
Abstract
Background:
Breast cancer poses a significant public health challenge in Tanzania. Limited knowledge about breast cancer and negative attitudes toward screening practices contributes to delayed diagnoses and poorer patient outcomes. Catholic nuns, who are often nulliparous, represent a population with an increased risk of developing breast cancer. Despite this risk, they remain an understudied group regarding breast cancer awareness and screening practices.
Objective:
This study aimed to assess breast cancer knowledge and attitudes toward screening practices among Catholic nuns residing in Tanzania’s Lake Zone.
Study design:
The study was a cross-sectional design.
Methods:
A total of 385 Catholic nuns participated in the study. To ensure a representative sample, nuns were chosen through simple random sampling, giving each Catholic nun an equal probability of being selected. Data were collected using a self-administered questionnaire and then analyzed using STATA version 18.0. Both descriptive and inferential statistics were used to draw conclusions. In inferential statistics, logistic regression was used to test for associations between categorical variables. The test statistics were considered significant when the P-value was less than .05 at a 95% confidence interval (CI).
Results:
This study enrolled 385 catholic nuns. 57.1% (95% CI, 52.0%-62.1%) of all surveyed catholic nuns had inadequate knowledge of breast cancer. Misconceptions also emerged as significant risk factors for inadequate knowledge. Thus, lack of awareness of breast cancer risk factors increased the odds by 5.57 times (adjusted odds ratio [AOR]: 5.57; 95% CI: 2.84-10.92; P < .001). In addition, believing cancer was not inheritable (AOR: 2.65; 95% CI: 1.14-6.15; P = .024), misperceiving oneself as being in a low-risk group (AOR: 1.65; 95% CI: 1.03-2.66; P = .039), and underestimating the vulnerable age group (believing it is not above 40 years) (AOR: 2.60; 95% CI: 1.49-4.51; P = .001) were all significantly associated with higher odds of inadequate knowledge. Regarding the attitude toward breast cancer screening practices, 62.3% (95% CI, 57.3%-67.2%) of the catholic nuns had negative attitudes.
Conclusion:
These findings highlight the need for breast health intervention educational programs to improve breast cancer awareness among Catholic nuns. Such programs should address risk factors, symptoms, screening methods, and treatment options, dispelling misconceptions. By empowering nuns with knowledge, they can make informed decisions about their health and take charge of their well-being.
Introduction
Breast cancer is the most common cancer and the primary cause of cancer-related deaths among women globally. 1 In 2020, an estimated 2.3 million new cases were diagnosed (representing 1 in 4 new cancer cases), with 685 000 deaths (1 in 6 deaths). According to the World Health Organization (WHO), incidence rates vary significantly across regions. 2 Despite advancements in diagnosis and treatment, breast cancer remains a major threat to women’s health, particularly in low- and middle-income countries (LMICs). 3 These regions disproportionately suffer, accounting for more than 60% of new cases diagnosed in 2020. 4 The burden of breast cancer extends beyond individual suffering, creating substantial morbidity and economic strain on health care systems, societies, and economies.2,4
Sub-Saharan Africa (SSA) faces a stark disparity in breast cancer survival rates compared with developed nations. While developed countries like the United States boast an 86% 5-year survival rate, SSA struggles with a rate below 40%. 5 This concerning gap is projected to widen, with an estimated 19.3 million women, primarily from SSA, likely to be diagnosed with breast cancer by 2025. 6 Several factors contribute to this disparity, including limited access to early detection programs, multimodality treatments, and adequate health care facilities. 7 This signifies that the rate of prevalence of breast cancer among nuns globally is high. 8 A study done by Britt and Short 8 in Verona, Italy, estimated that cancer was 5 times more frequent among Sisters (nuns) than other women and ascribed this excess to an increased risk of breast cancer.
