
Abstract
Invasive breast cancer with axillary lymph node (LN) invasion is a continuing problem worldwide. The morbidity associated with axillary LN dissection along with the high rate of nodal downstaging after neoadjuvant chemotherapy (NACT) made the standard treatment shift towards less invasive surgery. Sentinel lymph node biopsy (SLNB) after NACT is associated with high false-negative rates (13%-14%). To overcome this problem, it was concluded that the positive nodes should first be indicated with image-detectable markers and then removed together with SLNB: targeted axillary dissection (TAD). This review aims to describe and evaluate the different marking techniques for TAD in patients with node-positive breast cancer treated with NACT, namely: clip placement and guidewire localization; clip placement and 125I-labelled radioactive seed localization; clip placement and skin mark; clip placement and intraoperative ultrasound; tattooing with a sterile black carbon suspension; magnetic seeds; radar and infrared light technology localization. Targeted axillary dissection techniques have shown false-negative rates below 9% and identification rates above 95%. The most studied technique is guidewire localization, as it is also the oldest one. However, according to data gathered from this review, some newer techniques have shown to be very promising due to their statistical results and management factors.
Introduction
Over the last century, surgical procedures in breast cancer patients have evolved from being disfiguring to relatively noninvasive. 1 The management of invasive breast cancer involves the effort of a multidisciplinary team to establish a correct diagnosis and staging. 2 Not only the type of systemic therapy, surgery, and radiation is decided according to the lymph node (LN) status but also the prognosis depends on the presence of nodal metastases.3 -6 In breast cancer patients with axillary metastasis, neoadjuvant chemotherapy (NACT) results in a complete pathological response in a still growing number of patients, which is due to improvements in the systemic treatments, mainly for triple-negative and human epidermal growth factor receptor 2 (HER2+) subtypes. 4 The high rate of nodal downstaging has led to the acceptance of sentinel lymph node biopsy (SLNB) to stage the axilla after NACT in patients who had a clinical and radiological complete response (40%-75%).4,7 Such paradigm shift allowed avoiding most axillary lymph node dissections (ALNDs) after NACT and its morbidity effects such as pain, paraesthesia, shoulder dysfunction and, more significantly, lymphoedema.8,9 Therefore, management of the axilla has shifted into a less radical and less invasive approach. Furthermore, in line with the ACOSOG Z0011 and AMAROS clinical trials, which showed no benefit of the completion ALND in selected patients with positive sentinel LN(s), current guidelines state that SLNB is sufficient, even in the case of nodal involvement, in most patients with small tumours who are receiving adjuvant therapies.10 -12
However, SLNB alone after NACT has a high false-negative rate (13%-14%) and, when the initially metastatic LN is marked, the sentinel LNs did not correspond to it in 23%.7,13 As the sentinel LN is the hypothetical first LN (or group of nodes) to which a cancer can drain to, this means that other nodes in the axilla can have residual disease, reinforcing the idea that SLNB is not enough to achieve the desired detection results. This also suggests that NACT can alter axillary lymphatic drainage pathways, leading to high false-negative rate (FNR). 14 To overcome these issues, the positive nodes should be marked before NACT, with an image-detectable marker, and then removed together with SLNB after NACT – targeted axillary dissection (TAD). After Caudle et al 3 showed that adding the excision of the clipped node to the SLNB was able to reduce the FNR to 1.4%, this strategy has been endorsed by some guidelines.10,13 In fact, with an FNR of 2%, oncological compromise would only affect approximately 1 in 10 000 patients, which does not justify the need for a more invasive strategy. 13
The best technique for TAD in patients with initially node-positive breast cancer who are clinically negative after NACT is still unclear. This review aims to describe and evaluate the different marking techniques for TAD in patients with node-positive breast cancer treated with NACT. The techniques will be compared for feasibility, advantages and disadvantages, specific side effects, identification rates (IRs) and false-negative rates. In addition, it will be briefly discussed in which sense these techniques can improve the treatment and quality of life of these patients.
Materials and Methods
An online search was conducted at PubMed with the search equation: ‘Breast Neoplasms’ [Mesh] AND neoadjuvant AND axilla*. The search was restricted to articles written in English, published in the period from 2010 to 2021. All types of articles were selected for review. Approximately 800 published articles were assessed. The studies considered relevant from the bibliographic references of the selected articles were also analysed. A total of 32 articles were selected as relevant references for this review, with preference for the most up-to-date literature.
