
Abstract
Introduction:
Cigarette smoking is common among individuals with substance use disorders and those undergoing addiction treatment. Cigarette use is highly comorbid with methamphetamine use, and among individuals who co-use methamphetamine and opioids, nicotine dependence may further complicate smoking cessation efforts. This study examines nicotine dependence levels and associated factors among people who use methamphetamine undergoing methadone maintenance treatment (MMT) in Vietnam.
Methods:
This cross-sectional analysis utilized baseline data from 667 participants enrolled in a randomized controlled trial designed to evaluate the effectiveness of various combinations of behavioral evidence-based interventions for methamphetamine use among patients on MMT in Vietnam (STAR-OM R01DA050486). Data on levels of nicotine dependence and other covariates including demographic, health status, treatment characteristics and substance use were collected. Nicotine dependence was measured using the Fagerström Test for Nicotine Dependence, with a score of 6 or higher indicating high dependence. Logistic regression estimated the association between nicotine dependence and various psychosocial and behavioral factors.
Results:
Overall, 96.7% of the participants were current smokers with 247 of them (38.3%) exhibiting high nicotine dependence. Greater severity of methamphetamine withdrawal symptoms (OR: 1.03; 95% CI: 1.01-1.05) and a high risk of depression, anxiety or stress (OR: 1.76; 95% CI: 1.14-2.72) were associated with increased odds of high nicotine dependence. Conversely, older age at onset of methamphetamine use was associated with lower odds of high nicotine dependence.
Conclusions:
Cigarette smoking was highly prevalent among individuals using methamphetamine during MMT, with many exhibiting high nicotine dependence. Providing smoking cessation support with efforts to manage methamphetamine withdrawal symptoms, could help improve cessation outcomes.
Introduction
Cigarette smoking is a leading cause of preventable death and disease worldwide, contributing to more than 7 million deaths annually. 1 Despite a gradual decline in global smoking rates, the number of smoking-related deaths continues to rise. By 2025, it is estimated that the smoking rate will be around 20.9% of the global population. 2 However, smoking prevalence remains disproportionately high among individuals undergoing addiction treatment. In Vietnam, where Methadone Maintenance Treatment (MMT) has been implemented since 2008 with smoking prevalence is notably high, especially among men (87.3%). 3 Studies examining cohorts with substance use disorders have demonstrated a substantial burden of smoking-related mortality. For instance, Callaghan et al reported that 39% of deaths in groups with opioid use disorder were attributable to smoking-related conditions. 4 Similarly, Bandiera et al found that individuals receiving treatment for mental health and/or substance use disorders experienced a significantly higher prevalence of tobacco-related mortality compared to the general population (approximately 50% vs 30%). 5
Among people receiving MMT, several factors have been identified as potential predictors of nicotine dependence. Prior studies have highlighted the influence of demographic, clinical, and psychosocial factors on smoking behaviors in this population. Duan et al reported that male gender and older age were associated with a higher likelihood of heavy smoking, 6 while Do et al found that employment and HIV-positive status were negative predictors of nicotine dependence. 3 Furthermore, both studies consistently observed that longer MMT duration was associated with a lower likelihood of heavy smoking.3,6 Clarke et al additionally noted that people with more severe opioid addiction as indicated by higher methadone doses, tended to exhibit greater nicotine dependence. 7 Moreover, illicit drug use and psychiatric disorders have been recognized as comorbid conditions contributing to increased smoking rates in this population.8,9
The co-occurring methamphetamine and opioids use have been shown to increase, raising concerns about its potential impact on health outcomes and treatment effort. 10 In Vietnam, alongside the widespread use of heroin, methamphetamine use has also risen among people who inject drugs, with 51% of participants in a recent study reporting current methamphetamine use. 11 A recent study also indicated that approximately 25% of people on MMT also use methamphetamine. 12 Research suggested that methamphetamine share reinforcing properties with nicotine, which may enhance the addictive potential of cigarette smoking.13,14 While evidence indicates that people on MMT have low smoking cessation rate, 15 the interaction between illicit methamphetamine use and smoking may significantly impact smoking cessation efforts in this population. Given these concerns, a deeper understanding of nicotine dependence among people on MMT using methamphetamine is crucial for informing targeted intervention. Therefore, this study aims to investigate nicotine dependence and associated factors among people using methamphetamine while receiving methadone maintenance treatment in Vietnam.
