
Abstract
Objectives:
Methamphetamine (METH) use has been associated with impairments in a variety of cognitive functions. In this study, it was aimed to assess the relation between cognitive measures and frequency of METH use.
Methods:
Ninety-eight participants with methamphetamine use disorder were assessed with Wisconsin Card Sorting Test (WCST), Victoria-Stroop Word Color Test (SWCT), Trail Making Test (TMT) A and B. Participants were followed up during 6-month period with multiple urine toxicology tests (at baseline, month 1, month 2, month 3 and month 6).
Results:
Participants who had their prescriptions regularly were more likely to have higher rates of METH-negative urine results (P = .003). Participants who had more correct numbers, completed more categories and had more conceptual level responses on WCST were more likely to use lower frequency of METH (OR = 0.006, P < .01; OR = 0.171, P < .001; OR = 0.024, P < .001; respectively). The higher error numbers and perseverative error rates on WCST were associated with more frequent METH use (OR = 0.023, P < .001; OR = 0.076, P < .001). Interference factor on SWCT was related with lower frequency of METH use whereas color naming factor on SWCT was related with higher rates of urine results (OR = 0.012, P < .001; OR = 3.628, P < .001; respectively). Higher TMT B-A score was related with more frequent METH use, although the significance disappeared after adjustment (OR = 0.002, P < .001). Having psychotic symptoms predicted less frequent use, but after adjustment for other significant variables, there was no significance.
Conclusion:
Lower frequency of METH use in the follow-up could be predicted by neurocognitive assessments. Deficits in executive functions, attention, set-shifting and mental flexibility seems to be the most effected domains and this effect may be independent from the severity of psychotic symptoms.
Introduction
Methamphetamine (METH) abuse is a global problem, in Turkey it is reported that the supply and use of methamphetamine have increased gradually within last 10 years. 1 About 27 million substance users are estimated to use amphetamine-type stimulants globally. 2 Amphetamines refer to both amphetamine and structurally similar METH, a more potent derivative of amphetamine. 3 Amphetamines act on the central nervous system, its acute effects include a heightened sense of alertness increased energy; heightened curiosity; anorexia; decreased fatigue; elevated mood; dose-dependent effects on focus, attention and concentration; and elevated interest in environmental stimuli. 4
Beyond the comorbidities including depression, anxiety, cardiovascular diseases, sexually transmitted infections or blood borne viruses associated with regular METH use, METH-induced psychosis may be representing an important aspect of the use disorder. 5 While METH use can precipitate and exacerbate psychotic symptoms in persons with schizophrenia, it has also been recognized that such drug use produced psychotic symptoms even in persons with no history of psychotic disorder. 6 Frequency of psychosis in METH use was reported to exceed 50% in some reports, especially in regular users. 7
Additionally, persons with METH use disorders entering in substance use disorder treatment are more likely to be referred by criminal justice system. 8 An increase in violent behavior was reported from a large-population study; 9.5 times greater with regular METH use, 2 times greater with psychotic symptoms in addition to METH use compared with METH users who had no use in the past month. 9 Greater criminal justice-related admissions might result in longer residential treatments and worse outcomes. 10
Within these context, there has been debate about what plays an important role in less frequent use and better treatment results. Lack of approved specific effective treatments and non-adherence issues for the disorder might have negative consequences for the patient and significant others. 11 In a recent study from 2 different rehabilitation centers investigating treatment drop-outs and METH-negative urine result rates, it was found that 25% of participants showed METH-abstinence at 12 months after residential treatment. 12 There has been a powerful emphasis on the fact that continuing abstinence declines over time with early periods of abstinence (especially first 24 weeks of treatment) predicting later and continuing abstinence.13,14
Cognitive impairment, on the other hand, is also a core feature of psychiatric disorders and a significant predictor of psychosocial functioning.15,16 The possibility of identifying a distinct cognitive profile in substance use disorders leads studies assessing cognitive functioning in patients. Chronic methamphetamine use has been associated with impairments in a variety of cognitive functions including episodic memory, executive functions, information processing speed, motor skills, language, and visuo-constructional abilities. 17 These higher-level cognitive processes are closely associated with impulsive behaviors, compulsive drug use and craving therefore cognitive impairments may increase the risk of relapse among individuals with METH use. 18 Among the core executive functions inhibition (especially behavioral and cognitive) and related attention processes plays an important role in abstinence. Dealing with drug related cues and craving are also crucial aspects of drug-free lives. Thus cognitive functions such as problem solving, set-shifting, and mental flexibility are essential when abstinence is desired. Although emerging evidence in the literature with cognitive impairments shows the association with lower treatment retention, no study investigated the aforementioned domains among the same METH users sample.18-20
For these reasons, we proposed to carry out a study to understand the effect and interaction of cognitive functioning, severity of psychotic symptoms, demographic factors and medications with a 6-month follow up among METH users which were followed in the outpatient treatment clinic (OTC). Recognizing the predictors of less frequent METH use and its interaction with medication adherence may be helpful for patients and practitioners to create more effective treatment process.
