews (step 1), generated on an individual basis initial codes (step 2), and then searched for themes overarching these initial codes (step 3). In 6 peer group meetings, common themes were specified (step 4), defined, and named (step 5). Finally, a thematic map can be generated (step 6). This last step was not taken into consideration in this study as we considered the description of the themes as informative enough.
Analysis started as soon as the first interview was completed. Each interview was analyzed separately and the findings discussed step-by-step in 6 different peer group meetings to obtain a collegial validation because interpretations may differ depending on subjective perspectives, which can then be integrated through discussion. 30
Ethical considerations
The study was conducted following the rules of good clinical practice and current Swiss federal law. The study was approved by the leading ethics board (KEK-ZH-Nr. 2012-0537 August 20, 2014) and additionally by the 5 corresponding cantonal ethics boards in Switzerland.
Results
Six focus group interviews with a total of 48 participants were conducted, comprising 17 physicians, 18 nurses, 6 community nurses, 4 social workers, a psychologist, a music therapist, and a chaplain. Their median work experience was 20 (5-39) years and concerning EOL care 13 (3-32) years (Table 1). The results are presented in 2 parts: (1) the experiences of HCPs providing EOL care in children in Switzerland and (2) the main needs for action that became evident.
Sample characteristics.
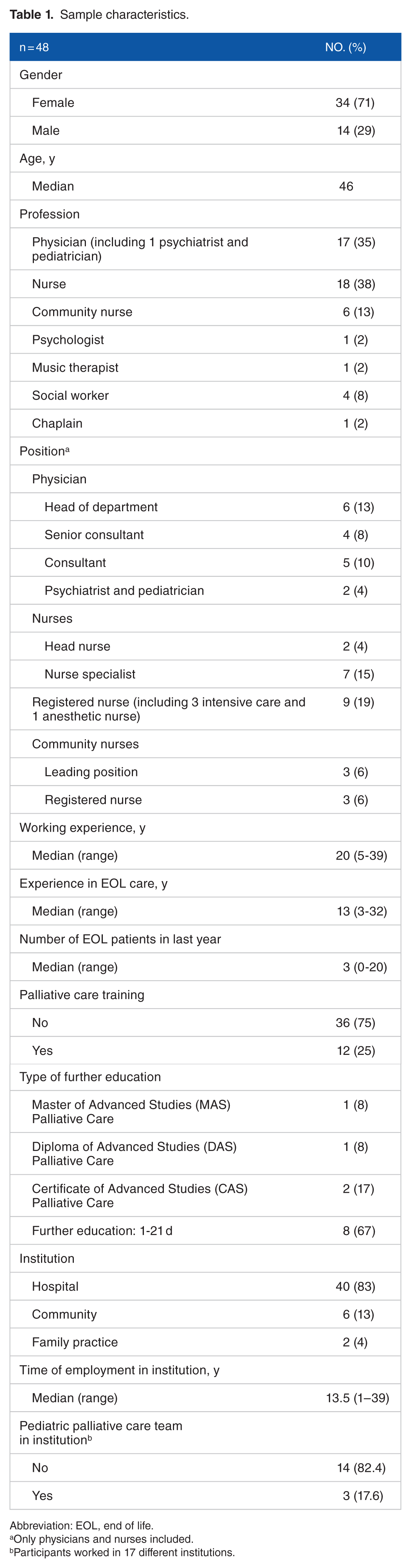
Abbreviation: EOL, end of life.
Only physicians and nurses included.
Participants worked in 17 different institutions.
Participants’ experiences in providing EOL care in children
All participants perceived EOL care as an integral part of their professional duty and as a very valuable part of their work. End-of-life care was described as being highly challenging by demanding high emotional involvement depending on the patient’s medical situation and the emotional struggles the families were going through. Most participants expressed the need to meet each individual family’s needs as comprehensively as possible. However, most of the study participants stated that they had not been sufficiently prepared to take over such a demanding task, and in fact, most of them did not have any specific PPC training.
