
Abstract
Background:
Male breast cancer (MBC) accounts for 1% of global breast cancer cases. On account of its rarity, very few prospective clinical trials have been carried out on MBC. Pakistan has the highest incidence of breast cancer in Asia, but very limited data are available on MBC.
Objectives:
The objective is to determine the clinicopathological characteristics and treatment patterns of MBC in Pakistani population.
Design:
This is a retrospective cross-sectional study.
Methods:
A retrospective cross-sectional study carried out using the cancer database of Shaukat Khanum Memorial Cancer Hospital & Research Center. Men with a histologically proven breast cancer, stage 0 to III disease and requiring surgical intervention were included. The Kaplan-Meier curve and log-rank test were used for survival analysis.
Results:
Sixty-eight patients with MBC were included with a median age at diagnosis of 55 years. Most patients were stage II (47.1%). Invasive ductal carcinoma (IDC) was the commonest type (89.7%). Estrogen receptor (ER), progesterone receptor (PR), and Her-2 receptor positivity were 92.6%, 86.8%, and 32.4%, respectively. Mastectomy was performed in 95.6% of the cases. Neoadjuvant and adjuvant chemotherapy was administered in 25 (36.8%) and 26 (38.2%) patients, respectively. Fifty-five (80.9%) patients received adjuvant radiotherapy. Most of the patients (89.7%) received tamoxifen. The 5-year overall and disease-free survival was 88.2% and 80.9%, respectively. Patients receiving neoadjuvant chemotherapy had a better overall and disease-free survival (P = .025).
Conclusions:
Male breast cancer occurs at a relatively earlier age in Pakistani population as compared with Western men. Mastectomy is the preferred surgical option for MBC on account of the advanced disease and delayed presentation. Neoadjuvant chemotherapy has a statistically significant effect on overall and disease-free survival, but in spite of these benefits, it remains underutilized.
Introduction
Male breast cancers (MBCs) account for 1% of global breast cancer cases. 1 Incidence of MBC is on the rise. 2 On account of its rarity, very few prospective clinical trials have been carried out on MBC. Although numerous retrospective studies have been conducted on MBC in developed countries, the challenges associated with record keeping and follow-up has limited the availability of retrospective data from developing countries. Pakistan has the highest incidence of female breast cancer (FBC) in Asia, and although no population-based study has been done on MBC as yet, it can be extrapolated that the country has a relatively high incidence of MBC as well. 3 Lack of awareness, low literacy rates, lack of adequate health facilities, absence of screening protocols, and poor health care system has made addressing challenges posed by breast cancer very difficult in the developing world.4-6 With MBC, these challenges are compounded on account of its uncommon occurrence and the general misconception that breast cancer is an exclusively female disease. 7
Male breast cancer is a disease distinct to its female counterpart in age at which it presents, lymph node stage/status and higher proportion of estrogen receptor (ER)-positive tumors.8-10 These differences make its management different from FBC. The aim of this study is to look at the disease characteristics and treatment patterns of MBC in a resource-limited developing country. This includes analysis of the retrospective data for the preferred surgical modalities, post-operative morbidity, use of neoadjuvant/adjuvant therapy, and the prognostic factors affecting survival in patients with MBC.
Materials and Methods
Design
This is a retrospective, cross-sectional study, carried out using the institutional cancer database. A review of the cases of MBC requiring surgical intervention, during an 11-year period (January 2010 to January 2021), was carried out. Males with a histologically proven breast cancer, stage 0 to III disease and requiring surgical intervention were included in the study. Patients with missing follow-up data and a prior diagnosis of cancer other than MBC were excluded. Variables observed included, demographic information, presenting symptoms, duration of symptoms, Charlson comorbidity index, tumor characteristics, treatment modalities, post-operative morbidity, and disease recurrence. American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines were used for the reporting of ER, progesterone receptor (PR), and Her-2 receptors. The study is being reported in accordance with “Strengthening the Reporting of Observational studies in Epidemiology” (STROBE) guidelines. 11
Statistical analysis
Overall survival (OS) is the time from the diagnosis of the disease to the death of the patient. Disease-free survival (DFS) is the time from the diagnosis of the disease to the first episode of loco-regional recurrence, distant progression, or death of the patient. The Kaplan-Meier curves were used to estimate the OS and DFS, whereas comparison between survival distributions of the samples was done using log-rank test (P < .05). SPSS (Version 26) was used for data analysis and plotting of Kaplan-Meier curves.
