
Abstract
Purpose:
As many as 50% of patients with cancer develop acute skin reactions to some degree with radiotherapy. Proactive skin care is often recommended to minimise these skin reactions and maintain the integrity of the epidermal barrier; nevertheless, no consensual guidelines are systematically used. This multicentre, observational, prospective study evaluated the tolerability and benefit of supportive and barrier protective skin care products in preventing radiotherapy-induced skin reactions in 253 women initiating radiotherapy (exclusive or adjuvant) for breast cancer.
Methods:
Patients received a kit of 5 commercially available skin care products before the first radiotherapy treatment. The following variables were assessed: cutaneous adverse events, investigator-assessed skin reactions (oedema, erythema, dryness, desquamation) before and after radiotherapy course, investigator, and patient opinion on products benefit. Results were analysed by frequency of product use (heavy versus low).
Results:
Average age was 60 years (range: 34-85). Over 92% of patients reported good to excellent tolerance on irradiated skin for each product. During the 6-week radiotherapy period, we observed that heavy product users had less skin reactions than the low users, particularly within 10 days of radiotherapy initiation (8% versus 18%; p = .031). Positive physician’s opinion on product use was more frequent for high (66.6%) versus low (32%) users. Patient-assessed patient benefit index was generally >1, indicating relevant treatment benefit, with a tendency for better benefit in high versus low users.
Conclusions:
These results support recommendations to use skin care products to minimise the impact of secondary cutaneous reactions with radiotherapy cancer treatment.
Introduction
Radiotherapy and combined radio-chemotherapy protocols have improved the prognosis and long-term survival from many malignancies. Thus, patients and treating physicians are increasingly required to manage acute cutaneous reactions associated with radiotherapy.1,2
Radiotherapy causes a variety of acute cutaneous reactions, commonly defined as acute radiodermatitis, that occur in the first 6 months from the beginning of treatment and can range from mild erythema and dry desquamation to severe confluent moist desquamation. 3 A study conducted by Barkham in the United Kingdom revealed that 52% of radiation therapy centres reported seeing dry desquamation associated with radiotherapy. 4 Acute radiodermatitis has also been reported to occur in 90% of treated patients with breast cancer and head and neck cancer. 5 In fact, any patient with head and neck cancer or breast cancer receiving external beam radiotherapy could be at some risk of developing these reactions.
Acute damage occurs right from the initial radiation dose when the first lot of basal cells are destroyed, although the acute side effects become apparent in average 2 to 3 weeks after the beginning of therapy. The remaining cells cornify and therefore shed faster than healthy skin. This process disrupts the balance between normal cell production at the basal layer and cell destruction at the skin surface. This process continues with continuing radiation. 6 With cumulative radiation doses reaching 20 Gy, skin barrier dysfunction manifests as dryness, flaking of the skin, or desquamation as folliculitis (skin rash), xerosis, pruritus, and hyperpigmentation. In addition, the skin becomes more sensitive to allergens and ultraviolet radiation and prone to infection. The primary role of supportive skin care is to maintain integrity of the epidermal barrier.
Although radiodermatitis is not life-threatening, it may become exceedingly uncomfortable if poorly managed. Some small, controlled studies have illustrated the benefit of using cosmetics as part of supportive therapy during treatment for breast cancer.7,8 However, 2 comparative studies found no difference between a barrier film and a glycerine-based product. Thus, there is not enough sufficient evidence to support gold standard therapy for the prevention of skin-induced reactions.9,10 These recent studies highlight the previously reported, limited, and conflicting nature of the literature at this time. 11 Nevertheless, regular skin care assessment and close collaboration between radiation oncologists and dermatologists to manage skin reactions early and throughout treatment have been repeatedly suggested to improve patient comfort, enhance quality of life, and improve clinical outcome.11–19 Also, a mini review suggested that prophylactically protecting vulnerable areas such as the axilla and inframammary fold from friction in patients with breast cancer may decrease the severity of radiation-induced moist desquamation, enhancing their quality of life as well as minimising treatment breaks. 20
Furthermore, radiotherapy, when combined with targeted chemotherapy, may exacerbate individual signs and symptoms of both therapies, resulting in severe xerosis, inflammation, and, more importantly, skin thinning, and necrosis of the upper dermis and epidermis. 21
Nevertheless, research into understanding the role of supportive skin care to prevent and manage radiodermatitis is important. Although there is some literature concerning skin care products in alleviating the severity of skin reactions, to our knowledge, there is no real-life data concerning the effect of using a combination of hygiene products. 22
This study was performed to investigate the benefit of using non-pharmaceutical skin care products to more effectively prevent and manage skin toxicity and improve quality of life for patients with breast cancer treated by radiotherapy.
