
Abstract
Background:
Breast cancer molecular subtypes share various prognostic profiles, and luminal A molecular subtypes have a better prognosis compared with other molecular subtypes. However, whether metabolic syndrome or individual risk factors of metabolic syndrome influence on the development of molecular subtype remains elusive. We aimed to assess the association between metabolic syndrome risk factors and breast cancer molecular subtypes among patients with metabolic syndrome in a clinical setting.
Methods:
In total, 101 breast cancer patients with mean age, 58.4 ± 8.5 years, and overt metabolic syndrome prospectively were recruited. Immunohistochemistry procedure was used to determine molecular subtypes. Assessment of clinical, biochemical, and anthropometric parameters was performed. Logistic regression analysis was used to assess the relationship between risk factors and breast cancer molecular subtypes categories. A similar approach was used to assess the relation between breast cancer molecular subtypes and menopause.
Results:
Comparison of metabolic syndrome individual risk factors according to breast cancer molecular subtypes no statistical difference was found for systolic (P = .33) and diastolic blood pressure (P = .17), fasting glucose (P = .77), triglycerides (P = .62), high-density lipoprotein (P = .33), body mass index (P = .87), and waist circumference (P = .81). A positive trend was found between high-density lipoprotein and HER2+. No association was found with other risk factors. Moreover, an association was found between HER2+ categories and menopause.
Conclusion:
In breast cancer patients with metabolic syndrome, we observed an increased trend between high-density lipoprotein and HER2+ molecular subtype, suggesting that underlying dyslipidemia may favor poor prognosis. HER2+ was associated with menopause which may influence further expression of HER2+ .
Introduction
Breast cancer (BC) among the women is the main cause of cancer mortality in developing countries, 1 and the second cause of cancer deaths in developed countries. 2 Breast cancer is a heterogeneous disease, and the presence of various receptors determines pathological heterogeneity by intrinsic molecular subtypes. 3 Breast cancer intrinsic molecular subtypes are categorized as luminal A, luminal B, human epidermal growth factor receptor 2 positive (HER2+), and triple negative (TN). 4 The BC molecular subtypes differ in treatment and their prognosis.5,6 Previous studies suggest that the metabolic syndrome (MetS) and BC link varies by intrinsic cancer subtype.7-9 Metabolic syndrome as a spectrum of conditions that includes abdominal obesity, high glucose levels, dyslipidemia, and the presence of hypertension. Hence, MetS was reported to be associated with an increased risk of BC. 9 Individual risk factors of MetS such as body mass index (BMI) were more likely associated with hormone receptor-positive tumors.10-12 A more recent study reported that obesity negatively impacted on survival and incidence of distant metastasis in women with BC with specific molecular subtypes, for example, HER2+. 13
In the last decade, molecular profiles and gene assay have contributed to highlighting the heterogeneous nature of BC. 14 However, in women with MetS, few studies have investigated the association of MetS individual risk factors with molecular subtypes of BC and their impact on molecular subtypes of BC remains scarce. Furthermore, a lack of epidemiological data from developing countries on the prevalence of MetS, on one hand, and the other hand rise of BC incidence in these countries with the younger population, should be considered an utmost priority.15,16 Understanding the role of the individual risk factors of the MetS on the development or progression of molecular subtypes of BC with poor prognosis may provide important alternatives for disease prevention and health cost expenditures reduction in respective countries. Furthermore, given intervention policies in the prevention of MetS in the general population may serve as a strategy and preventive program for cancers or BC in particular. 17 Thereby reducing the risk of BC in women using interventions strategies in practice for the reduction of cardiovascular diseases such as blood pressure and/or lipid-lowering, accounting that MetS is a crucial risk factor for cardiovascular disease, may be an important opportunity for risk reduction and BC in women with MetS, also.
Therefore, we aimed to investigate the association of the MetS individual risk factors with molecular subtypes of BC among newly diagnosed BC women patients with and without menopause.
