
Abstract
Background:
Despite an increase in methamphetamine use and subsequent hospitalizations, the majority of Canadian hospitals currently lack harm reduction strategies for substance use. This can mean that people with lived experience of methamphetamine use are faced with a number of difficult decisions to make when admitted to hospital. Caring for people with lived experience of methamphetamine use can also be problematic with zero tolerance policies requiring abstinence to be maintained. This analysis set out to understand potential health care issues due to a lack of harm reduction strategies from the prospective of people with lived experience of methamphetamine use as well as health care/service professionals.
Methods:
Based on a larger study, this secondary analysis explored issues discussed by people with lived experience of methamphetamine use and health care/service professionals regarding the challenges of providing harm reduction approaches in the hospital setting. A total of 108 individuals with lived experience of methamphetamine use completed a qualitative component of a mixed-method interview. In addition, 31 health care/service professionals participated in virtual focus groups and one-to-one interviews. Responses were analyzed using an ethnographic thematic approach.
Results:
People with lived experience of methamphetamine use reported 3 choices upon admission: leave or avoid the hospital, stay but experience unsupported withdrawal, or stay but hide their substance usage from health care professionals. Health care/service professionals described 2 options: uphold zero tolerance that can lead to stigma and a lack of knowledge regarding addiction, or accept harm reduction but be unable to implement such strategies. This could lead to health being compromised due to policy and practice that requires abstinence. Neither group of participants described a good choice for them.
Conclusion:
Current policy and education related to substance use needs to be revised.
Introduction
The prevalence of methamphetamine use has developed into a significant health concern in North America, prompting what many have deemed a methamphetamine “crisis.”1 -3 A recent study conducted in Vancouver, Canada found that the prevalence of reported crystal methamphetamine use among people who reported intravenous substance use within the prior 6 months rose from 19% in 2006 to 36% in 2017. 4 Daily use also rose from 1% to 12% among 2 prospective cohorts of people who inject substances between 2006 and 2017. 4 Similar trends have been observed in the United States,5,6 particularly among people aged 26 or older, 7 as well as on a larger international scale. 8 Methamphetamine use was found to have increased during the COVID-19 pandemic 9 with one study reporting an increase from 5.9% to 8.2% among patients diagnosed with or at risk of a substance use disorder in the U.S. 10 A decrease was noted in Australia however. 11 In Ontario, Canada, methamphetamine has been found to be a direct contributor and detected in 26.7% of opioid-related deaths during the pandemic. 12 The COVID-19 pandemic has also had profound effects on the methamphetamine supply market.11,13 Due to increasing costs of methamphetamine, people who use methamphetamine have described switching to injection methods of administration and contamination of product with fentanyl which has led to more poisonings in this population. 13 Many countries around the world had to adopt a telehealth approach or home delivery service for harm reduction programs during the COVID-19 pandemic. 14 Increased prevalence of stimulant use such as methamphetamine in the community has been found to be associated with an increase in inpatient hospitalizations 15 and utilization of community harm reduction services. 16
People who use methamphetamine may seek treatment for any number of reasons, including substance use disorder, other mental health issues, or a physical health issue related to substance use. However, harm reduction strategies which seek to reduce the physical and social harms associated with substance use are currently lacking in hospitals. Examples of harm reduction strategies for methamphetamine and stimulant use include sterile needle exchange and smoking equipment, 17 safe consumption sites, 18 overdose education, naloxone kits for polysubstance use, greater access to social services, 6 use of clean paper for snorting, and drug-checking tests to detect what is present in the substance. 19 Harm reduction services have been found to be effective in increasing life expectancy, 20 and decreasing frequency of methamphetamine use, 21 HIV infection rates,22,23 intravenous use in public and needle sharing among frequent service users. 24
The lack of harm reduction practices in hospitals has led to a multitude of adverse impacts for people seeking care who use methamphetamine. The strict zero tolerance policy for substance use in many healthcare settings can cause severe withdrawal symptoms for people who use substances and who have been admitted to hospital.25 -27 The emphasis on abstinence in hospital may also prompt people who use substances to use in secret in their patient rooms or public bathrooms.28,29 Indeed substance use has been found to continue within the hospital setting despite the presence and enforcing of abstinence.28 -31 The absence of safe needle exchange and disposal resources may force people who inject substances to reuse equipment or dispose of needles in unsafe locations.32 -34 When harm reduction strategies are present, people who use substances tend to report increased feelings of safety.35,36 Staff at a specialty HIV hospital reported improved confidence after receiving harm reduction training when initiating conversations with people who use substances. 37 Previous research has revealed that among individuals who inject substances and require prolonged intravenous antimicrobial therapy, there is a greater risk of bloodstream infections within inpatient hospital care compared to community-based outpatient care, possibly due to the lack of sterile equipment available. 30 Abscesses, hepatitis C, and vascular damage are also common among people who inject substances in unsafe environments.38 -42
