
Abstract
Marijuana use initiation is associated with numerous health and behavioral consequences, particularly among young adolescents. Finding easily identifiable risk markers for marijuana initiation is an important step for targeting primary and secondary prevention efforts. This study used data from the 2010-2014 National Survey on Drug Use and Health to evaluate the association between residential mobility (no mobility, low mobility, high mobility [ie, transience]), and major depressive episode(s) (MDE) on marijuana initiation among adolescents (12-17) and young adults (18-20). Age-stratified logistic regression models indicated that among 12- to 13-year-old adolescents, mobility in the past 5 years and past year MDE have a multiplicative effect on the odds of past year marijuana initiation. Among adolescents aged 14 to 15 years, both mobility and MDE were independently associated with marijuana initiation, but there was no interaction. Among older adolescents (aged 16-17 years), only transience (⩾3 moves in the past 5 years) was associated with marijuana use initiation, and although MDE was significantly associated with marijuana initiation, there was no interaction with mobility. Among young adults, mobility was not associated with marijuana initiation. Residential mobility among young adolescents is an easily identifiable risk marker that may serve as an indicator for physical and mental health professionals, school personnel, and parents to use in targeting both depression and marijuana prevention efforts.
Keywords
Introduction
Marijuana use is associated with a number of adverse physical and behavioral health outcomes, including poorer performance on neurocognitive tests, lower educational attainment, and risk of marijuana use disorder (ie, abuse or dependence).1–5 This is especially true for adolescent marijuana use initiates where the younger the age of first use, the more severe these outcomes tend to be.1–5
Residential mobility and residential transience are recently identified potential risk markers for mental health and substance use disorders, including marijuana use disorder.6–8 Residential mobility (ie, moving) has been shown to be a source of life stress and social disruption among adolescents that can interrupt friendship networks 9 and interfere with school attachment10,11 and has been linked to poor mental health outcomes.10,12 To date, the strongest evidence of the adverse psychiatric sequelae of residential mobility comes from a population cohort study in Denmark, which found that increasing number of cross-municipality residential moves from birth through 14 years of age increased the risk of developing a range of psychiatric disorders from mid-adolescence to early middle age, particularly marijuana use disorder (per medical record review using the International Classification of Disease, 8th to 10th revisions, marijuana misuse disorder). 7 In addition, moves during older childhood were more strongly associated with marijuana use disorder than moves earlier in childhood.
Although suggestive, it is not clear from this study whether residential mobility is a risk marker only for progression from marijuana use to marijuana use disorder or whether it is also a risk marker for marijuana use initiation. To date, there is no clear consensus as to the link between residential mobility and marijuana use initiation.
A 1998 Canadian study of Ontario residents found that residential mobility prior to age 16 was associated with an earlier age of marijuana initiation. 13 However, a more recent study using data from the UK-based Avon Longitudinal Study of Parents and Children found no association between childhood mobility and childhood marijuana use initiation in fully adjusted models. 14 These studies had significant differences in their methods. The Canadian study focused on cumulative number of moves prior to age 16, whereas the Avon study used number of moves prior to the data collection wave and controlled for the distance of the move. In both cases, analyses examined residential mobility as a continuous variable and did not examine whether there was a particularly high risk for marijuana use initiation among those who moved frequently, ie, were transient.
Residential transience is loosely defined as an uncommon, frequent rate of residential mobility and is a highly visible aspect of the larger construct of housing instability, which also includes homelessness and other problems in maintaining stable housing. 15 Similar to residential mobility, residential transience may act as a social stressor among adolescents. However, the frequent nature of the moves is postulated to produce more severe disruption to social networks including possible social isolation, preventing consistent access to health care, and inhibiting education attainment through multiple disruptions to school placement and educational program continuity. Most studies to date have focused on the relationship between any mobility and mental health problems and have not examined whether transience has a particularly strong association with marijuana use.