Personal relationships as a key aspect of EOL care
Most of the participants considered developing a relationship with the dying child and the family to be a relevant element of EOL care. Besides mutual trust and personal engagement, providing comprehensive and honest information contributed to the quality of this particular relationship. However, the relationship might also add to the likelihood of openly discussing difficult issues on treatment options, including unrealistic hopes and topics surrounding death. The challenge lay in striking a balance between creating a personal relationship and still being able to act professionally. Trusting relationships could be formed even in highly acute situations within a short period (eg, on a pediatric intensive care unit [PICU]):
In my experience, relationships can also be developed in a short time; not necessarily with the child, since the child might be brain dead or heavily sedated.—We talk to the child without getting answers directly, but we receive answers from the families. Although there is just a limited amount of time, relationships arise and are quite strong. We are a kind of a lifeline which they can hold onto to get information and some safety. (PICU nurse)
A sustainable relationship, based on familiarity and trust, allowed HCPs to embark on the process of EOL care. Their statements showed great respect and esteem for the burdening situations families were going through, indicating their strength and emotional work:
I remember one situation when parents told me—“well, we know the pathology of our dear child, we know that he will only be with us for a few months, and we longingly awaited his arrival; but what shall we do, we need to say goodbye. He should not suffer because of us, he should be as comfortable as possible . . .”—and you know, I was so impressed by this honesty and confidence, also in our team. This nearly blew me away. They were full of love and unselfish. (Nurse)
Constituents of effective EOL care
Participants consistently stressed the importance not only of establishing a sustainable relationship with the child and the family but also of being able to contribute to the well-being of the dying child, providing comfort and creating a peaceful and harmonious atmosphere. They saw several factors as being crucial in communicating with and caring for a child and the family. First, allowing parents enough time and providing support while they came to accept the definitiveness of incurability and finally let their child go. All the professionals stated that the child should be involved in this process as much as its developmental stage and health condition allowed. For HCPs, this implied being contactable and available to provide attention as necessary:
Stopping therapy and the phase directly after it is the most important for me. How the family is supported afterwards . . . This is really a task for the entire team, not only the doctors or psychologists. This is also our job as nurses; we need to accompany the families. How can they go on after this point? How can they handle this situation? What are their questions? They ask many questions about dying and death. How do we answer? What should we anticipate? In my opinion parents can become lost in this phase, thus it is very important. (Nurse)
Even in this phase, parents’ hope can be challenging and needs to be handled carefully, as a community nurse described:
Hope is a very important point. We shouldn’t work against hope and it is very important that we let it go unchallenged. Not unrealistic—we should still talk about unrealistic hopes, but hope as a concept remains very important.
Another aspect of effective EOL care is what participants called “the rhythm of each family’’. To take up with the rhythm of each family refers to the capability of listening attentively to their and their child’s needs, wishes, and sorrows, which might change over the course of the child’s illness trajectory. If necessary, HCPs act as role models and provide space for parents to relate to their child, for example, by facilitating play between parents and child.
Most HCPs maintained contact with the parents after the death of their child in some form. An intensive care physician described the importance of a closure session with parents:
There is always a so-called follow-up discussion after the child’s death . . . we look back on the illness, the course of the illness, treatment, what has happened and how the parents feel now. We encourage them to provide us with feedback. This can be very diverse: some parents are very thankful while others criticize us. But for me, only then is the task fully accomplished.
Challenges in the provision of pediatric EOL care
Many HCPs talked about their general difficulty in defining the goals of treatment anew; notably, to move from curative goals directly to EOL care or the decision to withdraw life support:
For me the hardest time is when treatment objectives need to be newly defined. It is at this moment that we as nurses or doctors realize that there is suffering. This is the point where we really have to change [the focus], provide [the child] with relief and finally need to let it go. For me this is the hardest situation. If the decisions are made as part of a team, it is easier though. (Nurse)
When this transition could not take place, many HCPs felt they were acting against their professional ethical values. This was the case when parents wished to carry on with a futile treatment against the recommendations of the attending team or when specialists and teams did not come to a consensus concerning the treatment of a child. In these situations, particularly the latter, the capacity to act could be hampered, or in the worst cases, totally disabled. Lack of clear leadership in handling a case could even block the decision-making process. As one physician explained,
We [in the team] have huge cultural differences and intense discussions. How should we accompany the families?—From offering everything to . . . It is more this tension that arises when the attending team does not agree on how to accompany a family in this process. (. . .) . . . it is these tensions, these uncertainties and lack of treatment approaches, which sometimes lead to never-ending meetings with twenty people, where nothing is decided, there is no agreement. This affects me very much.