Methods
Study population
Between periods of January 1, 2019, until December 31, 2019, newly diagnosed BC women patients at the Oncology Clinic of University Clinical Center of Kosovo were prospectively recruited in the study. Breast cancer diagnosed patients (n = 363) with histological confirmation received on cological treatment at the clinic. Before the individual treatment patients were assessed based on the presence of the 3 or more NCEP ATP III criteria. 14 Out of total patients (n = 363), only 150 BC patients met MetS criteria for inclusion. 18 Patients having 2 or fewer MetS risk factors were excluded. Women with BC (n = 101) and MetS were included in the analysis and patients refused to participate were excluded (n = 49).
The study has been approved by Ethics Committee of Faculty of Medicine and decision number 7036. All participants were informed consent and study compiled with principles of the declaration of Helsinki on human research. 19
BC molecular subtypes assessment
The immunohistochemistry staining process was performed by independent pathologists, blinded for patients characteristics and clinical information, on fresh or frozen BC tissue removed during the biopsy according to American Society of Clinical Oncology/College of American Pathologists guideline recommendations. 20 Immunohistochemically staining for estrogen receptor (ER), progesterone receptor (PR), HER2, and Ki67 was implemented in paraffin-embedded primary tumor tissue incisions and fixed in formalin.21,22 After microwave incubation with citric acid (10 mM), mouse monoclonal antibodies of ER, PR, HER2, and Ki67 were applied for 30 min at room temperature using diluted solutions such as anti-ER-1-100; anti-PgR-1-80; before dilution anti HER2; anti-Ki-67-1-200.23,24 After 3 rinses in Tris solution (TBS) and incubation with secondary antibody, positive brown staining was detected by standard avidin and peroxidase (ABC) technique with 3.3-diaminobenzidine (DAB) as the chromogen. The samples were stained with Mayer’s hematoxylin for 10 s, dried in alcohol, and evaluated. Estrogen and PR’s presence was tested, and positive (+) samples from the immunohistochemical examination were noted. The presence of HER2 receptors is included all results with a +++ score from the immunohistochemical analysis. In cases where HER2 is determined by ++ or otherwise as equivocal, then the tissue sample is further investigated by the FISH or CISH method to determine the amplification status of the HER2 gene. Molecular categories were correlated with immunohistochemical biomarkers. Determination of molecular subtypes was made by immunohistochemistry procedure and molecular subtypes were classified as luminal A (ER positive and/or PR positive/HER2-negative, Ki67 ⩽ 20%); luminal B (ER positive and/or PR positive/HER2 positive, Ki67 ⩾ 20%); HER2 positive (ER negative/PR negative/HER2 positive/any Ki67), and triple negative (ER negative/PR negative/HER2 negative/any Ki67). 25
MetS assessment
Metabolic syndrome assessment has been done by NCEP ATP III criteria.18,26 The 5 criteria were included: waist circumference (WC: >88 cm); triglycerides (>150 mg/dL or 1.7 mmol/L or on treatment); low high-density lipoprotein (HDL) cholesterol (<50 mg/dL or 1.29 mmol/L or on treatment); arterial blood pressure (>130/85 mm Hg or on antihypertensive treatment); fasting glucose (>100 mg/dL or 5.6 mmol/L or on antidiabetic treatment). Patients having 3 or more risk factors according to NCEP ATP III criteria have been diagnosed with METS.
Laboratory parameters assessment
Venous blood samples have been taken from all patients to determine biochemical parameters: triglycerides, HDL-cholesterol, and fasting glucose. The concentration of triglycerides has been determined by the enzymatic method with glycerol-3-phosphate oxidase (endpoint). The principle of the method is based on the hydrolysis of triglycerides by the action of the lipase enzyme and the conversion of glycerol obtained by the action of the glycerol-kinase enzyme to glycerol-3 phosphate. The principle of the method for determining the concentration of HDL-cholesterol is based on the reactions during which the cholesterol of low-density lipoprotein (LDL), very-low-density lipoprotein (VLDL), and hilo-micron fractions are decomposed by the action of the cholesterol-oxidase enzyme. The substance found in the working reagent solubilizes cholesterol from the HDL fraction and subsequently, HDL-cholesterol is determined by the enzymatic method, cholesterol oxidase. The serum glucose measurement was done through COBAS INTEGRA Glucose HK tape (GLUC2). The system contains in vitro diagnostic reagents for use in the COBAS INTEGRA system for the quantitative determination of glucose concentration.