We hypothesized that poorer performance on baseline WCST, SWCT, and TMT would predict more frequent METH use. Merging the lines of evidence of previous studies, we also hypothesized that METH users with better medication adherence would demonstrate lesser METH use compared to non-adherent group.
Materials and Methods
Participants and procedures
This study was planned as a longitudinal prospective cohort study and patients were enrolled from Antalya Atatürk State Hospital OTC. The eligibility criteria were relatively restrictive in an effort to avoid confounding factors. Inclusion criteria were being 18 to 65 years of age, having at least 5 years of schooling, admitted or referred to OTC for substance use treatment, able to understand and sign and informed consent, willing to complete study forms and provide urine samples and using methamphetamine within 30 days prior to the study participation. All the candidates had the ability to understand the Turkish language. Exclusion criteria were having current medical or psychiatric conditions causing impairment or psychiatric treatment in residential or outpatient clinic within 180 days prior to the study participation, meeting DSM-5 criteria for substance or alcohol use disorder except methamphetamine and nicotine, having any legal problem that would preclude consistent participation.
A total of 100 participants who had used methamphetamine within last month were enrolled. Participants were clinically interviewed whether they had had any psychotic episode in the past, none met any DSM-5 criteria for psychotic disorders.
A structured questionnaire was administrated face-to-face by researcher at clinic. Participants were evaluated at admission, and at each follow-up (1, 2, 3, and 6 months after the baseline interview). All participants were followed-up weekly with a structured group therapy program moderated by experienced clinicians. The program which is based on cognitive behavioral and motivation enhancement techniques consists of 20 sessions. Each session was organized with 12 to 16 participants and an experienced therapist. Recruitment of the cohort took place in 2020 and 2021, and follow-up interviews spanned the period from 2020 to 2022. Two patients who had severe suicidal or homicidal thoughts during the follow-up were excluded from the study and transferred to the residential treatment unit.
This study protocol was reviewed and approved by the Ethics Committee of Antalya Research and Training Hospital (approval number 5/19, date 03/09/2020). All subjects were contacted by the author and written informed consent was obtained from all participants. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Measures
Characteristics of past methamphetamine use
Methamphetamine use measures included amount of use during past month, frequency of use during past month (daily, more than weekly, weekly or less than weekly, no use in past month), main route of administration, age of first methamphetamine use, number of months of frequent, or problematic methamphetamine use.
Frequency of methamphetamine use in the follow-up
Urine toxicology analysis was used for every admission. Total number of METH-negative urine results were divided by total sample numbers (4) and multiplied by 100 to calculate the negative urine rate. All patients which were dropped out and gave no urine sample were accepted as positive.
Demographics
Demographics measured included age, sex, insurance, income, employment, schooling and marital status, frequency and amount of tobacco and alcohol use, screening for infectious diseases (HBV, HCV, HIV, VDRL-TPHA), and suicide attempts.
Clinical scales and neurocognitive process assessment
Participants were screened for positive psychotic symptoms using Scale for the Assessment of Positive Symptoms (SAPS). SAPS is a rating scale used by clinician to measure positive symptoms. The scale is split into 4 domains (hallucinations, delusions, bizarre behavior, positive formal thought disorder) and within each domain separate symptoms are rated from 0 (absent) to 5 (severe). 21
Cognitive flexibility was measured with the paper version of Wisconsin Card Sorting Test (WCST 22 ). At admission, all participants were assessed 1 time by same examiner in a quiet room to avoid any interferences that could influence their performance.