In settings where acute medical actions have priority, such as cardiology or intensive care, the difficulties associated with accepting palliative situations could be even more challenging. Health care professionals reported desperate situations where futile treatments were carried on with, leaving no time for the child and the family to deal with the imminent death, and causing considerable distress:
Such situations are hard for me, where we reach the end of a life and continue the treatment nearly to the end, the last 5 minutes. We are always in action. Nevertheless, we know that the patient will die. We accompany the parents and simultaneously continue the treatment. (Nurse, neonatology)
Closely related to this was a further distressing factor associated with the feeling of failure. In acute care settings, such as neonatology, decisions have to be made within a short time frame, and, depending on the setting, without support from an interdisciplinary team, as was expressed by a cardiologist:
In most cases, I can accept the patient’s and family’s fate. What bothers me most in these cases is the suffering of the parents and siblings. However, the greatest burden for me is to have the feeling, or see that it actually happened, that our treatment did not go very well. That is by far the most stressful situation I experience in my everyday work.
Ethical questions arose in all focus groups in the context of these issues. However, it appeared that ethical instruments were not routinely used even if they were in place. It remained open why structured ethical discussions did not take place or if they took place why they were not regarded as a helpful instrument.
An important further challenge was described in the understanding and function of their own professional role. Unease was expressed if the professional work exceeded the usual professional boundaries of curative work, such as contacting the families at home a long time after the child had passed away:
I exceeded my role as a hospital oncologist [by contacting a family 1 year after the death of a child]. After the [child’s] death I didn’t dare to ask regularly how they were doing, as I had the feeling that this would have been unprofessional . . . Concerning this, we are working in a vacuum.
Communication in EOL care situations was often related to further uncertainties, which already began when a serious diagnosis had to be discussed and bad news delivered to a child and his or her parents. But even after a child’s death, HCPs felt challenged when contacting the family intentionally or meeting them unexpectedly. They asked themselves, “Did I say the right things? Did I react appropriately in this situation?” In intercultural situations, the problem was even more pronounced. One physician described a feeling of “insecurity arising from the unknown” due to lack of knowledge about the traditions of another culture and the behavior considered appropriate when a patient dies. Lack of knowledge, training, and guidelines in PPC and EOL care also seemed to make participants feel insecure. This was less evident in institutions with a specialized PPC team.
Lack of professional and personal support during EOL care was also described as burdensome:
We are talking about serious issues here; we are talking about patients and parents. But what happens with us never interests anyone. Yes, it interests neither our employer nor anyone else. We always need to cope with everything and we never talk about it. (Physician)
The burden resulting from such demanding situations may lead to a higher level of distress for the HCPs than the actual death of the patient. In at least 2 focus groups, there was evidence of risky behavior (alcohol) or traumatization with avoidance behavior, which may also negatively affect the care of a child and the family.
Helpful strategies for coping with difficult situations
Strategies for coming to terms with very stressful situations are individual and depend on the personality of HCPs. Regardless of their profession, traditions such as sending a condolence card to the family after the child died or being present at the funeral were important and helpful. Informal talks with colleagues were also valued.
Some preferences varied with professional background. In general, physicians preferred more analytic discussions such as morbidity-mortality conferences or supervision for debriefing, whereas others preferred to combine analytic discussion with more personal talks with colleagues. As one doctor said,
There is no official follow-up discussion, no official review; or the review is really very factual, organ-related, arranged within the frame of a morbidity-mortality conference, when we receive the pathology reports. Then the case is reviewed from a medical perspective and there’s an attempt to establish an error culture . . . What is important in our team are unofficial, social moments after the morning report, while drinking coffee . . . if someone feels unwell or has guilt feelings . . .
Nurses often preferred to reflect on events in a less medical way with supervision during EOL care situations or in structured debriefing sessions. The participating HCPs described many different rituals conducted in nursing teams. For example, in one PICU, the nurses put a candle, angels, and stones on a little table close to where the patient was before he or she died. Another goodbye ritual is described here:
For two years we have had a goodbye ritual with pastoral supervision twice a year. Every child [who died] over the previous half year receives a place there and we can simply talk about how we dealt with the situations. I realized that sometimes there can still be questions that have not been clarified. Until now, only nurses have participated. (Nurse, PICU)
Participants’ valued talks held in the interprofessional team, but this was only possible in some institutions. Other important resources could be drawn on in an interprofessional approach, such as chaplains’ knowledge about other religions and perhaps new perspectives on a situation developed by involving professionals who did not belong to the “core team” of nurses and physicians.