Many people who use substances leave the hospital earlier than recommended,31,43 -45 or may avoid seeking care altogether.46 -48 Reasons may include discrimination from health care workers,43,44 and inadequate pain control.44,48 Ratings of “very or extremely painful” withdrawal symptoms have been reported by 20% of people who use methamphetamine in a recent study. 49 This can lead to people not receiving treatment for other conditions, exacerbating heightened vulnerabilities and potentially causing increased care requirements in the future.50,51 Causes of overdose and further harm have been found to be the result of unsafe consumption, tainted substance supply, or lack of supervision.52 -55
The implementation of harm reduction strategies in hospital settings would help increase the likelihood that people who use methamphetamine and other substances receive care that prioritizes safety and shared decision-making. The provision of such strategies could ultimately curb some of the adverse effects and poor health outcomes mentioned previously, and prevent aversion to care. The concept of providing harm reduction strategies in the hospital setting is largely uncommon but early adoption of this approach has begun in Canada. Edmonton has seen a supervised consumption service 56 and a bedside needle/syringe program 57 implemented into hospital. Hospitals in Vancouver 35 and Victoria 54 have implemented overdose prevention services. Two hospital emergency departments in Toronto also distribute free naloxone kits to patients. 58
This study sought to learn what people who use methamphetamine need in order to receive care in the hospitals more effectively. The study also collected data on the experiences and observations of health care/service professionals. This article represents a secondary analysis of first year data from an ongoing 4-year study into methamphetamine use and harm reduction strategies. The primary analysis of the study revealed that harm reduction was needed within the hospital setting and that substance use continues despite the current requirement of maintaining abstinence. The aim of this analysis is to further explore and highlight health care issues resulting from strategies not being offered in hospitals.
Method
Design
This study used a mixed-method approach to understand the experiences of people who use methamphetamine and health care/service professionals regarding how best to approach future harm reduction directions in hospital settings. Western University’s Research Ethics Board provided ethical approval (REB ID #115779). Lawson Health Research Institute (research arm of hospitals in London, Ontario) provided approval for the study to commence. Funding for this study was obtained from Health Canada’s Substance Use and Addiction Program stream that focused on methamphetamine use.
A purposive sampling frame was created to ensure a wide variety of individuals would have the opportunity to voice their experiences and opinions. Priority was given to individuals who identified as a minority (eg, Indigenous, Visible Minority, LGBTQIA2S+) to allow for greater representation within the sample. This frame aimed to include a similar number of people who identified as male and female as well as including those who identify as non-binary. The sampling frame also aimed to recruit health care/service professionals with frontline experience of working with patients with lived experience of methamphetamine use as well as individuals who serve this population through public health, social, or housing services.
Recruitment
Recruitment posters were placed in hospitals, mental health programs, safe consumption sites and homeless agencies with the contact details of the co-principal investigator and the research coordinator. The research protocol was also provided to hospital and agency staff to inform people with lived experience of methamphetamine use and discuss the study in greater detail. Potential participants were able to contact the research team and arrange their own interview at a time and location convenient for them. Research team members completed outreach visits at a number of different shelters for homelessness and at a safe consumption site. This entailed multiple research team members being given office spaces at various locations and meeting with clients directly to discuss the study with them and conduct subsequent interviews. Inpatients who identified past or current use of methamphetamine were informed of the study by their hospital care team.
As this study utilized an ethnographic method of analysis, the minimum number of people with lived experience of methamphetamine to be enrolled was 30 to 50 in order to achieve saturation. 59 As the qualitative interview was conducted at the same time as a quantitative component, the minimum number of people with lived experience of methamphetamine use to be enrolled was 104 based on sampling size calculations. To be included in the study, people with lived experience of methamphetamine must (a) be aged 16 to 85; (b) have received hospital services; and (c) have the ability to speak English to the degree necessary for participation. Participants who used polysubstances were also eligible for inclusion in the study as long as they self-identified current or previous use of methamphetamine. Individuals were excluded from the study if they had no current or previous experience using methamphetamine. Although there are no harm reduction strategies for any type of substance within the hospitals identified for this study, methamphetamine was the focus of this based on the requirement of the funding grant.