The WCST comprises response cards with different types of geometric figures in which participants are required to apply sorting principles through trial and error. Based on feedback of correct or wrong matches participants were expected to adapt to the changing sorting. 23 “Number of trials administered,” “total number correct,” “ total number of errors,” “perseverative responses,” “perseverative errors,” “non-perseverative errors,” “ratio of perseverative errors,” “conceptual level responses,” “ratio of conceptual level responses,” “number of categories completed,” “failure to maintain set,” “trials to complete the first category,” and “learning to learn” category raw points were calculated to represent executive functions.
The ability to inhibit cognitive interference was measured with Stroop Word and Color Test- TBAG form (SWCT). Stroop Test TBAG Form was developed for Turkish standardization studies and was formed by combining the original Stroop and Victorian Forms.24-26
The form consists of 5 sections. The subject’s task is simply to utter the words, color names or name the colors of the inks while ignoring the conflicting printed color names. Time was measured in each section. “Speed factor,” “Color naming factor,” and “Interference factor” measurements were calculated as mentioned in Jensen’s study. 27
Processing speed, sequencing, mental flexibility and visual-motor skills were measured with Trail Making Tests. The test consists of 2 parts (A and B) that must be performed as quickly as possible. Part A requires participants to connect numbers in ascending order whereas part B requires an alternation between numbers and letters. Time required to complete each task was measured. Difference score (B-A) and B/A ratio score were used in the study.24,28
Characteristics of the treatment episode
Participants which had dominantly persistent positive psychotic symptoms (suspiciousness, unusual thought consent and hallucinations) after 1 month abstinence were prescribed oral antipsychotics (APs) or long-acting injectable antipsychotics (LAIs). Oral antipsychotics were started with a dosage of 3 mg haloperidol dose equivalent. Patients who had used and benefited from antipsychotic use in the past were prescribed with the same oral/LAI antipsychotic. Clinical assessments were performed monthly and dosage was elevated to 6 mg haloperidol dose equivalent if clinically needed. LAIs were selected as aripiprazole LAI (400 mg/month) or paliperidone LAI (50 mg/month) which are the minimum dosages available in Turkey. Participants which had dominantly persistent affective syndrome (depression, suicidality, hostility, and self-neglect) after 1 month abstinence were started oral bupropion treatment with 150 mg/day and elevated to 300 mg/day if clinically needed. Participants which had dominantly persistent psychomotor withdrawal symptoms of methamphetamine use (psychomotor retardation, hypersomnia, hyperphagia, distractibility) after 1 month abstinence were started oral modafinil treatment 100 mg/day and elevated to 200 mg/day if clinically needed. Medications were continued during the follow-up process.
Statistical analyses
All statistical analyses were performed with SPSS (version 26.0, IBM) and included descriptive statistics for all categorical and continuous variables. Chi-square tests were used to examine the relationship between urine test results and medication adherence. A fixed-effects generalized linear model was used to determine predictors of frequency of METH use. The main outcome measure was the rate of METH-negative urine test results. In a separate second model, all significant variables (including age and level of education which may be confounding factors for neurocognitive assessments) were included and adjusted odd ratios were calculated. All missing urine test results were accepted as positive. To examine the correlation between sixth month urine toxicology results and clinically relevant continuous variables, Spearman’s correlations were used. For all statistical analyses, P-values were two-tailed and the level of significance was determined using the .05 level.
Results
Characteristics of the sample
Participants had a mean age of 29.4 ± 6.7 years. The majority of group were male (80.6%) and living with family (83.7%). 48% were unemployed, 44.9% were in no-income group, 51% had finished secondary school, 44.9% were single, and 51% had admitted to clinic voluntarily. Mean of SAPS scores of participants was 24.6 ± 20.6.