Materials and Methods
Study design and setting
This prospective, observational study was performed from June 4, 2013, until January 29, 2015, and enrolled women starting breast cancer radiotherapy from 4 centres: CHU de Poitiers and Centre Oscar Lambret, Lille (France); Puerta de Hierro Hospital, Madrid (Spain); and the McGill University Health Centre (Canada).
Patients and evaluations
Patients were eligible for inclusion if they initiated adjuvant, neo-adjuvant radiotherapy, or exclusive radiotherapy for the treatment of breast cancer following either a segmental mastectomy or a total mastectomy. The investigating physician identified patients who were likely to have dermatologic side effects to the treatment. Patients with Fitzpatrick skin types I to VI were considered. Patients were excluded if they had metastatic cancer, skin cancer or any pre-existing skin disorders that could interfere with the results of the study (atopic dermatitis, contact dermatitis, psoriasis, rosacea, severe photosensitivity, scleroderma, or xerosis), a known allergy to cosmetic ingredients or a past history of allergy to cosmetic product.
The study period was 6 weeks to reflect the standard radiotherapy duration. Patients were assessed by a radiation oncologist at the initiation and at the end (6 ± 2 weeks later) of the radiotherapy treatment course. The following variables were assessed: skin reactions (oedema, erythema, dryness, and desquamation), cutaneous functional signs (pruritus, pain of skin, sensitivity, tingling, and burning sensations), cutaneous comfort, and the tolerance of the supplied products. Furthermore, patient satisfaction and morale were reported via the use of the patient benefit index (PBI). 23 Study staff recorded how often the patients applied each product: never, often, or every day. If a patient mentioned an adverse event during the treatment, an evaluation was performed. Non-cutaneous adverse events were reported in this study only if the investigator felt these significantly affected the study data.
Products
Once enrolled, each patient was given a kit containing 5 commercially available, non-pharmaceutical skin care products and an information brochure explaining the indications and properties of each product: when and how much product to apply (once or twice a day or when needed). The following products were included in the kit: a thermal water spray (La Roche-Posay Thermal Water), an emollient (Lipikar Balm AP), a cleanser (Lipikar Cleansing Oil), a wound healing cream (Cicaplast Balm B5), and a sunscreen (Anthelios SPF50+ Smooth Lotion; La Roche-Posay Dermatological Laboratory, Levallois-Perret, France). These products were specifically formulated with gentle ingredients that respect skin physiology and tested for use on sensitive skin.
Statistics
Analyses were performed with SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA).
The qualitative variables were described as number and percent of the different response modalities and the quantitative variables as number, mean, standard deviation, median, minimum, maximum, and number of missing data. Significance threshold was 5%, except the normality tested at the threshold of 1% (Shapiro-Wilk test). Product usage score was the sum of the frequency each product used in the kit: Never used = 0, Used from time to time = 0.5, Used often = 1, and Used every day = 2. Three groups were then defined: low users (score <5), heavy users (score ≥5), and not evaluable (score not computable because of missing data). The delay between the initiation of the radiotherapy and the appearance of skin reactions was compared between low and heavy users by a Student t test or a non-parametric Mann-Whitney test if the assumption of normality is questionable. An analysis of variance (SAS Proc Mixed) was also performed with relevant variables showing homogeneity problems between low and heavy users at baseline as covariables.