In Tanzania, breast cancer is the second most common cancer, accounting for 14.4% of new cases, and the second leading cause of cancer-related deaths among women.3,9 Alarmingly, breast cancer incidence in Tanzania is projected to rise up to 82% by 2030. 10 This increase, coupled with the fact that most women are diagnosed in advanced stages when treatment is less effective, suggests an increase in breast cancer deaths. 11 Several risk factors for breast cancer have been documented such as family history, genetic and reproductive predisposition, advanced age, and exposure to toxic agents. 12 Due to these risk factors, catholic nuns are among the risk group because they are largely nulliparous, and this puts them at a high risk of developing breast cancer. Their distinctiveness is a greater risk of developing breast cancer than the general population.13,14
Breast cancer screening is crucial for early detection, which increases treatment success and survival rates. Mammography (MMG) is the primary screening tool, but clinical breast examination (CBE) and breast self-examination (BSE) are cost-effective alternatives in resource-limited settings. Early detection saves lives, improves quality of life, and reduces financial burden.15,16 Catholic nuns do not undergo regular screening due to poor uptake of available breast cancer preventive services, limited availability of screening program centers in their convents, inadequate knowledge, misunderstanding of the value of screening, fear of being diagnosed with breast cancer, and fear of stigmatization. 15 This contributes to the failure of early detection of breast cancer among nuns. Although catholic nuns live in monasteries within communities in LMICs, where health promotion programs are in place, their participation in existing programs is low. Studies have shown that poor participation in breast cancer screening is responsible for late diagnosis and poor overall survival outcomes after diagnoses of breast cancer.17,18
However, little is known about general breast cancer awareness, prevention, and early detection practices among catholic nuns from low-resource countries, including Tanzania. This baseline knowledge is essential to the development of culturally and linguistically appropriate educational programs that promote understanding of and attention to evidence-based, lifestyle-directed breast cancer prevention interventions, breast health awareness, and early detection and treatment. Catholic nuns can bring about a significant change in the overall perspective of their lives regarding screening practices and positively influence their attitudes and beliefs. Therefore, this study investigated the breast cancer knowledge and attitudes toward breast cancer screening practices among catholic nuns within Lake Zone in Tanzania.
Materials and Methods
Study design
This study employed a cross-sectional design to recruit Catholic nuns residing in the Lake Zone of Tanzania. A total of 385 Catholic nuns participated in the study. To ensure a representative sample, nuns were chosen through simple random sampling to give each catholic nun has an equal probability of being selected. We focused on the 4 highly populated Congregation centers of catholic nuns within the lake zone. Inclusion criteria were Catholic nuns aged between 20 and above years who were living in convents at the time data were collected with no previous cancer diagnosis and who were ready to participate in the study. The actual data collection of this study was conducted from June to November 2023.
Sample size and sampling procedure
The study recruited 385 catholic nuns residing in the Lake Zone of Tanzania. This sample size was adjusted to account for an anticipated 10% non-response rate. The sample size calculation employed Cochran’s formula for estimating a single proportion, 19 with a desired level of precision of 5% significance level and a prevalence of breast cancer of 34.4%. 20
Data collection tools
The data were collected using a structured questionnaire developed based on a literature review of similar studies on breast cancer knowledge and attitudes toward breast cancer screening practice among women.21 -25 The questionnaire consisted of 4 main sections, Section 1 included demographic questions with 5 questions, and Section 2 included 10 questions to assess breast cancer knowledge, whereby 3 out of 10 questions assess knowledge of the symptoms and signs of breast cancer. Section 3 was designed with 6 behavior and hypothetical questions that can influence individual knowledge. Section 4 consisted of questions to assess nuns’ attitudes toward breast cancer screening. The section had 10 questions, whereby 9 questions assessed attitude and 1 question asked if a nun ever performed breast cancer screening (1 = yes/0 = no), ie, self-breast examination, MMG, or clinical examination.
Pretest
To ensure the questionnaire accurately captured the intended data, we employed a careful 2-step process. First, we established content validity by having a panel of 4 experts review the questionnaire for comprehensive coverage of the target concepts and clarity of language suitable for the target audience. Second, we conducted a pilot test with 35 participants to identify any potential issues with the questionnaire’s wording, instructions, or missing elements. This combined approach of content validity assessment and pilot testing strengthened the overall validity of the questionnaire.