Health care/service professionals were recruited via email and word-of-mouth from the study’s Advisory Group, which included health care professionals as members. The recruitment poster and research protocol were provided and allowed for interested health care/service professionals to make contact and discuss the study further. The study aimed to recruit up to 60 health care/service professionals to ensure saturation 59 of unique experiences and perspectives within the health care field.
Procedure
Informed consent was obtained before all interviews and any concerns were addressed prior to commencing an interview or focus group. People with lived experience of methamphetamine use completed a mixed-method one-to-one interview while health care/service professionals completed a qualitative focus group or one-to-one interview. All qualitative interview guides (developed by the research team) were semi-structured and open ended to facilitate open dialog of the topic of harm reduction and methamphetamine in hospital settings (see Appendices A and B). Interviews were completed either in-person or via phone. All in-person interviews with people with lived experience of methamphetamine use maintained physical distancing and use of personal protective equipment was adhered to by the research staff as well as participants. Health care/service professionals enrolled in the study participated in virtual one-on-one discussions or virtual focus groups using teleconferencing software. Health care/service professional interviews lasted between 30 and 60 minutes and qualitative interview components with people with lived experience of methamphetamine use lasted between 2 and 33 minutes depending on participant preference. Interviews were conducted by members of the research team trained in qualitative research methods. Following the interview, people with lived experience of methamphetamine were offered a $20 honorarium for their time. Health care/service professionals were offered a $5 coffee gift card as a gratitude for their participation. All qualitative interviews were recorded and transcribed verbatim.
Analysis
All transcripts were analyzed using thematic ethnographic analysis. This method of analysis utilizes 4 phases which include: data collection and documentation, categorization of initial themes, identification of patterns or values as they relate to broader social and cultural environments and finally identification of major themes. 60 Themes and subthemes were identified based on people with lived experience of methamphetamine and health care/service professionals’ responses during interviews or focus groups. Interconnections between themes were examined that illuminated issues associated with absence of harm reduction strategies in hospital. Responses from people with lived experience of methamphetamine use and health care/service professionals were analyzed separately, and themes were then compared for crossover and corroboration. Grouping of themes and quotes were validated by 2 qualitative researchers and the co-principal investigator.
Findings
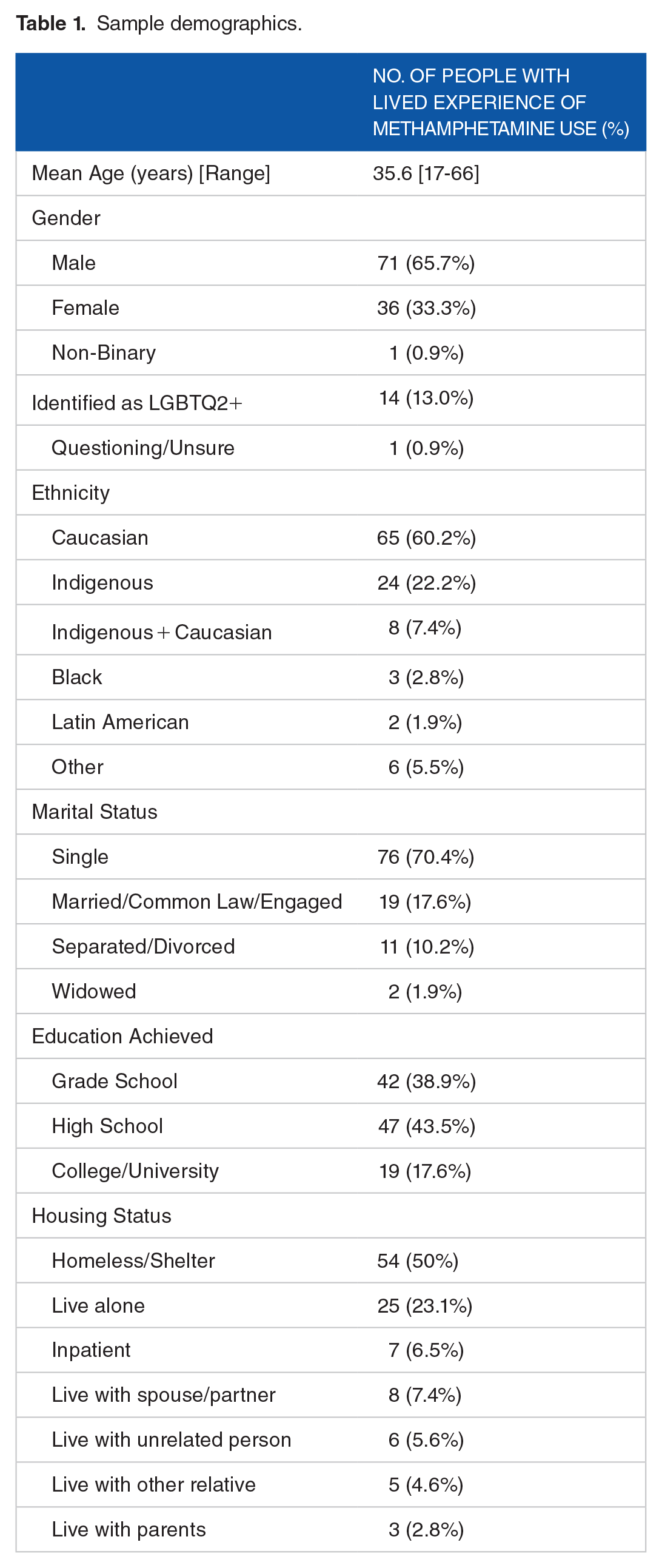
The study enrolled 121 individuals with lived experience of methamphetamine use with 108 completing the qualitative component. Thirteen participants either declined or did not complete the qualitative component of the interview. From the 108 interviews where the qualitative component was completed, 38 were conducted via telephone and 70 were in-person. See Table 1 for demographics.