The delay was also analysed in 2 classes (delay ≤ 10 days and delay ≤ 14 days), and the comparison between low and heavy users was performed by a χ2 test and by a multivariate analysis for binary data (SAS Proc Glimmix) to take into account relevant variables showing homogeneity problems between low and heavy users at baseline.
Ethics and legal statement
Patients received an information leaflet explaining the aim of the study, its duration, the method, the constraints, and the foreseeable risks associated with using these products.
All written medical data remained anonymous and each patient was identified by a unique alphanumeric code. This code consisted of the country code (2 letters and a 3-digit number (ie, from 001 to 999). The investigating physicians and all the people partaking directly or indirectly in the study (coordination, control, analysis, etc) were bound to keep any information related to this study strictly confidential.
The electronic file compiling the data recorded in the study was submitted to the French Commission in charge of Personal Data Protection (CNIL) for evaluation and approval in September 2012. The study protocol and corresponding appendices were also transmitted to a French Research Ethics Committee (CPP) for information purpose in December 2012.
Each investigating centre was responsible for submitting the protocol to its hospital ethics committee and obtaining the corresponding approval, whenever applicable. A copy of each written approval was sent to the monitoring centre of this study.
Results
Patient characteristics
Four investigating centres enrolled 253 female patients in this study. In total, 122 patients were enrolled in Poitiers and Lille (France) (48%), 69 in Montreal (Canada) (27%), and 62 in Madrid (Spain) (25%). The mean age was 60 ± 11 years and ranged from 34 to 85 years. Most patients (72%) had fair skin (skin types I-III) and 28% had dark skin (skin types IV-VI). At inclusion, 92% of patients were initiating adjuvant or neo-adjuvant radiotherapy and 8% only radiotherapy for breast cancer (95% after a segmental mastectomy and 5% after a total mastectomy).
Based on the Union for International Cancer Control (UICC) classification of breast cancer (from tumour, node, metastasis [TNM] classification), 67% of patients had stage I disease (T1N0M0) (Table 1). The volumes of irradiated mammary gland were less than 500 cm3 for 17% of patients, between 500 and 1000 cm3 for 56%, and more than 1000 cm3 for 21% of patients (5% had a total mastectomy). The average area treated by radiotherapy was equivalent to 4.3 ± 2.1 palms (range: 1-10). The auxiliary lymph nodes were not included in the irradiation field. The average treatment duration was 5.6 ± 1.3 weeks (range: 3-9), the average number of radiotherapy fractions was 26.8 ± 5.7 fractions (range: 15-35), the average fraction size was 2.2 ± 0.3 Gy (range: 1.7-3.2), and the average total dose was 56.9 ± 7.6 Gy (range: 42-66). Hormonal therapy was included in the treatment for 63% (n = 159) of women, but only 15% (n = 37) were taking hormonal therapy at the start of radiotherapy.
UICC classification of breast cancer (based on TNM classification) (N = 243).

Abbreviation: UICC, Union for International Cancer Control.
Breast Cancer TNM Classification, 7th edition, 2010, and UICC stage.
The TNM system identifies the pre-therapeutic clinical stage noted ‘cTNM’ and the postsurgical anatomopathological stage noted ‘pTNM’.
Product use
Figure 1 shows the frequencies at which different products were used during the study. The 3 products most frequently used were Lipikar Cleansing Oil, Lipikar Balm AP, and Cicaplast Balm B5. The application of the products had no negative effect on the overall radiation therapy. Product tolerance on the irradiated zone was rated good to excellent by more than 92% of patients for each product (Figure 2).

Frequencies of use of the different products of the kit.

Evaluation of product tolerance on the irradiated zone.
Overall, 57% of patients were classified as heavy users, 36% as low users, and 7% were non-evaluable. Table 2 presents product use by country.
Low and heavy users distribution per country.