Other measurements
Office blood pressure was measured in all patients in sitting position, and the mean of 2 consecutive measurements with an interval of 5 min difference was recorded. Anthropometric measurements included weight and height also. Body mass index was calculated as a weight divided by squared height. In standing, position, and gentle breathing WC was measured at the midpoint between the lower rib and the iliac crest in all patients. Study questionnaires have been used to collect information on physical activity, menstrual status, hormone replacement therapy use, age of the first pregnancy, breastfeeding, status of menopause, alcohol use, smoking status, cancer family history, the education status, and residence area.
Statistical analysis
Distribution of continuous and categorical variables was provided using standard methods to compute mean, standard deviation (SD), and frequencies with percentages (%). The departure from normality was evaluated using Shapiro-Wilk’s statistics. The analysis of variance (ANOVA) was used to compare MetS individual parameters according to BC subtypes categories. Similarly, MetS individual parameters were compared according to menopause status (Figure 1). Logistic regression used to assess the relationship between MetS parameters and molecular subtype categories, in univariate analysis (Figure 2). Furthermore, the same approach was used to assess the relation between molecular subtypes and menopause, and a luminal A category was used as a reference group. A statistical test was conducted with 2-sided significance, and P values ⩽ .05 were considered statistically significant. Statistical analysis was performed using SPSS version 21 IBM SPSS Statistical package version 21 (Chicago, IL, USA).
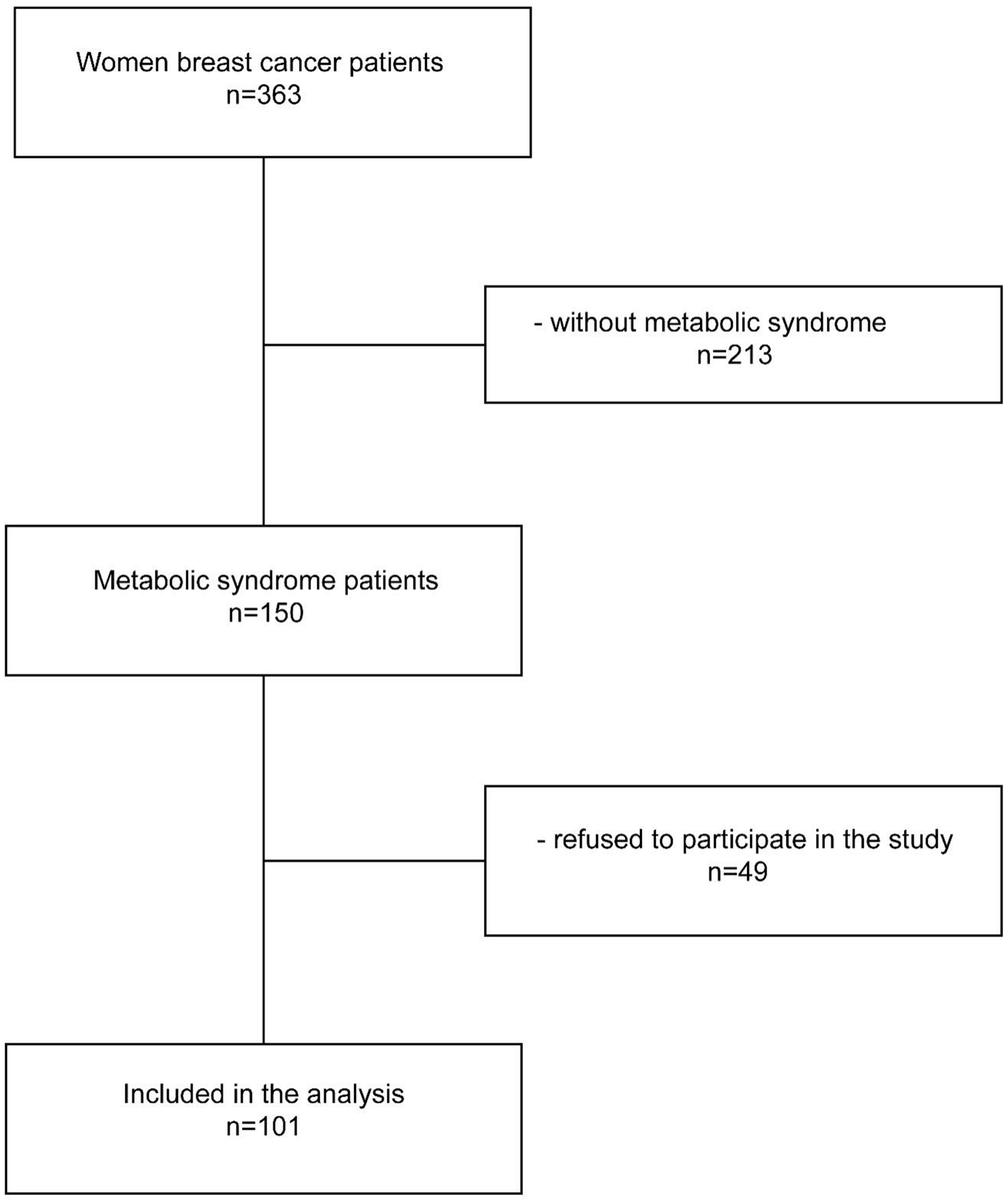
Flowchart of study.

Relationship of breast cancer molecular subtypes with metabolic syndrome and menopause.
Results
A total of 101 female BC cases with MetS were included in the analysis (Table 1). The mean age was 58.4 ± 8.5 years. Among women, 73 (72.3%) were menopausal and 28 (27.7%) were premenopausal. The whole cohort comprised 12 patients with Luminal A, 48 patients with luminal B, 27 patients were HER2+, and 14 patients were TN with molecular subtypes.
Patients’ characteristics.
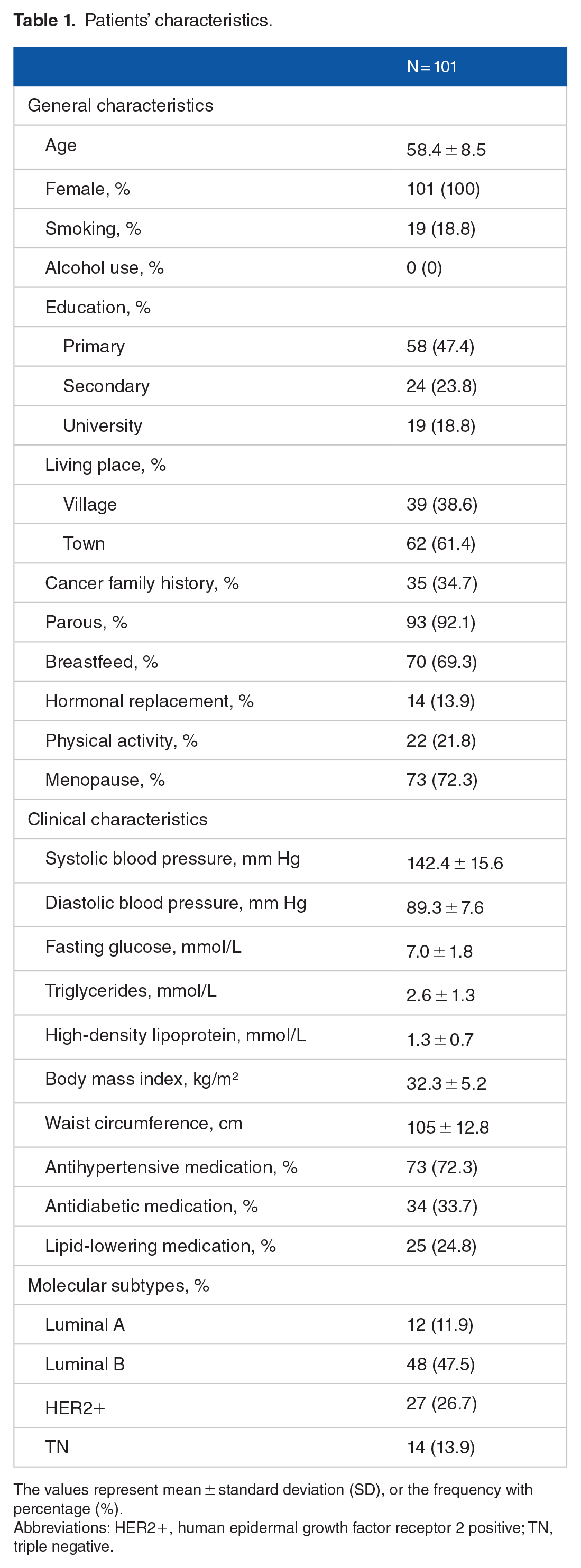
The values represent mean ± standard deviation (SD), or the frequency with percentage (%).