Needs for improvement in EOL care
Most participants saw great potential for improvement of structures in both hospital and home care settings, as well as in education and training. For this to happen, quite a few things need to be changed on national and societal levels.
Putting specialized PPC teams and thus professional leadership in place was rated as a definite facilitator, supported by the 2 focus groups taking place in institutions with established PPC teams. Such a team should consist of a PPC physician as well as specialists from other professions. The teams should have an advisory function, leaving the care itself to the attending team. Members of the specialized PPC team could act as a neutral third party in cases of conflicts, and they could provide support in caring for children at home and make domiciliary visits:
. . . there would be a team of specialists from Palliative Care who could be consulted, with whom you could have a look at what could be a good path for this child. (Nurse PICU) If only there were pain relief teams in all hospitals, and palliative care teams, who could make home visits, be mobile and not be blocked for some reason or other.
Improving the structures of care in a hospital setting
According to most of the study participants, the current structures of many pediatric hospitals hamper good PPC and EOL care. The shortage of beds and personnel prevailing in PICUs was raised as an aggravating factor in preventing the attending teams from meeting the needs of a family with a child at the EOL:
Parents have very different needs . . . how much time they need to say goodbye. We shouldn’t urge them, they should decide when it happens (to finally disconnect the child from the respirator), who from the family should come before it happens. And then it may happen, that they say that they still need another night, although parents are clear about the decision. And on the next day someone else from the family needs to come.—We are working in the PICU and have limited space . . . Of course there are limits, we can’t say that we’ll wait another week, e.g. in case of a child on a respirator. But we have a certain latitude to allow parents to say goodbye as they need to. (Physician PICU)
Most nurses wished to provide more intense and thus time-consuming care for children at the EOL. This requires financial, human, and spatial resources to allow more family-centered care and provide families with enough privacy, for example, in a separate room.
Continuity and consistency of care is very important, but not always provided. Defining clear and, where possible, standardized procedures for EOL care could be helpful. But also clarity and consensus regarding the treatment are needed, for example, advance care planning, including the definition of responsibilities for complex patients. Patients with complex medical problems may require people from different professions to be involved or even different disciplines. In addition, transitions need to work properly within the institutions, as well as between the hospital and home setting in both directions:
It is extremely hard, because it feels like being in a bubble, like within [name of hospital], it may work, but outside it is completely different. And there the continuity of care is once again harder to achieve, even if we have connections, a network, we know that there are professionals out there . . . [but] the bridges are hard to build, as there are no structures. This is very unsatisfactory. (Nurse)
Improving care in the home setting
Clear regulations for and ways of attending to children medically at home are missing. Physicians are needed who are easily reachable and can make home visits. One physician put it like this:
What I find very hard, as a doctor in the hospital, is to care for patients who are at home for a long time. In such cases I’d wish for a doctor in the neighborhood for whom I can still act as a reference for discussion, but who is available to care for the child. From community nurses we hear that it would be good to have a doctor coming by, but I am employed here in the hospital . . . I realize the needs, also my own wish to visit the patients . . . I would really appreciate the opportunity to take care of patients at home while working in the hospital or having external doctors who are interested in the topic and committed to networking.
Community nurses usually said that they would prefer to have the same specialist from the hospital remain involved in the care of a child at home. This applies not only to physicians but also to psychologists and nurses. Generally, participants said that it would be desirable to have more care options at home.
Vocational training and educational needs
Most participants said that they needed to know more about PPC and EOL care:
If we want to do our jobs in the best possible way, we need to be trained and competent. This may apply to certain participants at this table, but I can’t say that for myself, that I have any special training in caring for dying patients; no psychological or similar training. We somehow work instinctively. Maybe not necessarily wrong, but we have no training. And thus, we need to talk about what competence actually means and which one we need. (Physician)
Topics with highest priority were mostly related to not only medical care, such as symptom management, but also quality of life and providing comfort. Other aspects considered important were communication, building up a relationship with patients and their families, and needs-oriented care and coordination. More knowledge about other cultures and religions and how they deal with illness, dying, and death should also be covered. In addition to patient-related and family-related aspects, many participants expressed the need to learn more about coping strategies, defining their own professional roles and professional boundaries. Such training should be imparted as practically and close to the patient as possible. A specialized PPC team could also be helpful in covering educational needs. In addition, a national database and network were considered important.