Results
Patient and disease characteristics
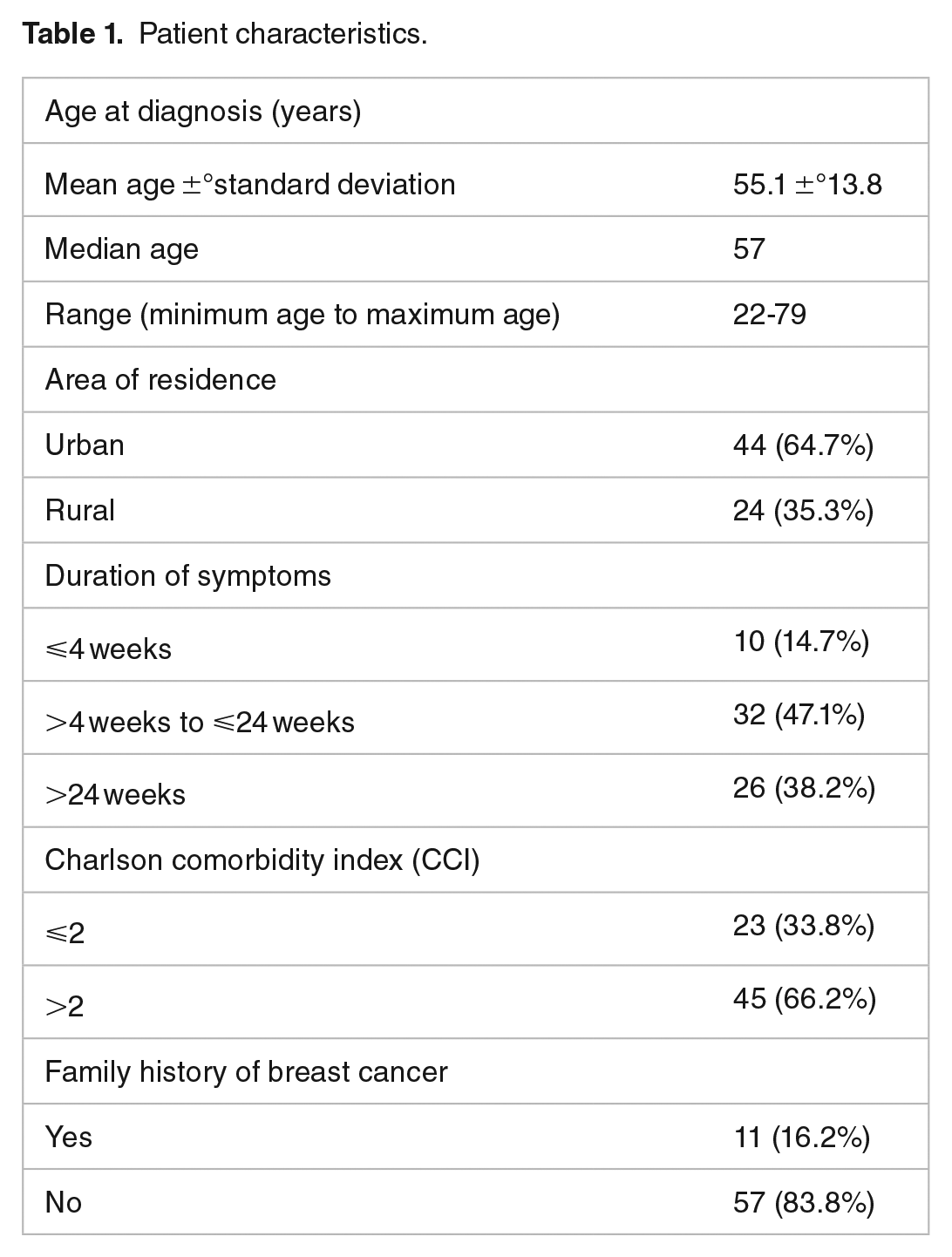
A total of 68 patients were included in the study. The median age at the time of diagnosis was 55 years. 36.8% of patients were 50 years old or younger at the time of diagnosis. The median duration of follow-up was 34.5 months. The median duration of symptoms prior to diagnosis of the disease was 20 weeks (Table 1). Presenting complaints included lump (91.2%), nipple discharge (17.6%), skin ulceration (5.9%), and gynecomastia (1.5%).