Internal Consistency
To assess the questionnaire’s internal consistency for Likert-type scale questions, Cronbach’s alpha test was calculated. The coefficient from Cronbach’s alpha test was used to assess the reliability of the 9 questions used to assess attitude toward breast cancer screening practices. The results from Cronbach’s alpha test yielded satisfactory results, with an alpha coefficient of 0.8621. Since the reliability coefficient is above the threshold of 0.70 or 70% implying that the attitude data are reliable.26,27
Data analysis
The survey data collected were managed using Microsoft Excel. We use a frequency distribution table to check whether there are missing and erroneous data. Luckily, after data cleaning, we encountered no missing data in our dataset. Thereafter, data cleaned were imported to STATA 18.0 for further analysis.
The 7 items to assess the catholic nuns’ breast cancer knowledge were added up to generate a new variable named knowledge score, with a range of 0 to 7 score. The overall knowledge status regarding breast cancer knowledge was established as a dummy variable whereby respondents with a score below the mean score (<4.08) 28 were regarded to have inadequate knowledge and labeled “1,” otherwise were regarded to have adequate knowledge and labeled “0.” On the other hand, in assessing nuns’ attitudes toward breast cancer screening practices, 9 items were added to establish an attitude score with a range of 9 to 36, whereby the higher the score, the higher the likelihood of an individual having a negative attitude. The overall attitude status regarding breast cancer screening practices was established as a dummy variable, whereby respondents with a score below the mean score (<26.47) 28 were regarded to have a negative attitude toward breast cancer screening practices and labeled “1,” otherwise had a positive attitude and labeled “0.”
Then, descriptive statistics of demographic characteristics, breast cancer knowledge, and attitude items were presented using the Frequency Distribution Table and Figures. In addition, multivariable logistic regression adjusted by the respondent’s demographic characteristics was used to assess factors associated with breast cancer knowledge among catholic Nuns. Notably, all statistical tests were conducted at a 5% significance level.
Results
Socio-demographic characteristics
A total of 385 catholic nuns were enrolled in this study. One-quarter of all surveyed catholic nuns were aged 41 to 50 years old (ie, 17.9% [n = 69] vs 18.4% [n = 71]). Most of the catholic nuns had secondary education level (40.0%, n = 154), followed by degree education (36.1%, n = 139). 32.5% (n = 125) depended on their fellow catholic nuns to get information about breast cancer screening, while 28.8% (n = 111) were informed using Television. Table 1 documents the results.
Participants’ socio-demographic characteristics (n = 385).

Knowledge of breast cancer
The study has shown that more than half of the catholic nuns surveyed had inadequate knowledge of breast cancer (57.1%, n = 220, 95% confidence interval [CI], 52.0%-62.1%). This was attributed by only 38.7% (n = 149) to knowing the meaning of breast cancer, 23.6% (n = 91) know the meaning of the spread of breast cancer, 61.3% (n = 236) think breast cancer presented as a painless breast lump, and 66.7% (n = 257) think that nulliparity women are more at risk to get breast cancer. Table 2 documents the results.
Participant response about knowledge of breast cancer (n = 385).

Knowledge of the signs and symptoms of breast cancer
Furthermore, we investigate the knowledge of the signs and symptoms of breast cancer (Figure 1). It was revealed that 87.3% of all surveyed nuns do not know the swelling of the armpit breast and movable lumps in the breast are some of the signs of the breast, 83.1% think changing the size and shape of the breast is not the signs of breast cancer, while only 33.8% think a changing color or discharge from the nipple could be a sign of breast cancer.

Respondent’s knowledge of the signs and symptoms of breast cancer.
Factors associated with knowledge of breast cancer among catholic nuns
The analysis identified differences in breast cancer knowledge among nuns based on their education level. Nuns with secondary and university degrees had significantly lower odds of inadequate knowledge compared with their less educated counterparts, with adjusted odds ratios (AORs) of 0.46 (95% CI: 0.23-0.91; P = .026) and 0.36 (95% CI: 0.18-0.70; P = .003), respectively. This indicates a protective effect of higher education on breast cancer knowledge acquisition.
However, concerning misconceptions also emerged as significant risk factors for inadequate knowledge. Lack of awareness of breast cancer risk factors increased the odds by 5.57 times (AOR: 5.57; 95% CI: 2.84-10.92; P < .001). In addition, believing cancer was not inheritable (AOR: 2.65; 95% CI: 1.14-6.15; P = .024), misperceiving oneself as being in a low-risk group (AOR: 1.65; 95% CI: 1.03-2.66; P = .039), and underestimating the vulnerable age group (believing it is not above 40 years) (AOR: 2.60; 95% CI: 1.49-4.51; P = .001) were all significantly associated with higher odds of inadequate knowledge. Table 3 documents the result.