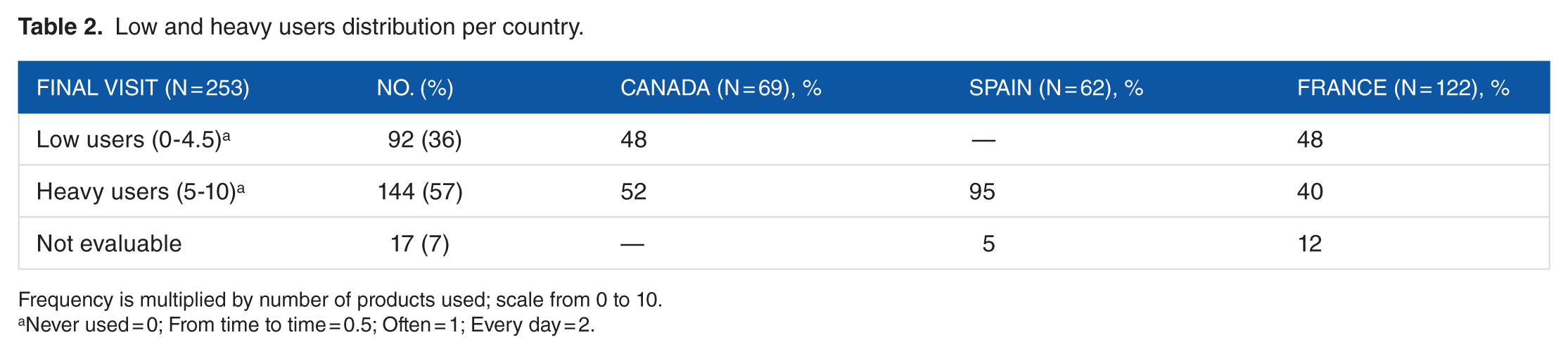
Frequency is multiplied by number of products used; scale from 0 to 10.
Never used = 0; From time to time = 0.5; Often = 1; Every day = 2.
Types, severity, and time frame of skin reactions
During the study, 215 patients (85%) developed at least one skin reaction, most frequently radiation dermatitis (86% of those patients), erythema (11%), desquamation (1%), and some rash, pruritus, or eczema (2%). Severity of the reaction was grade 1 for 93% of patients and grade 2 for 7% of patients. Radiation dermatitis worsened in 48% of cases and erythema in 29% of cases. The onset of skin reactions from the beginning of the radiotherapy was on average 18.9 ± 8.1 days (range: 5-45). For events that appeared within 10 days of the beginning of the radiotherapy, investigators reported that the percentage of patients presenting first skin reaction was significantly lower for heavy users versus low users. No significant difference was noticed for later skin reactions; nevertheless, low users presented more reactions than heavy users (Figure 3).
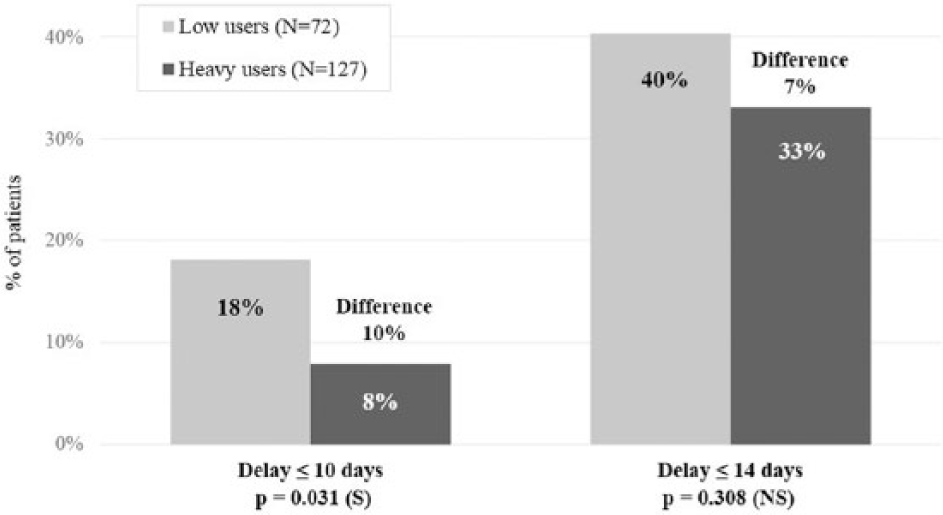
Time to onset of skin reactions: onset from the beginning of the radiotherapy.