Substance use
About 96.9% of participants were using tobacco products. 62.2% had not been using alcohol, 29.6% were social drinker which was defined as drinking alcohol in social settings or while socializing with others without any risky or potentially unhealthy behaviors associated with their drinking. Participants reported frequent use of methamphetamine for a mean of 24 ± 19.2 months. The mean age of the first use was 26.4. Smoking was the most common route of administration (91.8%). Almost half of users had used daily (49%), followed by more than weekly (28.6%). At admission, majority of participants’ urine test results were positive for methamphetamine (72.4%) (Table 1).
Sample characteristics and drug use related variables.

48% of participants (47) applied to OTC at first month, 22.4% of participants (22) applied to OTC at second month, 18.4% of participants (18) applied to OTC at third month, 9.2% of participants (9) applied to OTC at sixth month. Mean ratio of methamphetamine-negative urine test results was 17.7 ± 29.8.
Characteristics of the treatment episode
About 24.4% (n = 24) of participants used oral antipsychotics (olanzapine, haloperidol, paliperidone, amisulpride, risperidone, aripiprazole). About 16.3% (n = 16) of participants used LAI antipsychotics (aripiprazole LAI, paliperidone LAI). 12.2% (n = 12) of participants used bupropion, 10.2% (n = 10) of participants used modafinil, and 5.1% (n = 5) of participants used bupropion + modafinil. 7.1% (n = 7) of participants used LAI antipsychotic + modafinil, 6.1% (n = 6) of participants used oral antipsychotic + modafinil, 5.1% (n = 5) of participants used oral antipsychotic + bupropion, and 2% (n = 2) of participants used LAI antipsychotic + bupropion. Eleven participants used no medication (11.2%). A total of 59 participants (60.2%) used antipsychotics whereas there was no significant difference in terms of demographics (P > .05; data not shown).
Neuropsychological assessment results
WSCT results are shown in Table 2. Mean of numbers of trials administered was 111.3 ± 18.6. Mean of numbers of categories completed was 4.5 ± 2. Mean ratio of perseverative errors was 17.9 ± 10.7. Mean ratio of conceptual level responses was 56.1 ± 20.7. Mean of learning to learn category points was −0.09 ± 16.02.
Descriptive statistical overview of Wisconsin Card Sorting Test, Stroop Word Color Test, and Trail Making Tests results.

Abbreviations: SD, standard deviation; SWCT, Stroop Word Color Test; TMT, Trail Making Test; WCST, Wisconsin Card Sorting Test.
SWCT and TMT results are shown in Table 2. Mean score of speed factor was 13.3 ± 6.2 seconds, color naming factor was 0.53 ± 0.06, interference factor was 18.9 ± 11.4 seconds. Mean of total time to completion for part A was 34.2 ± 12.3, for part B was 140.9 ± 86.1 seconds.
Relationship between medication adherence and urine analysis results
In terms of treatment compliance, 48% (n = 47) of the participants applied to OTC, 33.7% (n = 33) received all of their planned prescriptions and 26.5% (n = 26) of all participants had methamphetamine-negative urine test results at first month (P < .001). At second interview (month 2), 22% (n = 22) of the participants applied to OTC, 19.4% (n = 19) received all of their planned prescriptions, and 17.3% (n = 17) of all participants had methamphetamine-negative urine test results (P = .022). At third interview (month 3), 18.4% (n = 18) of the participants applied to OTC, 14.3% (n = 14) received all of their planned prescriptions and 14.3% (n = 14) of all participants had methamphetamine-negative urine test results (P = .13). At last interview (month 6), 9.2% (n = 9) of the participants applied to OTC, 8.2% (n = 8) received all of their planned prescriptions and had methamphetamine-negative urine test results (P = .003) (Figure 1).

Percentages of negative and positive urine toxicology results during the follow-up.
Relationship between neuropsychological assessment scores and urine test results
Among WSCT subsets, total number of trials administered scores and total number of errors were negatively correlated with the ratio of negative urine test results (r = −.39, P = .016; r = −.38, P = .021). Ratio of perseverative errors scores were negatively correlated with the ratio of negative urine test results (r = −.47, P = .003). Ratio of conceptual level responses scores were positively correlated with the ratio of negative urine test results (r = .37, P = .026). Among SWCT and TMT subsets, no item was significantly correlated with urine test results (data not shown).