Sample demographics.
The study also enrolled 31 health care/service professionals to participate in virtual focus groups as well as individual discussions. The sample was largely comprised of registered nurses (n = 26) with 3 specializing in public health nursing and 5 in mental health. A nurse practitioner, a harm reduction service manager, an epidemiologist, a social worker and a housing services manager also participated.
Thematic analyses
A large number of issues were identified by people with lived experience of methamphetamine use and health care/service professionals with a separate stream for each (see Figure 1). The overarching issues for both streams included zero tolerance and a lack of harm reduction practices as a result of current policy and insufficient knowledge about addiction. For both people with lived experience of methamphetamine use and staff, they experienced this as a “no-win” situation where both sides experienced difficulties and frustrations.

Resulting issues due to lack of harm reduction.
When patients who used methamphetamine were admitted to the hospital, they were faced with 3 difficult choices regarding their use. The first was to leave the hospital or avoid it altogether. People with lived experience of methamphetamine use reported leaving as a result of health needs not being met, perceiving stigmatization, and experiencing withdrawal symptoms. The second choice was to stay within the hospital but endure withdrawal. Staying and experiencing withdrawal led to a number of undesirable behaviors such as feeling aggressive as well as adverse health reactions. This theme was interconnected with leaving and avoiding the hospital as withdrawal meant that individuals’ needs were not being met in the hospital setting. Withdrawal was also connected to the third choice, stay in hospital but hide their methamphetamine usage by continuing to use secretly. This option allowed patients to receive care for their health concern but also sustain usage which places even more risk to themselves. Undesirable consequences such as changes in behavior and aggression as well as risks of infection, unsafe discarding of needles and adverse health reactions were all potential risks highlighted by people with lived experience of methamphetamine use and health care/service professionals.
Heath care/service professionals stated that current policies did not allow for harm reduction in hospital and that there was a lack of knowledge about methamphetamine use, and addiction in general, presently. It was acknowledged that for patients leaving the hospital, stigma and concealment of substance use within the hospital were current ongoing issues for this population. This leads to a “no-win situation” where health care professionals are given 2 methods of practice. Upholding zero tolerance policies in place was one option which comes at a risk of reinforcing stigma against patients who use methamphetamine. It could also mean that education around stigma, substance use and addiction may be missed. The second option is to accept and promote harm reduction as a form of care. However, this was not possible which led to a state of frustration with a desire for change as well as concerns of providing ineffectual care.
People With Lived Experience of Methamphetamine—Analyses
Main theme: Leave/avoid the hospital
People with lived experience of methamphetamine use stated that they left the hospital early in 2 scenarios: discharging themselves against medical advice (due to withdrawal symptoms or negative interactions with health care staff) or being discharged prior to completion of treatment course. Reasons for being told to leave the hospital included bringing methamphetamine into the hospital and leaving the hospital for an extended time in order to obtain substances.
People won’t stay in hospital because they get their dope subcutaneously and they don’t get high from it. Now, if you’re weighing your habit versus your health, most people in my position are going to pick their habit over their health, and healthcare knows this, and yet they don’t make any changes. (Participant 021)
Others described that they felt their medical needs were not being met and left the hospital, even if it was detrimental to their health. Specific needs discussed by people with lived experience of methamphetamine use including withdrawal management, pain management, and not receiving perceived stigma or discrimination.