Methods
Study Design
This cross-sectional study utilized baseline data from a large randomized controlled trial designed to identify the optimal combinations of evidence-based interventions to reduce methamphetamine use among people on methadone treatment in 2 biggest cities (Hanoi and Ho Chi Minh) in Vietnam (STAR-OM R01DA050486).16,17
Study Population
Participants provided their verbal consent for screening. Screening included a face-to-face interview with a research assistant to complete the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) 18 and some sociodemographic questions in a private room, and a urine drug screen for methamphetamine. Participants were eligible if they (1) were aged ⩾16 years, (2) scored 10 or higher on the ASSIST for methamphetamine use OR have a positive result on the urine drug screen for methamphetamine, (3) agreed to to participate in the study and provided a written informed consent. People with other psychiatric disorders or communication difficulties that hindered their ability to complete the questionnaire were excluded from the study.
A total of 6709 participants were screened across 15 selected MMT clinics, of whom 667 met the eligibility criteria and agree to participate in parent study. 19 A private space in each clinic was arranged to ensure privacy and confidentiality during the interview. Participants completed the survey administered by trained research assistants during their initial visit.
Measures
Outcome Variable
Smoking status was categorized into 3 groups: non-smokers, former smokers, and current smokers. Patients were classified as non-smokers if they never smoked, former smokers if they smoked but did not smoke in last 30 days while those who smoked in the last 30 days at the time of interview were categorized as current smokers. Among the current smokers, nicotine dependence was measured by the Fagerström Test for Nicotine dependence (FTND) instrument that is applied in other studies conducted in Vietnam.3,20 The point of each question is added up to give a total score ranging from 0 to 10. The higher the Fagerström score, the greater nicotine dependence, and based on the thresholds previously used in Vietnam by Gea Kõks et al 21 participants were categorized into 2 groups: 0 to 5: low dependence; 6 to 10: high dependence.
Covariates
Demographics
Socio-demographic variables consisted of age, sex, ethnic, marital status, education level, employment status, residential area.
Health Status
We used the Depression Anxiety and Stress Scales (DASS-21) to assess participants’ risk of psychological distress. The scale consists of 3 domains: depression, anxiety, and stress - each measured with 7 items rated from 0 (“Not at all”) to 3 (“Most of the time”). The Vietnamese version of this instrument has been used and validated previously, participants were classified as having a high risk of depression (>9), anxiety (>7), or stress (>14).22,23 Participants were then categorized as having a high risk of psychological distress if they met the high-risk criteria for at least 1 domain. Participants underwent a rapid HIV test to determine their HIV status.
Alcohol Drinking
To assess alcohol use, we used Alcohol Use Disorders Identification Test-Consumption (AUDIT- C) which was score ranging from 0 to 12, where 0 to 3 in women and 0 to 4 in men were low-risk drinkers, those who had score ⩾3 in women and ⩾4 in men were considered hazardous drinkers. 24 The AUDIT-C instrument has been validated and applied for Vietnamese population.25,26
Treatment Characteristics
Data on methadone treatment duration and dosage were extracted from medical records. Methadone dosage was categorized into 2 groups: low dose (<80 mg) and high dose (⩾80 mg). Treatment duration was classified into 3 categories: short-term (<12 months), medium-term (12-24 months), and long-term (>24 months).