The assessment of relationship between WCST subsets and urine test results showed that higher ratios of negative urine test results more likely to occur when a participant performed more correct numbers, completed more categories and had more conceptual level responses (OR = 0.006, P < .01; OR = 0.171, P < .001; OR = 0.024, P < .001; respectively). After the adjustment in the regression analysis the relation between conceptual level response subset and negative urine test result weakened. There was a negative relationship between abstinence, total trials, errors and perseverative errors. The higher error numbers and perseverative error ratios seemed to be related with lower ratio of negative urine results (OR = 0.023, P < .001; OR = 0.076, P < .001). In line with these results, higher total trial numbers predicted lower ratio levels of negative urine results (OR = 0.023, P < .001). The relationship persisted after adjustment for other variables.
Among factors related with SWCT, interference factor and color naming factor were related with negative urine results while speed factor showed no relation (OR = −0.012, P < .001; OR = 3.628, P < .001; OR = −0.002, P > .05 respectively). The relationship persisted after adjustment for other variables. In addition, lower TMT B-A scores predicted higher rates of negative urine results, however after adjustment this effect was not statistically significant in the same direction (OR = −0.002; P < .001).
Male, employed and non-daily METH users were more likely to have METH-negative urine results (OR = 0.811, P < .001; OR = 0.445, P < .001; OR = 0.107, P < .05). The relationship persisted after adjustment for other variables. Prescription of oral antipsychotics were negatively related with negative urine results (OR = −0.455, P < .001). Having psychotic symptoms predicted less frequent use, but after adjustment there was no significance (OR = 0.007, P < .001) (Table 3).
The relationship between negative urine result ratios and methamphetamine use, socio-demographics, neuropsychological assessment results and psychotic symptoms.
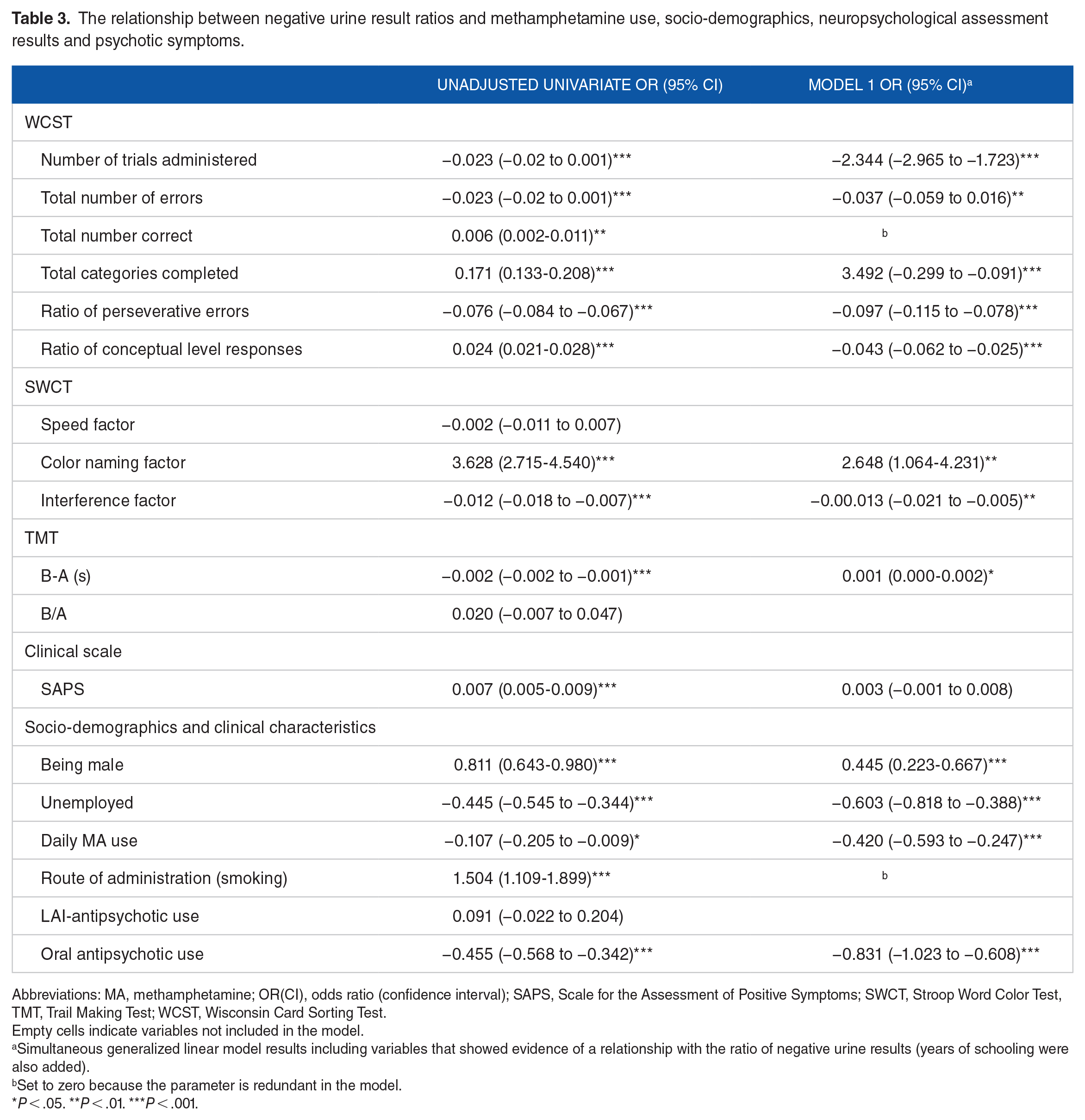
Abbreviations: MA, methamphetamine; OR(CI), odds ratio (confidence interval); SAPS, Scale for the Assessment of Positive Symptoms; SWCT, Stroop Word Color Test, TMT, Trail Making Test; WCST, Wisconsin Card Sorting Test.
Empty cells indicate variables not included in the model.
Simultaneous generalized linear model results including variables that showed evidence of a relationship with the ratio of negative urine results (years of schooling were also added).
Set to zero because the parameter is redundant in the model.
P < .05. **P < .01. ***P < .001.
Discussion
In this study predictors of less frequent METH use were aimed to examine and to the best of our knowledge this is the first follow-up study with METH users in Turkey.