Like, my experiences like, were sh**ty. Like I, you know it’s bad when they’re telling me like, you’re gonna lose your leg if you leave. And I’m like, f**k you and I sign the papers, knowing there’s like a 99% chance that I’m gonna lose my leg, and I’m still willing to walk out of this hospital because you’re not meeting my needs? (Participant 017)
Avoiding hospital care can be extremely detrimental to the health of an individual. Many reasons were given including stigma, unmet health needs, embarrassment and a lack of knowledge pertaining to addiction.
Like, they treat you unfair and everything. So I didn’t like going there, so I just stayed out here and deal with the problems at hand, right? . . .Until I actually had met (Doctor’s Name), I didn’t actually go to the hospitals for any of my treatments or any of my problems. Because like I said, I didn’t, I didn’t like the way they treated it right? (Participant 064)
Main theme: Withdrawing from substances while in hospital
Patients may try to stay within the hospital to complete treatment. This is not always a straightforward option however, and is fraught with the issue of withdrawal. This can lead to a number of responses including aggression, risks of adverse health reactions, and leaving the hospital without receiving the necessary care. This issue of withdrawal can also lead to the other 2 main themes, leaving or avoiding the hospital and continuing substance use while in hospital.
I’ve left countless times because of my withdrawals, and then I never got to complete my antibiotics or I never got, so I never got rid of my blood infection that I still have, you know? . . .Like last, the last time I was sick there, I had, I was supposed to be in there for three weeks, but I left after four days ’cause my withdrawals were too much . . .that’s why a lot of us leave the hospital, like you know, sign ourselves out early or just walk out because we’re sitting there and withdrawing and plus we’re in all that pain from why we’re there and they really just don’t give a s**t you know, ’cause it’s like from drug use. (Participant 071)
The risk of experiencing withdrawal can also be a deterrent to help-seeking from the hospital and can be linked to avoidance of health care.
So that’s why people would rather go to a detox facility for a week then to the hospital. They would rather suffer without their drugs for a week than go to the hospital, and get something that will take away the withdrawals because of the way they’re treated. (Participant 019)
There were also fears regarding the potential impact of experiencing withdrawal. Although methamphetamine alone is unlikely to result in death and is more likely to cause unpleasant reactions, polysubstance use involving other substances could have that consequence. This can also be a potential deterrent to not seek medical care due to the expectation of abstinence.
You can’t do that to a human’s body when we are highly addicted as what we are, doing it every day and you try to force us to quit cold turkey. Guaranteed within maybe a 3 week time period we’re dead. . . Because technically I see way too many people dropped out, not from massive heart attack and got buried because they were forced to quit, push them out to cold turkey. (Participant 090)
Main theme: Continuing to use but hide use while in hospital
Some people with lived experience of methamphetamine use discussed using in the hospital, often as a result of experiencing withdrawal and a perceived lack of medical attention. This use of substances was conducted in secrecy and involved concealment from staff.
And I’m there for a heart issue due to it [methamphetamine], but they don’t, then they don’t give me anything to make that the, the “Jones” [cravings]. I guess you could say that you received from them “go away”. . . So, how do they know I’m not going to be in the bathroom smoking more. . . Giving myself a heart attack, right? (Participant 046)
The concept of hiding usage was also influenced by the current zero tolerance approach and the consequences of breaching the rules. Hiding usage and maintaining secrecy was connected with the risk of being discharged from the hospital and leaving before treatment was completed. The concern of being told to leave the hospital meant that individuals would try to stay there while also trying to minimize withdrawal.
And wasn’t going to be honest about it, cause they do frown upon it. And then I don’t know, in a way I remember thinking I would get kicked out, so I’d hide in the bathroom and go do it. . . And then what if you overdosed on that too? ’Cause they don’t know. Right. And you’re right up against the door. Cause you don’t want anybody walking in and unfortunately in the hospital they have kind of rights to walk in and that I didn’t think it’d be wrong. (Participant 105)
Concealment also came in the form of refusing to disclose substance usage and feeling the need to lie to health care staff in order to avoid any potential repercussions.
I know, I know for myself, for the most part, it was the last couple of times I’ve gone there. I’ve had to lie about my use. They asked me if I’d been using it and I lie about it because I, ’cause I just automatically expect that they’re going to turn me away. (Participant 023)
Poorer health and risk of mortality (leave/avoid, withdraw, hide)
One of the outcomes for not providing harm reduction is using substances unsafely which could have negative consequences for the patient’s health. Poor health and mortality can be the result of all 3 choices faced by people who use methamphetamine.