Identifying highly visible risk markers for marijuana use initiation can greatly help target prevention efforts. Residential mobility, particularly transience, is readily apparent to parents, schools, and often health care providers and is an easily queried characteristic that can be use in screening for intervention. Therefore, evaluating an association between marijuana use initiation and residential mobility has the potential to have broad public health implications. Moreover, examining whether transience has a particularly strong association above that of average mobility can better target interventions to the highest at-risk populations and may identify a subgroup with particular service needs.
An additional consideration is the relationship between residential mobility, transience, and depression. Depression is a well-documented risk marker for marijuana use initiation, with a stronger association among younger adolescents. 16 Several studies have shown an association between residential mobility (or transience) and depression, and there is some evidence that the co-occurrence of transience and depression may be particularly associated with adverse mental health outcomes.8,17,18 For example, one study found that adults who moved ⩾3 times in the past year and who had had a major depressive episode (MDE) in the past year had a higher odds of suicidal thoughts, plans, and attempts than those with transience or MDE alone. 17 However, to date, there have been no identified studies that evaluate the interaction between residential mobility or transience and MDE on the risk of marijuana use initiation and examine whether the interaction of mobility (or transience) and MDE is particularly problematic for marijuana use initiation.
Using the prior studies as a foundation, this study evaluates the following hypotheses using a nationally representative sample of adolescents and young adults aged 12 through 20 years:
Residential mobility is associated with marijuana use initiation, and residential transience will have the strongest association with marijuana initiation.
The association between residential mobility (including transience) and marijuana use initiation will differ across ages from young adolescents through young adults and will be the strongest among older adolescents and young adults.
Major depressive episode will interact with residential mobility and transience to exacerbate the association with marijuana use initiation.
Methods
Data source
Data were from the 2010 through 2014 National Survey on Drug Use and Health (NSDUH), public use files.19–23 National Survey on Drug Use and Health is a cross-sectional complex survey of approximately 68 000 respondents annually and is a main source of data on the prevalence, patterns, and consequences of substance use and mental disorders in the US civilian, noninstitutionalized population, age 12 years and older. 24 National Survey on Drug Use and Health samples residents of households and noninstitutional group quarters (eg, shelters, rooming houses, and dormitories) and civilians living on military bases but excludes homeless persons who do not use shelters, active duty military personnel, and residents of institutional group quarters. National Survey on Drug Use and Health uses audio computer-assisted self-interviewing procedures to provide the respondent with confidentiality and to increase honesty in reporting illicit drug use and other sensitive issues. Weighted response rates for adolescent respondents to NSDUH ranged from 80.0% to 85.0% in the 2010 through 2014 NSDUHs.24,25
Because these analyses focused on past year marijuana use initiation among adolescents and young adults, the sample was restricted to respondents aged 12 through 20 years, who had not used marijuana for the first time more than a year prior to the survey to create a retrospective cohort design (n = 95 626; excluded n = 22 180).
National Survey on Drug Use and Health is conducted under the oversight of the RTI International Institutional Review Board (IRB). Informed consent is obtained from all respondents. This study was conducted using the publicly available, de-identified public use files and was therefore exempt from IRB review.
Measures
The primary outcome was past year marijuana use initiation. Past year marijuana use initiation was calculated by taking the age of the respondent and subtracting the age at which they reported first using marijuana. Those who were the same age or 1 year younger when they first used marijuana were considered past year marijuana initiators (n = 8937). Those who had never used marijuana were considered noninitiators (n = 88 689).
There were 3 independent variables. The primary independent variable was residential mobility and residential transience. Residential mobility was measured in the NSDUH as the number of residential moves a respondent had in the past 5 years (0, 1, 2, 3, 4, 5, ⩾6 moves). Residential transience, which is considered to be a higher rate of relocation than average, has no consistent definition in the literature; therefore, we categorized moves into no mobility (0 moves), low mobility (1-2 moves), and transience (⩾3 moves) in the past 5 years, which equated to 53.5%, 32.7%, and 13.8% of the sample, respectively. Mobility was not treated as a continuous variable because the data are not truly continuous, it is right censored at ⩾6 moves, and has a floor effect (ie, no mobility) and because we were interested in whether low mobility and high mobility (ie, transience) were differentially associated with marijuana use initiation.