Methamphetamine Use Characteristics
Methamphetamine use was defined as use of either tablet methamphetamine or crystal methamphetamine. These characteristics were assessed through self-report, including age at onset of methamphetamine use, history of methamphetamine injection (intravenous and/or intramuscular injection), and methamphetamine use in the past 30 days. Specifically, the age at onset was determined based on the earliest age reported for initiation of either form. History of methamphetamine injection was defined as ever having injected either form. Methamphetamine use in the past 30 days was assessed by asking participants whether they had used either tablet or crystal methamphetamine during that period.
The severity of methamphetamine withdrawal symptoms was measured using the Amphetamine Cessation Symptom Assessment (ACSA), which measures symptoms across 3 domains: fatigue (3 items), cravings (2 items), and anxiety (11 items), with higher total scores indicating greater withdrawal severity. 27 The ACSA has been previously utilized in studies conducted in Vietnam. 28
Statistical Analysis
Descriptive statistics were conducted to describe the characteristics and smoking patterns of the participants. Univariate regression models were used to explore the relationship between nicotine dependence and other factors. Any variables with a P-value < .1 was selected for multivariable model along with all variables of well-documented predictors (eg, age, sex, alcohol use, methamphetamine use characteristics, psychological distress, MMT dose, MMT duration) regardless of statistical significance. Multicollinearity among the independent variables was assessed using the Variance Inflation Factor (VIF). Variables with a VIF exceeding 5 were considered for removal based on the magnitude of VIF and theoretical considerations. The final multivariable model retained variables with acceptable levels of multicollinearity. The data was analyzed using Stata 17.0 software.
Study Ethics
The study was approved by the Ethics Committees at Hanoi Medical University (122/GCNHDDDNCYSH-DHYHN) and Ho Chi Minh City University of Medicine and Pharmacy (433/HDDD-DHYD). All participants provided written informed consent prior to their participation in the study. The study was conducted in accordance with relevant laws and institutional guidelines.
Results
Table 1 illustrates the characteristics of the participants. Among 667 participants, the majority were male (88.9%), with mean age was 41.4 years (SD = 7.4). Most participants belonged to the Kinh ethnic group (96.5%) and had an educational attainment of less than 12th grade (70.0%). Nearly half were married or cohabiting with a partner (48.7%), and 62.5% were employed. Approximately one-third of the participants met the criteria for hazardous drinking. The mean age of first methamphetamine use was 31.7 years (SD = 10.2), and 18.7% reported a history of methamphetamine injection. The mean score for methamphetamine withdrawal symptoms was 8.9 (SD = 9.7). In the past 30 days, 77.7% of participants reported methamphetamine use. Nearly 40% were at high risk for at least 1 psychological distress, including depression, anxiety, or stress. The majority of participants were undergoing long-term methadone treatment (70.7%), with approximately half receiving a low methadone dose (47.9%) and the remaining half receiving a high dose (52.1%).
Characteristics of the participants (N = 667).

Table 2 presents the smoking patterns among people who use methamphetamine undergoing MMT. Among 667 participants, 645 (96.7%) were current smokers, with nearly half reporting that they smoked their first cigarette within 5 minutes of waking up and found it difficult to refrain from smoking in prohibited areas. Most participants smoked less than 20 cigarettes per day, and only about one-third reported smoking frequently in the morning. More than a half (55%) of current smokers smoked even when they were ill and stayed in bed. The mean FTND score among current smokers was 4.6 (SD = 2.2), with nearly 40% of participants classified as having high nicotine dependence level.
Smoking-patterns of the participants (N = 667).

The logistic regression model presented in Table 3 shows that higher ACSA scores were associated with greater odds of high nicotine dependence (OR: 1.03, 95% CI: 1.01-1.05). Current smokers with high risk of metal illness also had 1.76 times higher odds (95% CI: 1.14-2.72) of experiencing high nicotine dependence. Older age at the onset of methamphetamine use was inversely associated with nicotine dependence, as individuals with an older age at onset had 0.95 times lower odds of having a high FTND score (OR: 0.95, 95% CI: 0.93-0.98).