But like I said, you’re a high risk of infections. Um, like, I didn’t, didn’t have clean gear and I was getting it in me one way or another in my years. So for me, it was putting it on my PICC line cause it gets right to the, an artery or whatever. And that was not a smart idea because the outcome could have been really scary and that, and then I wouldn’t have been telling them. And sometimes the only way doctors can fix things is by knowing what caused it. Right? (Participant 105)
The dangers of a sudden cessation from using high quantities of methamphetamine and/or polysubstance use due to abstinence rules could also have a negative effect on the individual’s health. 61 In extreme cases, severe health outcomes due to the shock of withdrawal from methamphetamine use is also a potential risk.
Readmission (leave/avoid, withdraw, hide)
Leaving the hospital against medical advice can result in health issues requiring further treatment or a worsening of symptoms therefore needing patients to readmit themselves. This can be the result of leaving/avoiding the hospital, attempting to withdraw, and hiding use of substances in the hospital setting. Not completing treatment due to substance use and/or not being able to access supports while in hospital may also require the patient to have to return. It was recommended by people with lived experience that health care/service professionals engage more frequently with them to avoid readmissions and to receive the treatment they need.
I feel like a little bit more hands-on with the individual and try to follow up with them and don’t let them just keep falling into the same cycle of whatever they’re doing and keep them back and forth between the hospital and outside not really getting anywhere. (Participant 067)
Lack of stability (leave/avoid, withdraw, hide)
Regardless of whether people with lived experience of methamphetamine use chose to leave/avoid the hospital, experience withdrawal or hide their use, they reported a lack of stability upon discharge. People with lived experience of methamphetamine use and health care/service professionals alike discussed how patients are discharged into the community without transition or resources made known. This can lead patients to fall into previous cycles of unsafe substance use and health compromising behaviors that caused health problems to begin with.
Like, so they send you to a detox center so that you can dry up for seven days and then they kick you out on the streets. And you have nowhere to go. And then, now you’re back in the same, same circle. (Participant 018)
Physical aggression (withdraw/hide)
One of the unfortunate responses to a lack of harm reduction strategies in hospital was the aggressive reactions of some patients. The effect of withdrawal can lead to individuals lashing out, which places others at risk.
Withdrawal, there’s been the possibility of people going violent, no self-awareness, you come down from the high and you’re going like, I gotta get high again. They’re forcing us to subdue to nothingness. It’s like, how can you do that to us? It’s like we’re going through this addiction. They make you go through the withdrawal. They say, you should just toughen up. (Participant 114)
Needle usage (hide)
A key issue of hiding substance usage in the hospital is the unsafe discarding, reusing, and sharing of needles. This can lead to a greater risk of infection, not only for themselves, but for others around them who could come into contact with discarded needles.
And so, but people needed, like they need to throughout the night, then they can just go there. So if they don’t have that, then they just use dirty needles and then they get like diseases and stuff. (Participant 101)
This was corroborated by some health care/service professionals who reported on the concept of zero tolerance for patients using substances while inpatient and that what can often follow is the concealment of use within the hospital.
. . .I can understand from a safety perspective, but at the same time it, it creates a situation where they’re on the fringes of the healthcare system simply because they have to choose between their addiction or their care. And, when something like that happens, they’re going to feel judged, they’re going to feel the need to hide their drug use from us, and if they’re doing that, one of two things is going to happen. Either they’re going to use drugs and we’re not going to know, and then we’re going to provide care that could lead to a whole bunch of interactions down the line that we don’t want to have, or they’re going to tell us and then we’re going to have that zero tolerance policy in place, then they’re not going to end up getting the care that they need. (Staff 028)
Health Care/Service Professionals—Analyses
Main theme: No win situation for health care/service professionals
A large number of the health care/service professionals were open to the idea of harm reduction and acknowledged that a great shift in focus would be required to implement such strategies. Some health care/service professionals expressed frustration and questioned why harm reduction cannot be implemented more easily. It was noted that being unable to offer harm reduction to patients can have negative implications in future. Maintaining the status quo of abstinence and not addressing the need for additional education or training could result in stigma continuing to exist and ideal health care being compromised.
But particularly if you add in on top of that inherent bias and then you add on top, like the person does have substance issues and they’re feeling like there’s gonna be sort of, prejudice against them. I think that it can escalate quickly and there’s not a lot of, there’s not a lot of education and discussion around how to manage those in a respectful way, that leaves both parties, both people safe and feeling respected both ways, because I think that often times it can escalate quickly because of the things I mentioned before (Staff 026).