Factors associated with inadequate knowledge of breast cancer among catholic nuns.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; P-value, probability value.
Attitude toward breast cancer screening among catholic nuns
We found that 27.5% (n = 106, 95% CI, 23.3%-32.2%) of the surveyed catholic nuns ever performed breast cancer screening, ie, self-breast cancer screening, MMG, or clinical examination. While, more than half of the catholic nuns had negative attitudes toward breast cancer screening practices (62.3%, n = 240, 95% CI, 57.3%-67.2%). The magnitude was attributed by most catholic nuns to have depression on losing one organ of a body and dying with a mean score of 3.06 (0.833), Anxiety after being diagnosed with breast cancer (Mean = 3.07, SD = 0.796), and absence of breast cancer screening and intervention their congregation. Table 4 documents the results. In addition, nuns with a negative attitude were more likely not to practice breast cancer screening practices (chi = 128.17, P < .001).
Attitudes toward breast cancer screening practice among catholic nuns.
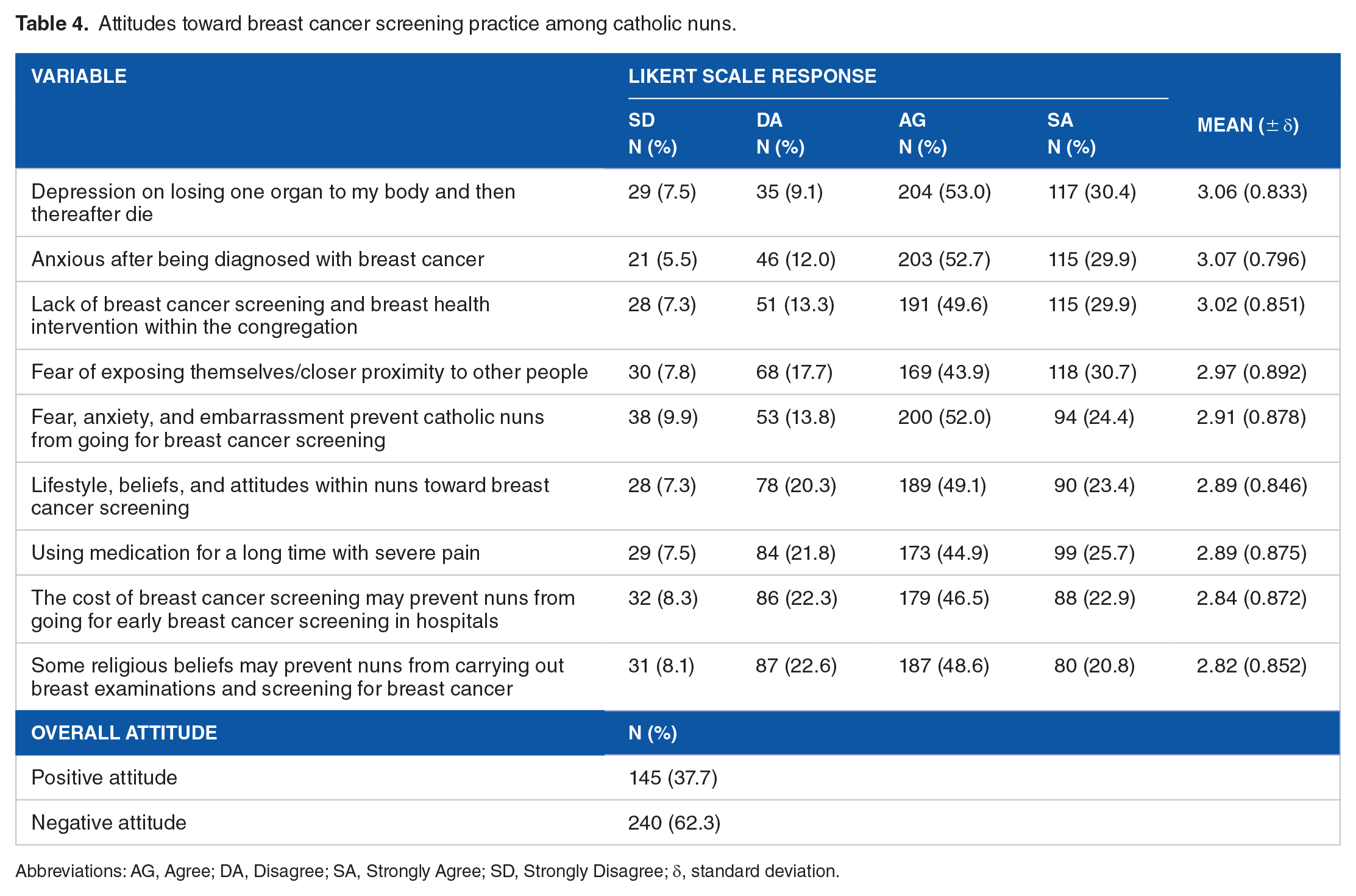
Abbreviations: AG, Agree; DA, Disagree; SA, Strongly Agree; SD, Strongly Disagree; δ, standard deviation.