Factors associated with high nicotine dependence among current smokers (n = 645).
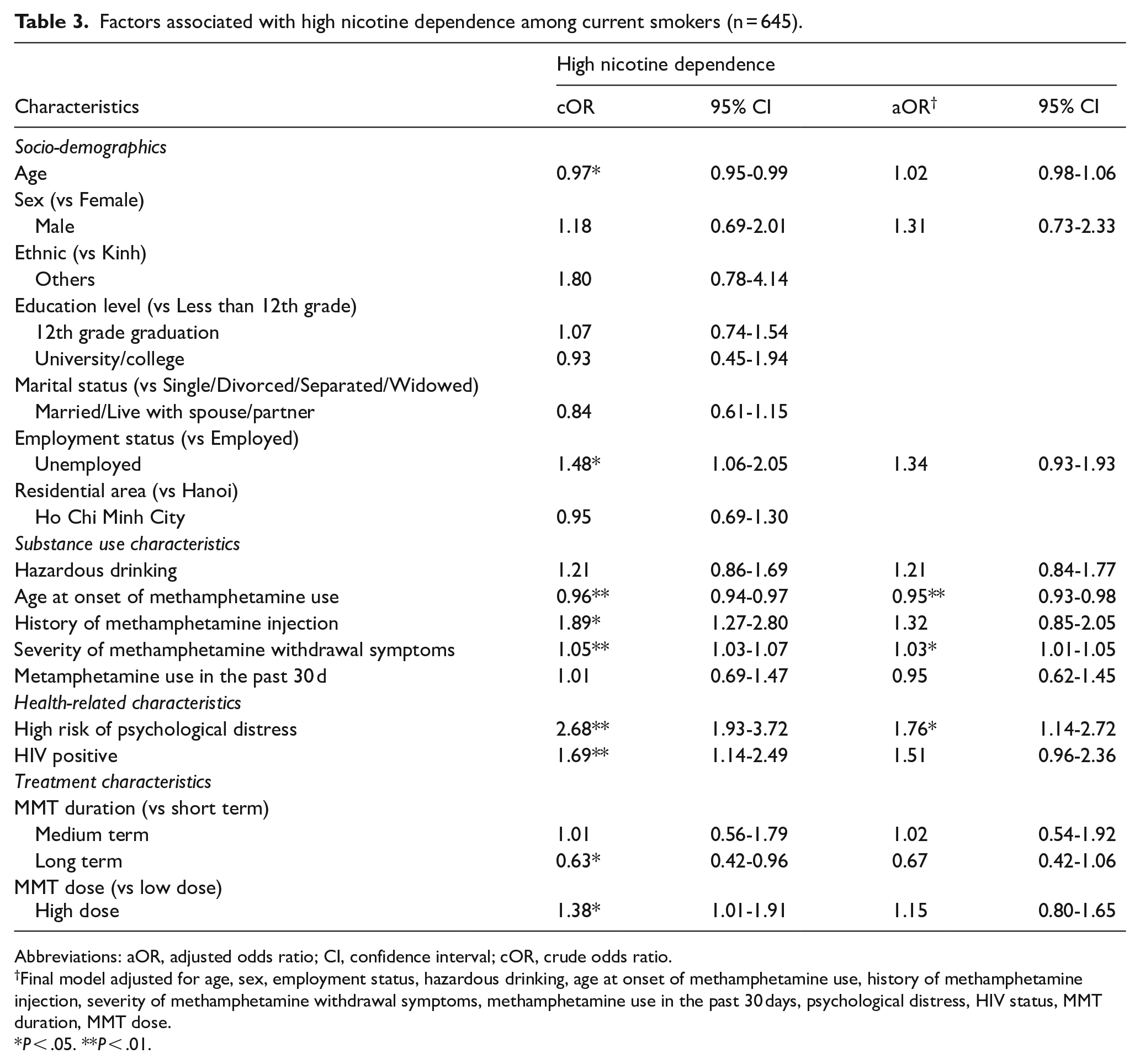
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; cOR, crude odds ratio.