Stigma/lack of knowledge
It was acknowledged by health care/service professionals that some staff do have biases regarding patients who use substances. This can be linked to the upholding of zero tolerance policies and reinforces these biases that substance use is a negative behavior, even representing poor decision-making or usage as a bad choice. This in turn creates a vacuum in the understanding of substance use and addiction. This lack of knowledge can then result in health care professionals becoming frustrated and impatient with patients who struggle with addiction and have different, potentially more intense, needs compared to the general patient population.
There basically seems to be very little tolerance for it from service providers. You know, there is a lot of like condescending comments that staff would make about certain patients when they know that they’ve been using and then they’re admitted. They’re like, “Oh, they always come back here”. ’Cause you know, we got them better here and then we discharge them and they start using again. And then they’re back here again, you know, there’s just a lot of frustration around patients using substances at all, they just sort of don’t really have tolerance for it or care to think about harm reduction strategies. (Staff 005)
Different views on current policies
With current policy, there is little to no opportunity to offer or provide any form of harm reduction. Methadone or suboxone can be prescribed for opioid substitution therapy but health care/service professionals noted that this was limited to specific physicians. Ultimately this can also lead to frustrations with health care/service professionals acknowledging they are providing ineffectual care for patients and are unable to provide harm reduction that could prove more effective.
. . . . And finding ways to try to prevent that patient population from feeling marginalized by our healthcare system like, for example, with that zero tolerance policy we were just talking about, like I just feel like that type of policy marginalizes them. (Staff 028)
Others felt that abstinence was a form of harm reduction and that zero tolerance policy was a preferred approach to addiction. However, this does not meet the definition of harm reduction. Education and training were therefore considered as an area for improvement to ensure that all staff fully understand the concept of harm reduction and can make an informed opinion.
Typically, we’re aware of it, not necessarily what products being used, but that they are going to be using drugs when they are outside of the hospital on like, on a break, hospital break or whatever and they come back. Normally we’re aware of that, so I feel like that could be harm reduction in a way that we’re not allowing them. (Staff 027)
Health care/service professionals also highlighted current issues of not providing harm reduction through the dangers of needles being unsafely discarded within the hospital by patients who used substances.
I think staff is, and it happens, we have needlestick injuries. . . from sticking needles under mattresses or stuffed in bed linens. (Staff 023)
Discussion
Patients who use methamphetamine coming to the hospital described having a choice of 3 options: 1. Leave/avoid the hospital, 2. don’t use but go into withdrawal, or 3. continue use but hide their use. Leaving or using in secret can also be the result of attempting withdrawal without supports and being unable to sustain abstinence in hospital. The initial 24 hours of methamphetamine withdrawal represents the peak of withdrawal severity and can include mental health issues such as anxiety and depression, fatigue and increased eating and sleeping.62,63 Psychotic symptoms have also been observed in the first week of withdrawal. 27 Using substances to alleviate withdrawal without the health care provider’s knowledge could lead to additional risks such as overdoses or interfering with treatment/medications. These 3 options are interconnected through the issue of withdrawal in addition to the overall lack of provision of harm reduction interventions to maintain abstinence. Withdrawal can lead to people using substances in secrecy within the hospital setting in order to reduce the effects of withdrawal, or simply leave the hospital due to needs not being met. Ultimately all 3 choices lead to the patient’s health being compromised. Without harm reduction practices, both patients and health care/service professionals face a no-win situation which can lead to ineffectual or compromised health care (as detailed in Figure 1). However, when harm reduction practices have been implemented in hospital, people who use substances have reported improved pain and withdrawal management. 64 In the absence of harm reduction practices, mental health issues can be exacerbated and characterized by aggressive behaviors which hospital staff may not be equipped to manage due to a lack of understanding. This lack of understanding can be associated with leaving the hospital prematurely due to poor pain management or withdrawal management.48,65This also contributes to people using substances concealing substance use. 29
Those experiencing pain may be at greater risk of using substances within the hospital 66 and so denial or delays to support can be counterintuitive to safety. This could also be the result of stigma. As discussed by people with lived experience of methamphetamine use and some health care/service professionals, there can be the preconception that a patient is demonstrating drug-seeking behavior for pain medications. This can lead to undertreatment of withdrawal and pain which can trigger mental health responses and patient-directed discharge as reported in previous qualitative 43 and mixed-method 48 studies. It can also result in the avoidance of seeking medical care, delaying health care and seeking care alternative options. 67 A key implication of the findings is for greater education and training on offer for health care professionals to advance understanding of addiction and to reduce stigma. Workshops for physicians provided by patients in recovery from lived experience of methamphetamine use have been found to be useful for changing practices and enhancing physicians’ understandings of their roles. 68 But future educational opportunities must also attempt to reach out beyond physicians to frontline staff who encounter and interact with patients more frequently.