In consistent with previous results, longer retention in treatment was found to be related with better treatment outcomes. Although in our study, results at month 3 did not reach at significance level; other assessments showed that participants who received prescribed medications properly were more likely to have higher rates of METH-negative urine test results. Brecht and Herbeck 14 reported that longer duration of the index episode treatment predicted longer time to relapse. Other studies conducted with patients with cocaine, heroin and alcohol use disorder also showed that participants who experience early relapse are likely to have more difficulty maintaining abstinence.29,30 The current study contributed filling the gap by examining not only abstinence but also less frequent use within the follow-up process.
METH use may lead to profound cognitive deficits, including deficits in executive functions, verbal memory, processing speed, response inhibition and attention tasks.17,31 In order to examine especially problem solving and set shifting WCST was used in our study. 22 In this study results indicated that METH users that continue to use drug performed worse in their executive functions. These results are consistent with those of previous studies which reported executive impairments in METH users. 32 Farhadian et al 33 reported that higher perseverative errors and lower scores in category subset of WCST were found in currently METH-abusing group. Changes in prefrontal cortex volume and white/gray matter densities may show association with poor performance on the WCST.33,35
Stroop test was used to examine distortion of attention, inhibition and set shifting domains. As a deterioration of executive functions, participants who dropped out earlier/continued to use drug performed worse in Stroop task. Worse performance in Stroop task was reported in previous studies.33-35 Deficits which was reported in our study in interference and color-naming but not speed factor suggesting that some aspects of attention are affected by METH use.36-39
TMTs are believed to measure the cognitive domains of processing speed, sequencing, mental flexibility and visual-motor skills. Part A is generally presumed to be a test of visual search and motor speed skills, whereas part B is considered to be a test of mental flexibility. 40 The derived TMT scores such as the difference score (B-A) is meant to remove the speed component from the test evaluation, while B/A ratio score provides an indicator of executive control function.41,42 Thus these two scores were used in our study. The difference score showed association with higher rates of METH use, although significance disappeared after the adjustment. In a recent study with alcohol use disorder patients, Moggi et al 43 reported that a significant impairment on TMT performance, especially for TMT part B. Consistent with the literature, our study showed that METH users which have worse difference scores may have cognitive impairment.