The second independent variable of interest was age. One hypothesis was that among older adolescents and young adults, there would be a stronger effect of residential transience, based on prior study findings. 7 To evaluate “windows” of potential vulnerability, age was categorized based on general developmental level and social norms (eg, young adults potentially going to college or moving out of their parents’ houses) into 12 to 13, 14 to 15, 16 to 17, and 18 to 20. Aged 20 years was selected as the top cutoff for age due to the growing number of laws legalizing marijuana use among those aged 21 years or older. Although 2-year-age windows were used for younger adolescents who have rapid maturation, a 3-year-age window was used for young adults due to the slower maturation in this group.
The third independent variable of interest was past year MDE (yes/no). Depression has been shown to have a strong association with marijuana initiation, and these analyses wanted to examine effect modification between MDE and transience on the odds of marijuana initiation. Past year MDE is measured based on criteria set forth in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. 26 More information on the measurement of MDE in youth and adults has been published extensively elsewhere. 27 In this sample, 11 060 adolescents and young adults had past year MDE.
Several covariates were selected to be included in all adjusted models a priori based on prior research and theoretical implications. These included sex, race/ethnicity, school enrollment or employment status, mother living in the household (for those <18 years), father living in the household (for those <18 years), metropolitan area, poverty status (based on family income and household size, defined per Department of Health and Human Services guidelines), and health insurance status. Parental residence in the household is not assessed for adult respondents (aged 18 years or older).
Analysis
All analyses were conducted using SUDAAN 28 version 11.0.1 to account for the complex weighted sampling design. All statistical tests were 2-tailed and tested at α = .05. First, weighted sample descriptive statistics were generated for the sample overall and by marijuana initiation status. Overall, the Shah Wald F tests were used to test for significant differences in covariate distribution by marijuana initiation status, and then, pairwise t tests were conducted for the proportions across each covariate group for those significant in the overall Shah Wald F test. The t tests were used (rather than χ2) for post hoc comparisons because they better reflect the test statistic under finite sample sizes in complex survey data. 29
Second, weighted annual average estimates of past year marijuana use initiation were generated by mobility in the past 5 years in each age group, and logistic regression was used to test the main effects of residential mobility on marijuana use initiation in each group. Next, an interaction effect was tested using logistic regression to statistically evaluate whether the relationship between residential transience and marijuana use initiation differed by age group. Interaction testing was conducted in unadjusted (ie, only the main effects and interaction term) and adjusted models.
Third, unadjusted and adjusted age-stratified logistic regression models were used to test the interaction between residential transience and MDE on marijuana use initiation in each age group. Age-stratified, 2-way interaction models are reported instead of a 3-way interaction model for improved interpretability, although a 3-way interaction model was tested for thoroughness.
Fourth, age-stratified logistic regression models including an interaction between mobility and MDE controlling for additional covariates were conducted to determine whether there was a significant association between residential mobility, MDE, and marijuana use initiation while controlling for other potential confounders.
Finally, additional logistic regression models were created to test the specificity of the association of residential mobility with marijuana use initiation versus operating as a more general indicator of substance use risk. Alcohol use is highly correlated with marijuana initiation and use. Therefore, we reran the existing models controlling for any past year alcohol use. Due to the high correlation between alcohol use and our outcome of interest, if the association between mobility and marijuana initiation remained significant after adjusting for alcohol use, then it suggests a marijuana-specific effect of mobility. However, if the association between mobility and marijuana use is attenuated, this suggests that mobility may operate as a risk marker for substance use in general.
Results
Correlates of marijuana use initiation
From 2010 through 2014, an estimated annual average of 2 764 200 adolescents and young adults, aged 12 through 20 years, initiated marijuana use in the past year. The weighted prevalence of past year marijuana use initiation generally increased with the level of mobility in the past 5 years, with those with marijuana use initiation more likely to report transience compared with those without initiation (15.8% vs 13.6%, t test P < .001, Table 1). Marijuana use initiation was also associated with older age, being non-Hispanic white, not having a mother in the household, not having a father in the household, living in a nonrural area, and having had MDE in the past year. Marijuana use initiation was not associated with sex, employment or school enrollment, poverty, or health insurance status.