Final model adjusted for age, sex, employment status, hazardous drinking, age at onset of methamphetamine use, history of methamphetamine injection, severity of methamphetamine withdrawal symptoms, methamphetamine use in the past 30 days, psychological distress, HIV status, MMT duration, MMT dose.
P < .05. **P < .01.
Discussion
This study found a high prevalence of smoking among methadone-treated people who use methamphetamine, the study revealed that nearly all participants were current smokers (96.7%). This prevalence is significantly higher compared to other studies conducted among people in addiction treatment in United States 29 and Vietnam.3,30 Additionally, our study revealed an average FTND score of 4.6 (±2.2), which is slightly higher than the average FTND score of 4.5 (±2.4) reported in a study of 1016 people undergoing MMT in 20173. However, when compared to a cross-sectional study on 1822 Central Vietnamese men, 21 where the average FTND score was 4.1 (±2.4) and 30% of participants had an FTND score of 6 or higher, the FTND scores and proportions in our study appear somewhat higher. The higher prevalence of current smokers and greater nicotine dependence observed in our sample can be attributed to the unique characteristics of our participants, who were not only undergoing MMT but also presented with active or potential disordered methamphetamine use. This is further supported by the finding that multiple substance use disorders were associated with greater severity of tobacco use disorder. 31
In terms of nicotine dependence as defined by the FTND as a predictor of smoking cessation, previous studies have shown that higher nicotine dependence is associated with greater difficulty in quitting smoking, with nicotine-dependent individuals being 4 times less likely to successfully quit compared to non-dependent smokers.32,33 However, research also suggested that cigarette consumption could predict cessation outcomes as quitting rates declining as the number of cigarettes smoked per day increases (smokers consuming 20 or more cigarettes per day had a cessation rate of 11.1%, while those smoking fewer than 20 cigarettes per day had a higher quitting rate of 24.6%). 33 Notably, while nearly 40% of participants in our study exhibited high FTND scores, the majority (92.9%) smoked fewer than 20 cigarettes per day. This finding underscores a potential opportunity for early smoking cessation interventions, as individuals with high nicotine dependence but lower cigarette consumption may still have a relatively greater chance of quitting successfully.
Our study found that greater severity of methamphetamine withdrawal symptoms was associated with an increased risk of high nicotine dependence. These findings align with existing evidence on the neurobiological pathways linking methamphetamine use and nicotine dependence. First, the association between methamphetamine withdrawal severity and nicotine dependence is consistent with neurobiological research indicating that both substances modulate the mesolimbic dopamine system, a key mechanism in addiction, thereby reinforcing their interaction.13 Nicotine has also been shown to modulate dopamine release in methamphetamine-sensitized individuals, promoting nicotine-seeking behavior as a means to counteract withdrawal-induced dopaminergic deficits.34,35 Additionally, behavioral conditioning may further contribute to this association, as frequent co-use of nicotine and methamphetamine strengthens cue-induced cravings and reinforces habitual smoking as a coping mechanism for withdrawal distress. 36 Therefore, individuals experiencing more severe methamphetamine withdrawal symptoms are more likely to engage in heavier smoking behavior and are at greater risk of high nicotine dependence. Given the observed relationship between methamphetamine withdrawal symptoms and nicotine dependence, our findings emphasize the need for integrated management of withdrawal symptoms alongside smoking cessation efforts among people on MMT.
Furthermore, we found that earlier initiation of methamphetamine use was associated with greater nicotine dependence, consistent with Yimsaard et al’s study on 991 participants using methamphetamine at a substance treatment center. 37 One possible explanation is provided by the gateway hypothesis, which suggests that early exposure to 1 addictive substance increases the likelihood of subsequent dependence on others.38,39 This mechanism may help explain the observed association between earlier methamphetamine initiation and greater nicotine dependence. However, our findings are limited to observed associations and do not establish causation. Therefore, future studies are needed to determine whether early methamphetamine use contributes to increased nicotine dependence over time.