Abbreviations: HER2+, human epidermal growth factor receptor 2 positive; TN, triple negative.
Comparison of MetS individual parameters according to molecular subtypes and menopause
Comparison of MetS individual risk factors according to BC molecular subtypes no statistical difference was found for systolic (P = .33) and diastolic blood pressure (P = .17), fasting glucose (P = .77), triglycerides (P = .62), HDL (P = .33), BMI (P = .87), and WC (P = .81) (Table 2). Similarly, when accounting for menopause status categories comparison of individual parameters of METS were nonsignificantly different, systolic (P = .69) and diastolic blood pressure (P = .16), fasting glucose (P = .38), triglycerides (P = .74), HDL (P = .87), body mass index (P = .10), and WC (P = .29) (Table 3).
Comparison of metabolic syndrome parameters according to breast cancer molecular subtypes.
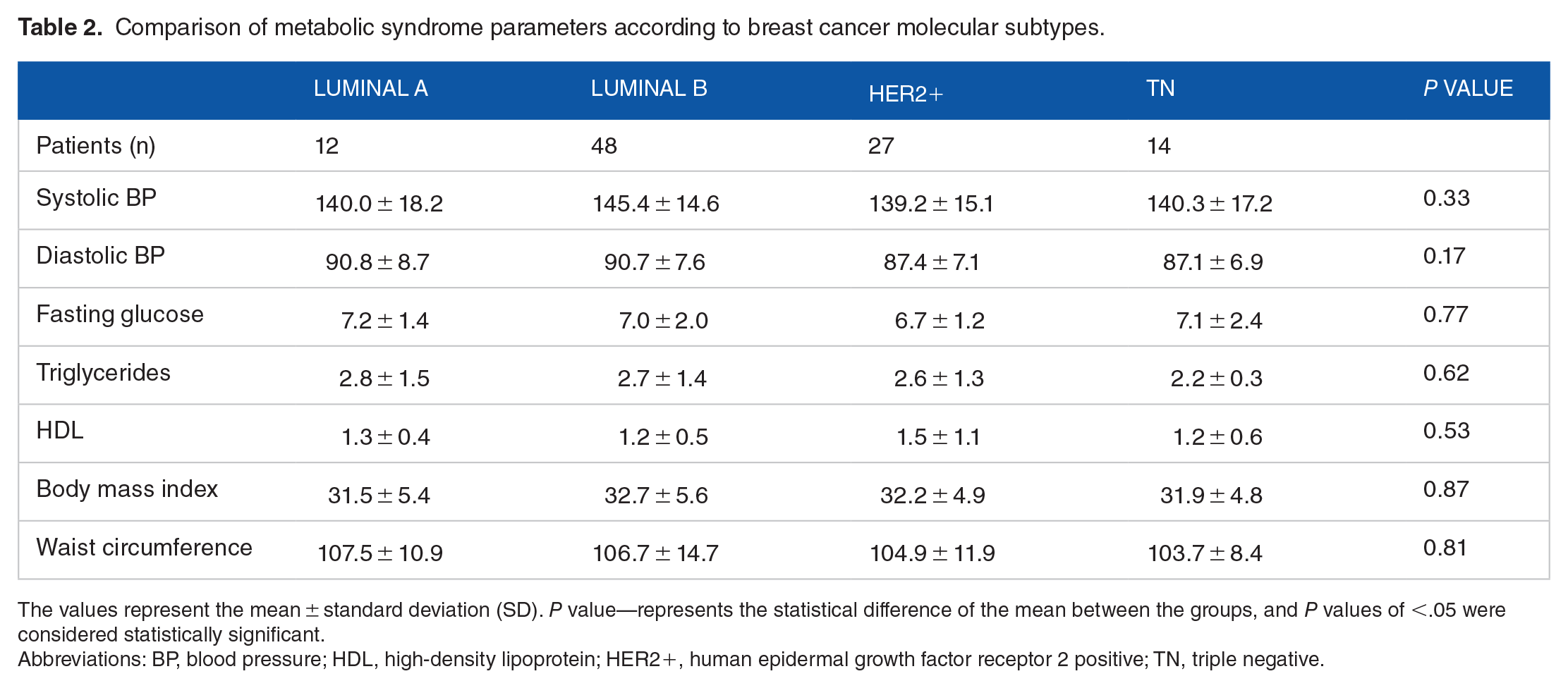
The values represent the mean ± standard deviation (SD). P value—represents the statistical difference of the mean between the groups, and P values of <.05 were considered statistically significant.
Abbreviations: BP, blood pressure; HDL, high-density lipoprotein; HER2+, human epidermal growth factor receptor 2 positive; TN, triple negative.
Comparison of metabolic syndrome parameters according to menopause status.
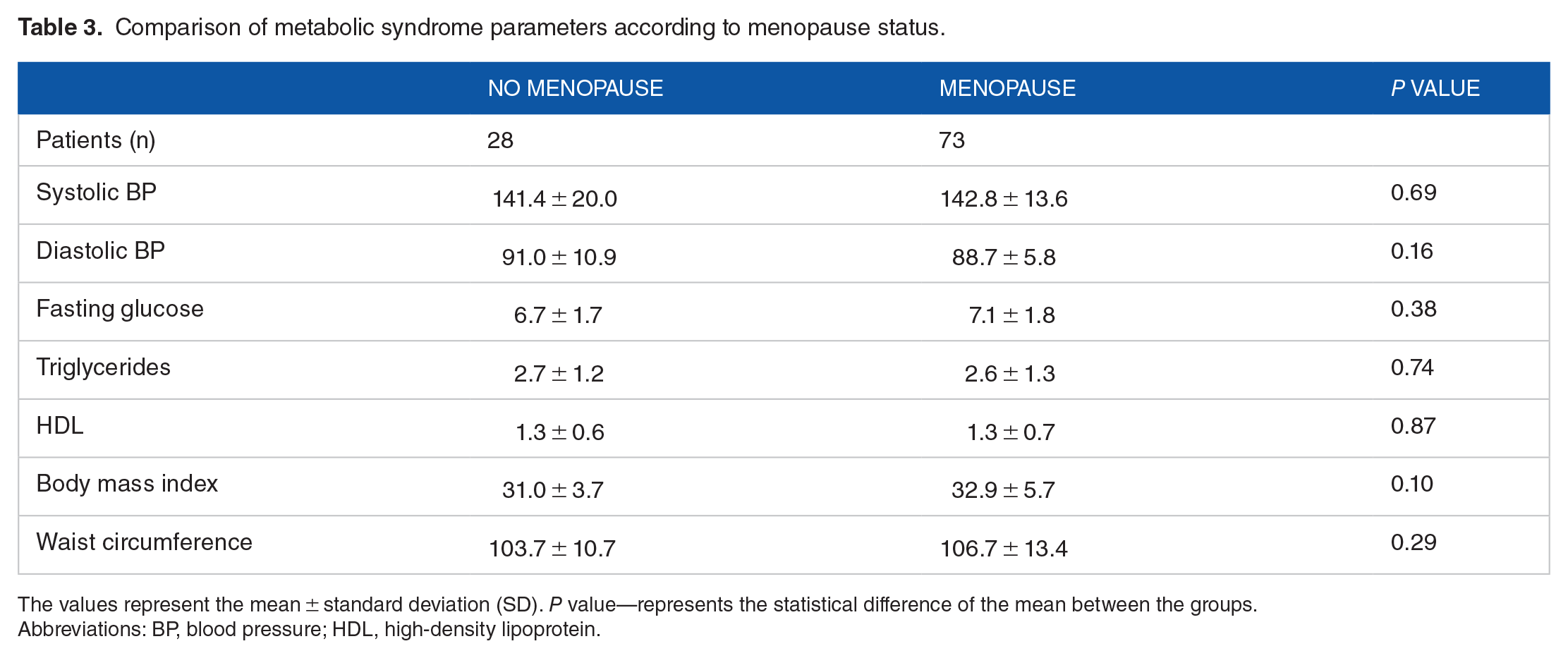
The values represent the mean ± standard deviation (SD). P value—represents the statistical difference of the mean between the groups.