Discussion
Our study revealed that more than half of the participating catholic nuns lacked adequate knowledge about breast cancer. Notably, a majority were unaware of how breast cancer spreads. However, there were positive findings. Most participants recognized breast cancer as a serious disease compared with others, and more than half understood that nulliparous women (those who have never given birth) have a higher risk. In addition, most nuns acknowledged the importance of early detection for better treatment outcomes. This limited knowledge about breast cancer is concerning and requires intervention. Our findings align with previous research by Joseph et al, 13 which linked inadequate knowledge to lower rates of breast cancer screening among nuns. Similar to our study, a significant portion could not accurately define breast cancer, and most were unaware of its metastatic potential.
Furthermore, our results, similar to a study done by Odusanya and Tayo, 29 reported that only 27% of nurses in a Nigerian hospital demonstrated knowledge about breast cancer. This suggests a broader issue with breast cancer awareness in health care settings. Studies conducted within Saudi Arabia (KSA) by various researchers 21 ,30 -32 also revealed similar trends, highlighting consistently low knowledge and concerning attitudes toward breast cancer screening among women. These findings underscore the urgent need for targeted educational programs to improve breast cancer awareness among catholic nuns and potentially other religious communities. Such programs should address risk factors, symptoms, screening methods, and treatment options. By empowering catholic nuns with knowledge, we can encourage early detection and improve overall health outcomes.
This study identified a concerning lack of awareness regarding early breast cancer warning signs among participants. Recognition of swelling in the armpit or movable breast lumps as potential signs was very low. Similarly, less than half of the participants identified changes in nipple color or discharge as a warning sign. Furthermore, awareness regarding changes in breast size and shape was even lower. These findings align with other researchers. A study by Prusty et al, 33 in Mumbai, India, found a similar lack of knowledge about symptoms, leading to late-stage detection. Likewise, another study in Lagos, Nigeria, revealed low awareness of early warning signs, with only 1.9% recognizing a painless lump as a symptom. 34
Another study conducted in Akinyele Local Government Area, Ibadan, Nigeria, 35 found that only 1.9% of participants identified a painless lump as a warning sign, 6.4% acknowledged swelling, 1 person (0.2%) acknowledged breast skin changes, 2 (0.5%) acknowledged discharge from the nipples, and another 4 (1%) considered nipple retraction as a warning signs of breast cancer. This deficit in awareness could be linked to the absence of educational programs within the studied congregations. A lack of breast cancer training programs and sensitization workshops dedicated to breast health education and addressing cultural sensitivities surrounding the topic might be contributing factors. It is important to note that knowledge about breast cancer is a key factor influencing a woman’s decision to perform regular breast cancer screening, as highlighted in previous studies.36,37
Our study revealed that more than half of the catholic nuns participating held negative attitudes toward breast cancer screening practices. This was evident as most participants agreed that fear, anxiety, and embarrassment prevented them from getting screened. In addition, they reported feeling anxious after receiving a breast cancer diagnosis. Furthermore, the participants revealed that lifestyle choices, personal beliefs, and overall attitudes could hinder their willingness to undergo breast cancer screening. These negative views primarily stemmed from factors including fears of body alteration due to potential treatment procedures, anxieties surrounding the possibility of a positive diagnosis, and the lack of dedicated breast cancer screening programs offered within their congregations.