Our study also found that 38.7% of participants had at least 1 psychological distress, a prevalence higher than the 26.8% reported in a previous study among people on MMT in Vietnam. 40 This difference may be due to variations in sample characteristics, as our study specifically included individuals who use methamphetamine, which is associated with higher odds of mental health outcomes. 41 Differences in assessment methods may also contribute to this discrepancy. Furthermore, the finding that participants with high nicotine dependence had much greater odds to be at high risk of psychological distress reinforces the well-documented link between psychological symptoms and nicotine dependence, as global studies have consistently shown a significant association between emotional distress and smoking behaviors.42 -44 The self-medication hypothesis provides 1 possible explanation, suggesting that individuals with mental illness use cigarette as a temporary coping mechanism due to its short-term mood-enhancing effects. 45 Additionally, emotional disorders may increase the risk of smoking initiation and dependence through maladaptive coping mechanisms. 46 These findings highlight the need to incorporate mental health care into smoking cessation programs, as addressing psychological distress may improve cessation outcomes among people on MMT.
Lastly, it is important to note that the FTND was developed to assess the physiological aspects of tobacco dependence and to help guide treatment decisions based on the severity of physical addiction. Although nicotine is only one of the many components in tobacco, it is primarily responsible for the substance’s addictive properties. In our study, we adopted the FTND to quantify nicotine dependence as a biological construct. Previous research has shown that while the FTND is a valid tool for capturing physical dependence, it explains only a limited proportion of psychological dependence in smokers. 47 Future studies may consider integrating complementary instruments to capture the broader spectrum of tobacco dependence, including psychological and behavioral dimensions, particularly in populations with complex substance use profiles.
The main strengths of our study were a large sample size and validated instruments (FTND, DASS- 21, AUDIT-C) that have demonstrated excellent reliability in numerous studies and in the Vietnamese context. However, several limitations should be acknowledged. First, the cross- sectional design limits our ability to draw causal inferences. Second, substance use behaviors were primarily self-reported, which may be subject to recall and social desirability biases. Third, the study was conducted in only 2 cities, potentially limiting the generalizability of the findings to all individuals receiving methadone treatment in Vietnam. Finally, no a priori sample size calculation was conducted, as the study utilized existing data from a larger parent study. Nonetheless, the sample size was sufficiently large to support robust statistical analyses and yield stable parameter estimates.
Conclusion
The findings reveal that current smoking and high nicotine dependence are prevalent among people with methamphetamine use undergoing MMT in Vietnam. Assessing early methamphetamine use history and severity of methamphetamine withdrawal symptoms could help identify individuals at elevated risk of nicotine dependence. Providing smoking cessation support, alongside managing methamphetamine withdrawal symptoms could enhance cessation efforts in this population.
Supplemental Material
sj-docx-1-sat-10.1177_29768357251347819 – Supplemental material for Exploring Nicotine Dependence Among People Using Methamphetamine During Methadone Maintenance Treatment in Vietnam
Supplemental material, sj-docx-1-sat-10.1177_29768357251347819 for Exploring Nicotine Dependence Among People Using Methamphetamine During Methadone Maintenance Treatment in Vietnam by Nguyen Truong Giang, Nguyen Bich Diep, Nguyen Thu Trang, Pham Thanh Luan, Hoang Thi Hai Van, Do Van Dung, Michael Li, Chunqing Lin, Li Li, Steve Shoptaw and Le Minh Giang in Substance Use: Research and Treatment
Footnotes
Acknowledgements
We extend our sincere gratitude to the methadone clinics that participated in this study and to the participants who generously contributed their time and information. We also wish to acknowledge the research members for their efforts and expertise in shaping this work.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by National Institutes of Health (Grant number 1R01DA050486-01).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.