Abbreviations: BP, blood pressure; HDL, high-density lipoprotein.
Association of the MetS individual parameters according to molecular subtypes and menopause
A positive trend was found between HDL and HER2+ molecular subtype (odds ratio [OR] and 95% confidence interval [CI]: 1.42 [95% CI: 0.79-2.52]) (Table 4), whereas for other parameters no association was found with any molecular subtype of BC. When we assessed the relationship of molecular subtypes and categories of menopause, an association was found between HER2+ categories and menopause (OR: 4.40 [95% CI: 1.00–19.54.]) (Table 5). No association was found for other molecular subtype categories with menopause but observed increased trends for categories of luminal B (OR: 2.69 [95% CI: 0.73–9.86]) and TN (OR: 2.50 [95% CI: 0.49–12.63]), respectively (Table 5).
Association between metabolic syndrome parameters and molecular subtypes.

The OR with 95% CI represents estimate size between molecular subtypes and menopause in logistic regression analysis.
Abbreviations: BP, blood pressure; CI, confidence interval; HDL, high-density lipoprotein; HER2+, human epidermal growth factor receptor 2 positive; OR, odds ratios; TN, triple negative.
Association between breast cancer molecular subtypes and menopause in patients with metabolic syndrome.

The OR with 95% CI represents estimate size between molecular subtypes and menopause in logistic regression analysis.
Abbreviations: CI, confidence interval; HER2+, human epidermal growth factor receptor 2 positive; OR, odds ratios; TN, triple negative.
Discussion
In this cohort of patients with BC and MetS, we observed a trend between HDLs and HER2+ molecular subtype expression. Interestingly, HER2+ molecular subtype was associated with menopause, suggesting that menopause may induce further expression of HER2+ molecular subtypes in subjects with MetS.
Studies assessing the role of MetS in the development of BC provided important evidence showing an increased risk of BC in women before or in menopause, by establishing MetS as an important risk factor that plays important role in cancer development and BC in particular.27-30 However, BC molecular diversity plays a role in treatment management and prognosis, 3 and individual risk factors of MetS may differently influence in over-expression of particular molecular subtype with favorable or poorer prognosis. 21 A study in Italy among 500 BC women patients reported that individual parameters such as WC, waist-to-hip ratio, and HOMA index were associated with HER2+ molecular subtype expression. 9 Another report from sisters’ nationwide study, with more than 50,000 participants, showed that central obesity, defined as elevated WC and waist-hip ratio, was associated with increased risk for BC. Furthermore, this study reported an increased risk for postmenopausal BC among metabolic unhealthy women phenotype at enrollment, defined as the normal weight with one or more metabolic abnormality, including dyslipidemia, type-2 diabetes, elevated blood pressure, or central obesity, while obese or overweight women regardless accompanying metabolic abnormalities had increased risk for postmenopausal BC. In line with findings in this study in our patients, HER2+ was associated with postmenopause, which suggests menopause to be an important contributor to the BC development in general, a condition with hormone level abnormalities, such as estrogen and testosterone occurring prior, during and postmenopause contribute to BC occurrence 28 or poor prognosis molecular subtypes such as HER2+, in particular. Although our patients met MetS criteria, we did not find any significant difference in individual parameters between categories of premenopause or postmenopause nor between categories of the BC molecular subtypes. In this context, a certain amount of our patients were treated with antihypertensive (72.3%), antidiabetic (33.7%), and lipid-lowering (24.8%) medication possibly would mask or attenuate these metabolic differences of individual parameters. However, we observed an increased trend between HDL and molecular subtype HER2+, which may suggest that subclinical dyslipidemia might be the driver of the HER2+ molecular expression in postmenopausal BC. Moreover, most our patients were obese with central obesity which previously was described as the main driver of the association of MetS and the risk of BC. Central adiposity crucially correlates with insulin resistance as a key component of MetS, also.31,32 Evidence shows that increased abdominal fat may increase the risk for BC through elevated levels of estrogen, testosterone, and insulin-like growth factor. 