Improving policies at the national and societal levels
In general, most participants stated that there was a greater need for public attention and regard to be accorded to EOL in children:
I would like to say that there are children dying and, although there are not many, even if it is just one, it is extremely important that it is well cared for. Even if it is just a small number compared to adult PC, there are children . . . There have to be more well-trained teams and a logistical organization around it. (Physician)
Another need concerns better financing of EOL care to ensure enough human resources. This especially concerns personnel for home care. One community nurse said:
If the families’ needs have been really recognized and addressed . . . and in our area of the home care setting the financial aspects are for sure the fundamental pillars. We always have to fight for the financing of these hours, which are really needed by parents. And we can see that they regularly reach the limits of their resilience in addition to coping with such a stroke of fate.
Health care should be better regulated financially and legally to standardize PPC and EOL care. This would improve quality of care and also access to care. Funding would have to be extended to cover forms of care following the death of a child which have not been paid for up to now, including bereavement care.
Discussion and Recommendations
For the first time, this study focuses on HCPs’ experiences and needs in providing EOL care in all 3 language regions of Switzerland. One main finding was that most participants appreciated EOL care as a very important aspect of their work and also for its influence on their personal growth. End-of-life care was considered a task they definitely wanted to be involved in and did not want the work to be completely delegated to a specialized team. This result should be seen in the context of the increasing specialization and fragmentation in the field of medicine, including pediatrics. Nevertheless, HCPs encountered a number of weaknesses, challenges, and gaps in the care of children at the end of their life that could mostly be overcome by better basic education in PPC and improved institutional support.
Level of the individual HCP
Health care professionals expressed their readiness to be involved in EOL care and do their best to meet the needs of the child and his or her family. The study highlights that ethical aspects of difficult therapy decisions are not discussed sufficiently, and that few hospitals provide adequate debriefing and supervision for staff members.
Pediatric EOL care is mostly provided by HCPs without specialized training in PPC, as was the case with most participants in our study, especially physicians. Thus, many emphasized the need for vocational training and further education in PPC. This result is in line with other studies conducted in Europe, the United States, and Canada showing a high commitment of individual HCPs but shortcomings in their support from superordinate structures, such as institutions and health care structures.31–33
Recommendations concerning the individual HCP
Institutional support structures should be developed covering the different needs of individual HCPs involved in EOL care as well as the different professional groups and levels of experience. Vocational training and further education in PPC should be set up and expanded. The mode of training should be multiprofessional, including modular units related to the specific profession. Besides formal training, “real-life” interventions, teachable moments, and interactive learning tools are valued in the literature.8,33–35 Main topics for this multimodal training include the following: knowledge of the unique needs of children with complex chronic conditions, pain and symptom management (including palliative sedation), communicating poor prognoses, prognostic uncertainty and bad news, discussing resuscitation and withdrawing life support, specific needs of the sick child, including how to talk to the child, supporting siblings and parents, coordination of care, and bereavement support. In addition, the understanding of how families function as a system should be promoted, including cultural aspects and different attitudes toward illness, dying, and death. Collaboration with adult PC training programs could be of interest.
In particular, communication with the sick child and the parents should be regarded cautiously, as this need is well known, and most conflicts have their origin there.36,37 In addition, communication within a team plays a pivotal role in the handling of complex tasks and in preventing errors; it is not only associated with EOL. 38
Level of attending teams and institutions
A clearly voiced need was that for specialized PPC teams which provide support in the care of children at EOL. The holistic concept of PPC would start earlier in the disease trajectory; however, as this study focused on EOL, the complex tasks of PPC teams will not be discussed further. As PPC is not yet established in Switzerland and thus not accessible to all families and teams, the shortcomings described by the participants may reflect the particular situation within Swiss children’s hospitals, which may also be a special case compared with other well-developed European countries.