Comparison of Technologies
Clip placement and guidewire localization
This technique, which has been used to localize nonpalpable lesions in the breast, could be adapted to use in the preoperative image-guided localization of axillary LNs. 4 To correctly allocate the wire, mammography, ultrasound (US), and magnetic resonance imaging (MRI) can help localizing the LNs. 4 The low price point and the familiar, yet complex, surgeons and radiologists’ workflow may seem the primary benefits of this technology. Due to the risk of migration, the placement and removal must be performed on the same day.4,15,16 The wire is easily visualized protruding from the skin and can be followed by the surgeon to reach the targeted LN. 4 There has been some hesitation (both from radiologists and surgeons) to use these wires due to its known complications such as pain, hematoma, and adjacent tissue injury. 4 It was demonstrated a good concordance between the retrieval of the clipped node and the sentinel lymph node (SLN) (86%) associated with an accurate retrieval of the clipped node (92%). 9 The clipped node IR was of 97% when wire localization was used.9,11
Clip placement and 125I-labelled radioactive seed localization
The use of labelled radioactive seeds as a localization technique was initially designed for nonpalpable lesions in the breast. However, it is currently being adapted for the axilla. 4 The radioactivity level within the 125I-seed ranges from 0.1 to 0.3 millicuries, with a half-life of 60 days, which makes the scheduling of surgery easier besides being considered safe for human exposure.4,16 This technique’s advantages include decreased risk of displacement, better patient comfort and lower potential of injuries to the surrounding vascular structures during surgery. 16 Concerning the drawbacks, the most obvious is the exposure to radiation. It is not only an expensive and a complicated procedure, but it also faces legal problems for retrieval and disposal of radioactive materials. 4,15 It also requires the involvement of a nuclear physician and does not provide real-time visual guidance. 17 Nevertheless, the dose of radiation is small, and there is no significant exposure to people who may come into contact with the patient before or after surgery. 4 Seed loss, the need for special instruments to identify the seeds and seed migration are other potential disadvantages of this technique.9,18 Applying a marker clip to LNs under US guidance and then marking these LNs post-NACT with radioactive I125-seeds achieved an IR of 96.7% and concordance among clipped LNs and SLNs reached 91%.19,20 The clipped node was associated with FNR of 4.2%, and specifically localizing and removing the clipped node in addition to removal of SLNs resulted in an FNR of 2.0%. 16
Clip placement and skin mark clipped axillary nodes
Preoperatively, the clip localization was marked on the skin with the arm abducted at 90°, with an US probe placed perpendicularly to the skin. Then, a 21G needle is inserted perpendicularly into the skin to place the clip. Identification of the clip was based on its perpendicular distance from the skin, and morphology and position were determined relatively to surrounding structures based on pre-NACT diagnostic US. 7 In the SMART trial, there were no complications with the clip placement. Despite its different types, the one that had the highest rate of identification was the UltraCor Twirl (100%), mainly due to the improvements in its US visibility.7,21 When comparing to the visibility of other clips, these are still suboptimal, with reported rates of only 72% to 83%. This is mainly due to the NACT that causes shrinkage and fibrosis of the LNs, making them less hypoechogenic on US and harder to identify against a background of echogenic fat. 7 The advantages of this technique include it being noninvasive, wireless and radiation-free. It is also less expensive than other localizing devices and more accessible to health centres. 7 No complications of this technique were reported. Limitations of SMART trial included a small sample size and, as all patients underwent ALND, it was not possible to assess the compatibility with SLNB and to evaluate the FNR. 7
Clip placement and intraoperative US
Size, morphology, internal echogenicity, disproportionate enlargement, presence of eccentric or uneven cortical thickening and abnormal ‘rounding’ shape are sonographic features that characterize malignant LNs 16 (Figure 1).

Metastatic LN marked with a clip (yellow arrow), before NACT.