Physician and patient opinion
At the end of the study, the percentage of physicians with a positive opinion (very good, quite good, or good) of product benefit was significantly higher for heavy users (64%) than for the low users (32%) (p < .0001; Figure 4). Furthermore, relevant benefit of the kit of products (PBI >1) was reported by significantly more patients in the heavy user group (93%; PBI: 2.9 ± 1.1) versus the low user group (86%; PBI: 2.7 ± 1.2; p = .095) (Figure 5).

Overall opinion of investigating physician, at the end of this study, regarding skin benefit of dermocosmetic products kit on irradiated skin.

Patient benefit index (PBI).
Discussion
The purpose of this prospective observational study was to evaluate the benefit of using a non-pharmaceutical skin care kit containing a thermal water, cleanser, emollient, wound healing cream, and sunscreen in preventing radiation dermatitis. The patients included had mainly stage 1 breast cancer and received radiation therapy for at least 4 weeks, which is typical adjuvant for this type of malignancy. We found, as previously reported, that 85% of patients declared having at least one skin reaction. 3 The skin reactions appeared early, within 5 days from the start of the treatment at the earliest but in average within 19 days as usually noticed. By 10 days of radiotherapy, 12% of patients had exhibited some skin reactions (of whom 70% had radiation dermatitis). Interestingly, we noticed that heavy product users had significantly fewer early skin reactions (within 10 days of initiating radiotherapy) compared with the low users (8% versus 18%; p = .031). Although this was an open, observational study, performed in 4 radiotherapy centres, the results suggest that following an appropriate skin care routine could delay the appearance of early appearing skin reactions. This further supports the current thinking that radiotherapy-related cutaneous adverse events are linked to skin barrier dysfunction. In addition, these results were associated with a better overall opinion of investigating physician and a higher relevant benefit for the patients. All the skin care products used during this study were well tolerated.
Interestingly, nearly all patients in Spain were heavy users as opposed to patients in France and Canada, who had a nearly even split between heavy and low users. Product advice was given differently in Spain, explaining the higher use. This may also confirm previous reports that found research-based evidence from the literature for prophylactic use of adequate skin care products are not consistently implemented. 24 In countries such as France and Canada, this may be because radiation dermatitis prevention with skin care products has only recently been implemented. This disparity could explain the lack of more significance in the results, especially for the onset of radiation dermatitis.
To our knowledge, this is the first study to investigate a full skin care protocol including thermal water, cleanser, emollient, a wound healing cream, and sunscreen. This differs from previous research which studied one product or washing only. Although the study was prospective, the design was limited by the absence of a control group. Also, it would have been valuable to have more detailed recordings of the dermatologist’s clinical evaluations. This study nevertheless provides additional support for the use of appropriate skin care protocol in the management of cutaneous reactions due to radiotherapy. Further controlled research is needed to confirm the efficacy of the individual products.
These preliminary results nonetheless support the benefits of using adapted skin care products during the radiotherapy.
Footnotes
Acknowledgements
The authors acknowledge Amy Whereat, Speak the Speech Consulting, for assistance in writing this manuscript, as well as Nedjwa Abbadi, MD; Morgane Bernard; and Christelle Guyomard from IRIS the monitoring centre of this study. They also thank M. Fortuné and G. Le Dantec for technical assistance and SYLIA-STAT for statistical analyses.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by La Roche-Posay Dermatological Laboratory, France.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.S. and D.M. are employees of La Roche-Posay Dermatological Laboratory, France.
Author Contributions
Conceived and designed the study: SS, DM, RJB. Performed the study: AB, CR, TH, DP, CDF, FLT, BCD, EL, RJB Analyzed the data: SS, DM. Wrote the paper: SS,DM, RJB.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.