Characteristics of adolescents aged 12 to 17 years by past year marijuana initiation, 2010-2014 annual averages: percentages and standard errors.

Test for differences by marijuana initiation status: Overall Wald F test, P < .01.
Not collected among adults aged 18 to 20 years.
College students living in dorms are excluded from the poverty status calculation (n = 2434).
Pairwise t test P < .05.
Pairwise t test P < .01.
Mobility and age
Figure 1 demonstrates the weighted annual average prevalence of marijuana use initiation by mobility and age group. Overall, adolescents and young adults with transience in the past 5 years were significantly more likely to have initiated marijuana in the past year. The Shah Wald F test analyses demonstrated a significant main effect between mobility and marijuana use initiation in the total sample and all but the oldest age groups (P < .05). Pairwise testing indicated that among the younger age groups, both low mobility and transience were significantly associated with past year marijuana use initiation, whereas among those aged 16-17 years, only transience was associated with marijuana use initiation. There was no main effect between residential mobility or transience and marijuana use initiation among young adults aged 18 to 20 years.
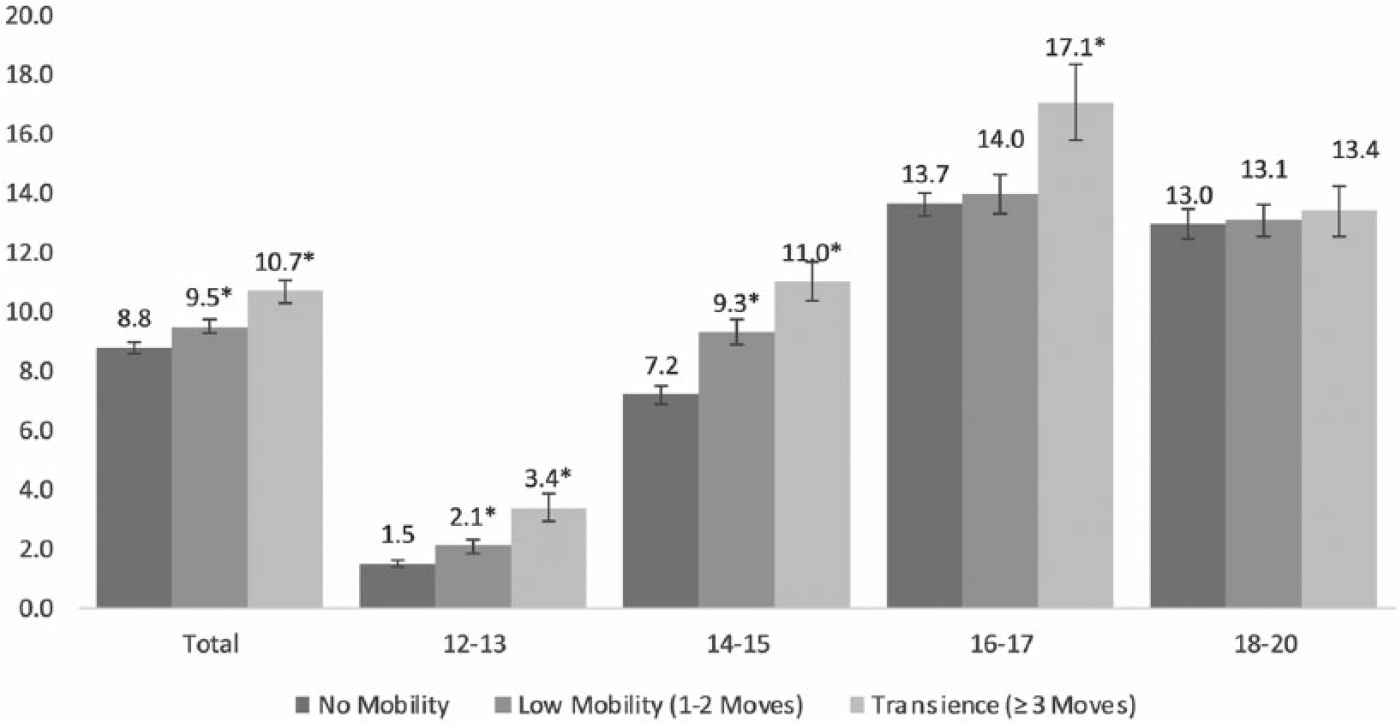
Past year marijuana use initiation among adolescents and young adults by level of mobility in the past 5 years, overall and by age. 2010-2014 annual averages, percentage, and standard error (National Survey on Drug Use and Health). *Difference between marijuana use initiation among this level of mobility was significantly different from the estimate for marijuana use initiation among those with no mobility within that age group.