Across a wide range of possible cognitive predictors of less frequent use of METH, we found predictive user characteristics (gender, working status, route of administration, daily use and oral antipsychotic use during the follow-up). Several alternative explorations should be considered. In previous studies, being male has not been reported as a predictor of abstinence and this result may seem interesting.12,15,44 But due to sample size limitation, the result must be interpreted with caution.
We found that unemployment was negatively associated with better outcomes. Unemployed persons have been associated with higher rates of illicit substance use in previous studies. Employment problems resulting lack of insurance may impair the access to the medication. 45 A study assessing the data from the 1993 to 2016 Treatment Episode Data Set reported that unemployment rate was negatively associated with treatment admissions for stimulants. 46
Injecting METH has been related to a lower probability of abstinence and smoking (vs injecting) predicted better outcome in our study.12,44 However this result should be interpreted with caution because of the small sample size. Counseling strategies may focus on syringe users to increase treatment rates.
METH-induced psychosis has been associated with many environmental and genetic risk factors but the course of symptoms varies across the subgroups. It was reported that 26% of all patients had symptoms after a month, and the rate dropped down to 16% after 3 months. 47 A study reporting the data 3 years after treatment in METH-users found no relationship between psychotic diagnosis and treatment retention. 48 In our study, SAPS scores did not predict rates of negative urine results in adjusted model. However given that negative relationship between oral antipsychotic use (vs LAI antipsychotic use) and less frequent use; there may be another common factors beyond the positive psychotic symptoms such as impulsivity related behaviors.49,50
These findings seem to support the cognitive impairment theory in METH users and its relevance with non-adherence and relapse. There are several explanations including neurotoxic effects of methamphetamine on dopaminergic and serotonergic nerve terminals Cognitive impairment as well as altered decision-making in methamphetamine users was reported to contribute to the high rate of relapse even after long-term withdrawal. 51 Thus cognitive training programs or bias modification treatments may lead to promising treatment results. Lately a study from China reported that patients with METH use engaged in the cognitive training program had better cognitive performance after 4 weeks of training, which coincided with changes in impulsive risk decision-making tasks. 52 Moreover, studies have shown that computerized working memory training showed promising treatment effects and even brain plasticity in SUD patients using such stimulants as cocaine and amphetamine. 53 Although there are studies which reported no association between cognitive functioning and relapse, study limitations may play a confounding role in those results. 54
Limitations
This study has several limitations. First, methamphetamine use was confirmed with urine toxicology analysis monthly. However lapses limited with a few days and related false-negative results may have gone unnoticed. Second, heterogeneity and small sample size may influence the results. Inclusion of last month METH users may have contributed to heterogeneity, because of recreational user groups. Third, although patients who had missed the appointments were phone-called in 3 different times, drop-outs may be containing abstinent groups. Another limitation of our approach was that comorbidities with impulsivity and personality disorders were not screened in our study which seems to be an important limitation. Exposure to cues, stress, staying connected with drug-using peers, family factor, and participation in support groups are other protective factors which were not measured in our study.
Conclusion
In conclusion, patients with better treatment compliance had lower relapse rates. Clearly, how to increase treatment retention is still a challenging mission for specialists to overcome. Future research needs to address the difficulties and causes of the potential dropout from treatment risk. Moreover, our results suggest that participants with cognitive impairment in baseline assessment were more likely to have the probability of more frequent METH use even in the patient groups without psychotic symptoms. Deficits in executive functions, attention, set-shifting, and mental flexibility domains may be playing an important role in cognitive impairments. Findings on the difference of cognitive functions in METH users need replication with bigger sample size. Further comparisons of groups with longer follow-up periods could be informative.
Footnotes
Funding:
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SK designed the study, analyzed the data, wrote the manuscript.
Statement of Ethics
This study protocol was reviewed and approved by the Ethics Committee of Antalya Research and Training Hospital (approval number 5/19, date 03/09/2020). Written informed consent was obtained from all participants. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Data Availability Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from the corresponding author.