Patient characteristics.
Histologically, invasive ductal carcinoma (IDC) was the most common type (89.7%). The rest included ductal carcinoma in situ (DCIS) (5.9%) and rare subtypes (4.4%). At the time of diagnosis, most patients were stage II (47.1%), followed by stage I (36.8%) (Table 2). Disease recurrence was reported in 13 (19.1%) cases, and the median time to recurrence following completion of treatment was 25 months.
Tumor characteristics.

Treatment
Mastectomy was performed in 95.6% of the cases, and only 2 patients (2.9%) had breast conservation surgery (BCS). 26.5% had sentinel lymph node biopsy (SLNB) alone. 67.6% of patients had axillary lymph node dissection (ALND) with or without SLNB, whereas no exploration was carried out in the rest (5.9%). The surgical morbidity rate was 13.2%. These included surgical site infection (7.4%), arm lymphedema (2.9%), and post-operative bleeding (2.9%).
Neoadjuvant and adjuvant chemotherapy were administered in 25 (36.8%) and 26 (38.2%) patients, respectively. 66% of patients receiving chemotherapy had axillary lymph nodes positive for metastasis. 55 (80.9%) patients received adjuvant radiotherapy. 67.3% of these had a tumor size of ⩾5 cm or axillary lymph nodes positive for metastasis. Most of the patients (89.7%) received tamoxifen as an adjuvant endocrine therapy.
Survival analysis
The 5-year OS for the patients included in this study was 88.2%. The 5-year OS Kaplan-Meier curves for the patients according to their stage of disease, age at the time of diagnosis, comorbidity index, nodal status, neoadjuvant and adjuvant chemotherapy are given in Figure 1. The difference in survival was statistically significant only in the case of neoadjuvant chemotherapy (P = .025). Figure 2 shows 5-year DFS for the patients by their T category, nodal status, and administration of neoadjuvant chemotherapy. Disease-free survival difference was statistically significant in the case of neoadjuvant chemotherapy (P = .015). The difference according to nodal status trended toward statistical significance (P = .08).

The 5-year overall survival Kaplan-Meier Curves for male breast cancer patients according to (A) age at diagnosis, (B) stage of disease, (C) Charlson comorbidity index, (D) nodal status, (E) neoadjuvant chemotherapy administration, and (F) adjuvant chemotherapy administration.

The 5-year disease-free survival Kaplan-Meier Curves for male breast cancer patients according to (A) nodal status, (B) T category, and (C) neoadjuvant chemotherapy administration.
Discussion
Our work is one of the first studies originating from Pakistan on MBC and describes the disease characteristics and preferred treatment modalities in this population. The median age of diagnosis was in the late fifties in contrast to developed countries where it tends to be in the mid to late sixties.9,12,13 This is similar to FBC, which also occurs at an earlier age in Pakistani population as compared with the Western population.14,15 Our study confirms that IDC is the most common histological subtype of MBC.9,12,13,16-18 Lobular breast carcinoma is very uncommon among men, as lobules and acini are not present in male breast. 19 Most patients (91.3%) presented with stage II or III, which is in contrast to the work of Mangone et al, who reported 40% stage I and 54% stage II or III tumors in Italian population. 10 This indicates a relatively advanced stage of disease at the time of diagnosis in the Pakistani population as compared with its Western counterpart.10,12,13,18 This was further confirmed by the increased likelihood of axillary nodal metastasis in our patients.9,12,13 The factors accounting for this delayed presentation in patients of male breast carcinoma have not been investigated; however, illiteracy, poor social status, and lack of appropriate health care facilities have been identified as factors responsible for delayed presentation of FBC in developing countries,4-6 and some of these factors may be responsible for the delayed presentation of males with breast cancer. We found MBC to be ER and PR positive in most of the cases, and this finding is supported by the existing literature.12,13,17
A vast majority of the patients underwent mastectomy. This was the case despite the fact that there is no proven significant survival difference between males undergoing BCS and mastectomy.9,12 Zaenger et al reported comparable survival outcome between early MBC patients undergoing BCS and modified radical/simple mastectomy, even though only 46% of the BCS patients received adjuvant radiotherapy to complete the traditional breast conservation therapy. 20 Cloyd et al found that MBC patients undergoing BCS were more likely to be older and have advanced disease at the time of diagnosis. Despite these findings, breast cancer-specific survival was unaffected by type of surgery. 21 Breast conservation surgery, therefore, is a viable yet underutilized surgical option for MBC.9,12,20-22 However, the actual number of suitable candidates for BCS may be limited given the scanty breast tissue in males and the retroareolar location of MBC in many of the cases, both of which makes challenging the excision of the tumor with adequate margins. Breast conservation surgery is a less feasible surgical option in the Pakistani population given the delayed presentation and advanced stage of the disease at the time of diagnosis as compared with the Western population. These results are hardly surprising as mastectomy remains the commonly practiced surgical option even for FBC in the developing world on account of factors such as poor follow-up and lack of radiotherapy facilities.23-25 Surgical evaluation of the axilla was carried out in most of the patients (>90%) with SLNB being used adequately for staging of clinically node-negative patients.