However, the Z1071 trial exposed evidence demonstrating that US is not a precise method for identifying normalized axillary nodes following NACT as more than 50% of cases are still pathologically positive. 22 It also concluded that TAD is a more accurate procedure for staging the LNs after NACT.2,9,22 This led to the use of marker clips to be identified by US. These can be divided in 2 categories: a metallic clip typically made of stainless steel or titanium and a sonographically visible metallic clip with an associated bioresorbable material typically made of collagen, polylactic acid, or polyglycolic acid, which absorbs water over time. 4 Although some studies refer this technique to not have any problems regarding clip migration or complications related to the clip insertion or patient distress, others are worried about the possibility of migration and extrusion.23,24 This is a situation that can happen in 50% of procedures using sonographically visible water-absorbing clips. 4 Nevertheless, there is the advantage of the time that a clip can remain visible, making the scheduling of surgeries and clip placement much easier.4,24 In addition, it is also a very cost-effective technique, and in re-excision rates, it can be superior to wire localization. 25 The technique is very safe in experienced hands, with close to a 100% success rate.7,24 In 1 study, 95.7% marker clips were identified preoperatively and successfully removed using intraoperative US; in the remaining patients, the HydroMARK clip was successfully removed after ALND. 4 This suggests that sonographically visible hygroscopic or metallic clips could be a reasonable choice for use in intraoperative US axillary localizations. 4
Tattooing with a sterile black carbon suspension
For tattooing, black ink was injected adjacent to the soft tissue and into the cortex of the node through US guidance. The radiologist marked the location of the LN on the skin with an oil-based pen to guide the surgical incision.26,27 Tattooing with activated charcoal has been reported to yield high IRs in preceding studies of 95% to 100%,19,26 -28 Black ink has the advantage of being identified up to an average of 130 days19,27,28 as well as being an affordable alternative to the already existing methods. 19 It is also unnecessary to verify the removal of a clip or radioactive seed during surgery. 27 There is also some clinically negligible risk of charcoal absorption or migration and the long-term complications of tattooing should be further validated using cohort studies. 27 The diagnostic performance of TAD using sterile black carbon suspension showed values as follows: FNR 8.3% and accuracy 95%. Concordance among tattooed LNs and SLNs is not absolute, indicating an improvement in the accuracy of post-NACT SLNB with the help of TAD as this technique selects to remove marked LNs not supposed to be SLNs. 19
Magnetic seeds
The magnetic seed uses a 1 × 5 mm surgical stainless-steel marker.4,29 It can be detected using a magnetometer (Sentimag®), which provides information about how far away it is and its direction to the marker. 18 Seed placement performed under US guidance is similar to sonographically guided clip placement. The seed is localized in the operating room using the Sentimag® magnetometer.4,18 Magseed® appears to be an accurate, safe and nonradioactive method for precisely localizing axillary LNs, with 97% of target LNs being successfully removed in surgery. 18 On a trial, seed loss was reported in 1 patient. Besides that, no documented complications occurred. 18 Major disadvantages of using magnetic seeds are the cost of each seed and depth limitation.9,18,30
Radar and infrared light technology localization
Nonradioactive infrared (NIR)–activated electromagnetic wave reflector is implanted under imaging guidance, and an audible signal from the implanted reflector is then detected percutaneously using the manufacturer’s system.4,15,31 The use of NIR fluorescence for SLN mapping has several advantages over conventional modalities such as real-time visual guidance, superior depth penetration, as well as broader availability compared with radioactive tracers. 17 Also, the reflector is approved for long-term placement so it could be placed before the NACT. Due to its scheduling benefits, lower levels of anxiety, better comfort and improved clinical management were achieved. 32 No cases of reflector migration were reported.4,15 Considering the greater scheduling flexibility, shorter operating times, lower re-excision rates and reduced deployment times, it may be possible to make some indirect financial savings due to its effectiveness in spite of its initial higher and recurrent cost. 32 The clip is 12 mm long which is relatively large compared with the normal-sized LNs. This may cause some uncertainty regarding the placement as it may need to be placed adjacent to an abnormal LN.4,15 Savi SCOUT®, which is an approved console to detect reflectors’ localization, was successful in 97% (125 of 129; 95% confidence interval [CI] = 92%-99%) patients. Of the 4 unsuccessful cases, 3 were due to an inability to obtain an audible signal. 31 Nonetheless, this indicates that this technology is highly accurate and may help to successfully retrieve metastatic nodes and facilitate surgical planning in the axilla. 4 It was reported a re-excision rate of 12.8% (Table 1). 15
Comparison of targeted axillary dissection techniques.