33 Besides central obesity may play a primary role, 28 yet MetS as a whole have been suggested to increase the risk of BC rather than a specific parameter of MetS. 34 Also, adipose tissue is the site of production of the leptin fat cell hormone with angiogenic properties. 35 Adipocytes in contact with BC cells increase the production of proinflammatory cytokines (IL-6) and the plasminogen activator inhibitor (PAI-1). Increased lipolytic activity serves as energy source for cancer cells, thereby adipose tissue and adipocytes support tumor-genesis and metastasis. 36 , Human epidermal growth factor receptor 2 positive is closely connected with fatty acid synthase (FASN), phosphatidylinositol 3-kinase (PI3 K), AKT, and mechanistic target of rapamycin (mTOR), which play role in lipid metabolism. Insulin-like growth factor 1 (IGF-1) and leptin can modulate HER2+ signaling pathway. 37
On the other hand, due to the increasing incidence of the BC in southeastern Europe, 16 approaching this problem requires cheaper alternatives, considering the lack of funds allocated for preventive and curative means by governments of respective countries, especially Kosovo. Based on presented results, we hypothesize that a good strategy for the reducing the BC burden might be beneficial to be involved and join efforts of family physicians, cardiologists, and other specialties to tackle dyslipidemia and other MetS risk factors with early implementation of appropriate treatment as a preventive intervention strategy, which might result in a lower incidence of BC in general and poor prognosis molecular subtypes in particular. An interesting approach would be also nonpharmacological or promotion of nightly fasting and a better diet, as suggested by a study using US National Health and Nutrition Examination Survey data, which resulted in better glycemic control and sleep and potentially reduced BC recurrence. 38 This might be a novel dietary intervention strategy with significant implications for public health.
Strength of this study includes the detailed characterization of the molecular subtypes with the most advanced histopathological procedures and standardized data collection. Our study prospectively included newly diagnosed BC patients with comprehensive information on potential risk factors for BC. However, the number of patients included might be a limitation of the study. Also, the cross-sectional analysis of the individual parameter limits to draw causal inferences on the role of studied parameters.
Conclusion
In BC patients with MetS was observed an increased trend between HDL and HER2+, suggesting that underlying dyslipidemia may favor the development of molecular subtypes with poor prognosis. Moreover, HER2+ was associated with menopause, which may play a mediating role in further expression of HER2+. Further studies with a larger sample of patients are warranted to elaborate on the role of MetS individual risk factors and/or menopause.
Footnotes
Acknowledgements
The authors acknowledge the patients’ contribution and willingness to participate in the study. They appreciate the contribution and dedication of study nurses from the Institute of Oncology of the University Clinical Center of Kosovo, also.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Study concept and design were performed by D.A.I. and S.M.K. Acquisition, analysis, or interpretation of data was performed by D.A.I., S.M.K., and B.M. Drafting of the was performed by D.A.I. and B.M. Critical revision of the for important intellectual content was performed by D.A.I., S.M.K., D.H.T.K., R.K., and B.M. Statistical analysis was performed by D.A. and B.M. Administrative, technical, or material support was performed by D.A.I. All authors read and approved the final.