The interprofessional and interdisciplinary conflicts described that lead to ethical questions and probably inconsistencies in the treatment of an individual child may have further sources outside particular EOL care issues. In some situations, regular ethical discussions could already solve some of these problems and lead to better-balanced treatment decisions. It was unexpected that this well-established instrument within Switzerland was not used more consistently or was at least not experienced more helpful and supportive. Nevertheless, EOL situations can lead to challenging communication between single HCPs, attending teams, and even within institutions. 38 The role of a specialized PPC team in such a difficult situation could be a neutral, independent, and mediating one, providing support to the team and to the family.39–41 Johnson et al 42 showed that clearly assigned tasks facilitate good teamwork within PPC teams and can minimize stress.
“Palliative” patients wish to spend as much time as possible at home. Thus, they also receive care in outpatient and home care settings, which is why we included community nurses in the focus groups. How much support resident physicians and pediatricians provided varied greatly. To allow safe and comprehensive care at home, these nurses formulated their need for better support from physicians and specialists from the treating hospital. At the same time, physicians from the hospital wished support from pediatricians close by the patient’s home, which must not be a contradiction but a concept of collaboration and networking. The quality of care greatly depends on these supportive, well-functioning services.20,43,44 However, even in countries where consultative services are established, these teams do not cover home care. 18
Recommendations for institutions
The urgent need for specialized PPC and pain teams to collaborate in a consultative manner with the attending teams correlates with other studies.18,45 Children’s hospitals should have a concept for EOL care and establish collaboration with specialized PPC teams in larger, mostly tertiary, pediatric hospitals. Large institutions should regularly offer basic education and training courses in PPC and EOL care to meet most HCPs’ need for more training. Particular attention should be paid to communication skills and teamwork, including supervision across all hierarchical levels. Apart from PPC and EOL care, the systematic use of ethical discussions could serve as major support in difficult decisions.
For the home setting, specialized PPC is needed to the same extent as in the hospital and should be provided as such. A networking with existing structures under inclusion of the family’s pediatrician might be a valuable source and also an educational opportunity.
Level of national and public health care
For nationwide advancement in the provision of a particular service, such as PPC and EOL care, greater attention needs to be paid to the particular needs of children having life-limiting diseases and their families.
Recommendations at the level of national and public health care
The decision to provide a formalized service to this vulnerable group of patients should not depend on the decision of individual organizations but on public health care. The impact of such a step could be observed in several countries, particularly Germany among Switzerland’s neighbors, where PPC is much further developed compared with Switzerland. 20
Strengths and limitations
A wide range of HCPs’ experiences and needs were gathered using focus group interviews with interprofessional groups across Switzerland. This allowed a comprehensive perspective from different settings where EOL care is applied. Furthermore, the inclusion of 3 different language regions allowed for detection of national diversities. Many of our recommendations assigned for Switzerland are transferable to other countries, even if PPC is implemented to a higher stage. This applies particularly for educational and training needs in PPC and support from superordinate structures within institutions and higher health care structures.
Several limitations have to be mentioned. First, the focus group method limits the generalizability of our findings, which could have been improved by a mixed-methods approach including a systematic survey with questionnaires. Second, the transferability of data is limited to the Swiss context; however, several findings are in harmony with previous studies in comparable settings. Third, the perspectives of HCPs from existing specialized PPC teams are lacking. This was extensively discussed in the research group, which came to the decision that the current situation of Switzerland lacking general PPC support should be the focus of the study.
Conclusions
End-of-life care is recognized as an important duty of all HCPs across different pediatric settings of care and professions. The key aspect in EOL care provision was the capacity to establish a relationship with the dying child and his or her family and to permit individual and high-quality care. Ethical dilemmas and problems in collaboration within the interprofessional team can hamper this goal and lead to considerable stress among HCPs. Basic vocational training and support from specialized PPC teams should be standard in national concepts for palliative and EOL care in children.
Footnotes
Acknowledgements
The authors would like to acknowledge all participating health care professionals for their contributions, which provided insights into a most delicate area of their work and their personal attitudes on a most complex aspect of life.
Peer Review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 995 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Federal Office of Public Health, Switzerland.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
EB, EC, and PL conceived and designed the experiments; analyzed the data; wrote the first draft of the manuscript; contributed to the writing of the manuscript; agree with manuscript results and conclusions; jointly developed the structure and arguments for the paper. EB and EC made critical revisions and approved final version. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication, authors have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.