The logistic regression test for the age by mobility interaction on the odds of marijuana use was significant (Shah Wald F test = 4.64 [6], P < .001), indicating that the association between mobility and initiation was not consistent at all ages. This interaction remained significant when all covariates (and MDE) were included in the model (Shah Wald F test = 2.27 [6], P = .04); therefore, all further models were stratified by age group (12-13, 14-15, 16-17, and 18-20).
Four age-stratified logistic regression models were then used to test for a significant interaction between mobility and MDE status on marijuana use initiation. The interaction of mobility and MDE on the odds of marijuana initiation was significant only among 12- to 13-year olds (12-13 Shah Wald F test = 4.04 [2], P < .05; 14-15 Shah Wald F test = 0.78 [2], P = .463; 16-17 Shah Wald F test = 1.17 [2], P = .314; 18-20 Shah Wald F test = 2.42 [2], P = .093). Similar results were obtained in fully adjusted models; therefore, mobility by MDE interactions was retained only in that model. The final models were stratified by age and included all a priori selected covariates and the significant interaction where appropriate. For additional thoroughness, we tested the 3-way interaction between age, mobility, and MDE on marijuana use initiation. This was significant in both unadjusted and adjusted models (P < .05, detailed results available on request). However, for easier interpretability, we present the age-stratified results below.
Stratified models
As noted, the residential mobility by MDE interaction was significant for the youngest adolescents only, those aged 12 to 13 years. Among young adolescents with no MDE, low mobility in the prior 5 years was not associated with increased odds of marijuana use initiation (Table 2). However, among young adolescents, transience in the absence of MDE was associated with 1.8 times the odds of past year marijuana initiation (odds ratio [OR] = 1.89, 95% confidence interval [CI] = 1.34-2.67). Past year MDE among young adolescents who had no mobility was associated with 4.1 times the odds of marijuana use initiation (OR = 4.09, 95% CI = 2.37-7.07), those who had low mobility and had MDE had 5.0 times the odds of marijuana use initiation in the past year (OR = 4.98, 95% CI = 2.51-9.86), whereas those who had transience and had MDE had 2.6 times the odds of marijuana use initiation (OR = 2.58, 95% CI = 1.40-4.75).
Adjusted ORs and 95% CIs of past year marijuana use initiation among adolescents and young adults aged 12-20 years, by age group.

Abbreviations: CI, confidence interval; NA, not applicable; OR, odds ratio.
College students living in dorms are excluded from the poverty status calculation.
OR significant at P < .05.
OR significant at P < .01.
In addition, non-Hispanic black adolescents in this age group were less likely than their white counterparts to have initiated marijuana in the past year, whereas young Hispanic adolescents were more likely to initiate marijuana use. Not having a mother living in the household and not having a father living in the household were both associated with significantly increased odds of marijuana use initiation. However, in this age group, sex, school or work enrollment, poverty status, metropolitan area, and health insurance status were not associated with marijuana use initiation.