Health care/service professionals and people with lived experience of methamphetamine use discussed the notion of stigma which can also be a contributory factor to leaving or avoiding the hospital and hiding their use of substances in hospital. With zero tolerance policies in place, stigmas can be reinforced that addiction is not an illness and that breaching these rules contradicts the philosophies of health care. Previous qualitative research has revealed stigma and fear of legal repercussions as a result of zero tolerance policies acts as a deterrent for using substances in hospital but also a deterrent for help-seeking. 47 A potential cause for perceived stigma may be health care professional burnout and frustration toward perceived failure to influence patients to maintain abstinence in hospital. 52 Particularly if health care professionals are trying to follow current hospital policy which may lead to either frustration with the policy itself or frustration toward the patient for not adhering. For some, abstinence represents a more ethically sound approach compared to harm reduction. This is also reflected in policy documents across Canada, where only a small number of documents discuss abstinence or reduction of use as a requirement for services. 69
Allowing for the provision of substance use in hospital may be met with critiques from health care professionals, particularly if they are asked to facilitate usage. Liability concerns may also be factored into their ethical beliefs. Although this study may be disheartening upon reading the lack of suitable choices, there is growing literature and interventions in the hospital setting. Canadian hospitals have begun to integrate harm reduction principles into their care and other countries have hospitals that provide harm reduction strategies. In the U.S., fentanyl test strips distribution 70 and harm reduction equipment kits 71 have been provided in Philadelphia and San Francisco respectively. Equipment provision in Scotland 72 and needle exchange programs in Jersey 73 in hospital have also been implemented in the UK. A needle and syringe program has also been offered in an Australian hospital in Darlinghurst. 74 Future research into policy and legislation would be beneficial to observe what changes can be made, even if made incrementally. Lack of knowledge may also play a role with interactions between patients and health care professionals resulting in negative interactions and adding to potential stigma. 75
This study suggests health care policy and decision-makers must consider how to care for people who use substances and how to keep them engaged with their care in hospital. Although the literature base is still growing, this study illustrates the difficult choices that people who use substances have to make upon admission to the hospital. The qualitative themes that arose from the study revealed that health is compromised and ineffectual care is provided as a result of these choices. Ultimately indicating that the current health care approach is not ideal for people who use substances. The issues identified from this study have significant implications for future care and staffing with regard to providing care for this section of the patient population. Providing education to reduce stigma and greater awareness of withdrawal symptoms would represent a positive step in building therapeutic relationships. Enhancing levels of trust may not only encourage patients to access health care service but also to report their substance use to health care professionals during admission overall improving care. This could reduce the need for using substances secretly and also allow for a patient-centered approach where a care plan is devised based on this feedback to ensure safety and reduce conflicts with treatment.
Limitations
The study was largely conducted in one city in Ontario, Canada. As such the findings may not be transferable to other settings (eg, rural and larger, urbanized cities). The 31 health care/service professionals recruited for this study were mostly registered nurses and although this represents sufficient saturation of frontline staff, no physicians or other therapists were available to be enrolled. This could have provided a greater insight into the other dimensions of health care for this population of patients and other specific experiences. Some of the interviews for people with lived experience of methamphetamine use were by telephone due to COVID-19 restrictions. It is uncertain if in-person interviews would have produced different results.
Conclusion
A number of issues in health care for people who use methamphetamine and health care professionals were rooted in current policy pertaining to zero tolerance. Without harm reduction on offer, the health care system can expect to see increased levels of patients not receiving or completing treatment needed. As well there is a greater risk of health being compromised as a result of policy and current practice that suggests abstinence is more valued over patient engagement. Future research would benefit from looking at how these issues can be addressed proactively within the hospital through programs and interventions that emphasize harm reduction.
Footnotes
Appendices
Author Contributions
Three authors (CF, AR and MS) contributed to the conception and design of the study as well as funding acquisition. Three authors (CF, JS, and LS) conducted data curation, the qualitative analyses and developed the subsequent model. All six authors (CF, JS, LS, AR, CD and MS) contributed to the writing of all sections and made edits to the manuscript. All six authors contributed to the revision of the manuscript and have approved the submitted version. All six authors supported project administration and investigation, and provided supervision throughout the study including the writing process for this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge Health Canada’s Substance Use and Addictions Program and the staff at all our community partners and agencies for their support in this research.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.