Our research aligns with Okoronkwo et al 38 in identifying factors that limit breast cancer screening among Nigerian women. These factors include poverty, lack of knowledge about early detection, negative attitudes, and cultural/religious beliefs. Similar to Azami-Aghdash et al, 39 who studied Korean American women, cultural beliefs in Nigeria can lead to embarrassment and fatalism, hindering regular screenings. Studies in South Africa done by Ramathuba et al 40 and Nigeria 41 highlight similar trends. Low knowledge of breast cancer and screening methods is prevalent, despite some awareness. This knowledge-practice gap suggests the need for focused educational campaigns.
These findings align with a study conducted in Eastern Nigeria by Abiodun et al, 42 where only 8.4% of nuns reported performing regular breast examinations and the majority had never practiced BSE. In contrast, a study of Midwestern American nuns found that 37% practiced BSE monthly, while another 37% examined themselves occasionally and only 26% reported never performing BSE. 43 Similarly, another Nigerian study by Lissa 44 revealed low screening rates, with only 34.9% practicing BSE and just 9.1% having received a CBE in the past year. None of the participants in this Nigerian study had ever undergone a mammogram.
A recent study by Joseph et al 13 in Nairobi, Kenya, also found low uptake of breast cancer screening among nuns. Their study identified knowledge of screening options, access to congregational support, and regular hospital check-ups as key factors influencing screening participation. These findings suggest a widespread lack of awareness and knowledge about breast cancer screening among catholic nuns. Despite being a simple, inexpensive, and quick procedure, many nuns either don’t perform BSE at all or do so inconsistently. Several reasons have been proposed for this, including a lack of confidence in performing the examination correctly, fear of discovering a lump, denial, and the association of breast cancer with death. The authors emphasize the need for comprehensive educational campaigns to address misconceptions and encourage catholic nuns to prioritize their health through regular breast cancer screening.
Strengths and limitations
This study serves as the first investigation in Tanzania to explore breast cancer knowledge and attitudes toward screening practices among catholic nuns residing in the Lake Zone. While the cross-sectional design limits establishing cause-and-effect relationships, focusing on this specific population provides valuable preliminary data on their breast cancer awareness. Although the findings cannot be automatically applied to all Tanzanian catholic nuns due to limitations in geographical scope, they offer a crucial starting point. This pioneering study’s contribution lies in its focus on a previously understudied group within Tanzania and its potential to inform future, more extensive research efforts.
Conclusions
These findings highlight the need for breast health intervention educational programs to improve breast cancer awareness among catholic nuns. Such programs should address risk factors, symptoms, screening methods, and treatment options, dispelling misconceptions. By empowering nuns with knowledge, they can make informed decisions about their health and take charge of their well-being.
Recommendations
The findings suggest a need for breast health interventions to improve knowledge and address misconceptions about breast cancer.
Efforts to create a more positive and supportive environment around breast cancer screening program within the congregations.
Encouraging open communication about breast cancer and breast cancer screening practices within the congregations can be beneficial.
To emphasize the need for further research to create more knowledge and utilization of breast cancer screening programs, particularly among under-served populations.
Declarations
Footnotes
Acknowledgements
This study is part of a PhD student thesis (ethical code: CREC/552/2022) approved by the joint Catholic University of Health and Allied Sciences (CUHAS)/Bugando Medical Centre (BMC) Review Board. The authors would like to express their gratitude to the Research and Oncology Department of CUHAS/BMC for their support. We also extend our thanks to the Catholic nuns who participated in the study.
Ethics approval and consent to participate
This study received ethical approval from the joint Catholic University of Health and Allied Sciences (CUHAS)/Bugando Medical Centre (BMC) Review Board (number CREC/552/2022). All participants provided written informed consent before participating. They were informed that participation was voluntary and they had the right to withdraw at any time without penalty. The ethics committee approved the written informed consent procedures as outlined in the CUHAS/BMC committee declarations.
Consent for publication
Not applicable.
Author contributions
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Competing interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.