Among adolescents aged 14-15 years, mobility and MDE had independent associations with the odds of marijuana use initiation. Adolescents with low mobility in the past 5 years had 1.2 times the odds of past year marijuana use initiation (OR = 1.19, 95% CI = 1.02-1.40). Those with transience had 1.3 times the odds of past year initiation (OR = 1.34, 95% CI = 1.13-1.59). Past year MDE was also independently associated with 2.2 times the odds of marijuana use initiation compared with those without MDE in this age group (OR = 2.18, 95% CI = 1.83-2.61). Not having a mother living in the household and not having a father living in the household significantly increased the odds of past year marijuana use initiation; moreover, those living in nonmetropolitan areas were less likely to initiate marijuana use compared with those who lived in a large metropolitan area. The other covariates were not significantly associated with marijuana use initiation in this age group.
Among older adolescents aged 16 to 17 years, low mobility was not significantly associated with increased odds of marijuana initiation. However, having transience in the past 5 years was associated with 1.3 times the odds of marijuana use initiation compared with no mobility (OR = 1.27, 95% CI = 1.04-1.56). Past year MDE was associated with 1.7 times the odds of marijuana initiation (OR = 1.72, 95% CI = 1.49-1.98) among adolescents aged 16 to 17 years. Similar to other models, not having a mother living in the household and not having a father living in the household were associated with increased odds of marijuana use initiation. Moreover, those with a family income 200% or more above the federal poverty level were more likely to initiate marijuana use in the past year, compared with those with a family income below the poverty level. Adolescents reporting a race/ethnicity of non-Hispanic other had a lower odds of initiation compared with non-Hispanic white, as did those living in a nonmetropolitan area compared with those living in a large metropolitan area.
Among young adults aged 18 to 20 years, there was no significant association between residential mobility and past year marijuana initiation. However, past year MDE was associated with 1.7 times the odds of marijuana use initiation (OR = 1.73, 95% CI = 1.43-2.08). The odds of marijuana use initiation was significantly lower among women compared with men, non-Hispanic other adults compared with non-Hispanic white adults, those not enrolled in school or work compared with those in school or working, those living in a nonmetropolitan or small metropolitan area compared with those living in a large metropolitan area, and among those without health insurance, compared with those with insurance.
Alcohol use adjusted models
Analyses to evaluate the specificity of the association between mobility and marijuana use initiation were conducted by replicating the analyses while including any past year alcohol use. Past year alcohol use was strongly correlated with past year marijuana initiation. More than 80% of all past year marijuana use initiates aged 12 to 20 years reported past year alcohol use, compared with less than a quarter of those who had not initiated marijuana use (81.7 vs 23.4, t test P < .001). This was consistent across all 4 age categories, 59.2% of adolescent marijuana use initiates aged 12 to 13 years, 72.3% of those aged 14 to 15 years, 82.5% of those aged 16 to 17 years, and 90.1% of those aged 18 to 20 years had used alcohol in the past year, compared with 5.3%, 16.7%, 29.5%, and 45.3% of nonmarijuana use initiates, respectively (t test P < .001).
In multivariable models adjusting for past year alcohol use, none of the mobility by MDE interactions were significant for any age group. Therefore, only main effects were modeled. Among adolescents aged 12 to 13 years, adolescents with transience had a 1.3 times greater odds of marijuana use initiation compared with those with no mobility (OR = 1.26, 95% CI = 1.04-1.55). There was no association between lower level mobility and marijuana use initiation after controlling for alcohol use. Moreover, the overall transience variable only approached significance (Wald χ2 = 2.95 [2], P = .056). Mobility was not associated with marijuana use initiation after controlling for alcohol use in any other age group (results not shown, available on request).