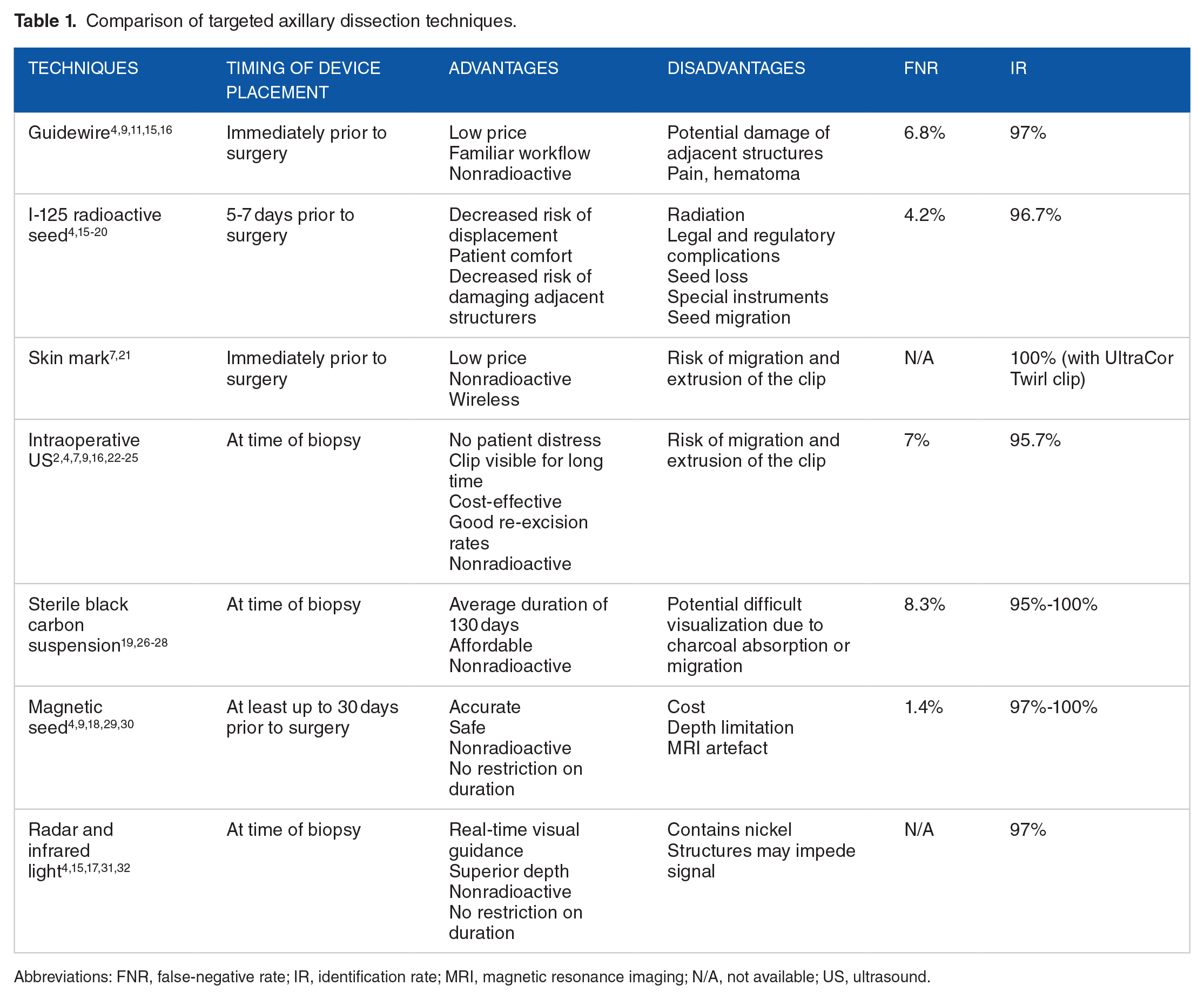
Abbreviations: FNR, false-negative rate; IR, identification rate; MRI, magnetic resonance imaging; N/A, not available; US, ultrasound.
Conclusions
Identifying metastatic nodes in the axilla after NACT is of the outmost importance in medical practice today. Therefore, there is an attempt to improve its current techniques. This is a necessity that arose from the limitations of the standard SLNB presenting an FNR above 10%, making it unsuitable for safely staging breast cancer patients.
To overcome this problem, several marking techniques for TAD were developed: clip placement and guidewire localization; clip placement and 125I-labelled radioactive seed localization; clip placement and skin mark; clip placement and intraoperative US; tattooing with a sterile black carbon suspension; magnetic seeds; radar and infrared light technology localization. Globally, TAD has presented FNR below 9% and IR above 95%. The most studied technique is guidewire localization as it is also the oldest one. However, according to data gathered from this review, some techniques have shown to be very promising due to their statistical results and management factors. For example, tattooing with a sterile black carbon suspension or clip placement and skin mark clipped axillary nodes could be a more practical option. They both performed equal or above the other techniques while only requiring the clip or the ink and US technology to place it correctly. The US component is a well-known technology which most health facilities have access to, besides being a more affordable option.
Even though it has been understood that TAD is more precise than SLNB alone, to better understand this procedure and maximize its potential, more studies need to be conducted, including larger number of patients.
Footnotes
Acknowledgements
Not applicable.