Adjuvant radiotherapy has been proven to increase local control in MBC patients following mastectomy. 26 It also improves OS, especially in men with positive lymph nodes. 26 In spite of these advantages, adjuvant radiotherapy remains underutilized.9,12,13 This is in contrast to the 55 (80.9%) patients in our retrospective analysis who received adjuvant radiotherapy. Oncological outcomes after neoadjuvant chemotherapy (NAC) are similar in lymph node-positive MBC and FBC; however, NAC is used to a lesser extent in males. 27 This observation was confirmed by our study as only 36.8% of the patients received NAC even though a higher proportion of patients presented with locally advanced breast cancer.
A 5-year survival rate of 84.7% was reported in MBC patients in a review of Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries (NPCR). 28 This needs to be interpreted with caution as stage IV cases were also included in the study. The 5-year OS in our study was 88.2%. Residences in high-income areas, PR-positive tumors and administration of chemotherapy, radiotherapy or endocrine therapy are some of the factors that have been reported as associated with better OS. 13 We found that only NAC had a statistically significant effect on OS and DFS. This can be explained by the low power of this study because of the small sample size. A limitation of our work is the absence of metastatic disease, inclusion of which would have given important information about the characteristics of the disease at the time of diagnosis. Our study relied on data from a single center, and although it highlights the clinicopathological features of the MBC in Pakistani population, the mode of treatment and the OS/DFS cannot be generalized to the Pakistani population because a great deal of institutional variation is expected in these. Most of the cancer patients receive treatment at public sector hospitals, which are overburdened and under resourced. 29 The OS/DFS of the patients being treated at our center, which provides integrated cancer care under one roof, may be better than the patients receiving treatment in public hospitals. A nationwide collection of long-term clinical and outcome data in public, private and trust hospitals is suggested to get a better understanding of the MBC in Pakistani population.
Conclusions
Male breast cancer occurs at a relatively early age in Pakistani population, and most are hormone receptors positive. Mas-tectomy is the preferred surgical option for MBC due to the advanced disease and delayed presentation in Pakistani patients. Neoadjuvant chemotherapy has a statistically significant effect on OS and DFS, but in spite of these benefits, it remains underutilized in the management of MBC patients. To address the shortcomings of our study, we propose a nationwide prospective study of MBC, incorporating public and private sector hospitals.
Supplemental Material
sj-docx-1-bcb-10.1177_11782234241233120 – Supplemental material for Clinicopathological Features and Treatment Outcomes of Male Breast Cancer in Pakistani Population: A 10-Year Retrospective Cross-Sectional Study
Supplemental material, sj-docx-1-bcb-10.1177_11782234241233120 for Clinicopathological Features and Treatment Outcomes of Male Breast Cancer in Pakistani Population: A 10-Year Retrospective Cross-Sectional Study by Ibtissam Bin Khalid, Albash Sarwar, Hassham Bin Khalid, Barka Sajjad, Bushra Rehman and Muhammad Asad Parvaiz in Breast Cancer: Basic and Clinical Research
Footnotes
Acknowledgements
The authors acknowledge Dr Amina Iqbal Khan, for providing expert opinion and proof reading the manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.