Discussion
These findings indicate that residential mobility, particularly transience, is a risk marker for marijuana use initiation, which is consistent with a number of prior studies on poor mental health indicators, substance use, and marijuana use specifically.6,7,12,13 Prior studies have found that residential mobility in older adolescents and young adults is a stronger correlate of mental health outcomes than among younger adolescents. 7 However, we found no independent association between residential mobility or transience and marijuana use initiation among young adults, and only transience was associated with marijuana use initiation among older adolescents. This may be due to different study designs, including different populations (ie, Canada, the United States, and the United Kingdom), different measures of mobility (eg, cross-municipality moves 7 vs any moves), or different mental health outcomes. Particularly, Mok et al who found cross-municipality moves in late adolescents were more strongly associated with marijuana use disorder than moves in younger adolescents while we examined marijuana initiation, a related but distinctly different outcome. There may also be some differences due to the inclusion of MDE in models with transience on marijuana initiation. Among younger adolescents, MDE is relatively uncommon, whereas MDE prevalence increases substantially after puberty and peaks in early adulthood. 30 It may be that prior study findings found a stronger association between mobility and marijuana in older adolescents because the association between MDE and marijuana was stronger and uncontrolled for in older adolescents in other studies. Thus, additional prospective research is needed for replication with additional statistical modeling of other marijuana outcomes and replication of our results in other populations.
Similar to prior studies, past year MDE was correlated with marijuana use initiation among all age groups. Moreover, young adolescents with both residential mobility (1-2 moves) in the past 5 years and past year MDE have particularly higher odds of marijuana use initiation. It is possible that residential mobility operates as a life stressor among those made more vulnerable to substance use by the presence of MDE.31,32 However, this relationship remained significant after controlling for other stressors and proxies thereof, including minority status, mother or father not living in the household, poverty level, and lack of health insurance, suggesting that residential mobility may have aspects that are associated with young adolescents’ substance use in a particular way. Possible explanations may be that residential mobility disrupts social support networks, leading to an increased risk of poor peer relations or an increased chance of meeting new, more delinquent peer groups, which prior research has found to be associated with marijuana use.33–36 Moreover, MDE may make it more likely that these disruptions lead to negative peer relations.37–39 Prior research has indicated that youth with MDE have a harder time making new friends and may be more likely to associate with a deviant peer group,38,40 but the specific mechanisms of stress related to residential mobility (particularly in the absence of homelessness) are understudied and remain an important avenue for future research. It is also important to consider the role of parental control on the mobility of children. Although our analyses controlled for some parental factors and related characteristics (eg, poverty status, mother or father living in the household [when available], and insurance status), we were not able to control for unmeasured characteristics such as parental history of substance use and mental health problems, which may affect mobility. Future research examining these factors is needed.
Post hoc analyses conducted to determine whether the association between mobility and marijuana use was specific to marijuana use suggested that mobility may be more of an indicator of general substance use risk, rather than a risk marker for marijuana use specifically. This supports the idea that mobility is acting as a general life stressor and may also be a marker of other risk processes leading to substance use initiation. As one of the first studies examining the role of mobility on marijuana use initiation, we focused on evaluating simple main effects and one interaction term. However, more advanced modeling techniques (eg, path analysis or other structural equation models) that can examine direct and indirect paths of mobility to substance use initiation are needed to better evaluate underlying mechanisms of effect.
In accordance with prior studies, there was a strong association between MDE and marijuana use initiation among all age groups, even in the absence of mobility. 16 One unexpected finding was that among 12- to 13-year olds with past year MDE, the OR for marijuana use initiation appeared to be higher among those with no and low mobility than among those with transience. This was the only age group in which low mobility had a larger OR than transience. Although there is no clear indication of why this might be, there are several possible explanations. First, the significant interaction effect may have been a result of type 1 error, which would mean that the significant action was a spurious finding and therefore only the main effects of MDE and mobility should have been modeled in this age group. Alternatively, there is evidence that small sample sizes among this age group may have underpowered analyses in this model. When the reference group for this model was changed from those with no MDE and no mobility to those with MDE and ⩾3 moves, there was no significant difference in the odds of marijuana initiation between those with low mobility versus those with transience for those with MDE. Moreover, the CIs for the estimates of marijuana use initiation among 12- to 13-year olds with MDE were large, suggesting substantial imprecision in the estimates. Alternatively, it may be that young adolescents with MDE are systematically different from those with MDE in ways that are associated with transience and not identified or on not available as covariates not collected in NSDUH. Major depressive episode in young adolescents is rare, and therefore, this possibility cannot be discounted. Future research with additional covariate controls (eg, reasons for moves, housing characteristics, and parental characteristics such as mental health history) and examination of young adolescents with MDE would greatly enhance future studies.
Notably, MDE and mother or father not living in the household were the only variables consistently associated with increased odds of marijuana initiation across all age groups (except young adults, where mother and father in the household was not available). Being of non-Hispanic “other” race/ethnicity and living in a nonmetropolitan area were associated with reduced odds of marijuana initiation but only among older adolescents and young adults. This reaffirms that different developmental windows may have different risk markers for marijuana use initiation. However, as NSDUH is not designed as a prospective study, other studies must be relied on to evaluate these types of causal risk factors and their interplay across development (as well as the role of living with parents among young adults). The main purpose of including these variables in this study was to control for possible confounding, rather than test causal hypotheses.
Another limitation to these findings is that MDE measurement and marijuana use initiation occurred during the same time frame (past year), preventing establishing temporality of these 2 variables in this study. Additional prospective confirmation of the role of residential mobility and transience, MDE, and marijuana use initiation would greatly strengthen these results. Although the youngest adolescents displayed an independent and multiplicative association between residential transience and MDE, on the odds of marijuana use initiation, the relationship between mobility and marijuana use initiation decreased across the older age groups. Although it may be that mobility and transience is not a significant risk marker for marijuana use initiation at older ages, it may also be that MDE lies in the causal pathway between mobility and marijuana initiation among older adolescents, and controlling for MDE obscures this association. Without age of onset and duration information for MDE, which are not available in NSDUH, it is not possible to evaluate this possibility.
Finally, it must be acknowledged that initiation of marijuana use does not always lead to regular use or misuse of marijuana. The NSDUH does not collect the age of initiation for regular marijuana use, which prevents the determination of the temporal order of mobility and initiation of regular use. Additional research is needed to evaluate whether mobility is only a marker for initiation or may also be associated with progression to regular use or misuse. Both prior research findings, which have indicated that early initiation is more strongly associated with adverse health effects than initiation among older adolescents, and this study findings, which indicate that mobility was most strongly associated with initiation in the youngest age group reinforce the significance of these findings.
Despite these limitations, this study is the first to examine the role of residential transience on marijuana use initiation and is the first to examine the association of mobility and marijuana initiation by age group. The use of a nationally representative sample of US adolescents and young adults strengthens the generalizability of these findings, and the additional evaluation of the interaction of mobility by MDE has provided further nuance to these results. Moreover, these findings provide a foundation for future research into the association between residential mobility and marijuana use. Future research may consider other important facets of marijuana use, such as the role between mobility and heavy use or the progression from use to marijuana use disorder and if the association between mobility and substance use initiation is specific to marijuana or represents an underlying vulnerability to any substance use. Moreover, future research is needed to extend to populations not covered in the survey frame, including homeless individuals not using shelter services, active duty military personnel, and those living in institutions (eg, psychiatric facilities or residential treatment homes).
Residential mobility and transience among young adolescents is an easily identifiable risk marker and may serve as an opportunity for physical and mental health professionals, school personnel, and parents to engage in screenings and conversations with youth about both depression and marijuana use to help primary and secondary prevention efforts. Moreover, city-based and community-based efforts at stabilizing high residential mobility may contribute to reductions in MDE and marijuana use among young adolescents and adults. Program evaluations of these efforts may consider evaluating these outcomes to aid to estimate the public health impact of these programs and to provide more information of possible causal relationships between mobility and mental health and substance use outcomes. 41
Footnotes
Peer Review:
Six peer reviewers contributed to the peer review report. Reviewers’ reports totaled 2714 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CG conceptualized this study, conducted analyses, and wrote the manuscript. VLF-H and JW contributed to analyses and writing of this manuscript.